
Abstract
Background:
Regular aerobic exercises could improve global cognition in older adults with mild cognitive impairment (MCI), such as aerobic dance a type of commonly practiced aerobic exercises. However, its effects remain debatable in improving the cognitive function in patients with MCI.
Objective:
The aim of this systematic review and meta-analysis is to evaluate the effects of aerobic dance on cognitive function among older adults with MCI.
Methods:
We searched articles in the MEDLINE, PubMed, Embase, and The Cochrane Library databases from inception to 28 February 2019, with the following criteria: 1) randomized controlled trials; 2) older adults with MCI; 3) aerobic dance intervention.
Results:
Five studies of 842 participants were identified. This meta-analysis showed that aerobic dance can significantly improve global cognition (Mini-Mental State Examination: MD = 1.43; 95% CI:[0.59, 2.27]; p = 0.0009; Alzheimer’s Disease Assessment Scale-Cognitive Subscale: MD=–2.30; 95% CI:[–3.60, –1.00]; p = 0.0005), and delayed recall ability (SMD = 0.46;95% CI: [0.30, 0.62]; p < 0.00001) in older adults with MCI. In addition, have positive effects on improving executive function (Trial-Making Test A: MD = –2.37;95% CI:[–4.16, –0.58]; p = 0.010; Trial-Making Test B: MD = –16.0; 95% CI: [–30.03, –2.11]; p = 0.020) and immediate recall ability (SMD = 0.24;95% CI: [0.01, 0.46]; p = 0.04).
Conclusion:
Aerobic dance significantly improves global cognitive function and memory in older adults with MCI. In addition, it also benefits executive function. However, due to the limitations as the review states, more randomized controlled trials with better study design and larger sample sizes should be conducted in the future research to make it much clearer.
Keywords
INTRODUCTION
Mild cognitive impairment (MCI) is an intermediary phase between the typical aging process and dementia. MCI includes group of people who suffer from cognitive impairment that occur at the early stage of dementia [1]. According to two recent meta-analysis of people aged over 60, the prevalence of MCI is about 15% [2, 3], while a third, a Chinese cohort study conducted in Beijing, indicated that the prevalence of MCI among elders was 16.6% [4]. In addition, the conversion rates from MCI to dementia and Alzheimer’s disease (AD) are 34% and 28%, respectively [2, 3]. Reduction of the risk factors could be an effective measurement against MCI [5], leading to a drop of the onset of AD at an early age. In addition, 15% of MCI can be reversed to normal [2].
Although there is no positive evidence supporting pharmacological interventions in alleviating cognitive function decline of MCI patients [6–9]. However, several non-pharmacologic interventions, including a Mediterranean diet [10], social connections [8, 11], and cognitive training [12–14] have shown promising results through observational research. In comparison, it has been widely illustrated that physical exercise plays an important role in slowing down the progression from MCI to dementia [11, 15–19], specifically benefiting executive function and memory [17, 19]. The possible mechanism could be the fact that physical exercise not only increase blood flow to the brain and improve function of cardiovascular system as well as it changes the whole metabolic system. Furthermore, physical exercise also involves cognitive and social activities, which might enhance overall brain function [20]. Two recent systematic reviews and meta-analysis reported that intervention such as physical activities including aerobic exercises, can improve cognitive function among older adults with MCI [21, 22]. Aerobic exercises are those exercises that involve large muscle groups activation, such as dancing, jogging, swimming and cycling, etc. [21].
Dance is a very popular community-based activity and commonly practiced aerobic exercise throughout the world. That requires emotional expression, social interaction, sensory stimulation, motor coordination, and bodily movements along with music. However, the intensity, duration, and frequency of such exercise may vary, such as in cha-cha, rumba, waltz, Tai Chi, etc. [23]. As believed, social connections may improve cognitive functions among older adults with MCI as a result of dancing [8, 11]. In addition, another study has indicated that music training may have a stimulatory effect on sensorimotor and auditory system, which may enhance cortical plasticity [24]. Since dance training combines all these factors, it therefore may enhance cognitive functions. Furthermore, it improves mood, fitness level, and self-confidence [25]. Although the exact mechanism of action of this phenomenon is not clear so far, several publications have founded possible mechanism, such as cell and functional magnetic resonance imaging (fMRI) theories [26–28].
Moreover, several recent studies have shown that aerobic dance could improve global cognition as well as other specific domains, such as executive function and memory retention in older adults without cognitive impairment [29–31]. Although few trials have focused on observing the effects of aerobic dance on cognitive impairment among older adults with MCI, the effects of aerobic dance on the global cognition or specific domain of the patients with MCI remains unclear. The aim of the current systematic review and meta-analysis is to determine the effects of aerobic dance on cognitive function in older adults with MCI within the published literature.
METHODS
Literature research
This study was conducted according to the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement [32]. We searched MEDLINE, PubMed, Embase, and the Cochrane Central Register of Controlled Trials for studies on the effects of aerobic dance. The search items included the combination of Medical Subject Heading terms (MeSH) and free words. Taking ‘mild cognitive impairment’ as an example: the relevant ‘MeSH’ is [cognition dysfunction], and the free word including: [Cognitive Impairments] [Mild Neurocognitive Disorder] [Cognitive Declines] [Mental Deterioration], etc. Firstly, we used ‘or’ to combine all those items. Secondly, we searched and combined the ‘MeSH’ and free words of ‘dance’, ‘cognition’, and ‘RCTs’, respectively. Thirdly, we used ‘AND’ to combine all items. Finally, we searched ‘All Field’ (search strategies for all databases are presented in detail in the Supplementary Material). All searches including MEDLINE, PubMed, Embase, and the Cochrane Library were performed from database inception to 28 February 2019.
Inclusion and exclusion criteria
To be eligible for inclusion in this systematic review, a research work has to satisfy the following criteria: 1) Study population over 50 years old, diagnosed as MCI by neurologists; 2) Aerobic dance as an intervention, such as cha-cha, rumba, waltz, and Tai Chi; 3) Participants in the control group received health education and/or exercise but not aerobic dance training; 4) Outcome measurements involved global cognition or other specific domains such as memory and executive function; 5) Randomized controlled trial (RCTs); 6) Published in peer-reviewed journals in English language.
Conference abstracts, case reports, and protocols were excluded from this review. Moreover, studies including elderly with Parkinson’s disease, stroke, cardiovascular disease, and other severe illnesses were also excluded from this study.
Study selection and data extraction
Two independent reviewers (ZQ and GYX) evaluated eligible studies and then extracted data. Disagreements were resolved by discussion or judgement from the third reviewer (ZY). The following information were extracted from each study: authors, country, age, sex proportion, number of participants, type of intervention, duration, frequency, intensity, the cognitive measurements, and their outcomes.
Quality assessments
Two independent reviewers (ZQ and GYX) assessed the risk of bias in the included trials using the Cochrane Risk of Bias Tool [33]. Furthermore, Selection Bias, Performance Bias, Detection Bias, Attrition Bias, Reporting Bias, and other Biases were evaluated, then assigned each of the above items as either high risk, low risk, or unclear according to the levels of bias. Disagreements between the two reviewers were resolved by discussion.
Statistical analysis
All the data was analyzed using RevMan V5.3 (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). In the meta-analysis, we synthesized continuous outcome data using mean difference (MD) and standard deviation (SD). When different measurements for the same outcome were performed in different studies, we used standardized mean difference (SMD) to obtain the summarized effect instead.
In addition, according to the difference of frequency and duration between trials, the clinic heterogeneity was observed; as a consequence, we used the random-effects model with generic inverse-variance was used to pool the effect and its corresponding 95% confidence interval (CI). I2 statistic were used to examine the heterogeneity of the included studies. Large I2 (>75%) suggests high heterogeneity in meta-analysis [33], therefore we only pooled studies when I2 was below 75%. In addition, to determine the causes of the heterogeneity, we conducted a sensitivity analysis by eliminating the studies one by one to identify the study that is heterogeneous from the other studies, by examining whether the I2 statistics changed substantially. Otherwise, we used a sub-group to modify the effects of the outcomes and the two-side p value <0.05 to indicate that the statistics are significant. Furthermore, Funnel plot was not used for assessing publication bias since the number of articles involved in the meta-analysis was very small.
RESULTS
Identification of studies
The flow chart (Fig. 1) illustrates the search strategy. Thirty-six articles were identified from the three main electronic databases, while four more articles were obtained from other sources for further eligibility screening. These articles were imported into the Endnote (a common reference management software) and thirteen duplicates were removed through the build-in function of the software. Subsequently, two reviewers (ZQ, GYX) removed ineligible articles by reading their titles, abstracts, and/or full text. Ultimately, only five studies were included in this systematic review and meta-analysis [34–38].

Flowchart for searching and selection of the included studies.
Study characteristics
The detailed characteristics of each trial are presented in Table 1. All the studies were reported between 2012 and 2018, and were conducted in four different regions (one from America [34], two from China [35, 37], one from Japan [36], and one from Greece [38]). A total of 842 participants were included in the review out of which 263 (31%) were male and the rest were female.
Characteristics of included trials
T, Training group; C, Control group; SD, standard deviation; HRmax, maximum heart rate; RAVLT, Rey Auditory Verbal Learning Test; VFT, Verbal Fluency Test; TMT-A, Trial-making Test part A; TMT-B, Trial-making Test part B; MMSE, Mini-Mental System Examination; ADAS-Cog, Alzheimer’s Disease Assessment Scale-Cognitive Subscale; DST, Digit Span Task; RBMT, Rivermead Behavioral Memory Test; FAS, F-A-S test; WMSR, Wechsler Memory Scale-Revised.
In addition, the dance style also varied across different studies, such as salsa, rumba, waltz, cha-cha, blues, jitterbug, tango, and Tai Chi. Four publications [34, 36–38] adopted a combination of salsa, rumba, waltz, cha-cha, blues, jitterbug, and tango, while one study [35] used Tai Chi only as their intervention. All the studies described their dance routine and were divided into three parts: 1) warm up for 5 to 10 min to reduce the risk of muscle injury and impacts on the respiratory system; 2) aerobic dance for about 30 min; 3) cool down for 5 to 10 min. Four trials [34, 38] were conducted twice or three times a week, while the other was once a week [36]. In addition, the duration of two studies was three month [34, 37], while that of the other was about a year [35, 38]. Only two studies [34, 37] clearly stated their exercise intensity and both were 60%–80% HR max. As for as age is concerned, the participants of four trials [34–37] were about 75 years old whether they were in the intervention group or control group, while in the other article their age was around 65 years old [38].
The outcomes of these trials were global cognition, memory (immediate and delayed recall), and executive function. These were measured using different cognitive assessment tools, for example, Global cognition was assessed using the Mini-Mental System Examination (MMSE) [35, 38], Montreal Cognitive Assessment (MoCA) [37, 38], and/or Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-Cog) [35]. On the other hand, executive function was assessed by Verbal Fluency Test (VFT) [34, 35], FAS (F-A-S test) [38], TMT-A (Trial-making test A) [34–38], and/or TMT-B (Trail Making Test B) [34–38]. The common assessed components of memory were immediate and delayed recall ability. In addition Digit Span Task (DST) [35, 37], Rey Auditory Verbal Learning Test (RAVLT) [34], and Rivermead Behavioral Memory Test 1 (RBMT1) [38] were used to assess immediate recall ability. Wechsler Memory Scale-Revised (WMSR) [37], RAVLT [34], Rivermead Behavioral Memory Test 2 (RBMT2) [38], and 10 min or 20 min story memory recall tests [35, 36] were used to assess delayed recall ability. All the five included studies adopted aerobic dance as their interventions, with stretching, toning exercise, health education, and usual care as their controls.
Quality assessment
To sum up, all the 5 studies were of an exemplary standard. Regarding the selection bias (i.e., randomization sequence generation), all the five articles tended to have an extremely low risk since they generated the randomization sequencing numbers by standard ways such as using number generators on a computer or algorithm. Two studies [37, 38] clearly showcased their method for allocation concealment, and we considered their selection bias (allocation concealment) as low risk. The other three studies did not mention allocation concealment and were considered as ‘unclear’ [34–36]. Due to the nature of the intervention, blinding the instructor and participants was impossible in all five studies. However, outcome assessments were blinded in all the five studies. We considered their blinding bias as high risk. For the attrition bias, almost every trial gave the desired outcomes. Reasons for dropping were clearly stated in each of the included trial. Therefore, we considered their risk of attrition bias as low. We considered the reporting bias for each trial as low risk, since all the outcomes they intended to study were reported and discussed in each study. Detailed information about the bias assessment was shown in Fig. 2.

Risk of bias in trials of each item. Green circle: The risk of bias was low. Red circle: The risk of bias was high. Yellow circle: The risk of bias was unclear.
Effects of aerobic dance intervention on MCI
Global cognition
Figure 3 summarizes the results on global cognition. All five trials assessed global cognition while using different assessment tools. To reduce heterogeneity, we used subgroups to analyze the outcomes based on the assessment tools. Results from pooling of three studies used MMSE to measure cognition impairment showing that aerobic dance could significantly improve global cognition (MD = 1.43; 95% CI: [0.59, 2.27]; p = 0.0009) [35, 38]. Results from the subgroup of two studies using MoCA, showed a high heterogeneity, so we did not pool the effect [32, 33]. One of the two trials reported that aerobic dance could improve global cognition by comparing MoCA scores among experimental and control group [38], but the other did not find any improvement. The main difference between those two studies were as follows: First, the duration was different. Zhu’s et al. trial trained participants for 3 months and found that there was no difference between the groups [32]. While Lazarou et al. with a longer period of study (10-month) found the effects were significant [33]. Second, the frequency of the two trials were different (35 min per day three times a week and 60 min per day two times a week), respectively. Thirdly, the sample size was different, the trial with 129 participants reported that MoCA scores improved significantly through aerobic dance [33], on the other hand, the other study with 59 participants reported the opposite result [32]. In addition, results of one study [35] using ASAD-cog to assess cognition indicated that aerobic dance enhanced global cognition in older adults with MCI (MD = –2.30; 95% CI: [–3.60, –1.00]; p = 0.0005).

Forest plot for aerobic dancing on global cognitive ability. MMSE, Mini-Mental State Examination; ADAS-Cog, Alzheimer’s Disease Assessment Scale-Cognitive Subscale.
Executive function
Figures 4 and 5 shows the effects of aerobic dance on executive function, which was assessed by using VFT, FAS, TMT-A, or TMT-B. Results of the analysis of each subgroup showed that aerobic dance positively enhance the ability of verbal fluency (VFT: MD = 0.22; 95% CI: [–3.43, 3.88]; p = 0.9; FAS: MD = 1.73; 95% CI: [0.58, 2.88]; p = 0.003) and executive function (TMT-A: MD = –2.37; 95% CI: [–4.16, –0.58]; p = 0.010; TMT-B: MD = –16.07; 95% CI: [–30.03, –2.11]; p = 0.020).
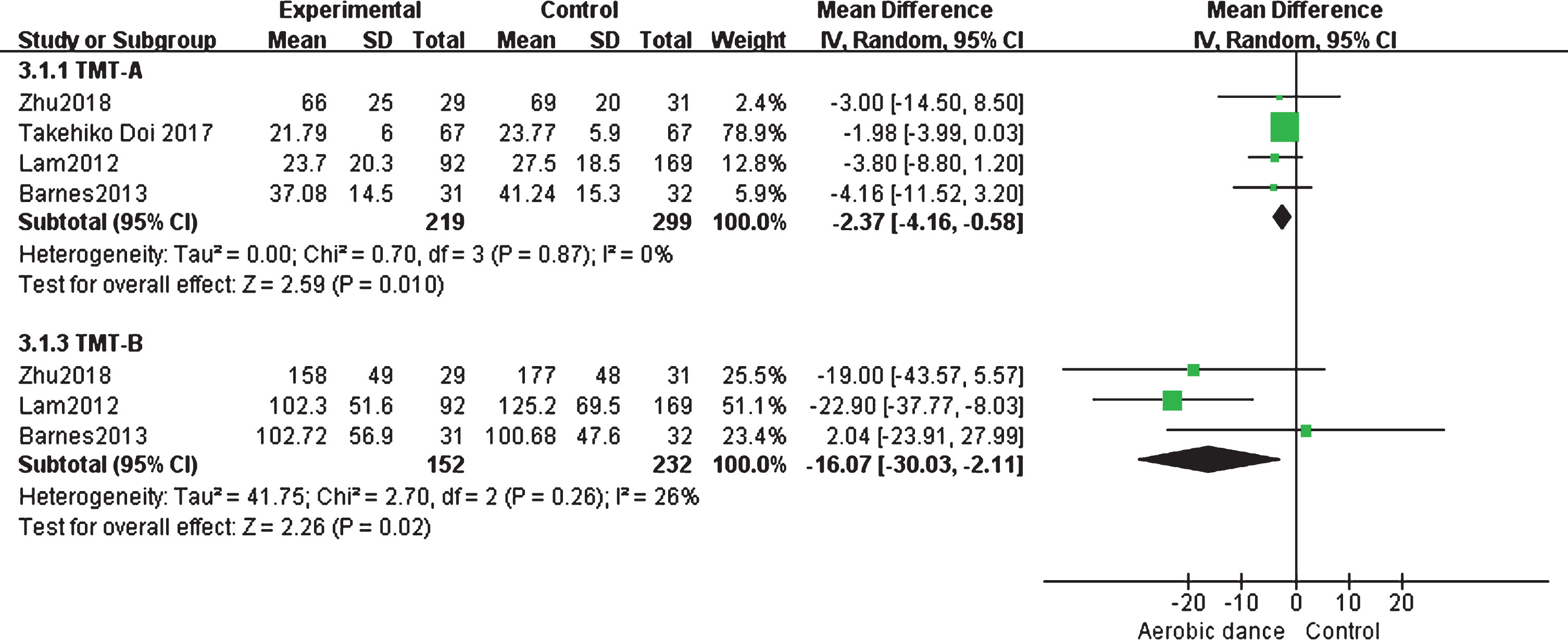
Forest plot for aerobic dancing on executive ability. TMT-A: Trial Making Test-part A; TMT-B: Trial Making Test-part B.
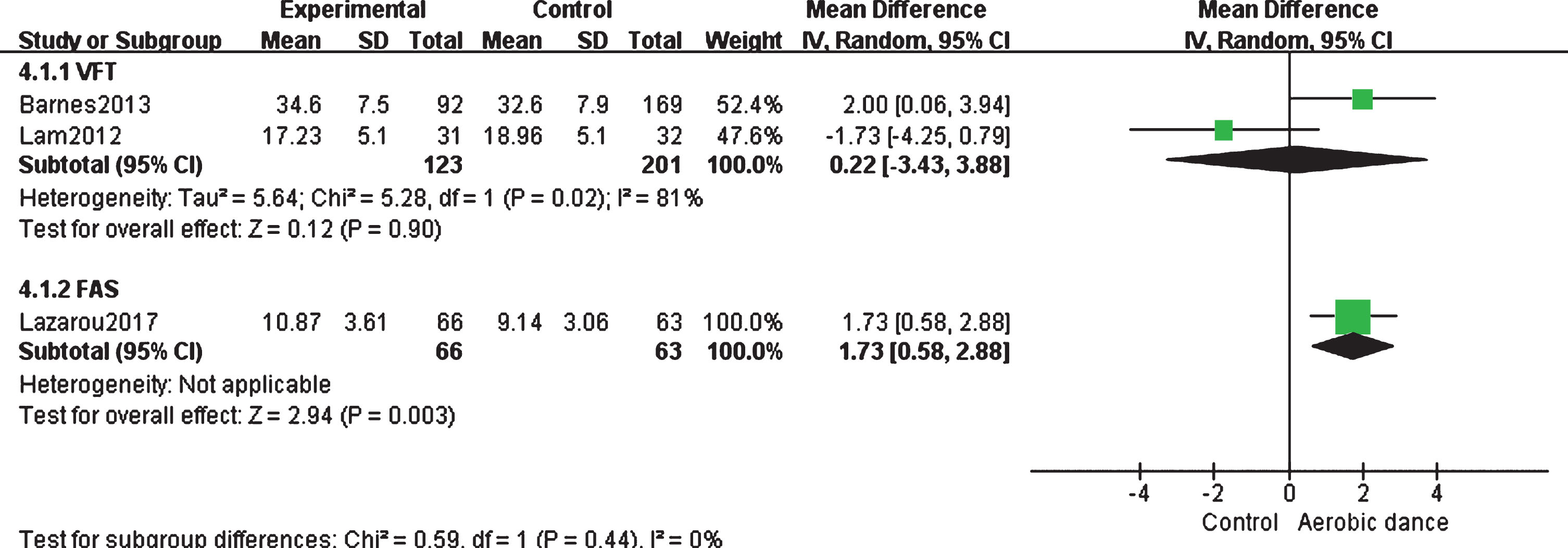
Forest plot for aerobic dancing on verbal fluency. VFT, Verbal fluency test; FAS, F-A-S test.
Memory
Memory was another domain of cognition and was commonly assessed by a participant’s ability of immediate and delayed recall. Among the five included trials, two used Digit Span Task [35, 37], while one employed RAVLT [34] and the other used RBMT1 [38] to assess the immediate memory recall. To ensure that the results from different trials could be synthesized, we calculated the standardized mean difference for each study first. The pooled results on SMD (Fig. 6) showed that aerobic dance intervention significantly improve immediate recall ability in older adults with MCI (SMD = 0.24; 95% CI: [0.01, 0.46]; p = 0.04). Similarly, the pooled results for delayed recall, were assessed using WMSR, RAVLT, RBMT2, and 10 min or 20 min story memory recall tests. Their results showed that aerobic dance significantly improve delayed recall ability amongst elderly with MCI (SMD = 0.46; 95% CI: [0.30, 0.62]; p < 0.00001). Finally, all the detailed data is shown in Fig. 7.

Forest plot for aerobic dancing on immediately recall ability.
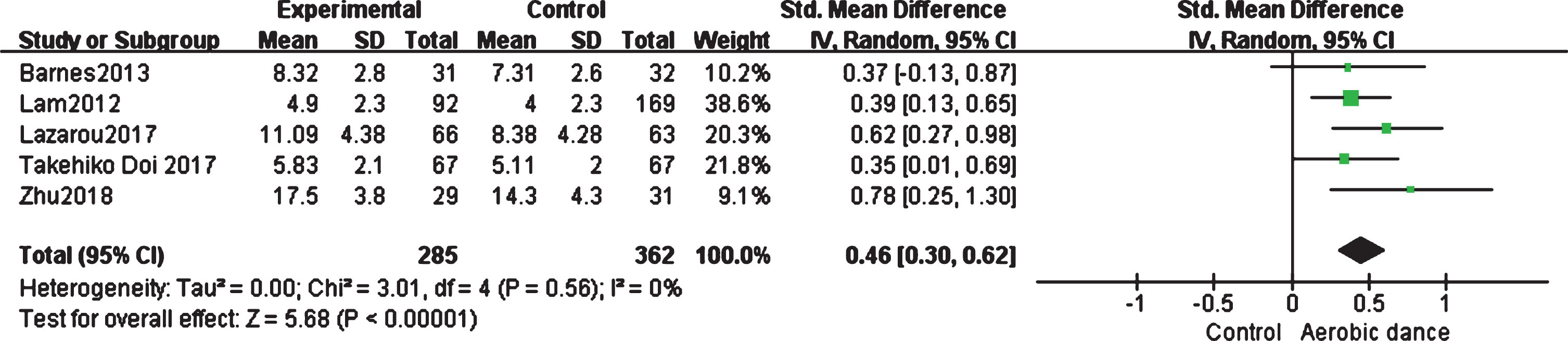
Forest plot for aerobic dancing on delayed recall ability.
DISCUSSION
Our systematic review and meta-analysis collected data from five RCTs freely available in the current literature. According to the results, aerobic dance significantly improves global cognition and memory in MCI patients. Additionally, the results showed that executive function and memory was slightly improved by performing aerobic dance.
However, some of the outcomes of these trials were inconsistent. As prior research indicated that changes in some domains of cognitive function may not be sensitive in a short period [21], different durations of these trails may lead to inconsistency in their outcome. For example, Barnes conducted a 3-month intervention and found that there was no difference between the experimental and control group in either global cognitive function and other domains [34]. On the contrary, other trials of longer duration or follow up period confirmed that cognitive function could be improved to some extent [35–38]. Moreover, Lam et al. reported better delayed recall ability 1 year later, while surprisingly there was no difference between experimental and control group after five months of intervention [35]. While using MoCA as the outcome of global cognition, one study found that there was no improvements after three months’ intervention [37]; on the other hand, the study with a 10-month training showed significant effects [38]. Only two involved studies clearly mentioned the intensity of aerobic dancing, with a target peak heart rate of 60%–75% and 60%–80% of maximum heart rate, respectively [29, 32]. This suggest that intensity maybe another factor of getting inconsistent results. Furthermore, the location, proportion of male and female, and their respective age were differences between studies. Two studies were from China [35, 37], one from America [34], and the remaining two studies were from Japan [36] and Greece [38], respectively. Sex distribution is another different characteristic, as two trials had balanced proportion between male and female and they were both around 50% [36, 37]. In Lam’s et al. [35] and Lazarous’s et al. [38] studies, the proportion of female was 76% and 78%, respectively, meaning they were almost three times as male. In addition, the type of aerobic dance intervention was not the same among five studies. For example, in Takehiko’s [36] and Lazarou’s [38] studies, the training group performed a mixed type of aerobic dance, while in the remaining other three trials, only one type of dance was practiced [34, 37]. Despite the fact that not all of the factors were the same, they showed positive effects on improving cognitive function of MCI by taking part in aerobic dancing activities.
One study with 60 participants conducted in Greece, which chose specific traditional Greek dance as their intervention that lasted for 24 weeks with two times a week for 60 min a session. Their result showed that dance improve cognitive functions, such as attention, verbal fluency, and executive function in MCI [39]. In addition, another similar study with a larger sample size using eight types of ballroom dance in Filipinos showed almost the same results [40].
The exact mechanism of how aerobic dance improves cognitive function in older adults with MCI remains unclear. However, two studies tried to find this possible mechanism. One is the changes in rhythm and the spatial awareness of the body during dance movements that activate place cells and grid cells [26]. The other possible mechanism may be that aerobic exercise delays the degeneration of nerve cells [27]. In addition, Qi et al.’s resting state-fMRI study showed change among cortical activation after aerobic dance. They found significant increase in the amplitude of low-frequency fluctuation in the bilateral frontotemporal, entorhinal, anterior cingulate, and parohippocampal cortex after three months of aerobic dance in MCI patients. As a matter of fact, many cognitive functions such as memory, executive function, and learning depend on the frontal cortex and medial temporal lobe, and activation of these areas through dance may result in functional improvements [28].
Strengths and limitations
Our systemic review and meta-analysis focused on identifying the possible effects of aerobic dance, that could be used as a treatment option for MCI patients. All the trials in this review were conducted and published within the last 5 years; therefore their results were the latest and most convincing. Furthermore, to ensure the quality of our study, we only included RCTs designed with high quality for this review.
However, there were some limitations of this review. Firstly, since aerobic dance was an emerging non-pharmaceutical intervention, very few trials in the area were available in the literature so far. Secondly, the sample size in each trial was not too large. Thirdly, the characteristics of the participants are quite different across different trials, such as cultural background, living conditions, social connections, and level of education. Therefore, the heterogeneity of the studies in this review is substantial and consequently, the obtained results may not be very convincing. In addition, literature search was only performed in the English language medium; therefore, some trials reported in other language may be missed.
Implications for future research
As discussed, RCTs with large sample size, longer intervention and follow-up period are needed to reach a better conclusion of the possible effects of aerobic dance on cognitive function in patients with MCI.
Only a few studies used resting state-fMRI and positron emission tomography to reveal the neural activities, brain volume, and functional connection between brain networks in MCI patients [41, 42]. These studies have revealed that aerobic exercise might increase the thickness of grey matter and hippocampal volume [43, 44]. But the mechanism of the effects of aerobic dancing on cognitive functions remains unclear. Therefore, further studies should include more conventional methods to reveal the correlation between the changes in neural activation, functional connections, and cognitive improvement in such patients.
Conclusion
This research review found that aerobic dance significantly improves global cognition and memory in older adults with MCI. In addition, it also benefits execution function to a large degree. On the other hand, due to the limitations stated, better design and large sample size trials are needed to reveal the true effects of aerobic dance on people with MCI in the future.