
Abstract
The QTc interval is the electrocardiographic manifestation of ventricular depolarization and repolarization. This marker is often prolonged in acute and chronic neurological conditions. The cause of the cerebrogenic QT prolongation remains unclear. The aim of the study was to analyze the relation between QTc interval and the degree of cognitive impairment and structural brain imaging changes in patients with dementia and mild cognitive impairment (MCI). To this aim, 269 patients were screened, of whom 61 met one or more exclusion criteria. The remaining 208 patients (56 control subjects, 44 patients with MCI, and 108 with dementia) were recruited. Eighty-five patients using drugs causing prolongation of QT interval were further excluded. The QT interval was measured manually in all 12 leads by a single blinded observer, assuming the longest QT value adjusted for heart rate by using the Bazett’s formula. All patients underwent a structural brain imaging and the following measures were obtained: the bicaudate ratio and the periventricular hyperintensity and deep white matter hyperintensity using the modified Fazekas scale. Prolonged QTc interval was prevalent in 1) patients with dementia, especially in those with moderate-severe degree; 2) subjects with impairment of praxis and attention, low functional status, and behavioral symptoms; 3) patients with global and temporal atrophy and with higher scores on the Fazekas or leukoaraiosis scales. Degenerative and vascular processes might play a main role in QTc interval prolongation because of the damage to brain areas involved in the control of the autonomic cardiac nervous system.
INTRODUCTION
The cortical control of sympathetic and parasympathetic autonomic functions, including cardiac rate and rhythm, is regulated across a neural network integrated within the anterior insula and cingulate cortex. The QT interval, representing the surface electrocardiographic measure of ventricular depolarization and repolarization, and the QT interval corrected for heart rate (QTc) are often prolonged in acute neurological conditions, such as subarachnoid hemorrhage (42%) [1] and ischemic stroke, as well as in a number of chronic conditions [2]. The cause for acute cerebrogenic QT prolongation remains largely unclear, although a major role of insular cortex has been proposed [3, 4]. In addition to acute conditions, autonomic cardiac dysfunction is common and well documented in distinct neurodegenerative diseases, such as dementia with Lewy bodies [5]. In other conditions including Alzheimer’s disease (AD), vascular and frontotemporal dementias, the results of previous reports are controversial and the underlying pathogenetic mechanisms inducing cardiac dysfunction remain largely unknown [6]. The main indexes, commonly used to evaluate the autonomic cardiac system are heart rate variability [7], Ewing’s Battery tests [8], and metaiodobenzylguanidine (123-ImIBG) cardiac scintigraphy, the latter being used for diagnostic purposes in patients with α-synucleinopathy [9]. Only two studies to date have analyzed the role of QT interval in patients with dementia [10, 11]. Both studies have demonstrated QT dispersion (QTD) mean values significantly higher in patients with AD compared to subjects with mild cognitive impairment (MCI) and healthy controls. In addition, QTD was found to be correlated with the degree of cognitive impairment.
The aim of the present study was to analyze the degree of QT interval prolongation in patients with dementia and MCI, evaluating the relationship between this electrocardiographic index and the degree of cognitive impairment assessed by neuropsychological testing and the structural brain imaging changes.
MATERIALS AND METHODS
All consecutive subjects who were seen at the outpatient Cognitive Impairment and Dementia Center of the University Hospital of Verona from January to December 2015 were retrospectively evaluated.
The study was conducted in accordance with local clinical research regulations. All data were collected by electronic medical records.
Patients routinely had medical, neurological, and neuropsychological evaluations, in addition to blood tests (full blood count, clotting, CRP, ESR, liver, renal and thyroid function, electrolytes, vitamin B12, vitamin D, folic acid, homocysteine).
The cognitive evaluation was done using Mini-Mental State Examination (MMSE) [12] and specific extended cognitive testing investigating higher cortical functions, including attention (Multiple Features Target Cancellation [13]; Trail Making Test, Part A and Part B [14]), phonemic and semantic fluency [15], constructional praxis (freehand copy of drawings; coping drawings with landmarks) [16], memory (digit span forward, digit span backward; Rey Auditory Verbal Learning Test) [16, 17], executive functions (Frontal Assessment Battery; clock drawing test; Stroop test) [18–20] performed by trained neuropsychologists.
The diagnosis of MCI was done according to Mayo Clinic criteria [21]. Patients were classified according to the score on MMSE as mild dementia (score 21–24) or moderate-severe dementia (score 10–19). Controls were subjects without diagnosis of cognitive impairment according to used criteria.
Daily function and functional independence were assessed using the 6-item version of the Activities of Daily Living (ADL) Scale [22], which evaluates independence or dependence in bathing, dressing, toileting, transfer, continence, and feeding, and the 8-item version of the Instrumental ADL (IADL) Scale [23], which refers to using the telephone, shopping, food preparation, housekeeping, laundry, use of transportation, taking medications, and ability to handle finances. For ADL, the degree of dependence was scored from 0 (none) to 6 (dependence in all activities) and graded as severe (>5), moderate (3 to 4), or mild (1 to 2). For IADL, the range was 0-to-5 or 0-to-8, depending on the exclusion of individual not applicable tasks (laundry, housekeeping, food preparation) and the degree of dependence was categorized as severe (6 to 8/8 or 4/5), moderate (3 to 5/8 or 2 to 3/5), or mild (1 to 2/8 or 1/5).
Assessment of dementia-related neuropsychiatric symptoms was performed with the use of the Neuropsychiatric Inventory [24], whereas depressive symptoms were scored with the Geriatric Depression Scale [25].
At first visit, a 12-leads electrocardiogram (ECG) was obtained in all subjects.
The QT interval was measured manually by a trained physician blinded to the participants status, in all 12 leads, from the beginning of the QRS complex to the end of the T wave, paying great attention to exclude the U waves unless they appeared to merge with the T waves. The leads showing the longest QT value were assumed to be the most reliable for clinical purposes. For the analyses, we stratified the patients into two groups based on the widely accepted values for normal, borderline, and prolonged QTc in relation to age and sex categories, by using the Bazett’s formula. The QTc interval was defined: normal if less than 430 ms (men) and 450 ms (women); borderline for values between 430 and 450 ms for men and 450 and 470 ms for women; prolonged if greater than 450 ms (men) and 470 ms (women) [26]. An altered QTc interval, by using the Bazett’s formula, was defined as longer than 430 ms for men and 450 ms for women.
A structural brain imaging study was performed in all patients, using computed tomography (CT) or magnetic resonance imaging (MRI), included T1-weighted or fluid-attenuated inversion recovery (FLAIR) images. Imaging data were analyzed by a neurologist who was trained by a neuroradiologist with expertise on neurodegenerative disease imaging.
Estimates of total brain atrophy were computed on axially acquired CT and MRI images by using the bicaudate ratio, i.e., the ratio of the minimum intercaudate distance to that of the inner skull along the same line [27, 28]. A pathological value was considered longer than or equal to 0.15 [29].
Temporal lobe atrophy was assessed by a qualitative analysis evaluating if the atrophy was present or absent by a neurologist who was trained by a neuroradiologist with expertise on neurodegenerative disease imaging.
White matter disease on MRI was rated and graded as periventricular hyperintensity (PVH) and deep white matter hyperintensity (DWMH) using the modified Fazekas scale [30].
The PVH severity was graded as follows: 0 = absent, 1 = cap or pencil-thin lining, 2 = smooth halo, and 3 = irregular PVH extending into the deep white matter. The DWMH severity was rated as follows: 0 = absence, 1 = punctuate foci, 2 = beginning confluence of foci, 3 = large confluent areas. White matter disease was assessed analyzing CT images as follows: 0 = absent; 1 = one lesion; 2 = more lesions; 3 = confluent lesions. In the present study, only MRI or CT graded 2 or 3 were considered pathological.
Exclusion criteria were: 1) history, symptoms or physical findings suggestive of cardiac disease and/or heart failure 2) congenital long-QT syndrome; 3) cardiac pacing; 4) complete bundle branch blocks; 5) electrolyte imbalances. The statistical analysis was first performed on data obtained from all patients fulfilling exclusion criteria (N = 208) and, to the aim of the study, in the group of subjects fulfilling exclusion criteria and not exposed to QT-prolonging medications (N = 123).
The primary endpoint was to investigate the prevalence of prolonged QTc interval in patients with cognitive impairment.
The secondary endpoints were to analyze the relationship between increased QTc interval and 1) cognitive impairment assessed by neuropsychological examination; 2) degenerative and vascular load evaluated by MRI or CT.
Statistical methods
Data are reported as mean and standard deviation (SD) or as absolute values and percentages as appropriate. Continuous variables were compared using the Student’s t-test or Mann-Whitney and categorical variables were compared using chi-squared or Fisher test. A probability value of less than or equal to 5% was considered significant. Correlations between MMSE score and cardiac parameters were assessed by logistic regression analysis and logistic regression adjusted for age and sex. Statistical analyses were conducted using SPSS software (SPSS v20, Chicago, IL, USA).
RESULTS
From January to December 2015, we screened 269 patients, of whom 61 met one or more exclusion criteria (severe cardiomyopathy with NYHA III or IV: 3 pts; cardiac pacing: 6 pts; complete bundle branch blocks: 30 pts; electrolyte imbalances: 6 pts; missing data: 16 pts). The remaining 208 patients (56 control subjects, 44 patients with MCI and 108 with dementia) were recruited and included in the statistical analysis. Eighty-five patients using one or more drugs causing prolongation of QT interval were further excluded (antiarrhythmics: 9 pts; antidepressants: 71 pts; antipsychotics: 37 pts; donepezil: 3 pts; rivastigmine: 6 pts).
Among patients with dementia, the following types were included: 27 AD, 5 frontotemporal dementia, 5 dementia-Parkinson complex, 19 vascular dementia, 1 normotensive hydrocephalus, 1 Lewy body dementia, 21 mixed dementia (vascular dementia and AD), and 29 other neurological conditions.
Clinical characteristics of the subgroups of patients are shown in Table 1. Among patients with dementia, mean age (p≤0.001) and disease duration (p = 0.001) were higher than in the other groups; other neurological diseases were significantly higher in the control and in the MCI groups than dementia category (p = 0.009); in the dementia group the female gender was more prevalent (p = 0.03).
Clinical and epidemiological features of patients
MCI, mild cognitive impairment.
In patients with dementia, the mean QTc interval was significantly greater than in the MCI group (dementia 441±29.55 ms versus MCI 425±24.55 ms; p = 0.003) and in the control group (dementia 441±29.55 ms versus control 424±18.78 ms; p≤0.001) (Fig. 1; Table 2). In addition, and compared to patients with MCI and controls, patients with dementia had a significantly higher prevalence of prolonged (controls 2%, MCI 11%, dementia 30%, p≤0.001) and altered QTc values (controls 23%, MCI 27%, dementia 59%, p≤0.001) (Figs. 2 and 3; Table 2). Within the dementia group the prevalence of altered QTc was higher in subjects with moderate-severe dementia than in those with mild dementia (60.5% versus 31.2% respectively, p≤0.001).
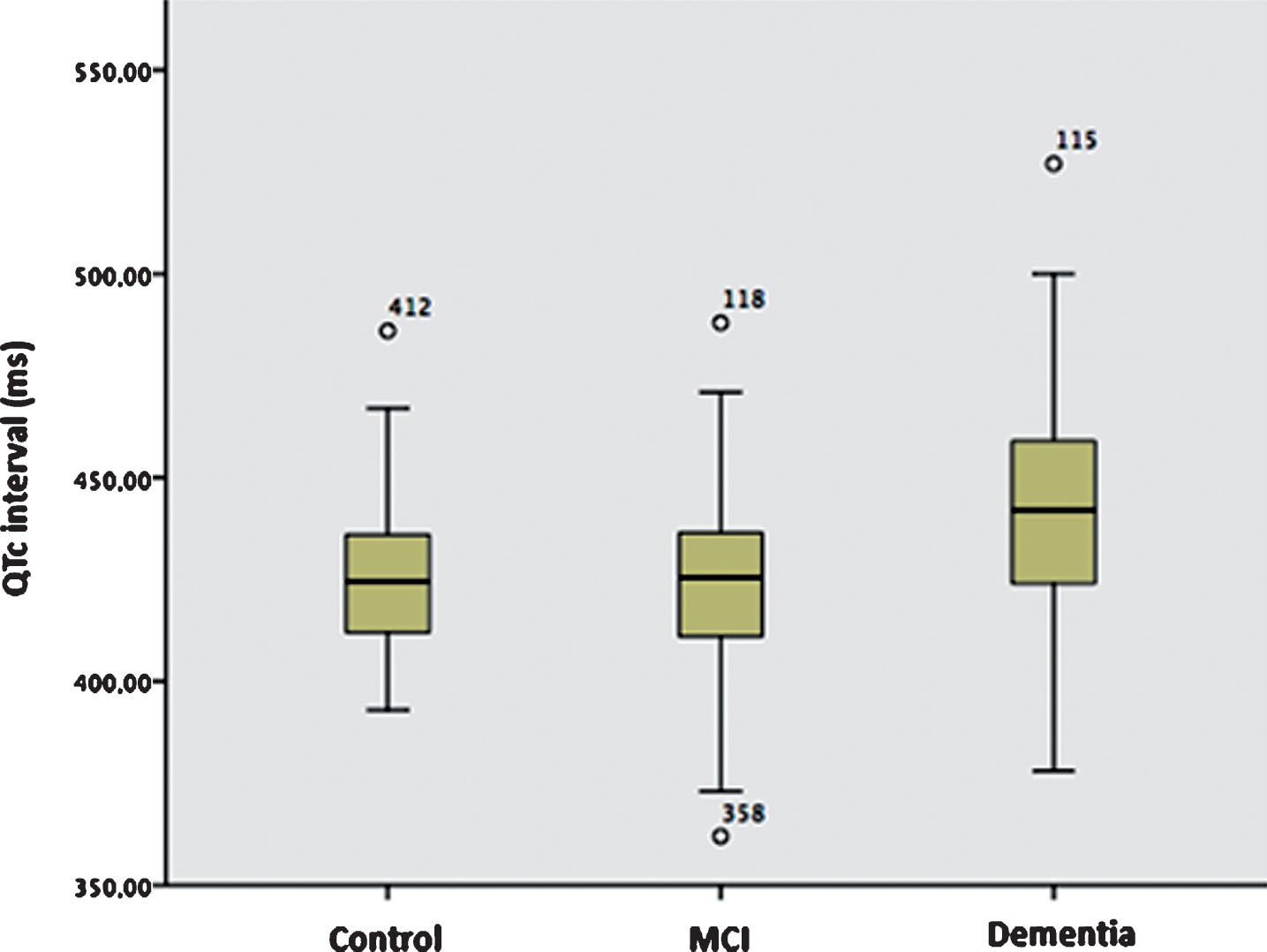
Mean QTc values in control group, mild cognitive impairment, and patients with dementia. As the figure shows, in the dementia group the mean QTc was significantly higher compared with the MCI group (p = 0.003) and the control group (p≤0.001).
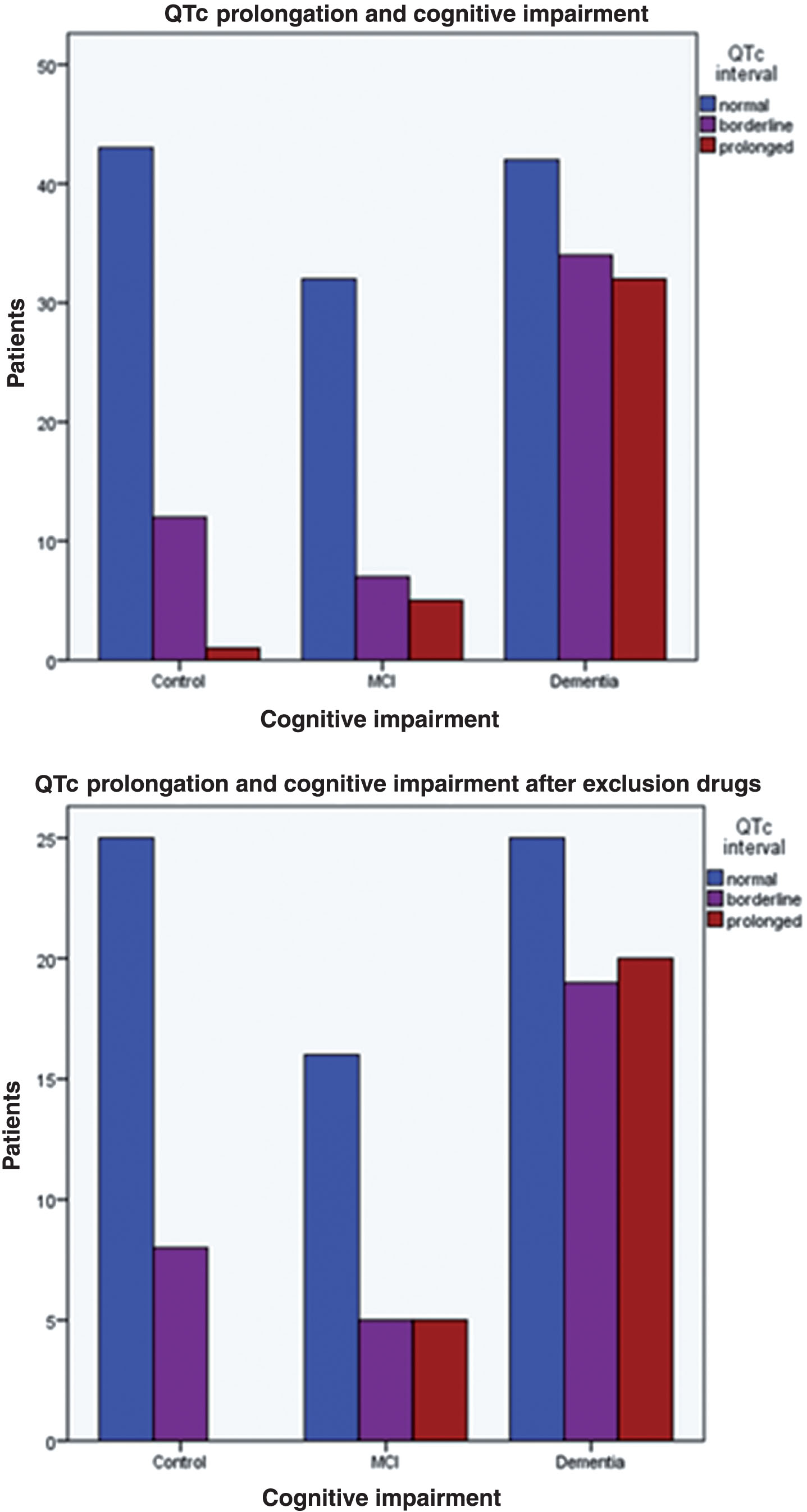
The prevalence of QTc interval prolongation in controls, mild cognitive impairment, and dementia before exclusion drugs (p≤0.001) and after exclusion drugs (p≤0.001).
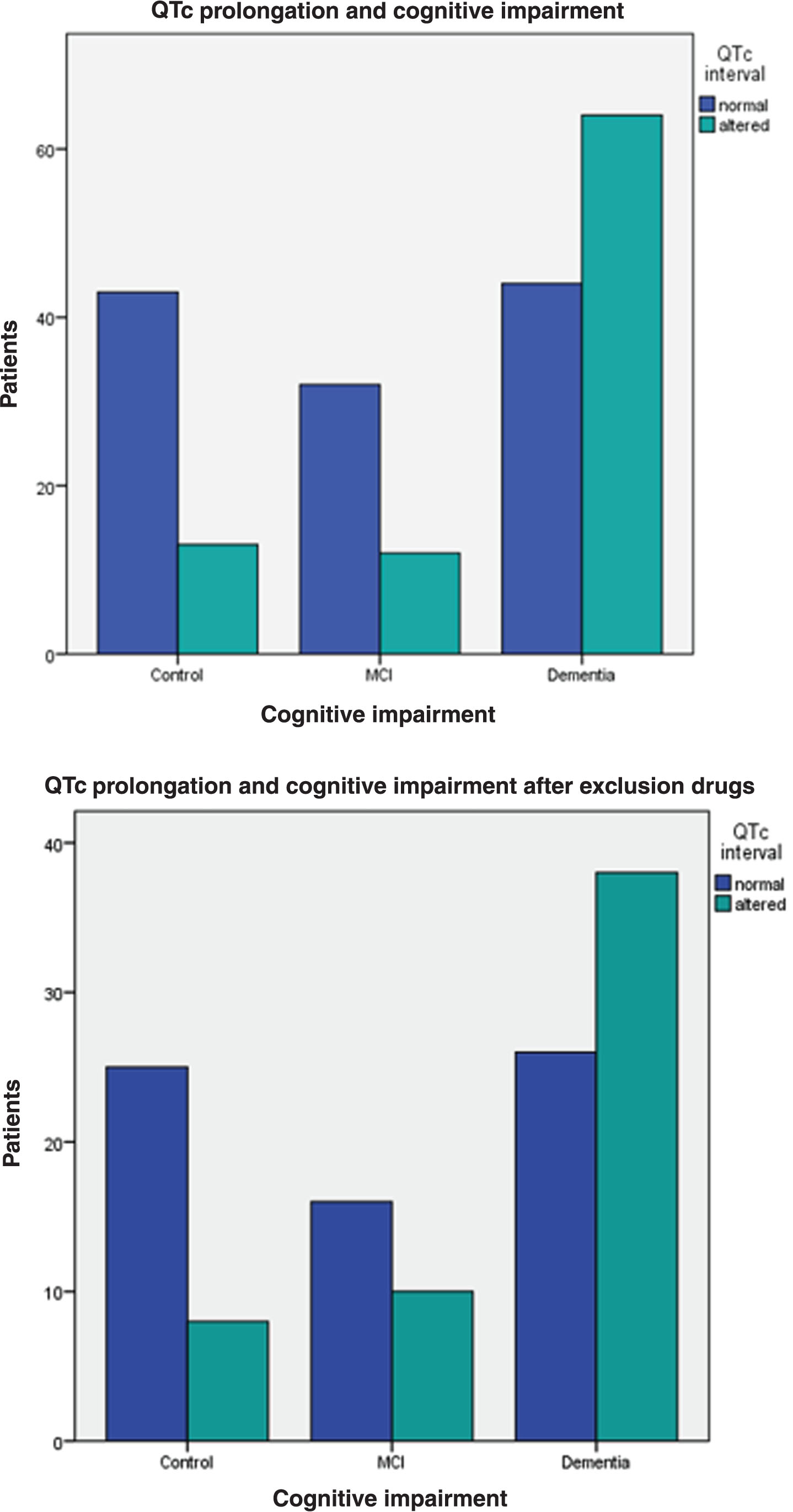
The prevalence of QTc interval alteration in controls, mild cognitive impairment, and dementia before exclusion drugs (p≤0.001) and after exclusion drugs (p≤0.001).
QTc interval in different groups studied
†Denotes subjects not taking QT-prolonging drugs.
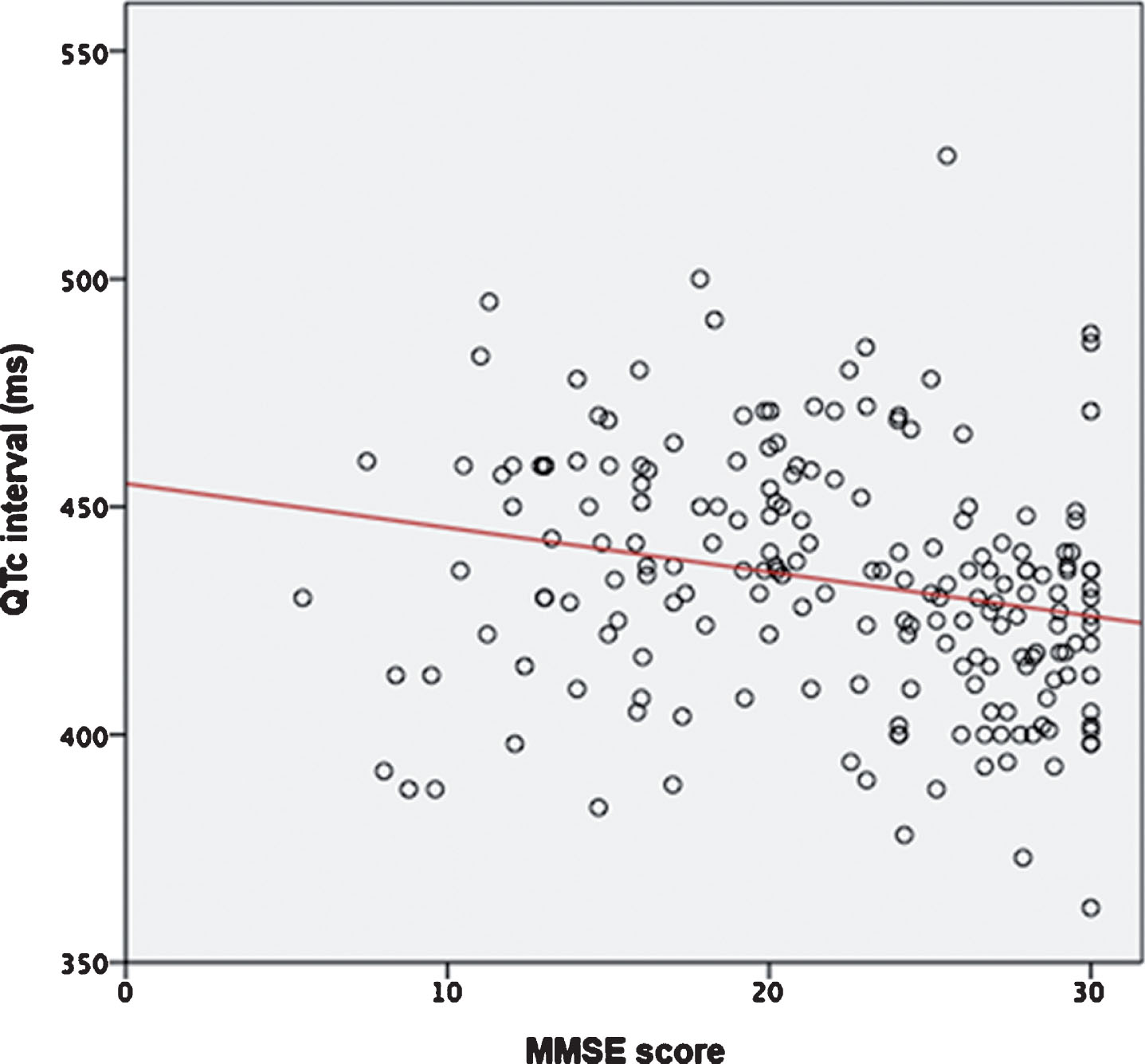
As to the neuropsychological scores, a significant correlation was found between QTc interval and both raw MMSE (p≤0.001, R = 0.26; age/sex-sted p = 0.001, R = 0.11) (Fig. 4; Table 3) and corrected MMSE (p = 0.001, R = 0.23; age/sex-sted p = 0.004, R = 0.10) (Fig. 5; Table 3). The prevalence of prolonged QTc was significantly higher in patients with impairment of attention and praxis (54.5% versus 29.2%, p = 0.02 and 55.3% versus 30.2%, p = 0.003, respectively) compared with other higher cortical functions investigated during neuropsychological examination. In addition, the QTc main value was also significantly higher in patients with deficit of attention (436.14±27.28 ms versus 427.20±23.34 ms, p = 0.035), praxis (438.36±24.56 ms versus 426.70±24.31 ms, p = 0.007), memory (434.04±26.89 ms versus 425.40±20.90 ms, p = 0.030), and executive functions (434.31±28.71 ms versus 426.05±19.47 ms, p = 0.057).
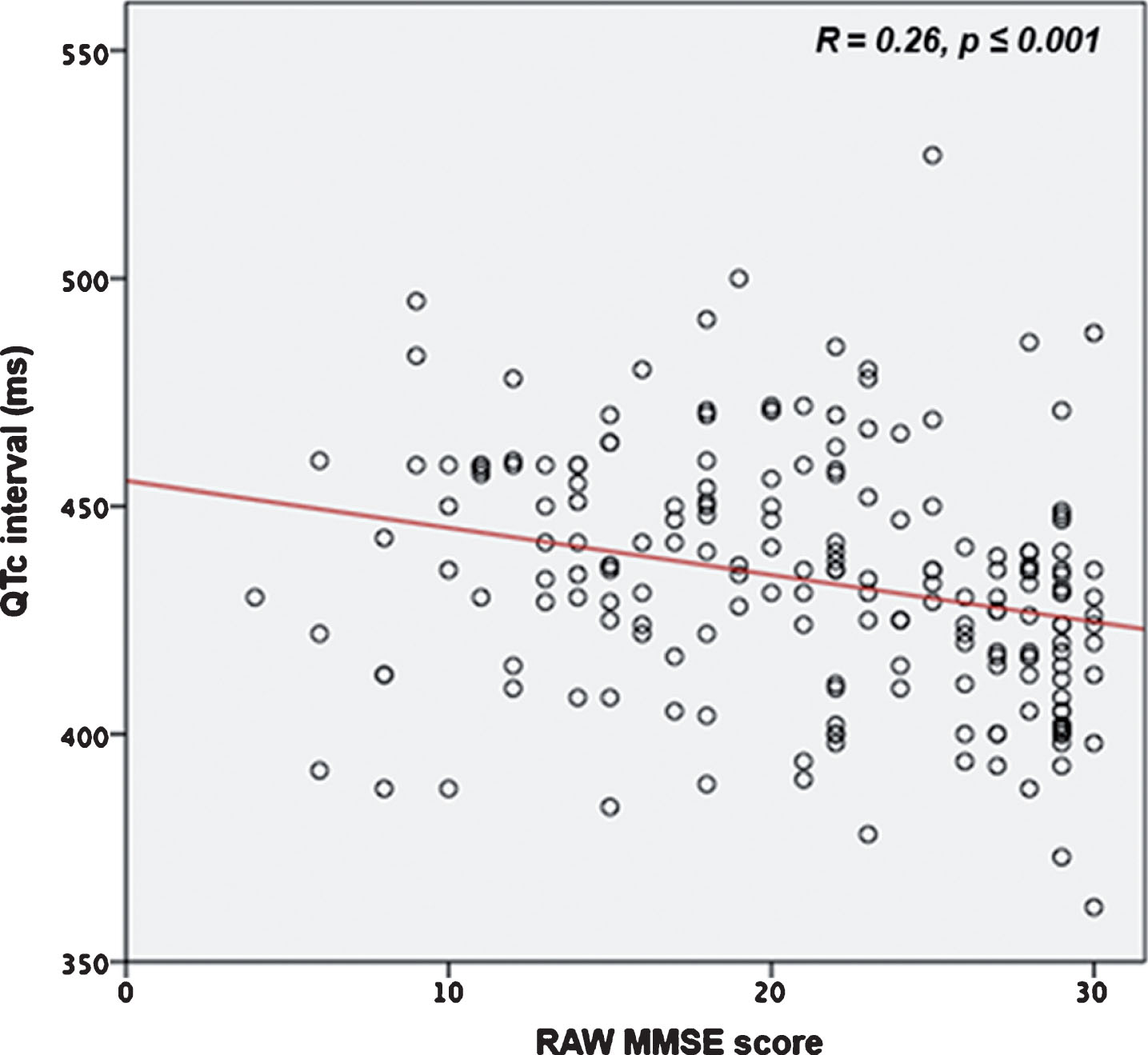
The correlation between raw MMSE and QTc (R = 0.26, p≤0.001).
The correlation between correct MMSE and QTc (R = 0.23, p = 0.001).
QTc interval and MMSE score
†Adjusted for age and sex.
In terms of functional status, the prevalence of altered QTc interval was higher in patients with severe and moderate disability assessed with ADL than in patients with mild disability (60.5% and 66.7% versus 34.9%, p = 0.002). Furthermore, the QTc mean value was longer in patients with severe (441.10±27.29 ms versus 430.20±25.24 ms, p = 0.023) and moderate disability (444.44±28.25 ms versus 430.20±25.24 ms, p = 0.029) than in patients with mild disability. Patients with severe disability assessed with IADL had a prevalence of prolonged QTc and a mean QTc value significantly higher than those with moderate or mild disability (respectively: 64.34% versus 37.70% and 32.9%, p = 0.001; 444.14±28.08 ms versus 429.85±26.71 ms, p = 0.013 and 444.14±28.08 ms versus 428.31±23.36 ms, p≤0.001). The prevalence of impaired QTc interval was higher in patients with behavioral and psychiatric symptoms of dementia (BPSD; 57.1% versus 34.8%, p = 0.034) and QTc mean value was also significantly longer in these patients (439.55±26.53 ms versus 430.85±23.76 ms, p = 0.033).
The analysis of brain imaging showed that patients with pathological bicaudate ratio had a higher prevalence of altered QTc and a longer mean QTc value than those with a normal ratio (respectively: 47.8% versus 22.2%, p = 0.011; 435.85±27.75 ms versus 423.03±21.51 ms, p = 0.024). Similarly, patients with temporal lobe atrophy had a higher prevalence of prolonged QTc and a longer mean QTc value compared with patients without atrophy (respectively: 47.7% versus 25.0%, p = 0.029; 436.49±26.48 ms versus 420.20±25.28 ms, p = 0.005).
Moreover, the prevalence of alterations of QTc interval was higher in patients with Fazekas grade 2 and 3 than patients with Fazekas grade 0 and 1 (51.1% versus 26.8%, p = 0.011). In addition, the mean QTc was longer in patients with pathological Fazekas score (438.66±29.20 ms versus 424.87±26.57 ms, p = 0.015). Similarly, patients with pathological leukoaraiosis (grade 2 and 3) had a higher prevalence of impaired QTc (53.0% versus 47.0%, p = 0.040) and a longer mean QTc interval compared with those without leukoaraiosis (439.18±26.82 ms versus 422.16±28.59 ms, p = 0.014).
The results remained consistent after exclusion of patients taking QT-prolonging drugs (Tables 2 and 3).
DISCUSSION
The main findings of the present investigation were that prolonged QTc interval was prevalent in 1) patients with dementia, especially in those with moderate-severe degree; 2) subjects with impairment of praxis and attention, low functional status and BPSD; and 3) patients with global and temporal atrophy and with higher scores on the Fazekas or leukoaraiosis scales.
To date, only two studies have found longer QTD values in patients with AD compared with those presenting MCI and controls. In addition, QTD was significantly associated with the severity of cognitive impairment [10, 11]. In neurological diseases, the QTc interval prolongation is not a mere indicator of arrhythmogenicity, but also an important marker of cerebral damage, according to previous reports [31]. It has been hypothesized that it might be the result of a sympathetic overexcitation mediated through the insular cortex. The prolongation of QTc interval in patients with dementia might represent a further demonstration of an impairment of the higher central autonomic regions, as previously described using other markers as the abnormality of the heart rate variability, especially in AD [32, 33].
In patients with dementia, chronic or occasional hypotensive episodes induced by neurovascular instability have been well demonstrated [34] and correlated with the severity of cognitive disorder [35, 36]. In addition, it has been shown that cerebral hypoperfusion occurs and contributes to development and progression of dementia by affecting more vulnerable brain regions, such as hippocampus and amygdala, brain areas involved in central autonomic control [37], and also regulating QTc interval. Therefore, patients with a lower cognitive performance assessed with MMSE score have higher probability to have QTc prolongation.
In terms of cortical functions, attention and praxis were associated with a higher prevalence of prolonged QTc interval. Attention is regulated by the dorsolateral prefrontal circuit and prefrontal circuit orbitolateral without a specific lateralization; praxis is mainly controlled by the frontal and parietal lobes but also by the temporal and occipital ones, with a left predominance [38]. The insular cortex plays a central role in the regulation of the heart–brain axis and is connected both with frontal and temporal lobe [39]. Accordingly, we may speculate the alteration of QTc interval might be the expression of the cerebral damage induced by the lesion of these brain areas.
Since the insular cortex is connected with the limbic area, mostly with the amygdala and the anterior cingulate cortex, we may hypothesize that patients with BPSD exhibit also a dysfunction of the autonomic nervous system for the involvement of this network. Moreover, patients with a less functional autonomy assessed by ADL and IADL had a greater degree of cognitive impairment and, therefore, a higher prevalence of impaired QTc.
Brain imaging data obtained by MRI and CT revealed a relationship between the extent of the degenerative process and/or the cerebral vascular load and the QTc prolongation. As the bicaudate ratio is commonly deemed a reliable index of global atrophy, it might be hypothesized that patients with a higher degenerative damage have a greater impairment of the cerebral autonomic network reflected by the prolongation of QTc. Furthermore, the greater prevalence of altered QTc interval in patients with AD may be explained by the temporal lobe atrophy with insular cortex involvement. Cerebral vascular load seems to be associated with a prolongation of QTc. Patients with mixed dementia, in addition to lesions in autonomic cardiac centers, might have an alteration of vascular origin which determines a blood pressure instability with subsequent dysfunction of the cerebral perfusion [40]. It has also been shown that patients with diabetes mellitus and vascular dementia have an important dysfunction of the autonomic nervous system with a reduction in parasympathetic activity and an increase in sympathetic function [41]. Taken together, the cerebral hypoperfusion might be responsible for both cognitive impairment and autonomic dysfunction control.
In the present study, the results remained unchanged after exclusion of patients taking prolonging-QT drugs. This finding suggest that the degenerative-vascular process might play a main role in influencing QTc interval because of the damage of the cerebral areas involved in the control of the autonomic cardiac nervous system.
Limitations
The single-center and retrospective design represents a potential limitation of this study. The sample size is relatively small, and the findings of our study should be confirmed by larger prospective trials.
Furthermore, as a consequence of the retrospectivity of the study, some ECGs were not performed during the first patient evaluation at the Cognitive Impairment and Dementia Center, but at different times. However, we have considered ECGs done within few months of the first evaluation.
Other limitations include the presence of CT and MRI data, and the retrospective design.
Conclusion
In the present study, the rate of prolonged QTc interval was longer in patients with more severe dementia, less functional autonomy, and with BPSD. Moreover, the cerebral global and temporal atrophy and the cerebral vascular load seem to be associated with a higher prevalence of QTc prolongation. This finding suggest that the degenerative-vascular process might play a main role in influencing QTc interval because of the damage of the brain areas involved in the control of the autonomic cardiac nervous system.
Further research is needed to elucidate the pathophysiology of cerebrogenic QTC prolongation in neurodegenerative diseases. First, advanced imaging techniques, such as functional MRI might allow a more detailed characterization of the intricate functions of the left and right insular cortex. Second, the predictive value of long QTc interval need to be assessed. The results of our study suggest that in patients with severe cognitive impairment, the QTc interval should be frequently monitored and QTc-prolonging drugs avoided or used with precaution.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/19-0632r2).