
Abstract
There is an ongoing debate about how cancer and dementia relate to each other, and whether their relation is biologically determined or caused by surveillance and survival bias. We aimed to circumvent these biases by determining the relation between the tumor marker carcinoembryonic antigen (CEA) and the risk of dementia in 6,692 participants from the population-based Rotterdam Study. We found that higher levels of CEA were associated with a higher risk of dementia (HR per standard deviation increase in CEA = 1.11, 95% CI 1.04; 1.18). This finding may indicate that cancer and dementia are positively associated, but the mechanisms underlying the relation between CEA and dementia warrant further investigation.
INTRODUCTION
Cancer and dementia are leading causes of morbidity and mortality worldwide [1, 2]. Although both diseases are common in the elderly population, their relation is poorly understood [3]. Various observational studies have shown that patients with cancer have a lower risk of developing dementia, and vice versa [4–8]. Different biological explanations underlying this inverse association have been proposed, including genetic predisposition for either promoting or suppressing cell proliferation and cell survival pathways [9]. Yet, patients with cancer or dementia are less likely to be screened for other diseases and have often a limited life expectancy. Therefore, methodological issues including surveillance and survival bias might drive the association toward an inverse direction.
Several studies have tried to tackle these methodological issues, for instance by studying the risk of dementia in patients with different stages of cancer. Patients with advanced stage cancers had the lowest risk of dementia, probably because their mortality risk is higher than that of patients with early stage cancer [10]. In addition, it has been shown that with appropriate model specification, patients with cancer do not have a lower risk of dementia [11]. Lastly, we have shown that persons with mild cognitive impairment (MCI), the transitional stage between normal cognition and dementia, even tended to have a higher risk of cancer than that of persons with normal cognition [12]. Although MCI and dementia share the same biological underpinnings, the life expectancy of persons with MCI is longer than that of patients with dementia, thereby limiting the effects of the competing risk of mortality. The higher risk of cancer in persons with MCI therefore suggests that the association between cancer and dementia might even be positive rather than inverse.
Studying the preclinical stage of one disease and linking it to the other disease could limit the effects of surveillance and survival bias, because the life expectancy of persons in the preclinical stage of a disease is longer than that of patients with clinically-manifested disease. Censoring for death as competing risk could result in biased effect estimates, if censoring happens to be informative [13, 14]. Also, studying the preclinical stage can reduce the effects of selective survival, i.e., those patients who survive cancer are likely to have some protective characteristics that help them to survive [15]. This can further improve our understanding of the biological association between cancer and dementia. Carcinoembryonic antigen (CEA) is an often-used tumor marker, usually in clinical settings to monitor cancer recurrence in curated cancer patients rather than for screening purposes. In this study, we used CEA as marker for preclinical, undiagnosed cancer in community-dwelling individuals free from clinically-diagnosed cancer and related this to the risk of dementia. Using this design, we aimed to circumvent the effects of the competing risk of mortality on the relation between cancer and dementia (see Fig. 1).
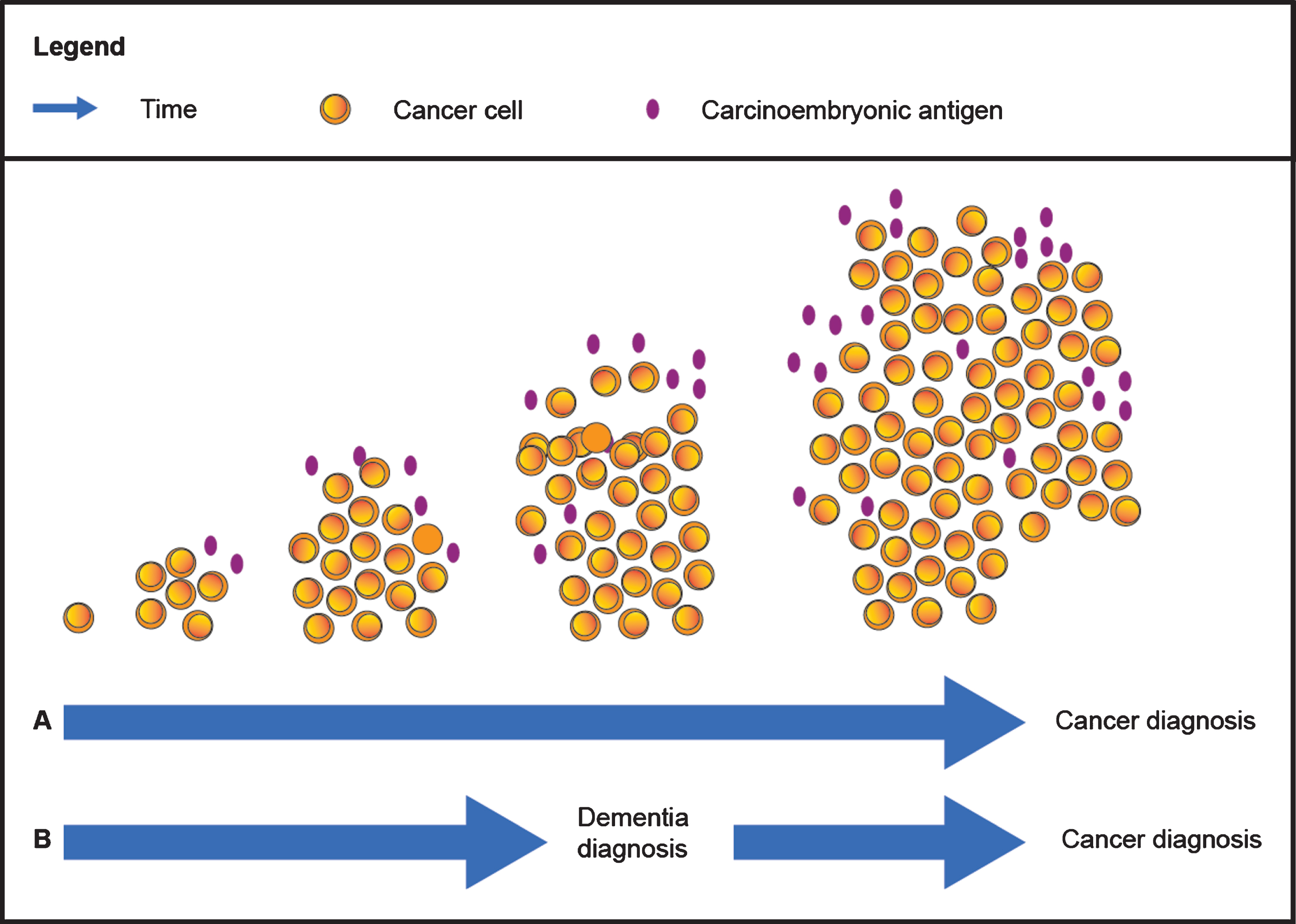
Schematic relation between carcinoembryonic antigen, cancer and dementia. The time between the first cancer cell and clinical manifestation of the disease can last up to many years. Before clinical manifestation of cancer, cancer cells might already produce different factors including carcinoembryonic antigen. Therefore, carcinoembryonic antigen levels could be elevated before the diagnosis of cancer (scenario A, upper arrow). It is also possible that a person develops both dementia and cancer. Before this person is diagnosed with dementia, this person can already have a preclinical stage of cancer (scenario B, lower arrow). During this preclinical stage of cancer, carcinoembryonic antigen levels might already be elevated. These carcinoembryonic antigen levels could therefore be used to link the preclinical stage of cancer to dementia.
METHODS
Study population
This study is embedded within the Rotterdam Study, a prospective population-based cohort designed to study the occurrence and determinants of diseases in the elderly population. The cohort has been described in detail previously [16]. Briefly, in 1990 all inhabitants aged 55 years or over from the district Ommoord in Rotterdam, the Netherlands, were invited to participate. This initial cohort (RS-I) comprised 7,983 participants and was extended (RS-II) in 2000 with 3,011 participants who had become 55 years of age or moved into the study district. In 2006, the cohort was further extended (RS-III) with 3,932 participants aged 45 years or over. In total, the Rotterdam Study comprises 14,926 participants (overall response rate 72%).
The Rotterdam Study has been approved by the Medical Ethics Committee of Erasmus Medical Center and by the board of The Netherlands Ministry of Health, Welfare, and Sports. A written informed consent was obtained from all participants.
CEA levels were determined in plasma samples of 7,305 participants that had been obtained during the third visit of RS-I (1997-1999) and the first visits of RS-II (2000-2001) and RS-III (2006-2008). From these 7,305 participants, we excluded those with a history of dementia (n = 75) or insufficient data to determine cognitive status (n = 65). In addition, we excluded participants with a history of cancer (n = 425) to study the association between CEA and dementia in a population free from clinically-diagnosed cancer. It is, however, possible that participants had an undiagnosed, preclinical stage of cancer at the date of blood sample draw. Lastly, we excluded participants without informed consent to access medical records during follow-up (n = 48). This resulted in 6,692 participants for analyses.
CEA assessment
Blood was sampled in EDTA coated tubes and centrifuged, of which subsequently plasma was aliquoted and frozen at –80°C according to standard procedures. CEA ( μg/L) was measured using the Roche Modular P800 Analyzer (Roche Diagnostics, Indianapolis, IN, USA). The coefficient of variation for intermediate precision was 17.3%, and for repeatability was 13.9%.
Dementia assessment
Participants were screened for dementia at baseline and subsequent center visits with the Mini-Mental State Examination and the Geriatric Mental Schedule organic level [17]. Those with a Mini-Mental State Examination score <26 or Geriatric Mental Schedule score >0 underwent further investigation and informant interview, including the Cambridge Examination for Mental Disorders of the Elderly. In addition, the entire cohort was continuously under surveillance for dementia through electronic linkage of the study database with medical records from general practitioners and the regional institute for outpatient mental health care. Available information on clinical neuroimaging was used when required for diagnosis of dementia subtype. A consensus panel led by a consultant neurologist established the final diagnosis according to standard criteria for dementia based on information collected during center visits and obtained from medical records (Diagnostic and Statistical Manual of Mental Disorders III-revised). Follow-up until January 1, 2016 was virtually complete (93.8% of potential person-years observed).
Other assessments
During home interviews, participants provided information on educational level, smoking status, and alcohol use. Educational level was categorized as primary education, lower (lower/intermediate general education or lower vocational education), intermediate (intermediate vocational education or higher general education), or higher (higher vocational education or university). Smoking status was classified into never, current, or former. Alcohol use was categorized as no use or any use. At the research center, height and weight were measured from which the body mass index (kg/m2) was computed. Diagnosis of cancer was obtained from general practitioners’ medical records (including hospital discharge letters), and through linkage with Dutch Hospital Data, regional histopathology and cytopathology registries, and the Netherlands Cancer Registry [18]. Follow-up of cancer registration was completed up to January 1, 2015.
Statistical analysis
Characteristics of the study population were stratified by normal (CEA < 5.0 μg/L) and high (CEA≥5.0 μg/L) CEA levels. This cut-off value between normal and high CEA levels has been proposed by the Colorectal Working Group of the American Joint Committee on Cancer [19].
We used Cox proportional hazards models to obtain hazard ratios (HRs) and 95% confidence intervals (95% CIs) to investigate the association between CEA (continuous and in quartiles) and the risk of dementia. In addition, we compared the risk of dementia in participants with normal CEA levels (CEA < 5.0 μg/L) and high CEA levels (CEA≥5.0 μg/L). CEA levels were standardized to obtain the effect per one standard deviation (SD) in CEA.
Follow-up time was used as timescale and started at the date of the blood sample draw until the date of dementia diagnosis, death, loss to follow-up, or January 1, 2016, whichever came first. We verified that the choice of the timescale (follow-up versus age) did not affect the results. HRs were adjusted for age at blood sample draw, sex, education, body mass index, smoking status, and alcohol use. The proportional hazards assumption was checked by visual inspection of the Schoenfeld residuals.
In sensitivity analyses, we censored participants after two and five years of follow-up to examine the strength of the association between CEA and dementia when CEA was measured more closely to the date of dementia diagnosis.
Lastly, to support the use of CEA levels as proxy for the preclinical stage cancer, we determined the relation between CEA levels and the risk of cancer using the same models as those used in the analysis for the relation between CEA levels and the risk of dementia. In this analysis we included the participants with a history of dementia or with insufficient data to determine their cognitive status. Follow-up time started again at the date of the blood sample draw, but ended at the date of cancer diagnosis, death, loss to follow-up, or January 1, 2015, whichever came first.
Multiple imputation was used for missing covariates (maximum of 0.9%) with five imputed datasets based on other covariates and outcome. Rubin’s method was used for pooled HRs and 95% CIs. Statistical analyses were performed using the package ‘survival’ in RStudio Version 3.3.2 [20].
RESULTS
Table 1 shows the characteristics of participants with normal (n = 6,238) and high (n = 454) CEA levels. The median (interquartile range) age of participants with normal CEA values was 60.3 years (56.3; 67.9), and that of participants with high CEA values was 60.2 years (56.3; 67.9). Participants with high CEA levels were more often current smokers than those with normal CEA levels. During a median (interquartile range) follow-up of 8.8 years (7.2; 14.5), 471 out of 6,692 participants were diagnosed with dementia, of whom 25 (5.3%) had high CEA levels.
Characteristics of the study population stratified by carcinoembryonic antigen level
Characteristics were measured during the visit of the blood sample draw. Data are presented as frequency (percent) unless indicated otherwise. Missing values are not imputed and therefore numbers do not always sum up to 100%. aPresented as median (interquartile range). bPresented as mean (standard deviation).
Higher levels of CEA were associated with a higher risk of dementia (HR per SD increase in CEA level = 1.11, 95% CI 1.04; 1.18, Table 2). Participants with high CEA levels had a higher risk of dementia than those with normal CEA levels, albeit not statistically significant (HR = 1.14, 95% CI 0.76; 1.72). Compared to participants with CEA levels in the lowest quartile, those with levels in the highest quartile had a higher risk of dementia (HR = 1.28, 95% CI 0.99; 1.65).
The association between carcinoembryonic antigen and the risk of dementia
Hazard ratios are adjusted for age at blood sample draw, sex, education, body mass index, smoking status, and alcohol use. aCarcinoembryonic antigen levels were standardized. bExpressed per standard deviation increase. CI, confidence interval; HR, hazard ratio; n, number of participants with incident dementia; N, total number of participants.
Sensitivity analyses yielded slightly higher effect estimates when censoring participants after two years (HR per SD increase in CEA level = 1.16, 95% CI 1.09; 1.23) and five years of follow-up (HR per SD increase in CEA level = 1.13, 95% CI 1.07; 1.20, Table 2).
Supplementary Table 1 shows the results regarding the relation between CEA levels and the risk of cancer. Higher levels of CEA were associated with a higher risk of cancer (HR per SD increase in CEA level = 1.18, 95% CI 1.15; 1.21). This relation was most pronounced in participants with high CEA levels (HR 2.51, 95% CI 2.00; 3.13). The effect estimates hardly changed when censoring participants after two and five years of follow-up.
DISCUSSION
CEA is a tumor marker widely used in oncology for surveillance and to assess treatment response. The observed association between higher levels of CEA and a higher risk of dementia may imply that patients with dementia are more likely to have preclinical cancer prior to their dementia diagnosis. These findings are further supported by a previous study showing that patients with dementia have higher CEA levels than healthy individuals [21].
The current findings indicate the possibility of a positive association between cancer and dementia. Given that higher CEA levels are associated with more advanced stages of cancer [22], the slightly higher risk of dementia when censoring participants after two and five years of follow-up might suggest that cancer is already more advanced shortly before dementia diagnosis. It has indeed been shown that dementia patients who were subsequently diagnosed with cancer, had more advanced stages of cancer [23]. Nevertheless, given that observational studies repeatedly find a lower risk of dementia in cancer patients [4], it is likely that cancer remains undiagnosed in the majority of the patients after dementia diagnosis. Cancer-related symptoms may be obscured by dementia-related frailty (i.e., surveillance bias), or remain subclinical due to early death (i.e., survival bias) [3].
The potential positive link between cancer and dementia may be explained by three proposed underlying mechanisms. First, cancer and dementia share multiple risk factors such as higher age, obesity, lack of activity, smoking, and alcohol use. Second, several pathways are involved in the pathogenesis of both diseases, including inflammation, genome instability, and angiogenesis [24]. Third, different proteins that are related to neurodegeneration, including amyloid-β and tau [25, 26], can be elevated in cancer patients, suggesting that these proteins might also be involved in the pathogenesis of cancer [27–29]. In addition, over expression of the amyloid-β protein precursor in cancer cells is associated with cell proliferation, migration, and invasion [29]. Also, the tumor suppression protein BRCA1 has been linked to dementia [30]. Higher amyloid-β burden was associated with BRCA1 dysfunction, resulting in more DNA damage and in deterioration of genomic integrity. Future research on potential underlying mechanisms should further elaborate on the relation between different types of cancer and cancer treatments, and dementia.
However, a word of caution is warranted. Although the tumor marker CEA is often elevated in patients with different types of cancer, including colorectal, pancreatic, and breast cancer [31], it is primarily used for monitoring recurrence in curatively treated patients with colorectal cancer [22]. Although we found that higher CEA levels were associated with a higher risk of cancer, CEA is not used for screening of cancer in the general, unselected population, because the sensitivity and specificity are limited [32]. CEA can be elevated due to other reasons apart from cancer, such as smoking, inflammation, and hepatic insufficiency [33, 34]. Despite the fact that these conditions are partly related to cancer, they offer an alternative explanation for our finding as drivers of the observed association between CEA and dementia.
In conclusion, the relation between CEA and dementia is intriguing and points toward a positive association between cancer and dementia and not to the often postulated inverse association. The mechanisms underlying the association between CEA and dementia and its causality warrant further examination.
Footnotes
ACKNOWLEDGMENTS
We gratefully acknowledge the study participants of the Ommoord district and their general practitioners and pharmacists for their devotion in contributing to the Rotterdam Study. Special thanks to Prof.dr. J.C. Kiefte-de Jong, Department of Public Health and Primary Care, Campus The Hague, Leiden University Medical Center, The Hague, the Netherlands, and Dr. M. Kavousi, Department of Epidemiology, Erasmus MC - University Medical Center Rotterdam, Rotterdam, the Netherlands for funding the measurements of carcinoembryonic antigen in plasma samples from participants of the Rotterdam Study (den Dulk-Moermans foundation, Leiden University Fund).
The Rotterdam Study is funded by Erasmus Medical Center and Erasmus University, Rotterdam, Netherlands Organization for the Health Research and Development (ZonMw), the Research Institute for Diseases in the Elderly (RIDE), the Ministry of Education, Culture and Science, the Ministry for Health, Welfare and Sports, the European Commission (DG XII), and the Municipality of Rotterdam. Further support was obtained from the Dutch Cancer Society (NKI-20157737). The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.