
Abstract
Background:
There is growing interest in public health strategies to modify dementia risk in midlife to reduce the burden of cognitive impairment in subsequent decades. Risk reduction messages should include key recommendations for women in response to the high prevalence of dementia observed in this population. Midlife is a critical period for dementia-related brain changes and psychosocial crises. Psychological well-being can improve resilience to crises, yet it is not well understood with respect to dementia risk reduction.
Objective:
This study aimed to examine the association between midlife psychological well-being and cognitive function in later life in women.
Methods:
The study included 703 women from the British 1946 birth cohort in the Medical Research Council’s National Survey of Health and Development. Psychological well-being at 52 years was assessed using the Ryff Scales of Psychological Well-being over six dimensions: autonomy, environmental mastery, personal growth, positive relations with others, purpose in life, and self-acceptance. Cognitive function at 69 years was measured using the Addenbrooke’s Cognitive Examination, Third Edition.
Results:
After controlling for cognitive ability at eight years, educational attainment by 26 years, occupational attainment and marital status by 53 years, depression, smoking, and physical exercise at 60–64 years, there was a significant association between greater personal growth and lower self-acceptance at 52 years, and better cognition at 69 years. However, there was no association between cognition and the other four Ryff scales.
Conclusion:
Most aspects of midlife psychological well-being, except for personal growth and self-acceptance, were not prospectively associated with cognition.
INTRODUCTION
With the global prevalence of dementia expanding rapidly, dementia risk reduction has emerged as a public health priority [1]. While dementia occurs mostly in older people, multiple risk factors exert varying influences throughout the life course [2–4]. In the absence of a cure for dementia, it is important that policy-makers promote evidence-based risk reduction messages that help individuals to take positive action. In particular, dementia affects a higher number of women than men, and they account for 60% of the global aging population [5]. Risk reduction messages should include key recommendations for women in response to the high prevalence of dementia in this group.
There is growing interest in modifying midlife risk factors to reduce the burden of cognitive impairment and dementia in subsequent decades. Midlife is seen as a crucial period at the beginning of dementia-related brain changes and cognitive aging [6]. Recent reviews of modifiable risk factors have highlighted physical activity and management of cardiovascular risk factors [4, 7], which are at the center of health-promotion activities. However, during midlife, people experience psychosocial crises due to increased financial and caregiving responsibilities and decline in physical health [8]. Psychological well-being can build resilience in the face of these crises. However, relatively little is known about psychological well-being in this context. This could modify the impact of stress on the brain and compensate for the long-term negative effects of early adversity during adjustment to aging [9]. In addition, the identification of midlife psychological factors that influence dementia risk could help policymakers to improve public messages in this context [10, 11]. Identifying the domain of psychological well-being associated with cognitive function in later life will help to improve public health strategies for the health promotion of middle-aged women who face midlife crises.
Previous studies have found mixed results regarding the associations between cognitive functioning and psychological well-being in older adults. Although an overall higher level of psychological well-being has been associated with better cognitive function [12], more recent studies suggest that specific domains, rather than overall well-being, are related to cognitive function, including negative affect [13], positive affect [14], and purpose in life [15–17]. These mixed results may have been due to the inability to control for childhood cognitive ability, which is a strong predictor of cognitive ability at later life [18]. The Medical Research Council (MRC) National Survey of Health and Development (NSHD, British 1946 birth cohort) is the oldest British birth cohort study [19] and measures psychological development, cognitive function, and lifestyle. Using this population, we investigated associations between midlife psychological well-being and women’s cognitive function in later life. We hypothesized that greater psychological well-being was significantly associated with better cognitive function. However, a key question is whether this association is adequately robust to control for childhood cognitive ability.
MATERIALS AND METHODS
Study design
The study used an observational longitudinal design.
Setting
The NSHD originally consisted of a socially stratified sample of 5,362 singleton children (girls: n = 2,547; boys: n = 2,815) born within marriage during one week in March in 1946 in mainland Britain [20]. The cohort has been followed up 23 times from birth to 69 years.
Participants
Participants for the present study were women 1) who responded to the questionnaire including the psychological well-being items at age 52 [21], and 2) who received a home visit from a research nurse and completed the assessment of cognitive function at age 69 [22]. A flow chart of sample extraction is presented in Fig. 1.
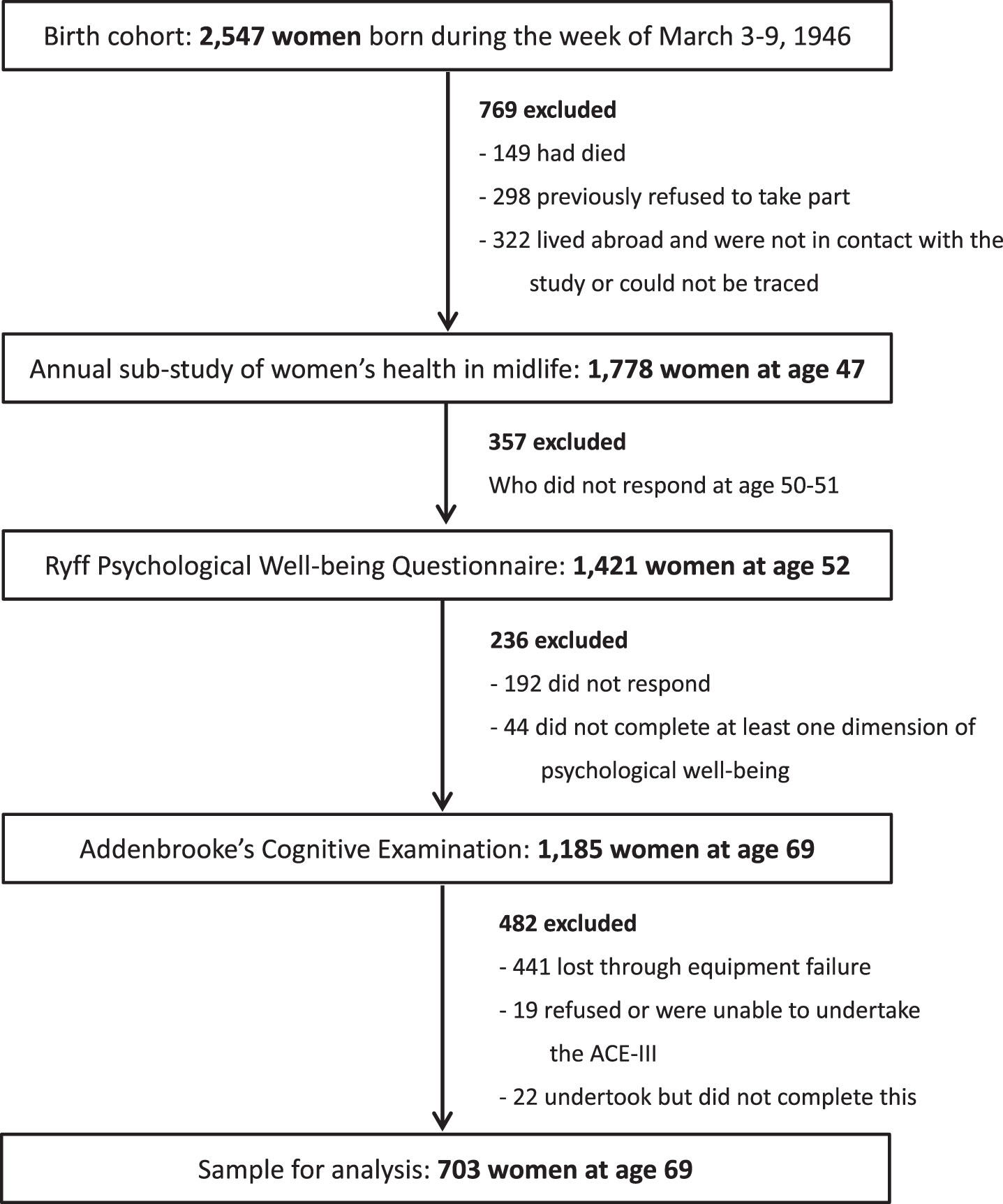
Flow chart of extraction of analytic sample.
The maximum sample in the analysis was 703, and these participants provided at least one dimension of psychological well-being at 52 years, undergoing an assessment of cognitive function at 69 years. We included all participants with any missing data on covariates.
Measurement
The main outcome variable was cognitive function at 69 years. Addenbrooke’s Cognitive Examination, Third Edition (ACE-III), was administered at home. The ACE-III is a cognitive screening battery commonly used in clinical practice to detect risk of Alzheimer’s disease and cognitive impairment [23]. It is scored across varying cognitive subdomains, with a maximum total score of 100. A higher score signifies better cognitive function. The ACE-III has been reported to have a good validity [24].
The main explanatory variable was psychological well-being at 52 years. This was assessed using a 42-item version of the Ryff Scales of Psychological Well-being. The scale includes seven questions within each of six dimensions: autonomy, environmental mastery, personal growth, positive relations with others, purpose in life, and self-acceptance. In total, 20 and 22 items are positively and negatively worded, respectively. The response format is six ordered levels labelled from ‘disagree strongly’ to ‘agree strongly’ [25]. Total scores for the dimensions range between 7 and 42, with higher scores indicating greater well-being. The Ryff Scales have a satisfactory validity [21]. Definitions of dimensions are described below [26]:
Autonomy: the respondent is self-determined and independent; able to resist social pressures to think and act in certain ways; regulates behavior from within; and evaluates self by personal standards.
Environmental mastery: the respondent has a sense of mastery and competence in managing their environment; controls a complex array of external activities; makes effective use of surrounding opportunities; and is able to choose or create contexts suitable to their personal needs and values.
Personal growth: the respondent has a feeling of continued development; sees self as growing and expanding; is open to new experiences; has a sense of realizing their potential; sees improvement in self and behavior over time; and is changing in ways that reflect most self-knowledge and effectiveness.
Positive relations with others: the respondent has warm, satisfying, trusting relationships with others; is concerned about the welfare of others; is capable of strong empathy, affection, and intimacy; and understands the give and take of human relationships.
Purpose in life: the respondent has goals in life and a sense of directedness; feels there is meaning to their present and past life; holds beliefs that give their life purpose; and has aims and objectives for living.
Self-acceptance: the respondent possesses a positive attitude toward the self; acknowledges and accepts multiple aspects of self, including good and bad qualities; and feels positive about past life.
To complement other domains in psychological well-being that are suggested to be associated with cognitive function in older adults, positive affect and life satisfaction measured at 60–64 years were also included in the study. Positive affect was measured using the Warwick-Edinburgh Mental Wellbeing Scale. All 14 items are positively worded and refer to feelings experienced over the past two weeks. Responses are scored from 1 to 5 points, and summed, with higher total scores representing greater positive affect [27]. Life satisfaction was measured using the Diener’s Satisfaction With Life Scale, containing five positively worded items, coded by a 7-point Likert scale. Total scores were calculated by summing the five items, with higher scores indicating greater life satisfaction [28].
Childhood cognitive ability at 8 years was used as a baseline measure, which was represented as the standardized sum of four tests of verbal and non-verbal ability devised by the National Foundation for Educational Research: reading comprehension, pronunciation, vocabulary, and non-verbal reasoning [29]. Childhood cognition was selected because it has been known to be a strong predictor of cognitive ability at later life, as well as level of education [18].
Other covariates included educational attainment by 26 years; occupational attainment (highest level of employment according to the UK Registrar General classification) and marital status by 53 years; and depression, smoking status, and level of physical exercise at 60–64 years. Covariate selection was based on the Lancet Commission review [4] and recent life-course studies in women [30, 31]. These variables were selected as they were included among nine modifiable risk factors of the review, and available measures from the NHSD cohort data. Depression, smoking status, and level of physical exercise were also assessed at 53 years in the cohort; however, variables at 60–64 years were used because they were suggested as risk factors in later life rather than midlife [4].
Educational attainment by 26 years was categorized as follows: no educational qualifications/vocational only (approximately 10 years), Ordinary level (11 years), Advanced level (13 years), and above/degree or equivalent (16 years). Occupational attainment by 53 years was classified into the following categories: professional/intermediate, skilled non-manual, or skilled manual/partly skilled/unskilled. Marital status at 53 years was categorized as single and never married, married, or divorced/widowed. Depression was measured using the 28-item General Health Questionnaire [32] at 60–64 years. This is a self-administered screening questionnaire for detecting recent (i.e., in the preceding few weeks) emotional symptoms. Each individual item is scored using a Likert scale ranging from 1 to 4, and the scores are recoded into binary values. The threshold score for potential common mental disorders in the current study was the sum of binary values of ≥6 (16.8% of the population) [33]. Affective symptoms are associated with memory problems in later life [34]. Smoking status at 60–64 years was defined as current smoker, ex-smoker, or lifelong non-smoker and corroborated via reports from younger ages. Regarding levels of physical exercise at 60–64 years, participants were asked how many times they had engaged in sports or vigorous activities during the preceding four weeks. Responses were classified as inactive (no episodes), less active (between one and four exercise episodes per month), or more active (five or more exercise episodes per month).
Statistical methods
Pairwise Pearson correlation coefficients were calculated for associations between dimensions of psychological well-being at 52 years. Pairwise Pearson correlations were also examined for associations between each covariate and psychological well-being. Linear regression analysis was conducted to assess the association between ACE-III scores at 69 years and psychological well-being at 52 or 60–64 years. The first model was a bivariate regression including only one independent variable. The second model adjusted for cognitive ability at 8 years. All other covariates were then included in a multiple model. The following categorical covariates were entered into the multiple model using dummy-coded variables: educational attainment by 26 years, occupational attainment and marital status by 53 years, smoking status, level of physical activity, and presence of depression at 60–64 years. As there were moderate correlations between dimensions of psychological well-being, each dimension was entered into the model separately. R-square was calculated as a measure for goodness of fit in the model with all covariates. The effect size was calculated with Cohen’s f2 for each dimension of psychological well-being. The effect size is small if the value of f2 varies around 0.02, medium if f2 varies around 0.15, and large if f2 varies around 0.35 [35]. In the regression analysis, full information maximum likelihood was used to estimate missing data [36]. A sensitivity analysis was employed using the multiple model where the dependent variable was each sub-domain of ACE-III instead of total score. Another sensitivity analysis in the multiple model was conducted where participants with mild cognitive impairment at 69 years were excluded from the sample. A validated cut-off score of 82 or below in the ACE-III total score [37] was used as an indicator of mild cognitive impairment (44 participants).
Stata 15.1 (StataCorp, Texas) was used to perform all analyses. All tests were two-tailed and significance level was set to 5%.
Ethics
Ethical approval for the study was obtained from the Greater Manchester Local Research Ethics Committee and the Scotland A Research Ethics Committee. Written, informed consent was obtained from study members at each wave of data collection. All procedures involving experiments on human subjects are done in accord with the Helsinki Declaration of 1975.
RESULTS
Compared to the 1,844 people excluded from the analysis, the 703 participants included in the present study had higher educational attainment by 26 years (χ2(2) = 93.69, p < 0.001) and occupational attainment by 53 years (χ2(2) = 51.86, p < 0.001), included fewer smokers (χ2(2) = 9.32, p = 0.009) and higher levels of physical exercise (χ2(2) = 11.22, p = 0.004) at 60–64 years. There was no significant difference in childhood cognitive ability, marital status at 53 years, or prevalence of depression at 60–64 years.
Complete ACE-III and psychological well-being data were collected for 703 participants. Participant characteristics and the mean scores for psychological well-being are shown in Table 1. Missing data was frequent in the Diener and WEMWBS measures; there were 316 participants who had at least one missing item in these variables.
Characteristics of study participants
SD, standard deviation. Cognitive ability at 8 years was represented as the standardized sum of four tests of verbal and non-verbal ability devised by the National Foundation for Educational Research: reading comprehension, pronunciation, vocabulary, and non-verbal reasoning. *Presence of depression was measured as total score of ≥6 in the 28-item General Health Questionnaire. Domains of psychological well-being at 52 years were measured using the Ryff Scales of Psychological Well-being. Positive affect at 60–64 years was measured using Warwick-Edinburgh Mental Wellbeing Scale. Life satisfaction at 60–64 years were measured using the Diener Satisfaction with Life Scale.
The total mean ACE-III score at 69 years was 92.3, ranging from 0 to 100 (SD = 5.7). The mean scores for sub-domains are displayed in Table 2.
ACE-III scores at 69 years
ACE-III, Addenbrooke’s Cognitive Examination (3rd version); SD, standard deviation.
There were weak (0.20–0.39) or moderate (0.40–0.59) correlations between all pairs from the six dimensions of psychological well-being at 53 years (range of Pearson correlation coefficients: 0.20 to 0.61).
There were weak correlations between each covariate and psychological well-being (Supplementary Table 1). The presence of depression at 60–64 years was weakly correlated with lower environmental mastery, lower positive affect, and greater life satisfaction of psychological well-being. Greater occupational attainment by 53 years was weakly correlated with higher personal growth and purpose in life. All other pairwise correlation coefficients were small, ranging from –0.16 to 0.17.
The results of the multiple linear regression analysis are presented in Table 3. In a bivariate multiple regression, lower environmental mastery, greater personal growth, greater purpose in life, and lower self-acceptance at 52 years were significantly associated with higher ACE-III total scores at 69 years. After adjusting for cognitive ability at 8 years, the association with environmental mastery and purpose in life became non-significant. The association with personal growth and self-acceptance remained significant at the 5% level after accounting for other covariates. Positive affect and life satisfaction at 60–64 years did not show significant associations with the ACE-III total scores in any of the adjusted models. Effect size of each dimension of psychological well-being was small, and less than 0.02.
Associations between psychological well-being dimensions at 52 years or 60–64 years and ACE-III at 69 years
N = 703; full information maximum likelihood estimation was used. ACE-III, Addenbrooke’s Cognitive Examination (3rd version), total score out of 100. CI, confidence interval. Domains of psychological well-being at 52 years were measured using the Ryff Scales of Psychological Well-being. Positive affect at 60–64 years was measured using Warwick-Edinburgh Mental Wellbeing Scale. Life satisfaction at 60–64 years were measured using the Diener Satisfaction with Life Scale. *Cognition at 8 years was measured using tests of verbal and nonverbal function. †Cognition at 8 years, educational attainment by 26 years, occupational attainment and marital status by 53 years, smoking status, physical activity, depression at 60–64 years.
In a sensitivity analysis where each sub-domain of ACE-III was entered as a dependent variable, greater personal growth was significantly associated with better verbal fluency (Supplementary Table 2). Lower self-acceptance was significantly associated with better attention and orientation, and memory (Supplementary Table 3).
The association of ACE-III total score with personal growth were non-significant (B = 0.04, 95% CI [–0.01, 0.09]) in the sensitivity analysis in which 44 participants with mild cognitive impairment were excluded from the sample. The association with self-acceptance remained significant (B = –0.07, 95% CI [–0.13, –0.02]) in this analysis.
DISCUSSION
In a large representative British population cohort, while most scales of the Ryff Scales of Psychological Well-being at 52 years were not associated with cognition in women at age 69, greater personal growth and lower self-acceptance were associated with higher scores for this outcome. These associations remained significant after controlling for childhood cognition, educational attainment by 26 years, occupational attainment and marital status by 53 years, and case-level emotional symptoms, smoking, and physical activity at 60–64 years. These findings suggest that this aspect of midlife psychological well-being contributes to women’s cognitive retention in later life.
This was the first study to demonstrate an association between midlife psychological well-being and cognitive function in later life in women in a general population-based study. Individuals could experience identity crises when faced with losses in health and independence [38]. Personal growth involves a sense of continued development, self-improvement, the use of personal talents, and the fulfilment of potential [39]. Moreover, people with a sense of personal growth tend to be open to new experiences and change in ways that reflect self-knowledge and effectiveness. It has been suggested that women’s personal growth helps them to negotiate stressful life events in old age [40] and manage the functional decline that accompanies aging [41]. Therefore, midlife personal growth could help women to adapt to change in later life and lead to resilience to cognitive aging. However, it should be noted that magnitude of the effect sizes found in this study was small even for personal growth. A sensitivity analysis showed that the association with personal growth was non-significant for all ACE-III sub-domains except verbal fluency, and after participants with mild cognitive impairment were excluded from the sample. There may have been confounders not included in the present study, such as personal traits. Midlife personal growth could represent a lifelong personality orientation that contributes to cognitive capacity from childhood. Specific personal traits such as high neuroticism, low openness, low conscientiousness, and extraversion are relevant to cognitive decline, and could influence the capacity for personal growth [42–44].
Purpose in life, which has been associated with reduced risk of dementia in past literature [14–17], was not associated with cognitive function in the present study. Using NSHD data enabled us to adjust for childhood cognitive ability in the analysis, may have accounted for this discrepancy. The significant association between lower self-acceptance and better cognitive ability in the present study is also surprising because higher self-acceptance has been linked with greater psychological resilience among women [41]. The results may have been influenced by the interaction with personal traits that are associated with high self-acceptance [45]. High self-acceptance is also linked with helping of others among women [46], so lower self-acceptance may have interfered with caring roles and occupational attainment. Care of ill or disabled family members is typically performed by women in midlife [47], and caring for older parents with dementia often needs to be balanced with the competing demands of employment and caring for children [5]. Women who work and care for someone with dementia often face negative effects on their careers, such as change from working full time to part time, taking a leave of absence from work, or job loss [48]. Future research should examine the pathway between personal traits, midlife psychological well-being, caring role in family, and cognitive function among women in older age.
Strengths and limitations of the study
The strengths of this study include the prospectively obtained measures of well-being and cognitive function in a general population-based sample. Other strengths include the use of an extensive and comprehensive measure of cognitive function (ACE-III) as an outcome variable. However, the study was subject to some limitations. Midlife psychological well-being was assessed only in women who had completed at least one annual sub-study in the preceding two years; therefore, the number of active women participating in the study could have been higher relative to that of those who had been excluded, and the association between psychological well-being and cognitive ability could have been underestimated. Because score precision of the Ryff Scales of Psychological Well-being decreased at higher levels [49], the association with cognitive ability might have been limited by the fact that scale scores were all above the mid-point. The analytic sample also had higher educational attainment compared to those excluded. Since educational attainment is an important influence on cognitive function, this sample bias should be carefully considered with regard to the generalizability of results to women in the general population. Due to childrearing responsibilities, some participants may have deferred their educational goals to after age 26. Educational attainment by age 26 may be an underestimate of women’s actual education levels. Our study did not include related attributes for women such as high homocysteine [50]. We did not adopt corrections for multiple testing as this has been controversial in epidemiological studies [51, 52]. Nonetheless it should be noted that our results may be subject to potential type I error. Furthermore, 69 years remains a young age for the assessment of cognitive ability in dementia, as dementia prevalence is 2% in people aged between 65 and 69 years in the UK [53]. It will therefore be valuable to conduct a follow-up study up at an older age.
Conclusions
Greater personal growth and lower self-acceptance at 52 years were associated with higher cognitive ability at 69 years in women. As personal growth represents the ability to change in ways that reflect self-knowledge and effectiveness, it may contribute to women’s cognitive preservation in later life. Future research should examine pathways between personal traits, midlife psychological well-being, role in caring family, and cognitive function in older age among women.
Footnotes
ACKNOWLEDGMENTS
This research was funded by the Grant-in-Aid for Scientific Research on Innovative Areas from the Ministry of Education, Culture, Sports, Science, and Technology of Japan, Grant Number: JP16H06395; and the JSPS KAKENHI through a Grant-in-Aid for Young Scientists (B), Grant Number: JP15K20796. The funding source played no role in the study design; data collection, analysis, or interpretation; or writing the report.