
Abstract
Background:
Multilingualism is associated with enhanced executive function and may thus prevent cognitive decline and reduce the risk of dementia.
Objective:
To determine whether multilingualism is associated with delayed onset or reduced risk of dementia.
Methods:
Dementia was diagnosed in the Nun Study, a longitudinal study of religious sisters aged 75+ years. Multilingualism was self-reported. Dementia likelihood was determined in 325 participants using discrete-time survival analysis; sensitivity analyses (n = 106) incorporated additional linguistic measures (idea density and grammatical complexity).
Results:
Multilingualism did not delay the onset of dementia. However, participants speaking four or more languages (but not two or three) were significantly less likely to develop dementia than monolinguals (OR = 0.13; 95% CI = 0.01, 0.65, adjusted for age, apolipoprotein E, and transition period). This significant protective effect of speaking four or more languages weakened (OR = 0.53; 95% CI = 0.06, 4.91) in the presence of idea density in models adjusted for education and apolipoprotein E.
Conclusion:
Linguistic ability broadly was a significant predictor of dementia, although it was written linguistic ability (specifically idea density) rather than multilingualism that was the strongest predictor. The impact of language on dementia may extend beyond number of languages spoken to encompass other indicators of linguistic ability. Further research to identify the characteristics of multilingualism most salient for risk of dementia could clarify the value, target audience, and design of interventions to promote multilingualism and other linguistic training as a strategy to reduce the risk of dementia and its individual and societal impacts.
Keywords
INTRODUCTION
The average age of the global population is steadily increasing. As such, the number of people suffering from age-related diseases, such as dementia, will also increase [1]. No pharmacological intervention can currently prevent or modify the progression of dementia [2]. Thus, identification of modifiable protective factors is key to guiding dementia prevention strategies. One potential modifiable factor is cognitive stimulation, which may delay or prevent dementia by enhancing resistance to neuropathology-induced cognitive decline through cognitive resilience, the ability to recruit and use neural networks more efficiently to maintain normal cognition despite neuropathology that might otherwise manifest as dementia [3–5]. Education and cognitively stimulating occupations and lifestyles are examples of factors suggested to increase cognitive resilience [5–7].
Another factor that may increase cognitive resilience is multilingualism. Some studies have reported a protective association of multilingualism with Alzheimer’s disease (AD) and related dementias [8]. Monolinguals have been found to manifest AD at younger ages than multilinguals speaking two [9–13] or three or more languages [14, 15]. This evidence of a ‘multilingual advantage’ in risk of dementia has been explained based on the premise that the use of multiple languages strengthens executive function, thereby enhancing cognitive resilience [9, 16–18], and is supported by evidence of anatomical [19–24] and biomarker [25] differences in the brains of multilinguals compared to monolinguals.
However, evidence of a protective effect of multilingualism on cognitive impairment, including dementia, AD, and cognitive decline, has been inconsistent. Reports of a protective effect of bilingualism have primarily been based on cross-sectional studies of clinic populations [9–13, 18], with population-based prospective studies not supporting this association [26–32]. This inconsistent evidence of the impact of multilingualism on dementia likely reflects differences in sample populations, study designs, and definitions of multilingualism. The populations studied are heterogeneous, with strong potential for confounding by these heterogeneous characteristics. Clinical samples reflect selection biases related to cognitive function and health service use; cross-sectional studies, with their prevalent cases, do not directly assess risk. How multilingualism is defined is also a factor: for example, some studies found significant impacts only when participants spoke more than two languages, rather than the more commonly studied two languages (i.e., bilingualism) [14, 34]. The variation in results calls into question the proposed protective mechanism of multilingualism for dementia, or at least the characteristics of multilingualism and populations that influence the risk of dementia. Research contributing to clarification of the evidence base for an association between multilingualism and dementia would also clarify the value, target group and design of interventions to promote multilingualism as a dementia prevention strategy.
Our aim was to investigate the impact of multilingualism on onset and risk of dementia in a population-based, prospective cohort study of older adults who were dementia-free at baseline. We examined this association in the context of standard demographic and genetic covariates as well as indicators of cognitive resilience and additional measures of linguistic ability.
MATERIALS AND METHODS
Study population
The Nun Study is a longitudinal study of aging in members of the School Sisters of Notre Dame [35–38]. Of 1,031 eligible participants aged 75 years and older at baseline in 1991, 678 (66%) participated, agreeing to annual cognitive and physical assessments, brain donation after death, and access to archival records. Participants and non-participants did not differ significantly by mean age, country of birth, mortality rate, or race. All participants were women with similar adult lifestyles, including social activities, social supports, marital and reproductive histories, alcohol and tobacco use, socioeconomic status (SES), and access to health services. Informed consent was originally obtained in 1990 and updated in 2006. Original ethics approval for the Nun Study was granted by the University of Kentucky Institutional Review Board. Ethics approval for this project was obtained from the Office of Research Ethics at the University of Waterloo.
Measures
Dementia
Cognitive assessments were completed annually for participants both with and without dementia. Cognitive function was assessed by trained gerontologists using the CERAD battery of neuropsychological tests [39]. The Mini-Mental State Exam (MMSE) was used to screen for global cognitive function [40]. Participants were assessed for dementia based on impairments in memory (Delayed Word Recall score <4) and at least one other cognitive domain (Verbal Fluency score <11, Boston Naming <13, or Constructional Praxis <8). All cut-off points were derived from normative data for the CERAD battery [41, 42]. Dementia diagnosis required participants to show functional decline in activities of daily living (ADLs), which included performance-based tests of feeding, dressing, standing, walking, and toileting [43, 44].
Multilingualism
Convent archives provided data on multilingualism, which had been collected in 1983 by an administrative questionnaire developed by the School Sisters of Notre Dame [45]. Participants reported the languages with which they had proficiency so that international mission placements could be determined. The number of languages reported ranged from one to five; because only a small proportion of participants spoke four or five languages, these categories were combined.
Covariates
Data on age, education, occupation, and written linguistic ability [36, 46] were obtained from convent archives. Education was categorized as having completed grade school, high school, a Bachelor’s degree, or a Master’s degree or higher. Since few participants had educational levels lower than a Bachelor’s degree, the two lowest educational categories were combined. Occupation was categorized dichotomously (teacher or other) as most participants were teachers: the mission of the School Sisters of Notre Dame is the education of women and children.
Autobiographical essays written by participants in early adulthood (18 to 32 years of age; mean 22 years) were coded to obtain measures of English written language skills [37]: idea density [47] and grammatical complexity [48]. Idea density was defined as the average number of ideas expressed per ten words. Grammatical complexity scores ranged from zero (one-clause sentences) to seven (sentences using multiple clauses and embedding). Mean idea density and grammatical complexity scores were calculated for each participant based on the final ten sentences of each autobiography, ranked within each convent, and divided into quartiles. Only 180 members of the original Nun Study population provided handwritten autobiographies; therefore, a sensitivity analysis using a subset of participants with these data was performed to supplement the main analyses.
Apolipoprotein E (APOE) genotype from buccal cells in living participants or from brain tissue obtained at time of autopsy was assessed using standard methods [49] and blinded to participant cognitive status. Immigration status (born in the United States versus other) was included to adjust for its potential effects on multilingualism [10, 33]. Analyses also considered the time period between cognitive assessments as a potential covariate. This study used data from 12 cognitive assessments; therefore, 11 transition periods (mean = 1.51 years in length; SD = 0.32) were evaluated for inclusion in the analyses.
Sample
Primary analyses were based on 325 participants without dementia at baseline who had a complete baseline cognitive assessment, at least one follow-up cognitive assessment, and data on multilingualism and APOE. Participants were excluded if they transitioned from demented to non-demented status at any assessment (n = 32), given the resultant ambiguity in the time of dementia onset. A sensitivity analysis adjusting for other linguistic ability measures (written linguistic skill measures of idea density and grammatical complexity) was conducted using a subset of participants with data on these linguistic measures (n = 106).
Analysis
Bivariate analyses included Pearson chi-square tests, with Yates continuity correction and Fisher’s exact tests as appropriate; independent sample t-tests, with Satterthwaite correction for unequal variances as required; and Cochrane-Armitage tests for trend. Given the study design of cognitive assessments on a scheduled (i.e., approximately annual) basis, discrete-time survival analysis was used to calculate the hazard probability of dementia (i.e., the proportion of participants at risk for the event that actually experienced the event in a defined time period), and whether it varied by multilingualism and time. A hazard function refers to the chronological pattern of the estimated hazard probabilities over time. The magnitude of a hazard function in a specific time period describes the magnitude of the estimated risk for the event in that time period— the greater the risk, the higher the hazard in the given time period. The discrete-time survival analysis produced assessments of the risk of dementia using hazard function estimates generated from logistic regression models, which also generated conditional odds ratios (ORs).
Variables considered for inclusion in the regression models included all multilingualism categorizations (i.e., four, three, or two categories for number of languages spoken), all time indicators (predictive estimates associated with each of 11 transition periods), occupation, education, baseline age, immigration status, and APOE ɛ4 status. Idea density and grammatical complexity were also considered in the sensitivity analysis. The selection of variables to include in the regression models was determined using the likelihood ratio test, which gauged model suitability by measuring the difference in deviance statistics between models. The likelihood ratio test established whether the inclusion of an additional parameter was justified by an appropriate decrease in deviance. This model selection method is preferred for choosing discrete-time survival regression models [50]. These models were assessed for fit based on Hosmer-Lemeshow goodness-of-fit test statistics and standard residual diagnostics, and tests of multicollinearity were performed. All analyses were conducted using SAS version 9.2 (SAS Institute Inc., Cary, North Carolina).
RESULTS
Of 325 participants, 33.5% (n = 109) developed dementia at some point during the 11 waves of follow-up (Table 1). Overall, age, number of follow-up assessments, and presence of an APOE ɛ4 allele were significantly associated with dementia. There was no significant association between dementia and multilingualism overall. However, significantly fewer participants speaking four or more languages developed dementia compared to those speaking fewer than four languages (5.9% [1/17] versus 35.1% [108/308]; p = 0.01). Participants who developed dementia were significantly older at baseline than participants remaining dementia-free (mean 83.8 versus 81.7 years; p < 0.001) (Table 1). Almost half (47.5%; 28/59) of APOE ɛ4 carriers developed dementia compared to 30.5% (81/266) of non-carriers (p = 0.02).
Participant characteristics by dementia status (n = 325)
APOE ɛ4, apolipoprotein E ɛ4 allele; SD, standard deviation. Note: Percentages may not total 100% due to rounding. 1Participants did not have dementia at any cognitive assessment. 2Participants were dementia-free at baseline cognitive assessment but developed dementia during the follow-up period. *p < 0.05; **p < 0.01; ***p < 0.001.
Dementia hazard ORs were calculated to determine the association between multilingualism and time of dementia onset (Table 2). Adjusted ORs for dementia in participants speaking two or three languages did not differ significantly from monolinguals; however, speaking four or more languages (compared to one language) was associated with a significant seven-fold decrease in dementia odds (OR = 0.13; 95% CI = 0.01, 0.65). Older participants at baseline were significantly more likely to develop dementia. The possession of an APOE ɛ4 allele was also associated with a significant increase in odds for dementia over the study period (OR = 2.53; 95% CI = 1.55, 4.05). Time, or each individual transition period, had a limited effect on the dementia hazard probability estimates, with none significantly associated with dementia development. Although participants speaking four or more languages had significantly lower hazard probabilities than monolinguals, these dementia hazard functions did not fluctuate over time, thus showing no effect of multilingualism on time of dementia onset (Table 2).
Dementia hazard odds ratios generated from a model of dementia hazard probability adjusted for multilingualism, baseline age, apolipoprotein E status, and transition time period (n = 325)
APOE ɛ4, apolipoprotein E ɛ4 allele; CI, confidence interval; OR, odds ratio. Note: Bolded values indicate statistical significance. 1No estimate available for transition period 11 as the parameter estimate was equal to zero.
Since dementia hazard function estimates were constant and persisted throughout the study follow-up period, dementia hazard probabilities were interpreted as having one value for a given group of participants over the entirety of the follow-up period, and the final model was reduced to exclude time as a covariate. The most statistically suitable model for dementia probability estimation consisted of a four-level multilingualism variable, age at baseline, and APOE ɛ4 status (Fig. 1). As in Table 2, this reduced model also showed no significant association with dementia for participants speaking two or three languages, but a significant protective effect for those speaking four or more languages.

Hazard functions for development of dementia by multilingualism, baseline age, and apolipoprotein E status (n = 325). Note: Hazard functions and probabilities were estimated using a model adjusted for all three variables. APOE-ɛ4, apolipoprotein E-ɛ4 allele.
The dementia hazard probability in APOE ɛ4 carriers was 2.4 times higher (p < 0.001) than in participants without an APOE ɛ4 allele (Fig. 1). Older age at baseline was also associated with greater dementia risk: compared to participants under 80 years of age who spoke the same number of languages and had the same APOE ɛ4 status, those 80 to <85 years old were 1.6 times (p < 0.05) and those aged 85 or older were 4.5 times (p < 0.0001) more likely to develop dementia. An interaction existed between the number of languages spoken and the other risk factors. For example, an APOE ɛ4 carrier who was 85 years or older at baseline and who spoke four or more languages (dementia hazard probability = 0.04) had a risk of dementia similar to an APOE ɛ4 non-carrier who was younger than 80 years at baseline and spoke only one language (dementia hazard probability = 0.03) (Fig. 1).
Written linguistic ability subset
A sensitivity analysis was performed to determine if the relationship between multilingualism and dementia hazard probability differed in the context of additional linguistic ability measures. This analysis was thus restricted to a subset with data on written linguistic ability (n = 106), resulting in a sample where all participants were born in the United States and had at least a high school education. Of 106 participants, 28 (26.4%) developed dementia (Table 3). Overall, number of follow-up assessments, education, presence of an APOE ɛ4 allele, and idea density were significantly associated with dementia. Although not statistically significant, almost twice as many monolinguals developed dementia as those who spoke two or more languages (39.4% [13/33] versus 20.6% [15/73]; p = 0.057). Higher educational attainment showed a significant protective association with dementia (p = 0.008). Approximately half (10/21) of the APOE ɛ4 carriers developed dementia compared to 21.2% (18/85) of noncarriers (p = 0.02). Although idea density was significantly associated with dementia, there was no significant association of bilingualism or multilingualism with either idea density or grammatical complexity.
Participant characteristics by dementia status: Written linguistic ability subsample (n = 106)
APOE ɛ4, apolipoprotein E ɛ4 allele; SD, standard deviation. Note: Percentages may not total 100% due to rounding. 1Participants did not have dementia at any cognitive assessment. 2Participants were dementia-free at baseline cognitive assessment but developed dementia during the follow-up period. *p < 0.05; **p < 0.01; ***p < 0.001.
All covariates, including each of the 11 transition periods, were tested in the sensitivity analysis to determine their significance to dementia probability estimation. The most statistically suitable model included APOE ɛ4 status, education, and a two-level idea density variable (i.e., first [lowest] quartile versus second, third, and fourth quartiles, which were combined given similar parameter estimates for the top three quartiles). Multilingualism was not significantly associated with dementia likelihood after adjustment for these variables (Table 4), although this may be due in part to the lower sample size for the sensitivity analysis. Participants who spoke three languages had lower dementia hazard probabilities than participants who spoke one language; those speaking four or more languages had the smallest dementia hazard probability estimates (Fig. 2). While speaking a greater number of languages reduced the dementia hazard probability estimates compared to participants with similar APOE ɛ4, education, and idea density profiles, none of these reductions were statistically significant. Participants with an APOE ɛ4 allele, low idea density or low education generally were at greater risk of developing dementia; however, individuals with these risk factors were still able to decrease their likelihood of dementia, albeit nonsignificantly, if they spoke more than two languages.
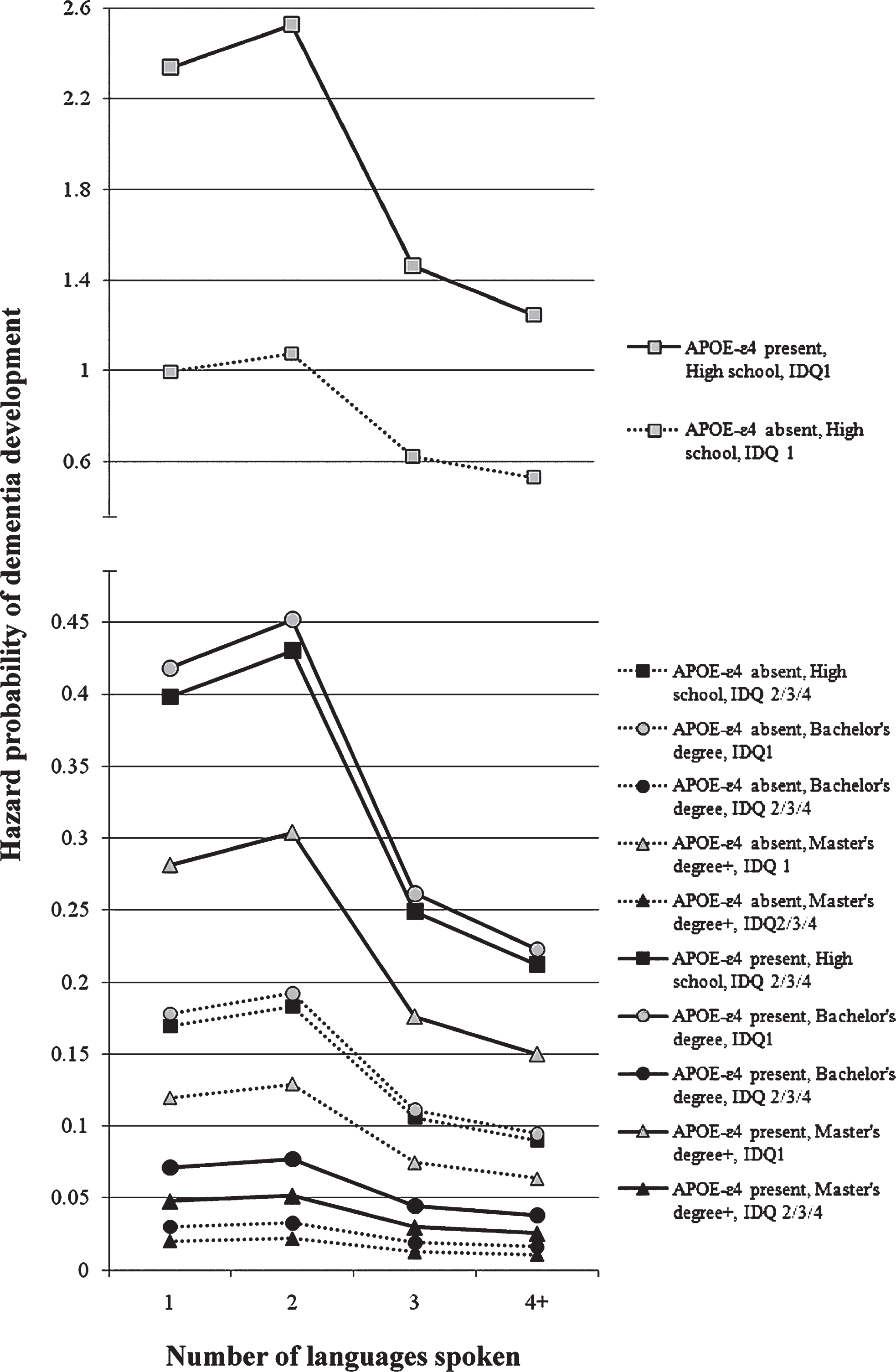
Hazard functions for development of dementia by multilingualism, apolipoprotein E status, education, and idea density: Written linguistic ability subset (n = 106). Note: Dashed lines represent hazard functions for participants without an APOE-ɛ4 allele. APOE-ɛ4, apolipoprotein E-ɛ4 allele; IDQ, idea density quartile.
Dementia hazard odds ratios generated from a model of dementia hazard probability adjusted for multilingualism, apolipoprotein E status, education, and idea density: Written linguistic ability subsample (n = 106)
APOE ɛ4, apolipoprotein E ɛ4 allele; CI, confidence interval; OR, odds ratio. Note: Bolded values indicate statistical significance. 1Lower idea density represents idea density scores from the lowest quartile; higher idea density represents scores from the top three quartiles.
DISCUSSION
We examined the association of multilingualism with onset and risk of dementia in prospective data from participants who developed dementia as well as from participants who remained dementia-free; analyses adjusted for standard demographic and genetic covariates, as well as indicators of cognitive resilience and additional measures of linguistic ability. Our study results are consistent with and extend those of other prospective, population-based studies [26–32]. Bilingualism (i.e., speaking two languages) did not significantly affect age at onset of dementia in our study. However, participants speaking four or more languages (but not two or three) were significantly less likely to develop dementia than monolinguals. The protection conferred by speaking multiple languages could reduce a given participant’s dementia risk, despite older age or the presence of an APOE ɛ4 allele. Sensitivity analyses investigating the influence of other measures of linguistic ability on the impact of multilingualism on dementia showed no significant association between dementia and any number of languages spoken, with the protective effect on dementia of speaking four or more languages weakened to nonsignificance in the presence of idea density. Thus, linguistic ability broadly was a significant predictor of dementia in our study. However, it was written linguistic ability (specifically idea density) rather than multilingualism that was the strongest predictor.
Differences between our results and those studies finding bilingual advantages with respect to dementia risk may be due to differences in populations, outcomes, or definitions of multilingualism. Differences in clinic and population-based samples may explain discrepancies between findings from memory clinic-based studies [9–13, 18] and those from our study and other population-based studies [26–32]. The lack of evidence to support an association between bilingualism and dementia is consistent with the results from other population-based prospective studies [26–32]. For example, Yeung et al. [26] found that bilinguals from a Canadian population-based cohort did not have a lower risk of dementia than monolinguals. Similarly, bilingual status did not protect against cognitive decline among a Japanese-American cohort [27], and non-native English speakers in the United States did not have a lower risk of dementia or AD [28]. Although associated with higher initial levels of cognitive performance, bilingualism was not found to protect against cognitive decline or development of dementia in a cohort of Hispanic immigrants to the United States [29]. Further studies have found no significant associations between bilingualism and the onset of dementia among Hispanic Americans [30] and a Swedish cohort [31]. Lastly, no significant differences were found in the decline of MMSE scores of bilinguals and monolinguals among an Australian cohort [32]. In addition, heterogeneity in sample characteristics such as age and APOE, powerful predictors of dementia, may contribute to differences in study results. In particular, despite the established influence of APOE on risk of dementia, most of the literature from either clinic or population-based studies did not consider the effect of APOE when assessing the association between multilingualism and dementia [9–13, 32].
Variations in study results may also reflect differences in the outcomes they study. Clinic-based studies [9–15, 18] have compared age at dementia onset or diagnosis between multilingual and monolingual patients from memory clinics. If the interest is in risk of dementia, clinic-based studies may miss important aspects of the relationship between multilingualism and dementia as they do not focus on individuals who remain cognitively intact. In addition, clinic-based cases are influenced by selection biases related to health service use. Both clinic-based and population-based samples often include prevalent dementia rather than incident dementia cases, such as those used in our study and which more directly assess risk of dementia.
Variation in reported results may also reflect variations in the definitions of multilingualism used across studies. Consistent with our results, some studies support a protective effect only when more than two languages were spoken. Chertkow et al. [14] found no significant differences between monolinguals and bilinguals in a clinic population; the only beneficial impact on AD appeared to be when three or more languages were spoken. Chertkow et al. suggested their results may reflect differing SES levels between monolinguals and multilinguals, as lower SES levels in multilinguals may nullify expected late-life cognitive benefits. In our study, however, all participants had similar SES levels yet results remained similar to those of Chertkow et al., suggesting that variation in SES may not explain their findings. Further evidence of a differential effect by number of languages spoken was reported by Kavé et al. [33], who found that participants who spoke four or more languages had better cognitive performance than those who spoke two or three languages. A population-based retrospective nested case-control study of multilingualism and cognitive impairment without dementia (CIND) also showed a greater benefit of speaking more than two languages: the risk of CIND decreased seven-fold in participants speaking three versus two languages [34].
In addition to the number of languages studied, past studies also vary in their measure of multilingualism. Our definition of multilingualism was not as stringent as in some of the studies which found bilingual advantages: we ascertained multilingual status through self-reports of languages spoken proficiently whereas other accounts of multilingual cognitive advantage have measured language proficiency through fluency testing or by having participants actively use the language(s) with which they claimed proficiency. The equal use of multiple languages every day (e.g., being “balanced” in many languages) was also not a requirement in our study. Use of more stringent definitions for multilingualism in some studies [9, 13] may explain why they found an association with dementia among those speaking two or more languages whereas we did not see any impact until our highest levels of multilingualism (four or more languages). It may also be that it is only these multilingual individuals who were actively using, or more likely to use, their multi-language capabilities in their daily life. That is, their job posting (location) and regular teaching duties may have been chosen specifically because they were highly capable in many different languages, and thus were placed into situations where they more regularly and actively made use of their linguistic abilities. This increased daily practice in use and coordination of multiple languages may have been the key to their development of cognitive resilience, over and above that of the participants who reported fluency in only two languages, and could explain why we only found protective effects for those speaking four or more languages. Based on the supply-demand framework of experience-dependent neuroplasticity (reviewed in [51, 52]), cognitive improvements occur when the demands on cognitive processes are greater than the available supply of cognitive resources (i.e., a supply-demand mismatch). If the demand of daily use of two languages were similar to the less stringently defined use of more than two languages (i.e., more languages, but lower intensity), then this framework would provide a theoretical rationale for the inconsistency in reported protective effects of bilingualism.
Overall, the variation in results calls the proposed mechanism of dementia protection by multilingualism into question: while multilingualism may bestow advantages in executive control upon a given individual, these advantages may not necessarily contribute to cognitive resilience. In contrast to little evidence of a protective effect of bilingualism in population-based studies, there is some evidence in these studies of a reduced risk of cognitive impairment and dementia in those speaking more than two languages. However, this is a highly selected population and individuals capable of speaking three or more languages (or four or more languages in our study) may be systematically different from those speaking one or two languages; it may be these traits rather than multilingualism that are associated with heightened cognitive resilience.
Linguistic ability more broadly defined than simply number of languages is another way in which these individuals may differ. Our analyses included additional measures of linguistic ability that have not been examined in previous studies of multilingualism. These measures from autobiographical essays written many decades before development of dementia may reflect not only linguistic ability but also more generally premorbid cognition function. Inherent multilingual disadvantages in types of linguistic ability (e.g., multilinguals exhibit less developed vocabularies in each of their known languages than monolinguals [53]) may conceal the true association of multilingualism with dementia. Measures other than multilingualism have been previously associated with dementia: low idea density has been significantly associated with greater dementia risk and cognitive decline [37, 46]. Therefore, incorporating idea density in the discrete-time survival analysis was expected to change the observed association between multilingualism and dementia: it did so, with the effects of multilingualism weakened in the presence of idea density. The lack of a significant association between written linguistic ability measures and multilingualism supports the separate effects of these factors. The influence on dementia of multiple linguistic measures and their inter-relationships thus warrants further exploration in studies of the association of multilingualism with dementia.
A strength of our study was the ability to assess multilingualism in the context of alternative measures of linguistic ability, which have not been examined in previous studies of multilingualism. Studies unable to examine multiple measures of linguistic ability may be more likely to find a significant association between multilingualism and dementia.
Our study is the first to our knowledge to evaluate the relationship between multilingualism and dementia using discrete-time survival analysis. Time of dementia onset and the duration an individual spent free of dementia could thus be factored into the dementia risk estimates. In addition, our analyses accounted for confounders not previously studied, and our participants were religious sisters whose similarity in adult lifestyles also controlled for many other confounders. Research in this area has been criticized for its inability to assess SES as a confounder, either because of the lack of data or the difficulty in separating confounding influences from immigration and SES. In our study, all participants had similar adult lifestyles, including SES-related characteristics such as income, in addition to similar social activities and supports, marital and reproductive histories, diets, substance use, and access to health services. We assessed the impact of important covariates and determined the impact of multilingualism within subgroups of these covariates, such as those defined by age and APOE status. The strong control of confounding factors addresses limitations present in much of the past literature, given the heterogeneity of populations studied and the potential for multilingualism to be related to other factors also associated with dementia.
Limitations of our study include the self-reported measure of multilingualism. Given that our investigation used secondary data collected years before the inception of the Nun Study, we did not have the option to objectively assess language proficiency, nor did we have data on other measures such as age at language acquisition. The questionnaire collecting data on multilingualism, however, was intended to facilitate future placements, including teaching positions abroad, and participants would therefore have presumably reported proficiency in only the languages in which they believed they could teach. In addition, a population-based study that used both self-report and objective measures of language ability found the same lack of association with dementia with either measure [29].
Our analyses were also limited by the size of our subset assessing alternate linguistic ability measures. The association between multilingualism and risk of dementia may have become statistically significant in a larger sample even after adjustment for the other linguistic ability measures, although the strength of the association observed was still much weaker than in the primary analyses. This subset may also have been subject to selection biases compared to the larger sample. In addition, the unique nature of our participants (religious sisters) means that our results may be less generalizable to other individuals. There is no cause to believe, however, that the relationship of multilingualism with dementia etiology would be altered in our population.
The question of whether multilingualism protects against the development of dementia is of broad interest and growing research activity. Contradictory reports reflect the complexities of this association. We found no evidence to support a later onset of dementia in bilinguals. A significant protective effect of multilingualism on dementia risk was observed only at the highest number of languages and weakened in the context of other measures of linguistic ability. Further research should evaluate the influence of multilingualism on dementia in prospective studies across populations, accounting for other measures of linguistic ability and important confounders. Further work is also needed to clarify characteristics of multilingualism most salient for risk of dementia, such as age at language acquisition, similarity of languages spoken, level of proficiency, and frequency of use. Such knowledge could clarify the value, target audience, and design of interventions to promote multilingualism and other linguistic training as a strategy to reduce the risk of dementia and its individual and societal impacts.