
Abstract
Background:
Studies from North America and Western Europe suggest stable or declining trends in impaired cognition across birth cohorts.
Objective:
We aimed to examine changes in the age-specific prevalence of cognitive impairment in the Czech Republic.
Methods:
The study used two samples from the population-based Czech Survey on Health, Ageing and Retirement in Europe. Age-specific prevalence of cognitive impairment (defined based on scores in verbal fluency, immediate recall, delayed recall, and temporal orientation) was compared between participants in wave 2 (2006/2007; n = 1,107) and wave 6 (2015; n = 3,104). Logistic regression was used to estimate the association between the wave and cognitive impairment, step-wise adjusting for sociodemographic and clinical characteristics. Multiple sensitivity analyses, focusing on alternative operationalizations of relative cognitive impairment, impact of missing cognitive data, and survival bias, were carried out.
Results:
The most conservative estimate suggested that the age-specific prevalence of cognitive impairment declined by one fifth, from 11% in 2006/2007 to 9% in 2015. Decline was observed in all sensitivity analyses. The change was associated with differences in physical inactivity, management of high blood cholesterol, and increases in length education.
Conclusion:
Older adults in the Czech Republic, a country situated in the Central and Eastern European region, have achieved positive developments in cognitive aging. Longer education, better management of cardiovascular factors, and reduced physical inactivity seem to be of key importance.
INTRODUCTION
Population-based studies conducted during the past decade, predominantly in high-income countries, suggest stable or declining dementia incidence and age-specific prevalence [1, 2]. According to reviews of the available evidence, no single protective or risk factor can fully explain these trends [1, 2]. However, societal changes that resulted in improved socio-economic conditions and healthcare probably had a positive influence on cognitive health [1, 2]. In particular, the evidence suggests that increase in years of education, improved control of hypertension and hypercholesterolemia, and decreasing occurrence of stroke and ischemic heart disease, likely played an important role [3–6].
Evidence regarding developments in cognitive health from non-western settings is rarer and prevalence estimates vary substantially across countries [7]. Even in Europe, there is a gap in knowledge. For example, data on trends in cognitive health from Central and Eastern Europe (CEE) are largely lacking [1]. No study from CEE was added into the most recent review, which again included predominantly studies from Western Europe and Northern America [2]. Even less is known regarding factors associated with possible changes in cognitive health in non-western settings. Data from low- to middle-income countries suggest variability in factors associated with cognitive impairment and dementia [7, 8]. For example, cross-sectional data from low- to middle-income countries indicated that physical health, rather than socioeconomic factors, predicted cognitive impairment [7]. Thus, it remains to be elucidated which factors influence trends in cognitive health in non-western settings.
With regards to Europe, a large morbidity and mortality gap between Western Europe and CEE is well known [9, 10]. For example, while cardiovascular morbidity and mortality have been declining since the 1970 s in Western Europe, the rates have been increasing in CEE during the second half of the 20th century [9, 10]. These unfavorable trends have been attributed to socioeconomic disruptions at the national levels, leading to excessive alcohol consumption, poor nutrition, low physical activity, material hardship, psychosocial distress, or high rates of depression [9–13]. These societal developments may influence trends and predictors of changes in cognitive health.
Subsequently, this study aims to assess the change in the age-specific prevalence of cognitive impairment in the Czech Republic, and determine whether sociodemographic or clinical factors might explain the change. The Czech Republic is a good country in the CEE region for examining changes in cognitive health due to recent socio-economic and health shifts and an ongoing reform of mental health care [14–17]. It is a post-communist country that underwent a rapid social and economic transition into a westernized society. Recent studies suggest major improvements in the control of cardiovascular risk factors and declining mortality from ischemic heart disease and stroke [18–20]. We hypothesize that these changes could contribute to the improvement of cognitive health of older adults in the Czech Republic.
MATERIALS AND METHODS
Source of data
Data from the Survey on Health, Ageing and Retirement in Europe (SHARE) were used. Modelled after the Health and Retirement Study (HRS) from the United States (US) and the English Longitudinal Study of Ageing, SHARE is a European prospective, multi-center study of community-dwelling individuals aimed at providing comparative data on population aging across Europe. SHARE collects information about participants’ health, social network, and economic conditions using computer-assisted personal interviewing (CAPI), as previously described in detail [21]. The first wave was conducted in 2004, followed by wave 2 in 2006/2007, wave 3 in 2008/2009, wave 4 in 2011/2012, wave 5 in 2013, and wave 6 in 2015.
Study sample
The Czech Republic joined SHARE study in wave 2, when 2,877 households were sampled. To maintain the original age structure and because of attrition due to death and loss to follow-up, SHARE replenishes its sample between waves. Refreshment samples were recruited and added 4,371 new households in wave 4 and 1,361 in wave 5. The response rate in wave 2 was 60% and retention of participants was 72% (wave 2 to 3), 82% (wave 3 to 4), 88% (wave 4 to 5), and 89% (wave 5 to 6) of the surviving respondents from the previous waves (Fig. 1).
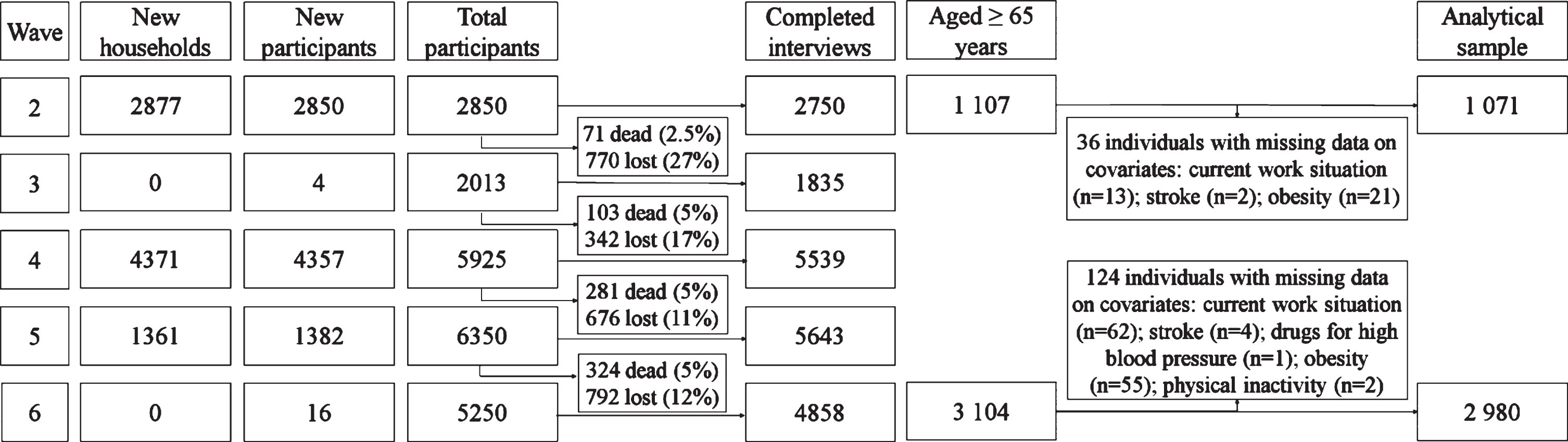
Share Czech Republic data collection flowchart.
To assess the change in age-specific prevalence of cognitive impairment, we identified two similar nationally representative cohorts that were examined with the same cognitive tests. We selected the wave 2 (2006/2007), when the Czech Republic joined SHARE, and wave 6 (2015), which provided the most recent data. This allowed examination of a change over 8-9 years period. In wave 2 (2006/2007), 2,750 individuals (on average 63 years old; 57% women) were interviewed. We restricted the analysis to participants aged 65 years and older (n = 1,107). We excluded 36 observations due to missing data on covariates, leaving 1,071 persons in sample for wave 2 (57% women, mean age 73 years, range 65– 95).
The wave 6 included predominantly individuals recruited from the refreshment samples (n = 2,757). However, 347 participants from the wave 2 also participated in wave 6, resulting in total 3,104 respondents. We excluded 124 observations due to missing data on covariates, leaving 2,980 in wave 6 for the analytical sample (58% women, mean age 73 years, range 65– 103). In the present study, we consider the individuals in wave 2 as “cohort 1” and those in wave 6 as “cohort 2”.
Definition of cognitive impairment
Cognition was assessed using four measures: verbal fluency, immediate recall, delayed recall, and temporal orientation. We re-coded each cognitive measure to a binary variable indicating impaired versus normal performance. First, we pooled together the scores from wave 2 and wave 6 and transformed them into z-scores, using the mean and standard deviation (SD) of this pooled population. Second, the cut-off for impaired performance was set at z-score 1.5 SD below the mean, which is a generally used criterion for relative cognitive impairment [22]. The thresholds corresponded to the following scores: impaired verbal fluency <9 animals; impaired immediate recall <3 words; impaired delayed recall <1 word; impaired temporal orientation <3 points. Participants with impaired performance in at least 2 measures were considered as having cognitive impairment.
In cohort 1, 1.5% (n = 16) individuals did not have complete data on cognitive measures compared to 4.2% (n = 126) in cohort 2. Participants with missing data on cognition may be more likely to have cognitive impairment [23], which can bias our results. Therefore, we present three scenarios (cognitive impairment 1– 3), where we handle missing data in different ways. Cognitive impairment 1 was the most extreme scenario, as we classified all individuals with any missing data on cognition as having cognitive impairment. Cognitive impairment 2 used two proxy variables to define cognitive impairment in individuals with incomplete data (see the Supplementary Material for details). For cognitive impairment 3, we executed a complete case analysis by excluding individuals with any missing data on cognition. Further, cognitive impairment 4 is defined based on a summary scale from individual cognitive tests.
Covariates
Covariates were chosen based on the existing literature as sociodemographic factors or variables related to cardiovascular and overall health that could explain the change in the prevalence of cognitive impairment [24–28].
Statistical analysis
We present participants’ characteristics as frequency (n, %), mean±standard deviation or median and interquartile range (IQR) and compared them between the two waves with a χ2 test, independent sample t-test and Mann-Whitney test, where appropriate. The characteristics of cohort 2, except for age and sex, were sex- and age-standardized to cohort 1. For multivariable analysis, we used analytical framework utilized by Langa et al. in a similar analysis based on the HRS [29]: We pooled data from cohort 1 and 2 and performed logistic regression with a dependent variable indicating whether an individual had cognitive impairment. A binary variable “cohort” that took the value of 0 for cohort 1, and the value 1 for cohort 2, was the independent variable. Odds ratio (OR) with 95% confidence interval (CI) were estimated for the association of the cohort with cognitive impairment. An OR lower than 1 indicates a lower prevalence of cognitive impairment in cohort 2. We ran models, which step-wise added groups of covariates. Model 1 was adjusted for age, sex, and birth cohort; Model 2 added education, and cardiovascular and overall health measures were included in Model 3. We assessed the potential multicollinearity using variance inflation factors (VIF). All covariates included in Model 3 had VIF less than 4 and were thus kept in the final model. In order to examine to what extent our predictors explain the differences in prevalence of cognitive impairment between cohort 1 and 2, we used a multivariate decomposition for nonlinear models [30].
All analyses were performed both with and without calibrated cross-sectional sampling weights. Several sensitivity analyses, focusing on alternative operationalizations of relative cognitive impairment, impact of missing cognitive data and survival bias, tested the robustness of our findings. Data was analyzed using STATA, version 15.1 and IBM SPSS Statistics for Windows, Version 23.0 (IBM Corp. Armonk, NY). See the Supplementary Material for details related to fieldwork, sampling, cognitive measures, operationalization of cognitive impairment 1– 4, definition of covariates, sampling weights, sensitivity analyses, and ethical considerations.
RESULTS
Characteristics of participants
The study sample included 1,071 individuals in cohort 1 and 3,104 in cohort 2, of those 318 individuals took part in both. Table 1 presents characteristics of the two cohorts (age- and sex-standardized to the cohort 1, and weighted using individual sampling weights). The raw data (unweighted and not standardized) are presented in Supplementary Table 1. Those in cohort 2 were more educated, more often lived with a spouse, and had a higher net worth (Table 1). They less frequently reported stroke and myocardial infarction, but more often reported having been diagnosed with high blood pressure, high blood cholesterol, and diabetes mellitus and to be taking cardiovascular drugs. In addition, they were less frequently depressed and physically inactive, but more commonly obese.
Characteristics of the study cohort
Note: cohort 1 = wave 2; cohort 2 = wave 6. All presented characteristics are weighted, using individual sampling weights. Except for age and sex, characteristics in wave 6 were age- and sex-standardized to the wave 2 cohort, using direct standardization. *p < 0.05; **p < 0.001. awave 2: 16 missing cases (1.5%); wave 6: 112 missing cases (3.8%). bwave 2: 13 missing cases (1.2%); wave 6: 118 missing cases (4.0%). cwave 2: 13 missing cases (1.2%); wave 6: 122 missing cases (4.1%). dwave 2: 0 missing cases; wave 6: 106 missing cases (3.6%).
Cognitive health of participants
Cohort 2 had higher scores on all cognitive tests. When classifying individuals with missing data as cognitively impaired, we observed that the age- and sex- standardized frequency of cognitive impairment in cohort 2 was 1.2 times lower than in cohort 1 (cognitive impairment 1: 11% versus 9%; Table 1). When we used proxy-variables to indicate cognitive impairment, its frequency was 1.6 times lower in cohort 2, compared to cohort 1 (cognitive impairment 2: 11% versus 7%). In the complete case analysis, the prevalence of cognitive impairment was 2.3 times lower in cohort 2 than in cohort 1 (cognitive impairment 3: 9% versus 4%). An alternative definition of cognitive impairment using a summary scale resulted in 1.8 times lower frequency of cognitive impairment in cohort 2 than in cohort 1 (cognitive impairment 4: 31% versus 17%).
Multivariable analysis
In multivariable analysis, cohort 2 was significantly associated with lower odds of cognitive impairment 1, adjusting for age, sex, and birth cohort (Table 2, not weighted OR 0.59; 95% CI 0.37 to 0.95; Model 1). This association was attenuated and lost statistical significance, when education was added into the model (not weighted OR 0.67; 95% CI 0.41; to 1.08; Model 2). The association was further attenuated by adding all other covariates (not weighted OR 0.72; 95% CI 0.43 to 1.21; Model 3). Cognitive impairment 1 was associated with higher age, stroke, high blood cholesterol, drugs for coronary heart diseases, depression, excessive alcohol consumption, and physical inactivity. Being a woman, higher education, and use of drugs for cholesterol were all associated with lower odds of cognitive impairment (Supplementary Table 2).
Association of cohort 2 (relative to cohort 1) with cognitive impairment
*p < 0.05; **p < 0.001; OR, odds ratio; CI, confidence interval. Model 1: age, sex, birth cohort. Model 2: age, sex, birth cohort, education. Model 3: age, sex, birth cohort, education, living with a spouse, net worth, currently working, stroke, myocardial infarction, high blood pressure or hypertension, high blood cholesterol, high blood sugar or diabetes mellitus, drugs for high blood pressure, drugs for cholesterol, drugs for diabetes mellitus, drugs for coronary heart disease, depression, alcohol, obesity, physical inactivity.
The multivariate decomposition indicated that the difference in prevalence was predominantly (88%) attributable to differences in characteristics of the two cohorts. The changes in prevalence of cognitive impairment 1 could be explained through reduction in physical inactivity, receiving medication for high blood cholesterol, increases in length of education, and reduction in stroke (Supplementary Table 3). Increases in proportion of individuals with high blood cholesterol has negatively influenced the observed prevalence changes.
The changes were similar for cognitive impairment 2, 3, and 4. Nevertheless, the associations remained statistically significant even after the progressive adjustments. We also observed analogous changes for individual cognitive domains (Supplementary Table 4). The weighted analyses provided similar trends in the estimates, but all associations were statistically significant due to a large sample size generated by the sampling weights. After excluding the 318 survivors from 2015 sample from the analyses, the results did not differ (Supplementary Table 5).
DISCUSSION
This study suggests a decline in age-specific prevalence of cognitive impairment in the Czech Republic over the period between 2006/2007 and 2015. The most conservative estimate suggests that the prevalence of cognitive impairment decreased by one fifth, from 11% in 2006/2007 to 9% in 2015. The reduction in physical inactivity, more intensive control of high blood cholesterol, and increases in the length of education were the main predictors related to the decline in cognitive impairment. The findings were robust to different ways of accounting for missing data and to several sensitivity analyses. To the best of our knowledge, this is the first study conducted in the region of CEE that reports on changes in cognitive health of older adults.
In high income countries, trends in prevalence of dementia varied across regions [1]. In Sweden, dementia prevalence remained relatively stable. On the other hand, a study from France and Spain yielded mixed results, and studies from the US and the United Kingdom reported declines in age-specific prevalence. The magnitude of the declines ranged from 12% to 21% per 10 years [1]. An American analysis based on data from the HRS, which is similar to SHARE, focused specifically on cognitive impairment and found a larger decrease of almost 29% [31]. The decline observed in our study, where our definition of cognitive impairment may indicate a spectrum of neurocognitive disorders, is similar in magnitude to the western countries and corresponds approximately to 20% for almost 10 years.
The downward trend in cognitive impairment co-occurred with several changes in the prevalence of risk and protective factors. In high income countries, the factors that influence changes in prevalence and incidence of dementia varied [1]. For example, education explained 6– 10% of the dementia prevalence changes in France and the US, but did not explain the trends observed in the Netherlands [1]. Similarly, the importance of cardiovascular factors varied across locations. In our study, the majority of the lower cognitive impairment prevalence in 2015 was explained by reductions in physical inactivity, improved control of high blood cholesterol, and increases in length of education. However, increased proportion of individuals with high blood cholesterol may be slowing down the improvements in cognitive health in the Czech Republic. Although causation cannot be assumed due to the observational design of this study, our findings are in line with those found in other Western European countries and the US [3–6].
Several methodological issues should be considered when interpreting our results. Our definition of cognitive impairment was based on scores from brief cognitive tests; clinically established diagnosis of dementia was not a part of SHARE. Unlike clinical diagnoses, our definition is not subject to shifts in clinical practice, which influences prevalence estimates [32]. However, we acknowledge that trends in the prevalence of clinically diagnosable forms of cognitive impairment (mild cognitive impairment, dementia, and Alzheimer’s disease) may not parallel those observed in our study. As there is no information about history of cognitive decline from a previous premorbid level, we may have included also cognitively healthy individuals in our definition of cognitive impairment. More specifically, our definition is based on a threshold derived from a relative comparison. First, we used impairment in two out of four individual domains as a criterion. This approach should be less sensitive to the relative nature of our definition. However, the cognitive tests used tap mainly into three cognitive areas and subsequently some other aspects of cognition, such as executive and visuospatial ability, were not measured. Memory complaints are typical in cognitive impairment, but it is possible that we may have missed the relatively smaller proportion of individuals with atypical cognitive impairment. Second, we used the relative threshold on a summary scale. The second definition suggested more pronounced decrease, yet the overall pattern was the same.
Non-participation and missing data are validity threats in aging studies [33, 34]. In our study, there were more missing data on cognition in 2015 than in 2006/2007 (4.2% compared to 1.5%), which prevents us from having an accurate estimate of the magnitude of change in cognitive impairment. The observed decline in prevalence could be an artefact if non-response was higher among those with cognitive impairment. To address this issue, we presented three alternative scenarios of dealing with missing data. In the most extreme scenario we assumed all individuals with missing data on cognitive measures had cognitive impairment. Even with this assumption, we have observed that the prevalence of cognitive impairment decreased by one fifth. Decline in the alternative scenarios, using proxy variables for defining cognitive impairment and complete case analysis, had a larger magnitude.
In addition, a form of selection into the sample is survival bias, which could decrease the validity of our estimates. Due to the SHARE panel design, 318 participants from wave 2 (2006/2007) were part of wave 6 (2015). These survivors had higher cognition, however, their exclusion from the analysis did not alter the results. Further, the use of weights, which were created to reduce potential selection bias due to non-response and attrition, did not alter our main findings. Another limitation is that the exclusion of institutionalized individuals from the sampling frame likely underestimates prevalence of cognitive impairment at both time points. It is not known how many older adults are institutionalized in the Czech Republic, but we assume they have a higher prevalence of cognitive impairment in comparison with the general population. If the proportion of institutionalized individuals increased from 2006/2007 to 2015, the observed decline may be overestimated. Finally, we acknowledge that participants in our analytical sample were more educated than the general population of the Czech Republic, which could underestimate the burden of cognitive impairment in both cohorts.
This study also has several major strengths. It is based on a large cohort of community-dwelling older adults, which was obtained via random sampling. The SHARE data collection was consistent across waves and included substantial training and quality back-checks. So far, no other country from the region of CEE has been able to contribute to the current literature concerning the world-wide trends in cognitive health [1, 2], due to the lack of directly comparable studies of population representative samples using the same methods across time. More studies from CEE are needed as individuals in these countries have a worse mental health profile than their counterparts in Western Europe and Scandinavia [27, 28]. To the best of our knowledge, no other country used SHARE data to analyze changes in the occurrence of cognitive impairment. An analysis similar to ours would be possible for Poland, which joined SHARE also in the Wave 2. Other CEE countries entered the SHARE project later, which precludes studying changes across time.
In conclusion, due to worldwide demographic aging, we need to anticipate social and healthcare needs, thus understanding trends in cognitive impairment is crucial. Even though there is not sufficient evidence from randomized controlled trials, a large body of observational studies suggests that increase in lengths of education and reduction in cardiovascular diseases could postpone the onset of cognitive impairment [35]. The present study provides indirect evidence that this could be achieved in a country situated in CEE. However, the full set of social, biological and clinical factors contributing to the downward trend in cognitive impairment is still unknown. Further population-based research is needed across CEE, which has poorer risk profiles across different countries, and if possible, the outcomes should be clinically validated. Future studies should also address aspects of incidence and survival.