
Abstract
Cerebral white matter (WM) represents the structural substrate of neuronal communications which is damaged by Alzheimer’s disease (AD). Aerobic exercise training (AET) may improve WM integrity in cognitively normal older adults, but its efficacy remains unknown in patients with amnestic mild cognitive impairment (MCI), a prodromal phase of AD dementia. Therefore, we conducted a proof-of-concept study that randomized 70 amnestic MCI patients to a 1-year program of AET or a non-aerobic stretching and toning (SAT), active control group. Thirty-six patients completed both baseline and follow-up MRI scans, and cerebral WM integrity was measured by WM lesion volume and diffusion characteristics using fluid-attenuated-inversion-recovery and diffusion tensor imaging respectively. Peak oxygen uptake (VO2peak) and neuropsychological function were also measured. At baseline and 1-year follow-up, WM lesion volume and diffusion characteristics were similar between the AET and SAT groups, although VO2peak significantly improved after AET. The AET group showed slight improvement in neuropsychological performance. When analyzing individual data, tract-based spatial statistics demonstrated that VO2peak improvements are associated with attenuated elevations in mean and axial diffusivities, particularly the anterior WM fiber tracts (e.g., genu of corpus callosum). In patients with amnestic MCI, we found that although AET intervention did not improve WM integrity at group level analysis, individual cardiorespiratory fitness gains were associated with improved WM tract integrity of the prefrontal cortex.
Keywords
INTRODUCTION
The global prevalence of dementia is rapidly increasing while we currently do not have effective treatments [1]. To date, most, if not all, pharmaceutical trials have failed to improve cognitive symptoms in patients with Alzheimer’s disease (AD), which may suggest that interventions initiated after symptomatic onset may not be able to reverse the brain pathologies that have accumulated over years or decades [2]. In contrast to treating dementia, mild cognitive impairment (MCI), which is an intermediate phase between normal cognitive aging and dementia, may be a better window for preventive therapies to slow further cognitive decline [3]. Therefore, understanding interventions that may delay onset or reduce risks of further cognitive decline in MCI represents a critical and timely need.
Cerebral white matter (WM) damage is one of the core pathological features of AD [4, 5]. Mounting evidence shows that AD and MCI both are associated with an increased volume of WM lesions [4] and altered diffusion characteristics of WM fiber tracts [5] when compared with age-matched cognitively normal controls. In particular, increased mean diffusivity, as measured by diffusion tensor imaging (DTI), has been shown to detect longitudinal WM changes associated with AD dementia and MCI [6]. Additionally, DTI provides axial and radial diffusivities that may help explain the neurobiological mechanism of WM damage such as axonal degeneration and demyelination [7].
Regular aerobic exercise may improve cerebral WM integrity [8–10], thereby preventing or slowing cognitive deteriorations associated with MCI and AD dementia [11–13]. In cognitively normal old adults, aerobic exercise training (AET) has been shown to increase prefrontal WM volume [8] and improve neuronal fiber tract integrity assessed by DTI [9]. Our recent cross-sectional study also demonstrated that in amnestic MCI patients, higher peak oxygen uptake (VO2peak), which is the gold-standard measure of cardiorespiratory fitness, is associated with higher fractional anisotropy and lower mean, axial, and radial diffusivities [10]. Collectively, these findings suggest the potential benefits of AET for improving WM integrity in older adults; however, no randomized controlled trial (RCT) has been conducted to investigate such effects in patients with amnestic MCI.
The purpose of the present study was to determine the effects of a 1-year AET program on cerebral WM integrity in patients with amnestic MCI. We hypothesized that 1) AET would decrease mean diffusivity of the global and/or regional WM fiber tracts in amnestic MCI patients when compared with a non-aerobic, stretching and toning (SAT) active control group, 2) cognitive performance would improve in the AET but not in SAT groups, and 3) VO2peak improvement would be correlated with changes in WM integrity and cognitive performance.
MATERIALS AND METHODS
Trial design
The present data were derived from a larger 1-year, single-blinded, proof-of-concept RCT comparing the effects of AET versus SAT programs on neurocognitive function in amnestic MCI patients [14]. In this RCT, MRI data were collected at baseline and 1-year follow-up from a subset of eligible participants who do not have contraindications such as metal implants or claustrophobia. This study was approved by the Institutional Review Board of the University of Texas Southwestern Medical Center and Texas Health Presbyterian Hospital Dallas in accordance with the guidelines of the Declaration of Helsinki and Belmont Report. The trial was registered at ClinicalTrials.gov (NCT01146717: Aerobic Exercise Training in Mild Cognitive Impairment Study). All subjects gave written informed consent before participation.
Participants
Recruitment was conducted in the Dallas-Fort Worth metropolitan area using community-based advertisements and through the University of Texas Southwestern Medical Center Alzheimer’s Disease Center. Inclusion criteria were men and women aged 55-80 years with a clinical diagnosis of amnestic MCI. These criteria were used because in this age range, the prevalence of MCI starts increasing [15] and exercise training can be implemented safely according to our previous studies [16]. For screening, an initial telephone interview was conducted to ask potential participants if they had 1) memory concerns, 2) progressive memory decline, and 3) participation in structured exercise program. Subsequently, those individuals who had memory concerns and were not exercising regularly were asked to visit our clinical office for further screening.
The diagnosis of amnestic MCI was based on Petersen criteria [17], as modified by the Alzheimer’s Disease Neuroimaging Initiative project (http://adni-info.org). All subjects had a global Clinical Dementia Rating (CDR) scale of 0.5 with a score of 0.5 in the memory category, in addition to objective memory loss as indicated by education-adjusted scores on the Logical Memory subtest of the Wechsler Memory Scale-Revised. All had Mini-Mental State Exam (MMSE) scores between 24 and 30.
Clinical evaluation was performed according to the recommendations from the Alzheimer’s Disease Cooperative Study (http://adni-info.org). Exclusion criteria included a diagnosis of AD dementia or other dementia types or major neurological, vascular, or psychiatric disorders (e.g., multiple sclerosis, stroke, schizophrenia). In addition, participation in regular exercise within the last 2 years, sleep disorders including clinically diagnosed or self-reported sleep apnea, uncontrolled hypertension, diabetes, and a history of smoking within the past 2 years were excluded. Severe obesity with body mass index≥35 kg/m2 were also excluded to safely conduct exercise training programs (detailed inclusion and exclusion criteria are presented in ClinicalTrials.gov: NCT01146717). To ensure the physical activity level before enrollment, each participant wore an Actical accelerometer for 1 week (Actical, Philips Respironics, USA), and those who spent >90 min of moderate-to-vigorous physical activity (>4.0 METs) per week were excluded.
Randomization and blinding
SAS V9.2 was used to generate the stratified randomization lists using a block factor of 4, where age (55-70 and 71-80 years old) and sex (men and women) were used for stratification. Investigators conducting outcome measurements were blinded to treatment assignment. Participants were instructed to maintain their normal daily activities aside from the assigned intervention program and not to disclose their group assignment to other participants.
Interventions
AET program
The AET program was created individually based on fitness level of each participant that was assessed by VO2peak testing. Training dose (i.e., intensity, duration, and frequency) was progressively increased for the first 26 weeks and maintained for the following weeks. Specifically, the program started with a frequency of 3 exercise sessions/week for 25-30 min/session at the intensity of 75-85% of maximal heart rate that was measured by baseline VO2peak testing. At week 11, participants started alternating between 3 and 4 exercise sessions/week for 30-35 min/session, and at the weeks in which they performed 3 exercise sessions/week, a high intensity exercise session was introduced which consisted of 30 min of walking at the intensity of 85-90% of maximal heart rate (e.g., brisk uphill walking). After week 26, participants performed 4-5 exercise sessions/week for 30-40 min, including 2 high intensity sessions. Each exercise session included a 5-min warm-up and a 5-min cool-down. Participants were allowed to perform other modes of aerobic exercise besides walking as long as they achieved the prescribed training dose. During each exercise session, heart rate was recorded continuously using a heart rate monitor (Polar RS400, Polar Electro, USA). Of note, this AET program meets the national physical activity guidelines which recommend 3-5 days of > 30-min moderate-to-high intensity aerobic exercise [18], and has been used successfully in our previous studies that showed significant cardiorespiratory fitness improvement in sedentary older adults [16].
SAT program
The non-aerobic SAT program was used as an active control group to keep participants engaged with a similar level of attention given to the AET group. The frequency and duration of the SAT program were also kept at the same level as the AET program. A stretching and toning exercise routine that focuses on the upper and lower body was used, and participants were asked to keep heart rate below 50% of their maximal heart rate during each session. At week 19, we introduced a second set of full body stretches that are more advanced than the previous set. After week 26, we introduced a set of low resistance theraband exercise that focuses on strengthening the upper and lower body.
In both AET and SAT programs, each participant was supervised for the first several weeks until they could comfortably exercise by themselves. Subsequently, a home-based exercise program was used, so participants could exercise by themselves at their convenient location and time to reduce study burden. During the study period, they were asked to perform the assigned intervention on top of their regular physical activities. To ensure adherence to each program, participants were required to keep a training log in addition to heart rate monitoring during each exercise session. In each month, participants visited our clinic to download heart rate data and review their training log together with an exercise physiologist to ensure implementation of the prescribed training programs. When adherence to exercise programs were not met with the prescribed intensity, duration, and frequency, in-person and/or telephone meetings were held to address the issues and encourage participants to continue the program.
Measurements and analyses
MRI data collection and processing
All MRI data were collected on a 3-Tesla scanner (Philips Medical System, Best, The Netherlands). The following imaging sequences were acquired: 1) 3D T1-weighted magnetization-prepared rapid acquisition gradient echo image, 2) DTI, and 3) fluid-attenuated-inversion-recovery (FLAIR) image. DTI data were collected twice at each time point and averaged to increase the signal-to-noise ratio.
T1 and DTI data were processed by the FreeSurfer software (version 6.0, Boston, MA, USA; http://surfer.nmr.mhg.harvard.edu/) and the FMRIB Software Library (FSL version 5.0, Oxford University, UK; http://www.fmrib.ox.ac.uk/fsl). First, T1 data were processed by the FreeSurfer’s cross-sectional pipeline (i.e., recon-all) which executes motion correction, removal of non-brain tissue, automated Talairach transformation, intensity correction, volumetric segmentation, and cortical surface reconstruction [19]. Subsequently, the longitudinal pipeline was applied to create a robust, unbiased, within-subject template and perform reliable detection of brain structural changes that may occur with intervention and/or aging [20].
The longitudinal tracts constrained by underlying anatomy (TRACULA) program was used to process DTI data [21]. TRACULA uses prior anatomical information obtained by an unbiased within-subject template generated by the longitudinal recon-all processing and automatically reconstructs the WM pathways based on global probabilistic tractography with the ball-and-stick model [22]. Consequently, the weighted averages of anisotropy and diffusivity measures were calculated from the 10 major WM fiber tracts: forceps major and minor, anterior thalamic radiation, cingulum-angular bundle and -cingulate gyrus, corticospinal tract, inferior longitudinal fasciculus, superior longitudinal fasciculus-parietal and -temporal, and uncinate fasciculus. Furthermore, DTI data were analyzed by tract-based spatial statistics (TBSS) in order to explore whether 1-year changes in anisotropy and diffusivity measures were associated with exercise interventions or individual changes in VO2peak at a voxelwise level [23].
WM lesion volume was measured from FLAIR images using the lesion prediction algorithm implemented in the LST toolbox (version 2.0.15; http://www.statistical-modelling.de/lst.html) which consists of a binary classifier of WM hyperintensities in the form of a logistic regression model [24]. T1 data were also used to improve the anatomical accuracy of WM lesion volume quantification. Detailed MRI data collection and processing methods are provided in the Supplementary Material.
VO2peak measurement
A modified Astrand-Saltin protocol was used to measure VO2peak [25]. During testing, treadmill grade was increased by 2% every 2 min until exhaustion while participants walked or jogged at a fixed speed, which was determined by individual fitness level. VO2 was measured during the 2nd minute of each stage using the Douglas bag method [26]. Gas fractions were analyzed by mass spectrometry (Marquette MGA 1100) and ventilatory volume was measured by a Tissot spirometer. Blood pressure, 12-lead electrocardiogram, and heart rate were continuously monitored during exercise testing to assess cardiovascular responses.
The VO2peak was defined as the highest VO2 measured from a > 30-s Douglas bag during the last stage of testing. In cases where we were not able to collect at least 30 s of the final stage bag, the test was repeated on another day. The criteria to confirm that VO2peak was achieved included an attenuation of VO2 elevation < 150 ml despite increasing work rate of 2% grade, a respiratory exchange ratio > 1.1, and heart rate < 5 beats/min of age-predicted maximal values. In all cases, at least two of these criteria were achieved, confirming the identification of VO2peak based on the American College of Sports Medicine guidelines [27]. Our previous studies showed that using this method, VO2peak can be measured reliably in sedentary older adults [16].
Neuropsychological function
In order to provide an assessment of episodic memory and executive function, the California Verbal Learning Test-second edition (CVLT) [28] and the Delis–Kaplan Executive Function System (DKEFS) [29] were included due to their widespread use, good norms, and sensitivity for detecting cognitive change and the effects of AET and cardiorespiratory fitness [30, 31]. Specifically, we used the standardized total and delayed free recall scores from the CVLT to assess episodic memory performance. Executive function was assessed by the Trail Making, Color-word interference, and verbal and category fluency test scores from the DKEFS.
Sample size estimate
The sample size estimate for this proof-of-concept RCT was based on potential improvements in neuropsychological performance with AET in cognitively normal healthy older adults due to the lack of similar RCTs in MCI patients at the time of trial initiation [32]. After 1 year of AET (treatment), we anticipated that the scores of memory and executive function assessment would improve by ∼0.6 standard deviations when compared with the SAT group (control). Assuming a 15% attrition rate and an α-level of < 0.05, 70 participants provided 80% power to detect an effect size of 0.60. The sample size estimate for MRI scans or WM integrity measurement was not performed because it was a secondary outcome of the trial [14].
Statistical analysis
Seventy amnestic MCI patients were enrolled in the trial [14], and 48 completed interventions (Supplementary Figure 1). For the present study, statistical analysis was performed on 36 patients who completed both baseline and 1-year follow-up MRI scans. To compare the AET and SAT groups, independent sample t-test and chi-square test were used for continuous and categorical variables respectively. Mixed analysis of variance (ANOVA) with two factors (i.e., group*time) was used to examine the intervention effects between the SAT and AET groups. For analysis of TRACULA output, hemisphere was further added as the 3rd factor (i.e., group*time*hemisphere). To assess the relation between changes in outcome measures, Pearson’s product moment correlation analyses were used.
For TBSS, general linear model was used to design statistical analysis, then executed by the randomise program. To compare intervention effect between the SAT and AET groups, we first calculated the pre-post difference images within each participant (e.g., post-intervention minus pre-intervention mean diffusivity images), then two-sample unpaired t-test was used to compare the SAT and AET groups. In addition, simple correlation analysis examined the association between individual changes in VO2peak and DTI metrics. For all TBSS analyses, multiple comparisons were corrected by threshold-free cluster enhancement with 5,000 permutations, then the corrected statistical maps were thresholded by p < 0.05. To confirm the TBSS results, we extracted the individual mean values of significant DTI metrics and plotted against VO2peak.
Statistical significance was set a priori at p < 0.05. For analysis of TRACULA output, significance levels for F-statistics were adjusted using the false discovery rate (q=0.05) for multiple tract comparisons. The outcome measurements are reported using mean and 95% confidence interval whereas demographic data are reported by mean and standard deviation. Statistical analyses were performed by SPSS 22 (IBM Corporation, Armonk, NY, 2011).
RESULTS
Participant characteristics were similar between the SAT and AET groups, including age, gender, education, MMSE scores, and VO2peak (Table 1). Also, the global measures of WM integrity, as assessed by WM lesion volume and DTI metrics, were similar between the groups (Table 2).
Baseline participant characteristics in the stretching-and-toning and aerobic exercise training groups
AET, aerobic exercise training; BMI, body mass index; MMSE, Mini-Mental State Exam; SAT, stretching and toning; VO2peak, peak oxygen uptake; SD, standard deviation.
Global white matter integrity measures at pre and post 1-year stretching-and-toning and aerobic exercise training programs
p < 0.05 are bolded. AET, aerobic exercise training; ANOVA, analysis of variance; AxD, axial diffusivity; FA, fractional anisotropy; G, group; MD, mean diffusivity; RD, radial diffusivity; SAT, stretching and toning; T, time; WM, white matter.
Intervention effect by AET and SAT groups
After 1 year, AET significantly improved VO2peak when compared with the SAT group (Fig. 1), regardless of using absolute (i.e., L/min) or relative units (i.e., ml/kg/min, % change). However, none of the global WM integrity measures showed the training effect specific to AET or SAT program (Table 2). In contrast, WM lesion volume increased over a year across all participants, and the TRACULA output also exhibited significant aging effects for elevated mean, axial, and radial diffusivity values measured from the forceps major, cingulum-angular bundle, inferior longitudinal fasciculus, and/or superior longitudinal fasciculus-temporal (Supplementary Tables 1–3). None of the fractional anisotropy measures showed significant age-related changes or exercise-related interaction effects (Supplementary Table 4). With respect to changes in cognitive function, letter fluency performance improved slightly within the AET group (Supplementary Table 5), but this change was small (∼1 point) and not likely clinically meaningful. No other cognitive measures showed any significant change in either intervention group, though many scores showed a slight improvement upon retest.
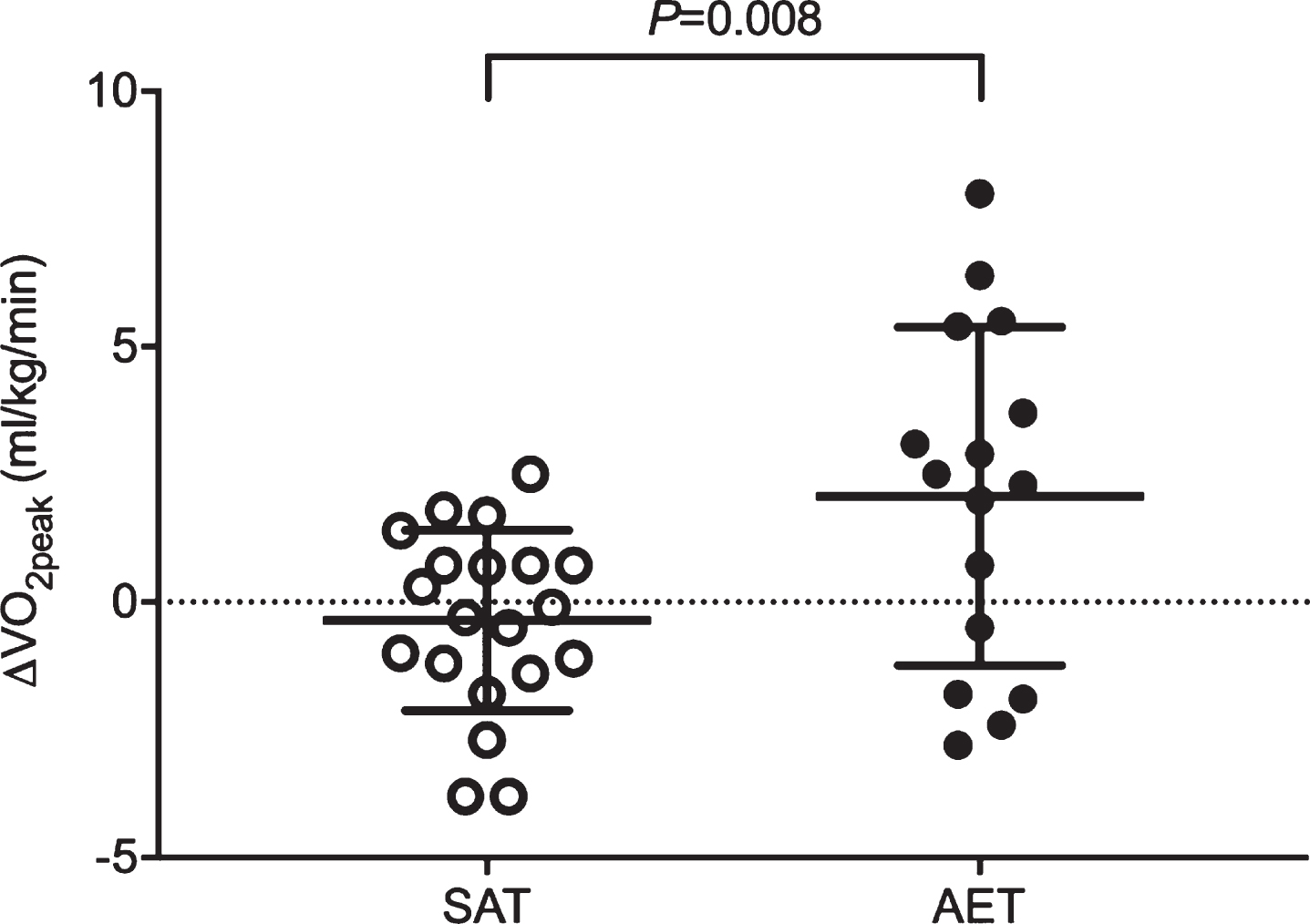
One-year changes in peak oxygen uptake (VO2peak) compared between the stretching and toning (SAT) and aerobic exercise training (AET) groups in patients with amnestic mild cognitive impairment.
Association with individual changes in VO2peak
After intervention, changes in VO2peak exhibited substantial individual variability within both AET and SAT groups (Fig. 1). This led us to the secondary analysis to examine the correlation of individual changes in VO2peak, DTI metrics, and cognitive performance. At the global level, individual improvements in VO2peak were associated with the reductions of axial diffusivity (r = -0.420, p=0.017) (Supplementary Table 6). The TRACULA output also showed a correlation between improved VO2peak and decreased mean diffusivity of the right anterior thalamic radiation (r = -0.487, p=0.0047).
TBSS analysis exhibited that increased VO2peak is negatively associated with decreased mean and axial diffusivities that accounted for ∼8% and ∼15% of the global WM skeleton voxels, respectively (Fig. 2A). Additionally, these significant mean and axial diffusivity voxels were spatially overlapped in most regions (Fig. 2B) and located in the anterior WM fiber tracts, including the genu of corpus callosum and the anterior corona radiata (Table 3). Moreover, we found strong correlations of the individual improvements in VO2peak with mean and axial diffusivity values that were extracted from the spatially overlapped significant regions (Fig. 3).
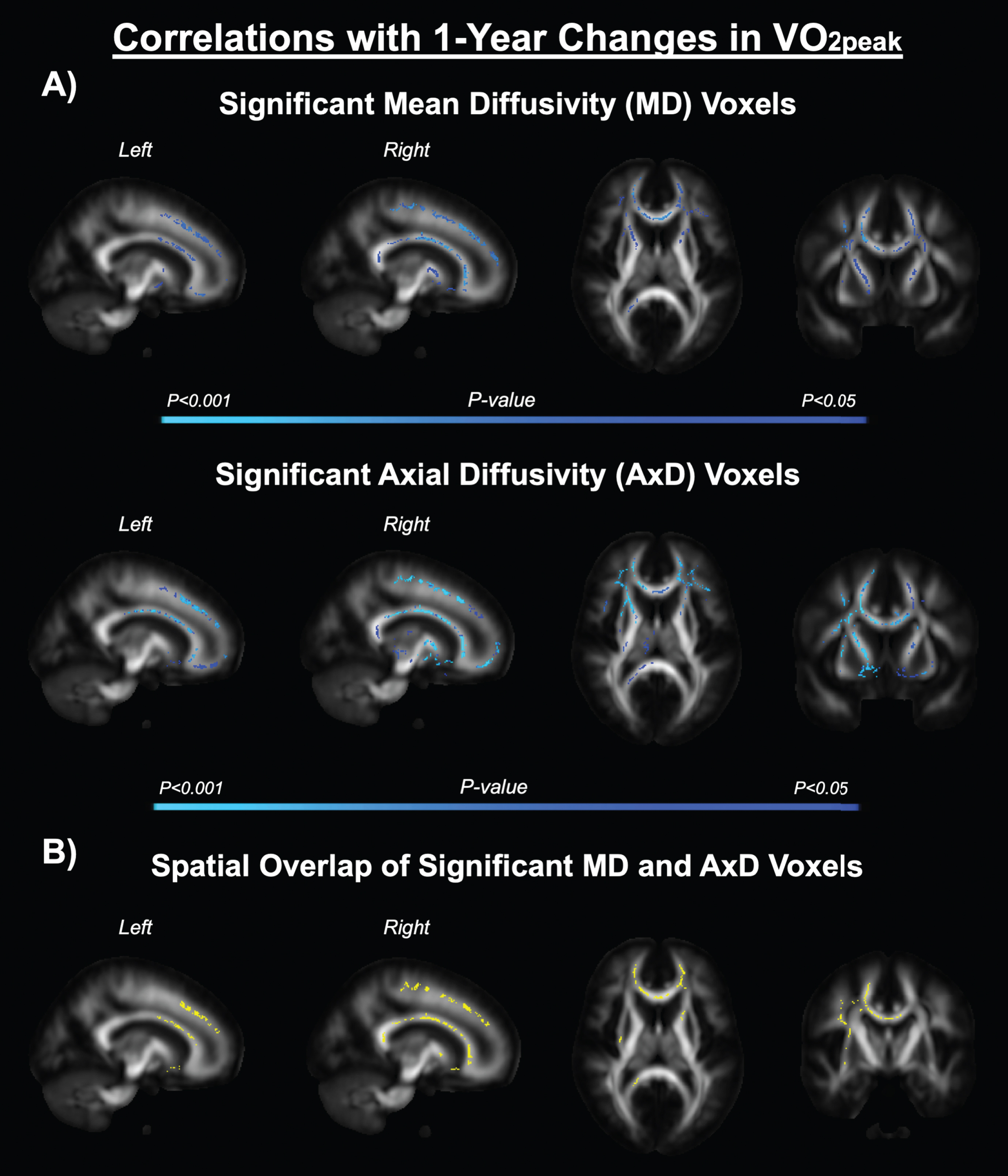
A) Tract-based spatial statistics (TBSS) results exhibiting the individual correlations between the 1-year changes in peak oxygen uptake (VO2peak) and mean and axial diffusivities across all participants. Statistically significant voxels are shown in blue. Color bars indicate p-value. B) Spatial overlap (yellow) of the significant mean and axial diffusivity voxels shown by A.
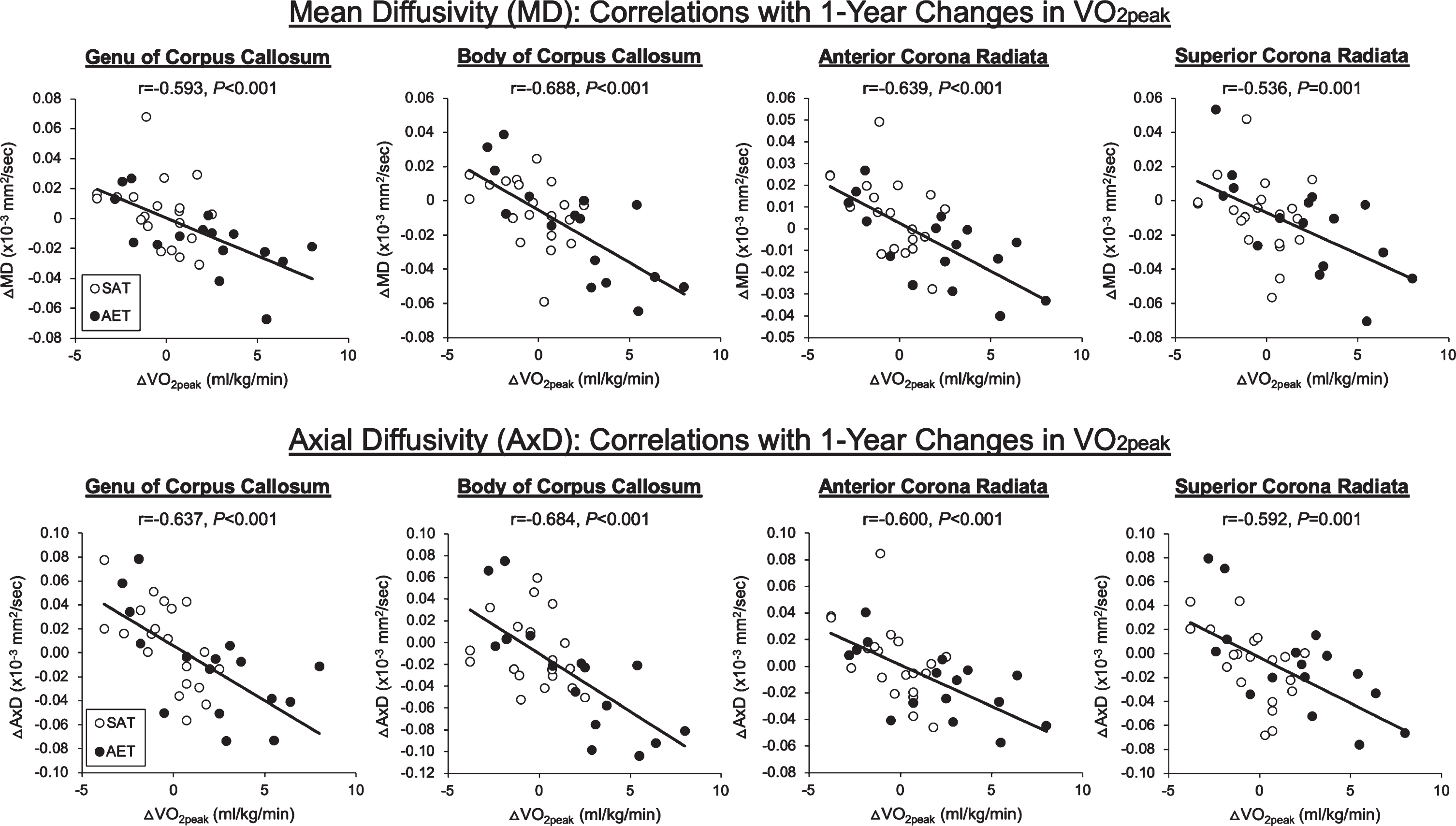
Simple correlations between the 1-year changes in peak oxygen uptake (VO2peak) and regional mean and axial diffusivities across all participants. The individual mean and axial diffusivity values were extracted from the areas shown by Fig. 2B. AET, aerobic exercise training group; SAT, stretching and toning group.
Anatomical location and the number (#) of significant voxels that are correlated with 1-year changes in cardiorespiratory fitness
The number of significant voxels were counted from the results of tract-based spatial statistic analysis shown by Fig. 2A and B. (%) represents the number of significant voxels relative to the entire size of white matter fiber tract. Each voxel is 1 mm3.
There were no significant correlations of any cognitive test scores with changes in VO2peak or WM integrity measures (data not shown).
Adverse events and training compliance
During the study, four adverse events occurred. During VO2peak testing, two had arrhythmia; during AET, one had ankle pain and another fell off the treadmill. The number of participants withdrawn or had adverse events was not different between the SAT and AET groups, however. The average compliance to intervention programs, as calculated by the ratio of prescribed exercise sessions over the actually completed sessions that participants achieved target heart rate, was 74%.
DISCUSSION
The main findings from this study are as follows. First, although AET program improved cardiorespiratory fitness when compared with the SAT group, no group differences in WM integrity and only slight improvements in cognitive performance were observed. Second, individual improvements in cardiorespiratory fitness were associated with the attenuated age-related deteriorations of WM integrity across the AET and SAT groups, particularly the anterior WM fiber tracts. These findings suggest that the magnitude of cardiorespiratory fitness gain is associated with regional improvement of WM integrity in patients with amnestic MCI.
What does this study add to the current literature?
According to a recent systematic review [33], most, if not all, of the previous investigations that examined the association of WM integrity with physical fitness or activity were cross-sectional and conducted in cognitively healthy adults. As an overall trend, these studies have shown weak correlations between global WM integrity and physical activity or fitness level. In contrast, voxelwise regional analysis (e.g., TBSS) revealed more consistent results that higher level of physical activity or fitness are correlated with better WM integrity in the prefrontal areas, including the genu of corpus callosum [33]. Consistent with these findings from cognitively healthy adults, we also reported from a cross-sectional study that higher VO2peak is associated with lower mean, axial, and radial diffusivities of the frontal WM fiber tracts in patients with amnestic MCI [10].
The current evidence available from interventional studies as to the effects of AET on WM integrity is limited to cognitively healthy adults and psychosis patients. Colcombe et al. demonstrated that 6 months of walking program increased prefrontal WM volume in cognitively healthy older adults when compared with control subjects assigned to stretching group [8]. Voss et al. conducted a 1-year RCT of walking versus stretching programs in cognitively normal older adults, and found positive correlations between individual changes in VO2peak and prefrontal fractional anisotropy within the walking group, although there was no group difference between the walking versus stretching groups after 1 year [9]. In another study that enrolled young and middle-aged healthy adults and schizophrenic patients, 6 months of cycling exercise was associated with increased fractional anisotropy of the motor-related WM fiber tracts in both participant groups when compared with the life-as-usual (control) group [34].
Accumulating evidence suggests that AET improves cognitive performance in healthy older adults [32, 36]. However, its effect for preventing or slowing cognitive decline in those who already have increased risks for developing AD dementia and other related dementias remains controversial. In this regard, the Agency for Healthcare Research and Quality recently reported that the current evidence is inconclusive to support the benefits of AET for preventing cognitive decline in patients with MCI or AD dementia [37]. Conversely, a high-intensity AET program showed the sex-specific benefits for improving executive function in amnestic MCI patients [38], suggesting that high intensity AET aiming to increase VO2peak may improve cognitive performance in MCI patients.
The findings from the current study are in large part consistent with previous studies suggesting that exercise-related improvement of WM integrity may depend on cardiorespiratory fitness gains, not necessarily participation in AET per se. Moreover, our findings add to the current literature that exercise training in amnestic MCI patients may preserve their brain neuronal plasticity via increased cardiorespiratory fitness [39], and protect them from the progressive deteriorations of neurocognitive function.
Methodological considerations
In this study, FLAIR and DTI data were collected to respectively examine macro- and micro-structural WM changes associated with exercise training and/or aging. To date, WM hyperintensity measured with FLAIR has frequently been used to assess WM abnormalities in old adults with normal or impaired cognitive function [40]. However, determination of WM hyperintensity with brain tissue segmentation is a dichotomous measurement and cannot provide mechanistic insights into microstructural damages. In contrast, DTI offers the ability to assess microstructural WM integrity in continuous scale which is made capable through quantifying a directionality and magnitude of water diffusion within the axonal fiber tracts [41]. Moreover, subtle WM abnormalities detected by DTI have been shown to precede the development of WM hyperintensities [42].
This study used two different methodological approaches to assess WM integrity (i.e., TBSS and TRACULA) and found consistent results indicating that improvements in cardiorespiratory fitness were associated with anterior mean and axial diffusivities over 1 year. The data analysis using TBSS and TRACULA is complementary. The former can detect brain areas that differ by group or intervention when individual DTI data are processed in standard space [23]. In contrast, the latter processes individual DTI data in native space; however, the calculated DTI metric values are averaged along the entire tract and may obscure potentially important information [22]. With these methods, TRACULA showed significant association between VO2peak and mean and axial diffusivities at the anterior thalamic radiation while TBSS showed similar associations at several prefrontal WM areas. Anatomically, the anterior thalamic radiations overlap with the areas detected by TBSS, including the anterior limb of internal capsule and the anterior corona radiata (Table 3); thus, we believe that the results from TRACULA and TBSS both support our hypothesis that improved cardiorespiratory fitness is associated with the prefrontal WM integrity. Furthermore, higher mean diffusivity reflects increased water diffusion in all directions, while higher axial diffusivity indicates increased diffusion parallel to a long axis of axonal fiber tracts [41]. In animal models, axial diffusivity has been shown to correlate with axonal damage [43]. Therefore, our results collectively suggest that cardiorespiratory fitness improvement is associated with attenuated axonal deterioration in the prefrontal WM tracts in amnestic MCI patients.
Nevertheless, caution should be taken when interpreting the results of DTI data. The typical voxel resolution of DTI is 2∼3 mm which can include hundreds of cerebral WM axons that, for example, are ∼1μm diameter in the human corpus callosum [44]. Also, their anatomical orientation, such as crossing fibers and diameter, could influence DTI metrics independent of fiber integrity [45]. Therefore, considering these potential limitations, we used TBSS which can analyze the center of WM tracts common to all subjects [23]. Also, the use of unbiased within-subject template through longitudinal FreeSurfer pipeline may have reduced the potential errors associated with data processing [20, 21].
In the current study, both AET and SAT (active control) groups performed exercise training. In this regard, our findings need to be interpreted carefully with the following considerations. First, it is possible that SAT altered WM integrity independent from the effect of AET. If true, SAT may have diluted the effects of AET on WM integrity. Second, no alterations in WM integrity over time may be explained by the potential benefits of AET and SAT that might have prevented age-related changes in WM integrity. Given these considerations, future research needs to incorporate control groups to isolate the effect of AET and to examine whether other modes of exercise, such as stretching or resistance exercise, can alter WM integrity.
Limitations and strengths
The findings from this proof-of-concept study should be interpreted within the context of following limitations. First, the sample size was small, though it was designed as a proof-of-concept study. Also, the attrition rate was high (∼31%) and MRI measurements were performed only in a subset of subjects, which may bias our results. Therefore, our findings need to be confirmed by future studies with larger samples. Second, although we observed a slight improvement on one cognitive task in the AET group, this change was minimal and there was no association between changes in WM integrity and cognitive function measures, which may limit clinical relevance of our findings. In our previous study, we showed cross-sectional associations among VO2peak, WM integrity measures, and cognitive performance [10]. However, it may be possible that structural changes in WM integrity associated with cardiorespiratory fitness improvement may require a longer time to have a meaningful impact on cognitive performance, or it may be that subgroups of subjects may experience cognitive enhancement while others do not. Third, although group-level analysis showed significant improvement of VO2peak after AET, there were a few participants who did not change or even decreased their cardiorespiratory fitness levels (Fig. 1). In this regard, non-responders have been a common finding in many exercise training studies which may be explained by individual genetic variability in response to exercise training [46], but the home-based exercise program we used in the current study may also have influenced participants’ adherence to the prescribed training dose. Therefore, future studies should be designed with the aim of maximizing gains in VO2peak, potentially with a more closely monitored exercise training program.
Despite limitations, this study has several important strengths. This is the first intervention study in MCI patients that investigated the effects of exercise training on WM integrity measurements, including WM lesion volume and diffusion characteristics. In addition, 1-year intervention programs offered a relatively long-time window to track age-related changes in these measurements. As a result, we observed age-related increases in mean and axial diffusivity which is consistent with previous reports that the former is sensitive to longitudinal changes in AD dementia and MCI patients [6]. Furthermore, the test-retest reliability of our WM measurements exhibited strong intra-class correlations which indicate the robustness of our imaging methods (Supplementary Figure 2). Last, VO2peak provided an objective measure of improved cardiorespiratory fitness [47], and unbiased criteria to monitor the improvement of physical fitness in previously sedentary MCI patients.
Conclusions
We found that 1) AET intervention increased participants’ VO2peak, but not their WM integrity or cognitive performance at the group level and 2) individual improvements in VO2peak, independent of the intervention applied, were associated with the attenuated age-related deteriorations of WM integrity in amnestic MCI patients, particularly the anterior WM fiber tracts. These findings are in large part consistent with the mounting evidence that improved cardiovascular health with physical exercise training can help prevent or slow age-related brain structural changes in older adults.