
Abstract
Background:
Dementia care management (DCM) aims to provide optimal treatment for people with dementia (PwD). Treatment and care needs are dependent on patients’ sociodemographic and clinical characteristics and thus, economic outcomes could depend on such characteristics.
Objective:
To detect important subgroups that benefit most from DCM and for which a significant effect on cost, QALY, and the individual cost-effectiveness could be achieved.
Methods:
The analysis was based on 444 participants of the DelpHi-trial. For each subgroup, the probability of DCM being cost-effective was calculated and visualized using cost-effectiveness acceptability curves. The impact of DCM on individual costs and QALYs was assessed by using multivariate regression models with interaction terms.
Results:
The probability of DCM being cost-effective at a willingness-to-pay of 40,000€ /QALY was higher in females (96% versus 16% for males), in those living alone (96% versus 26% for those living not alone), in those being moderately to severely cognitively (100% versus 3% for patients without cognitive impairment) and functionally impaired (97% versus 16% for patients without functional impairment), and in PwD having a high comorbidity (96% versus 26% for patients with a low comorbidity). Multivariate analyses revealed that females (b = –10,873; SE = 4,775, p = 0.023) who received the intervention had significantly lower healthcare cost. DCM significantly improved QALY for PwD with mild and moderate cognitive (b = +0.232, SE = 0.105) and functional deficits (b = +0.200, SE = 0.095).
Conclusion:
Patients characteristics significantly affect the cost-effectiveness. Females, patients living alone, patients with a high comorbidity, and those being moderately cognitively and functionally impaired benefit most from DCM. For those subgroups, healthcare payers could gain the highest cost savings and the highest effects on QALYs when DCM will be implemented.
Keywords
INTRODUCTION
At present, about 1.7 million people are estimated to live with dementia in Germany [1, 2]. Even though some latest evidence suggests a decline in age-specific incidences [3], prevalence of dementia is expected to double every 20 years due to an increase in life expectancy and a growing number of older people [4]. Dementia diseases represent one of the economically most important disease groups of older age [5, 6]. Without a cure, the focus of therapy and health care shifts to providing the best possible care.
According to variations in individual unmet needs and priorities of people with dementia (PwD), it is necessary to initiate and coordinate individualized patient-centered treatment and care that aimed to improve patients and caregivers outcomes and reduce health care cost for public payers [7]. This highlights the urgent need to incorporate the patient, (informal) caregiver, and other service providers in advanced care planning. Treatment and care needs are dependent on patients’ sociodemographic and clinical characteristics and thus, economic outcomes could depend on such characteristics. To address all these demands, interdisciplinary and individualized treatment and care are crucial.
Collaborative care programs have proven their potential to achieve this. Care and case management interventions are based on evidence-based guidelines and recommendations, are usually delivered in the community, aim to detect existing unmet needs, and enhance the coordination of treatment and care within the primary health care system [8]. There is some evidence that collaborative care and case management approaches are beneficial by improving person-centered outcomes in PwD. The systematic review of Reilly et al. [8] demonstrated that case management programs could reduce hospitalizations and the length of hospital stays, may postpone institutionalization, alleviate behavior disturbance and depression, and improve social support for patients and caregivers. In Germany, there is scientific evidence for the efficacy and safety of a collaborative care program as well. In a general practitioner (GP)-based cluster-randomized controlled trial with n = 634 patients, it was demonstrated that people who benefited from Dementia Care Management (DCM) showed better dementia-specific treatment, higher prescription rate of anti-dementia drugs, less neuropsychiatric symptoms, and higher Health-related quality of life (HRQoL). Furthermore, caregivers burdened was reduced [9, 10].
Only a few studies evaluated the cost-effectiveness of such programs, revealing inconclusive evidence [8, 11–15]. This has been acknowledged by the World Alzheimer Report 2016, highlighting the need for economic evaluations. Even though the Cochrane review [8] pointed out that case management increases the use of community services, it is more cautious about the economic impact by stating that overall healthcare costs “may be” reduced in the first year. Other published studies on case management and support programs in PwD reported a reduction in quality-adjusted life years (QALY), but still a non-significant reduction in cost, which would be an inadequate scenario [16, 17].
Michalowsky et al. [7] determined the incremental cost-effectiveness ratio (ICER) of the collaborative dementia care management versus usual care in Germany and confirmed a significant gain in QALYs by modestly reducing health care cost over a 24 months’ time horizon. However, savings in costs were rather uncertain.
The lack of significance may be due to lack of power for a cost effect as costs are highly skewed. It may also be due to an application of the program to individuals less likely to achieve improved health outcomes, reduced costs, or both. However, there is a lack of cost-effectiveness studies acknowledging the heterogeneous group of patients (for example, in sociodemographic or clinical parameters). Trial-based cost-effectiveness analyses typically adopt a cohort-based approach and compare the cost and effects of the intervention versus the control group using the entire trial sample. The individual effect of an intervention on the patient may be associated with certain individual sociodemographic and clinical characteristics of the patient, and its cost-effectiveness could therefore vary between subgroups. An individual cost-effectiveness analysis under consideration of different covariates could detect important subgroups where the effectiveness of such an intervention is higher from a health economic point of view.
Therefore, this study aimed to identify important sociodemographic and clinical characteristics of PwD receiving DCM that are associated with higher cost-effectiveness of the intervention.
MATERIALS AND METHODS
Study design
This analysis was based on longitudinal 24-months data of the DelpHi-MV trial, a pragmatic, GP-based, cluster-randomized controlled prospective intervention trial, evaluating a collaborative DCM [9, 10]. The DCM of the DelpHi-MV study was developed to support PwD and their caregivers in primary care [9, 18]. The DCM was operationalized as a complex intervention aiming to provide optimal treatment and care for PwD and support to caregivers in close cooperation with the treating GP. It was provided by dementia-specific qualified nurses and supported by a computerized Intervention Management System [19, 20].
In total, 136 GP practices participated in this trial. Based on simple randomization without stratification or matching (1:1), these practices were randomized to the intervention (DCM) or to the control group (usual care). GP practices checked patients’ eligibility for the trial (≥70 years, living at home) and screened for dementia using the DemTect procedure [21]. PwD of a GP whose practice was randomized to the intervention group received the DCM; PwD of control group GPs received care as usual. The study protocol and documents for written informed consent were approved by the Ethical Committee of the Chamber of Physicians of Mecklenburg-Western Pomerania (registry number BB 20/11). The design of the trial is described in the study protocol [9, 10].
Sample
Initially, 6,838 people were screened at 128 GP practices, and n = 1,167 (17%) PWD were found eligible for the study. 634 PwD gave an informed consent to participate in this study and n = 516 started the baseline assessment (intervention: 348 PwD; controls: 168 PwD). A detailed description of this sample is given elsewhere [22]. After completing the baseline assessment, n = 85 participants withdrew their informed consent, n = 73 passed away, and n = 6 postponed the first and second follow-ups, resulting in a sample of 408 and 352 participants who accomplished the first and second follow-up. This analysis was conducted on a sample of 444 participants who received either the DCM or usual care and completed the baseline and at least one of the two follow-up assessments or died (dead patients were included in this analysis) [23, 24]. The study flow chart and the drop-out analyses are described in more detail elsewhere [7, 25].
Intervention
The intervention was developed according to current guidelines [26–29], targeted at the individual participant level, delivered at participants’ homes by nurses with dementia-specific qualification, and focused on the management of interprofessional treatment and care, medication management and caregiver support and education. A specifically qualified nurse, the so-called Dementia Care Manager, collected data on medical, nursing, and social characteristics of each PwD and his or her caregiver [19]. The care managers subsequently identified patients’ and caregivers’ unmet needs. These needs were discussed, consented, and carried out in cooperation with the treating GP. The duration of the intervention was six months. The intervention is described in more detail by Eichler et al. [18]. Costs for implementing the DCM are presented by Michalowsky et al. [7]. Effectiveness, efficiency, and health economics of the DCM concept were published elsewhere [25, 31].
Data assessment
Comprehensive data assessments were conducted at baseline, and after 12 and 24 months of follow-up. Baseline assessment, intervention, and annual follow-ups were carried out by dementia care managers.
HRQoL was measured using the 12-Item Short-Form Health Survey (SF-12), a generic, multidimensional instrument that measures the physical dimension of HRQoL with respect to the perception of general health, physical functioning, bodily pain, and role limitations due to the physical health state, as well as mental dimensions including social functioning, mental health, and vitality and role limitations due to emotional state [32].
Healthcare resource utilization was assessed retrospectively through face-to-face interviews. Within the standardized interviews with the PwD and their caregivers (as well as, if possible, with the professional care staff), a list of widespread healthcare resources and services were used. The utilization review assesses medical care services uses, such as physician visits, in-hospital treatments, medications, medical aids and therapies, ambulatory care, day care, and nursing home care.
Sociodemographic data included age, gender, and living situation (alone versus not alone). In addition, the following clinical variables were assessed: cognitive impairment (Mini-Mental State Examination, MMSE) [33], comorbidity (Charlson Comorbidity Index, CCI) using ICD-10 diagnoses listed in the patients GP files [34], depression (Geriatric Depression Scale, GDS) [35], and deficits in daily living activities (Bayer Activities of Daily Living Scale, B-ADL) [36].
Missing values were handled by Multiple Imputation by Chained Equations (MICE). Multiple imputation models were specified for each variable and adjusted for age, gender, living situation, and comorbidity [24, 38]. Imputations were conducted on the item level, adding 50 additional data sets for each missing variable [7, 39].
Calculation of QALYs and costs
Health utilities were derived from the SF-12 using the method of Brazier & Roberts and used to calculate QALYs for each patient separately [40]. The responses to the SF-12 were converted to health utilities using the SF-6D algorithm. A linear change of HRQoL between baseline, 12 months, and 24 months was assumed, which is consistent with the nature of dementia diseases, represented by growing cognitive and functional deficits, in turn, increasingly affecting HRQoL. In addition, a linear relationship for the change of HRQoL has been found to be the most commonly used approach in the trial-based CEA literature and has been applied in other recent economic evaluations targeting PwDs [41–44]. In case of death (the exact date was recorded), the utility value was assumed to equal zero. Finally, individual QALYs were calculated by using the area under the curve technique and discounted at 5% per year [41, 42].
Published unit costs were used to calculate the average costs per patient. All costs were discounted at 5% per year and were calculated from a public payer’s perspective in 2018 Euros over the two-year follow-up trial period [45, 46].
Definition of subgroups
Previous analyses revealed that, for example, patients living situation, comorbidity, or functional impairment were associated with higher costs or lower quality of life [7, 48]. Therefore, specific patient subgroups of this analysis were derived from the following sociodemographic and clinical variables: sociodemographic characteristics considered were age (<80 years versus 80 years and older), sex (male versus female), and living arrangements (living alone versus not living alone); clinical characteristics considered were degree of comorbidity based on CCI (low (<2), high (2-3), and very high (>3)) [34], severity of cognitive impairment based on MMSE Score (none (>26), mild (20–26), and moderate to severe (0–19)) [29, 33], and deficits in daily living activities based on the B-ADL (no deficit (1.0–2.0), mild deficits (2.1–5.0), and high deficits (5.1–10.0) [36]).
Subgroup cost-effectiveness analysis
For each subgroup cost-effectiveness analysis, the complete sample has been split to generate consistent and homogeneous subgroups according to the mentioned sociodemographic and clinical variables listed above. Within each split sample, a full cost-effectiveness analysis was conducted, assessing the cost-effectiveness of the DCM compared to the control group as follows: The incremental cost-effectiveness ratio (ICER) was calculated using the incremental cost per QALY gained by the DCM program compared with usual care [49]. Due to the dependency of patients to clusters (GP practices), incremental costs and QALYs were estimated using linear regression models with random effects for the GP [41, 51]. Because of a highly skewed distribution of cost, standard errors and confidence intervals were estimated by bootstrapping (2,000 replications) [52]. To handle sampling uncertainty in the ICER, we used non-parametric bootstrapping, creating 1,000 resamples [53]. The probability of the DCM being cost-effective was calculated using these resamples and different willingness-to-pay (WTP) margins and displayed using cost-effectiveness acceptability curves [54, 55]. The methods used for this analysis were consistent with those of published methodological guidelines for undertaking economic evaluations [56]. All statistical analyses were performed using the software STATA/IC Version 13.0 [57].
Sensitivity analysis: Implementing interaction terms to analyze the association between the individual cost-effectiveness and patient’s characteristics
We assessed the impact of the DCM on individual total costs, QALY, and individual cost-effectiveness by using multivariate linear regression models with random effects as well. Total healthcare cost, QALYs, and the individual net monetary benefit (NMB), as a measure for the cost-effectiveness, was used as dependent variables. The individual NMB was assessed according to the recommendation of Ridder et al. [58–60]: each subject’s NMBi was defined as follows, using the observed data on the effects (ei) and cost (ci) for a PwD (i):
The individual NMB approach requires a selection of a willingness-to-pay margin (λ). Due to the subjective nature of which ceiling ratio was used, we selected a threshold of 40,000€, 80,000€, and 160,000€ per individual QALY (see Supplementary Table 1) [59].
To explore if the cost-effectiveness varies by subgroups, we used the following binary operators to specify factorial interactions between the subject characteristics and the intervention indicator as variables of interest: Study group (intervention) with age (reference:>80 years), sex (reference: female), living situation (reference: living alone), deficits in daily living activities (B-ADL) (reference: no deficits), cognitive deficits (MMSE) (reference: no indication for cognitive deficits), and comorbidity (CCI category) (reference: low comorbidity). Dummy variables were used as factor-variable operators for the categorical sociodemographic and clinical characteristics. The interaction terms with the intervention group were used to control for homogeneous effects across the single patient groups and to assign the mean cost, QALYs and individual NMB for different patient groups [61]. The interaction terms were additionally included as model variable. Each model was additionally adjusted for sociodemographic and clinical variables that were not included in the interaction term. Because of the highly skewed distribution of healthcare costs, standard errors and confidence intervals were again estimated by bootstrapping (2,000 replications) [62]. A description of the used STATA code, as well as visualization or the residuals of the linear regression models, are presented in Supplementary Document 1.
RESULTS
Characteristics of the study population
Patients were on average 80 years old, mostly female (60%), on average mildly cognitively (mean MMSE 22) and functionally impaired (mean B-ADL 4), and half of them were living alone (51%). 39% of the patients had a very high comorbidity (more than three comorbidities in addition to dementia). Table 1 describes the characteristics of the study population divided into intervention and control group. There were no significant differences in socio-demographic and clinical characteristics between intervention and controls. Subgroup sizes were as well balanced in the intervention and the control group.
Subject characteristics by treatment group (n = 444)
MMSE, Mini-Mental State Examination, Range 0–30, higher score indicates better cognitive function; B-ADL, Bayer-Activities of Daily Living Scale, range 0–10, lower score indicates better performance. *The MMSE is less sensitive for detecting milder forms of cognitive impairment (43%) compared to the DemTect procedure (80% to 100%) that was used for the screening in GP practices and the subsequent inclusion of patients in the trial [75, 76]. Therefore, it is possible that some patients, who were screened positive for dementia, are not cognitively impaired according to the MMSE (score 27 to 30). However, the number of false positive cases should be lower as demonstrated by the MMSE.
Incremental cost, QALYs, and ICERs overall and for subgroups
Overall, PwDs receiving the DCM tended to incur lower cost of 569€ (95% CI: –5,466€ –4,328€) and gained on average 0.05 (95% CI: –0.04 –0.14) more QALYs compared to care as usual over the 24 months’ time horizon. Therefore, DCM dominated the usual care.
For subgroups, features associated with the most promising ICERs were female and alone living, mild deficits in daily living, moderate to severe cognitive deficits, and a high comorbidity.
For females (–4,307 € and +0.04 QALY), and PwD living alone (–3,642 € and +0.03 QALY) as well as for PwD with mild functional (–2,678 € and +0.05 QALY) or moderate to severe cognitive deficits (–5,574 € and 0.10 QALY) and for PwD having a high comorbidity (–7,416 € and +0.07 QALY), the incremental cost was lower and the incremental QALYs was higher as compared to the entire sample, indicating a stronger dominance of the intervention. A description of the incremental cost and QALYs of the subgroups is presented in Table 2 and Supplementary Figure 1.
Description of incremental cost, effect and ICER of total sample and different identified subgroups
MMSE, Mini-Mental State Examination, Range 0–30, higher score indicates better cognitive function; B-ADL, Bayer-Activities of Daily Living Scale, range 0–10, lower score indicates better performance; SD, standard deviation; CI, confidence interval; ‡p < 0.01.
Table 2 summarize the differences in costs and QALYs at 24 months. Compared with usual care, the dementia care management was associated with higher QALY and lower cost for the total sample after 24 months. Incremental QALY and costs indicating that the dementia care management was more likely to be less costly and more effective according to QALY. For female and alone living patients with mild deficits in daily living, mild cognitive deficits and high comorbidity the incremental costs decreased but more QALY were gained. Therefore, the dementia care management still dominates the usual care from a cost-effectiveness perspective.
Probability of cost-effectiveness
The probability of cost-effectiveness for the total sample valued 88% at a WTP threshold of 40,000€ per QALY gained. For old PwD (≥80 years) the probability of the DCM being cost-effective (i.e., had a higher NMB relative to control) was much higher compared to the young PwD (<80 years) at the WTP of 0€ and 40,000€ per QALY gained (65% versus 39% and 87% versus 48%, respectively). It can be observed that the probability that the intervention is cost-effective was very high in females compared to males at the WTP of 0€ and 40,000€ per QALY gained (86% versus 2% and 96% versus 16%, respectively). In addition, compared to PwD not living alone, the probability of cost-effectiveness was much higher in PwD living alone at WTP thresholds of 0€ per QALY and 40,000€ (82% versus 13% and 96% versus 26%, respectively).
The probability of cost-effectiveness was higher in PwD with high deficits in ADL at a WTP threshold per QALY of 0€ (63% versus 24%, respectively) and 40,000€ (97% versus 16%, respectively). Furthermore, compared to PwD with no cognitive deficits (according to MMSE after screening), the probability of cost-effectiveness was higher in PwD with moderate cognitive deficits at a WTP threshold per QALY of 0€ (93% versus 18%, respectively) and 40,000€ (100% versus 3%, respectively). Compared to PwD with low comorbidity, the probability of cost-effectiveness of the DCM was higher in PwD with high comorbidity at WTP thresholds per QALY of 0€ (75% versus 37%, respectively) and 40,000€ (96% versus 26%, respectively). The probabilities of cost-effectiveness for the total sample as well as for each subgroup are presented in Fig. 1.
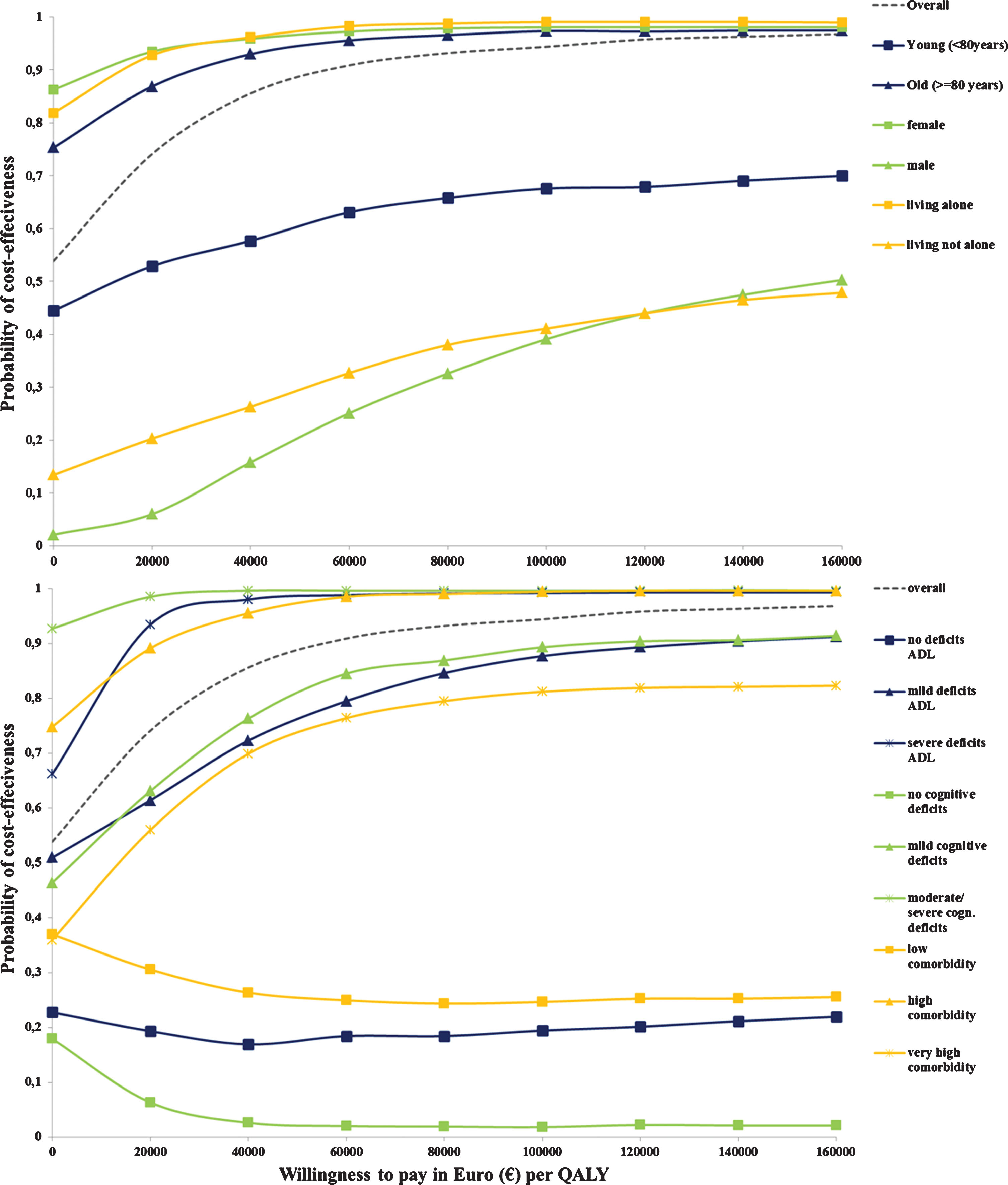
Cost-effectiveness acceptability curves, DCM intervention overall and subgroups.
Sensitivity analysis: Associations between different interaction terms and individual cost-effectiveness
The multivariate linear regression analyses revealed that female PwD (b = –10,873, SE = 4,775) who received the DCM caused significantly lower total healthcare cost over the 24 months’ time horizon compared to females receiving care as usual. Female PwD who received the DCM caused slightly higher cost for day and night care, medication, and medical aid, but significantly lower cost for in-hospital treatments (5,579€ versus 9,468€) due to fewer days stayed in a hospital (9 days versus 16 days) as well as lower cost for nursing home care (2,230€ versus 4,697€) due to a delayed institutionalization (12.4 months versus 4.4 months) over a 24 months’ time frame compared to female PwD receiving usual care. Furthermore, mildly (b = +0.226, SE = 0.093) or moderately cognitively impaired PwD (b = +0.232, SE = 0.105) and highly functionally impaired PwD (b = +0.200, SE = 0.095) showed a significant association with higher QALYs compared to those subgroups receiving usual care. Table 3 represents the association between different interaction terms (study group intervention # sociodemographic or clinical subgroup) and cost and effects of the DCM intervention compared to care as usual.
Association between different interaction terms (study group intervention # sociodemographic or clinical subgroup) and cost and effects
***0.001, **0.01, *0.05; 1comparison with control group patients having no indication for cognitive impairment; 2comparison with control group patients having no deficits in daily living activities; 3 comparison with control group patients having a low comorbidity.
The interaction between receiving the intervention and female sex (b = +11,733, SE = 3,721), living alone (b = +8,417, SE = 3,676), mild or moderate to severe cognitive deficits (b = +13,456, SE = 4,657; b = +12,621, SE = 5,579), as well as a high comorbidity (b = +13,007, SE = 4,607) were associated with a higher individual NMB at a willingness-to-pay threshold of 40,000€ /QALY, demonstrating that the DCM was more cost-effective for these subgroups. Associations remain stable at the ceiling ratios 80,000€ and 160,000€ but coefficients rise linear with increasing ceiling ratios.
The sensitivity analysis of the association between the interaction terms and the individual NMB for the ceiling ratio of 40,000€, 80,000€, and 160,000€ (λ) is displayed in Supplementary Table 1.
DISCUSSION
In this study, we describe the cost-effectiveness of DCM for different subgroups, providing valuable information to answer our question “Who benefits most from DCM?” from a patient and payer perspective. While DCM was associated with higher QALY and lower cost for the total sample after 24 months on average, the results were not statistically compelling. In part this may be due to inadequate power as costs in general and in this case tend to be highly variable. However, it may be also due to the application of the DCM in a diverse population, with some subjects more or less likely to respond to the intervention with improved outcomes and reduced costs. In our subgroup analyses, we suggested that DCM was especially promising for specific subgroups, specifically for women, people living alone, and people with higher comorbidity and higher cognitive and functional deficits. Particularly notable is that our findings were confirmed within linear regression models using interaction terms and the individual NMB of each PwD.
The DCM was more cost-effective in female PwD due to significantly lower costs for in-hospital treatment and nursing home care over a 24 months’ time frame. In addition, the DCM was more cost-effective in patients living alone, especially due to fewer physician visits and thereby significantly lower healthcare utilization and costs for treatment and care. PwD with mild and moderate to severe cognitive deficits, high functional deficits, and high comorbidity gained significantly more QALYs than patients without cognitive and functional deficits and low comorbidity.
The result that patients living alone benefit more from DCM is intuitive since patients not living alone received often more support and care from their relatives. Their needs are usually detected through the caregiver, who often lives in the same household. Because patients living alone have more often no relatives or caregivers able to provide informal care needed to maintain as long as possible at home. These PwDs can benefit most from a collaborative care management due to their higher number of unmet needs that could be addressed. In particular, arranging day and night care services as well as ambulatory care services could prevent unnecessary hospitalization and delay the institutionalization. Therefore, patients living alone showed lower incremental cost and higher incremental effects when their individual unmet needs were adequately addressed, as part of the DCM.
We found that female PwD who received the DCM caused lower cost and had higher QALY than male patients. The relatively higher net benefit for female within the sensitivity analysis implies that the value of the incremental benefit exceeded the incremental costs. The reasons could be the same as for patients living alone: Because female patients at a high age probably might have more often fewer relatives or carers, were living alone, and had high number of unmet needs. Thus, females can benefit more from collaborative care management programs. In addition, female patients receiving the collaborative care management had significantly lower cost for in-hospital treatments due to fewer days stayed in a hospital as well as lower cost for nursing home care due to delayed institutionalization.
In addition, PwD with a high comorbidity experience lower incremental costs and more QALYs through the intervention as PwD with low or very high comorbidity. Thus, for PwD with high comorbidity the dementia care management still dominates the usual care from a cost-effectiveness perspective. In our previous analysis, we identified a non-linear distribution of costs between the comorbidity subgroups and detects the lowest total costs in PwD with a high comorbidity [47]. Our present cost-effectiveness analysis demonstrates the same tendency. The probability of cost-effectiveness of the DCM was higher in PwD with a high comorbidity compared to PwD with a low or very high comorbidity. It could be supposed that comorbidities in PwD are under-reported, which may also point to an inappropriate management of the comorbidities and that intensive treatment of some comorbidities in dementia patients is inappropriate. This possibly indicates that treatment and care for PwD with high comorbidity is not as extensive as for those without complex needs. Thus, PwD with high comorbidity might have more unmet needs and can benefit more from a DCM through addressing these unmet needs adequately.
The sensitivity analysis with the NMB approach is consistent with the results of the multivariate approach; however, the NMB approach involves both cost and effectiveness estimates, and it would be incorrect to infer that the net-monetary benefits are significant simply because the corresponding coefficients from the cost and effect equations were individually significant [63]. However, the subgroups of female PwD, PwD with mild or moderate to severe cognitive deficits as well as PwD with high deficits in activities of daily living revealed as well significant NMB values. It could be assumed, that these subgroups showed higher and significant individual NMB due to lower significant incremental cost or higher significant incremental effects in the multivariate model. In addition, the NMB approach demonstrated more significant results in some selected subgroups than the multivariate approach. The association between different interaction terms and individual net monetary benefit with ceiling ratios of 40,000€, 80,000€, and 160,000€ indicated additionally significant NMB values for patients living alone and for PwD with a high comorbidity. However, the NMB method revealed no substantive changes in the results of the multivariate approach and confirmed the results of the cost-effectiveness acceptability curves.
Several studies evaluated the cost-effectiveness of DCM [64–70]. For dementia care or case management programs, only a few studies provide details on the cost-effectiveness compared to care as usual. For example, one study from the Netherlands evaluated the cost-effectiveness of two different types of case management compared to usual care. The results showed that less QALY were gained compared to usual care [71]. Another study of care-coordination of dementia patients showed a non-significant decrease of QALY as well [17]. These results are not equivalent to our findings. The patients in these trials were significantly more cognitively impaired. Consequently, the DCM was initiated later in the progression of dementia diseases. This could be an explanation for the finding of lower cost-effectiveness of previously published studies.
Another study assessed the cost-effectiveness of community-based occupational therapy compared with usual care in older patients with dementia. The results revealed that the intervention is cost-effective compared to care as usual [72]. The results are comparable to our findings. Furthermore, one analysis evaluated the cost-effectiveness with the NMB framework for preventive home visits in older people. The study evaluated the cost-effectiveness of preventive home visits. Costs and QALY were higher in the intervention group, but differences were not significant. For preventive home visits at a WTP per QALY of 50,000 EUR, there is a 15% probability that the intervention would be deemed cost-effective [73]. However, the results of these analyses are not readily comparable to the demonstrated results of our study as well due to the different sample characteristics and considerable differences in the intervention. In addition, most of the previous studies did not focus on important subgroups and did not analyze the individual cost-effectiveness. To our knowledge, there is presently no other study that detects subgroups of PwD who could benefit most from a DCM.
Because dementia is not curable today, there is a need for optimum treatment and care for those being affected by dementia. The increasing number of PwD is a major challenge for the health care system and society due to the increasing utilization of health care resources and the associated high healthcare expenditures [5, 6]. That is the reason why it is important to provide optimal support and evidence-based treatment for the affected patients to improve their living and care situation and to enable PwD to stay in their own home as long as possible. Innovative collaborative care models for PwD have met several of these challenges, and have been successful in the provision of optimal support and evidence-based treatment.
Our results provide detailed information on the costs and effects for specific patient groups that could benefit most from a dementia care management. They can, thus, support the implementation into routine care.
Due to demographic and societal transition, the number of PwD living alone increased. As a result of the aging population, there is an increasing number of especially female PWD who do not have any relative, friend, or neighbor close by who can take care of them. Eichler et al. (2016) revealed the high proportion of PwD living alone in Germany and demonstrated that PwD living alone were significantly more often female and older and have more unmet needs, less access to health care, untreated medical conditions, and earlier nursing home transition [74]. For those PwD, the DCM is a potential solution to achieve optimal coordination and management of treatment and care. Our result revealed that for the growing subgroup of females and alone-living PwD, a collaborative care management could be very beneficial by improving certain outcomes. Identifying subgroups for whom DCM is an especially good value could be of vital importance for decision makers in the health care system in order to improve the allocation of resources in face of the increasing economic burden due to dementia diseases.
Limitations
Several limitations of the study have to be taken into consideration. Firstly, the DelpHi-trial was conducted in Mecklenburg Western Pomerania, a mostly rural area in Germany. The generalizability of the results might be limited due to the region under analysis. However, due to the population-based design with GPs in a leading role, our results will likely extend to other regions, at least to those with similar characteristics.
Second, the number of patients between the intervention and control group was not adequately balanced. Due to the impossibility to blind the intervention, patients in the control group withdrew the informed consent more frequently. In addition, there are differences between the group sizes of selected subgroups. To reduce uncertainty in the estimation procedure, we used non-parametric bootstrapping with 2,000 replications and stratified for cluster and group distribution. Nevertheless, the different group sizes in some subgroups could have affected the results.
As shown in our previous cost-effectiveness analysis of the DelpHi-MV trial, drop out was significantly associated with being in the control group and very likely before starting the baseline assessment (n = 118 of 634, representing 19% of the total sample). GPs were not informed about their randomization status but become aware of their status during the course of the study due to the nature of the intervention. This could have led to a decreased motivation for the recruitment in the control group and thus to the higher drop out in controls before starting the baseline assessment. In addition, a lower comorbidity and a higher functional impairment of the PwD as well as a nonparticipation of the caregiver were significantly associated with a drop out. (Drop-out analyses presented in the trial flowchart were published elsewhere [7].) However, as pointed out in the result section, there were no significant group differences regarding sociodemographic and clinical data at baseline.
Third, we collected the healthcare resource use data via comprehensive standardized computer-assisted personal interviews and analyzed the self-reported information about utilization retrospectively for a period of one year. There might be a recall-bias that could lead to an under- or overestimation of the utilization. However, more comprehensive primary data from health insurances were not available and a national health institute does not exist in Germany. To minimize gaps in the self-report, the study assistants were trained to ask for proxy estimates as well wherever a caregiver was available.
Lastly, the net-benefit regression results depend on the maximum WTP per unit of effect. In general, there is a great difficulty in obtaining the WTP information. Caution should be exercised when normative statements are based on those values. Due to the controversy about which ceiling ratio to use, we calculate a series of NMB values by using a huge range of cost-effectiveness ceiling ratios. The cost-effectiveness acceptability curve offers a convenient presentation of cost-effectiveness results for a range of threshold values of additional health benefits. However, the net-benefit framework has the same limitations as traditional cost-effectiveness analyses.
Conclusion
This analysis indicates that the cost-effectiveness of DCM significantly differs in consideration of several subgroups. Collaborative care may be especially valuable for specific subgroups allowing tailoring such programs to PwD most likely to achieve significant cost savings and gains in QALYs. Specifically, we showed that women, PwD who were living alone, and PwD with a high comorbidity could benefit most from a DCM. For these subgroups, the DCM shows the highest individual cost-effectiveness compared to the usual care. Furthermore, PwD that were moderate to severely cognitively or functionally impaired achieved a higher gain in QALYs due to the DCM. Implementation of DCM into routine care could be most beneficial for these patients.
Footnotes
ACKNOWLEDGMENTS
This study is part of the DelpHi-MV trial (Dementia: Life- and person-centered help in Mecklenburg- Western Pomerania) and was funded by the German Center for Neurodegenerative Diseases (DZNE) and the University Medicine of Greifswald. Development, coordination and implementation of the DelpHi-MV study were influenced by input from several experts in their respective field and supported by an experienced field study team.