
Abstract
Background:
Recent studies have shown that amyloid-β (Aβ) burden influenced white matter (WM) integrity before the onset of dementia.
Objective:
To assess whether the effects of Aβ burden on WM integrity in cognitively normal (CN) individuals were regionally specific.
Methods:
Our cohort consisted of 71 CNs from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database who underwent both AV45 amyloid-PET and diffusion tensor imaging. Standardized uptake value ratio (SUVR) was computed across four bilateral regions of interest (ROIs) corresponding to four stages of in vivo amyloid staging model (Amyloid stages I–IV). Linear regression models were conducted in entire CN group and between APOE ɛ4 carriers and non-carriers.
Results:
Our results indicated that higher global Aβ-SUVR was associated with higher mean diffusivity (MD) in the entire CN group (p = 0.023), and with both higher MD (p = 0.015) and lower fractional anisotropy (FA) (p = 0.026) in APOE ɛ4 carriers. Subregion analysis showed that higher Amyloid stage I-II Aβ-SUVRs were associated with higher MD (Stage-1: p = 0.030; Stage-2: p = 0.016) in the entire CN group, and with both higher MD (Stage-1: p = 0.004; Stage-2: p = 0.010) and lower FA (Stage-1: p = 0.022; Stage-2: p = 0.014) in APOE ɛ4 carriers. No associations were found in APOE ɛ4 non-carriers and in Amyloid stage III-IV ROIs.
Conclusions:
Our results indicated that the effects of Aβ burden on WM integrity in CNs might be regionally specific, particularly in Amyloid stage I-II ROIs, and modulated by APOE ɛ4 status.
INTRODUCTION
Amyloid-β (Aβ) deposition in Alzheimer’s disease (AD) can be detected by amyloid PET preceding the onset of cognitive decline by several decades [1, 2]. In addition, diffusion tensor imaging (DTI) studies demonstrate loss of white matter (WM) integrity in AD starting from the preclinical phase [3–7]. Increased mean diffusivity (MD) and decreased fractional anisotropy (FA) on DTI are regarded as biomarkers reflecting the loss of axons and myelin in the WM [8, 9]. Previous studies have investigated the relationships between Aβ deposition and WM integrity in the preclinical phase of AD. In a cohort of non-demented elders, two studies reported similar findings that subjects with lower cerebrospinal fluid (CSF) Aβ level showed higher MD and lower FA on DTI [10, 11].
Since the CSF levels of Aβ failed to show spatial difference of Aβ deposition, subsequent researches have examined the relationships between neuroimaging of Aβ deposition and WM integrity using amyloid PET [12, 13]. However, results have been inconsistent. For instance, one study found that an increase of neocortical Aβ burden assessed by amyloid PET was associated with an increase of MD in cognitive normal (CN) adults [12], whereas another study failed to find such an effect when assessing global Aβ level that are commonly used for classifying subjects into Aβ-positive or negative [13]. Based on these findings, we hypothesized that the associations between Aβ load and WM integrity in the asymptomatic phase of AD would be regionally specific.
Up to now, both autopsy [14–16] and PET [17] evidence have suggested that the ordering of regional Aβ deposition followed a relatively consistent pattern. The deposition of Aβ plaques starts from the basal temporal and medial frontal cortices, then spreads to the rest of associative neocortices, primary sensory-motor regions and medial temporal areas, and lastly the striatum. Grothe et al. defined these brain regions as Amyloid stages I, II, III, and IV, respectively [18]. Of the regions mentioned as showing loss of WM integrity in persons with Aβ accumulation, the neocortices are most relevant [12, 19], which are the first to develop Aβ pathology and correspond to Amyloid stages I and II [18].
In our study, we investigated the possible associations between Aβ deposition assessed by AV45 amyloid PET and WM microstructure assessed by DTI in cognitively normal (CN) individuals from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database. We assessed regional Aβ deposition in those brain regions, which are known to show increased susceptibility to Aβ pathology as defined by the in vivo established Amyloid staging model [18]. We hypothesized that the possible associations between high Aβ load and loss of WM integrity only existed in those neocortical regions corresponding to Amyloid stages I and II. Furthermore, we explored whether the possible associations were influenced by APOE genotypes.
MATERIALS AND METHODS
Study subjects and ADNI database
All participants recruited in our study were from the ADNI (ADNI-2 and ADNI-GO) cohort. The ADNI was a public-private partnership, which was led by principal investigator Michael W. Weiner, MD. Established in 2003, the ADNI aims to track the progression of mild cognitive impairment (MCI) and early AD using PET, magnetic resonance imaging (MRI), other biological markers, as well as neuropsychological and clinical assessment. Till now, the ADNI database has recruited over 1,500 individuals from no less than 50 sites across Canada and America. All participants provided written informed consent. More information can be found at http://www.adni-info.org. In our study, we restricted the present analyses to CN individuals whose data of AV45 amyloid-PET, DTI, WM hyperintensities (WMH) volume, and APOE genotype were available. Detailed descriptions of inclusion and exclusion criteria for CN individuals have been reported previously [20, 21]. Briefly, subjects were clinically categorized by ADNI centers as CN with a Mini-Mental State Examination (MMSE) scores of 24–30 where lower scores suggest more cognitive impairment (range, 0–30), and a Clinical Dementia Rating (CDR) score of 0 where lower scores indicate less cognitive impairment (range, 0–3). Subjects were assigned to the APOE ɛ4 carriers when carrying at least one APOE ɛ4 allele. Finally, our study recruited 71 CN individuals, including 23 APOE ɛ4 carriers and 48 APOE ɛ4 non-carriers at baseline (Table 1).
Subject disposition and demographic characteristics
Data are given as mean±standard deviation unless otherwise indicated. CN, cognitively normal individuals; APOE, Apolipoprotein. The differences in demographic characteristics between APOE ɛ4 carriers and APOE ɛ4 non-carriers were tested using t tests for continuous variables and Chi-squared tests for dichotomous variables. Bold text indicates p < 0.05.
DTI data
DTI data was downloaded from the ADNI database. A detailed description of DTI image acquisition and processing can be found at http://adni.loni.usc.edu/datasamples/mri/. In brief, to segment WM regions of interest (ROIs), the FA image from the Johns Hopkins University (JHU) DTI atlas [22] was registered to each subject using mutual information based elastic registration algorithm which was described previously [23]. Then, the deformation was applied to the stereotaxic JHU “Eve” WM atlas labels using nearest neighbor interpolation to avoid intermixing of labels. This placed the atlas ROIs in the same coordinate space as our DTI maps. Finally, fifty-two WM ROIs were determined by the JHU white-matter tractography atlas. A list of the fifty-two WM ROIs can be found in Supplementary Table 1. For MD and FA on DTI are widely used biomarkers of WM integrity [8, 9], we computed average MD and FA values of the fifty-two WM ROIs for each individual as global MD and global FA, which represent the level of global WM microstructure.
AV45 amyloid-PET data
AV45 amyloid-PET data was also downloaded from the ADNI database. A detailed description of PET image acquisition and processing can be found at http://adni.loni.usc.edu/datasamples/pet/. In our study, we assessed global and regional AV45 amyloid-PET levels separately. Firstly, we averaged Aβ tracer uptake across four cortical regions (frontal, anterior/posterior cingulates, lateral parietal, lateral temporal) as global Aβ load that are commonly used for classifying subjects into Aβ-positive or negative [24]. And then we applied a recently proposed in vivo staging system of regional amyloid [18], that suggests Aβ deposition initiates in the basal temporal and medial frontal cortices (Amyloid stage I), then spreads to the rest of associative neocortices (Amyloid stage II), primary sensory-motor regions and medial temporal areas (Amyloid stage III), and lastly the striatum (Amyloid stage IV) [18]. We chose four brain regions corresponding to Amyloid stages I–IV as ROIs (shown in Fig. 1). We averaged Aβ tracer uptake across brain regions that are included within each Amyloid stage ROI as stage-specific regional Aβ load. A list of brain regions that are included within each Amyloid stage ROI can be found in Supplementary Table 2. Finally, these mean values were normalized to the eroded WM reference region to obtain global and regional SUVR scores. The reason for choosing the eroded WM as a reference region was that reference regions containing subcortical eroded WM in cross-sectional studies appeared to be more accurate and sensitive when compared to cerebellum [25–29], and a recent study showed that WM Aβ tracer uptake may be an early predictor of WM microstructure [30].
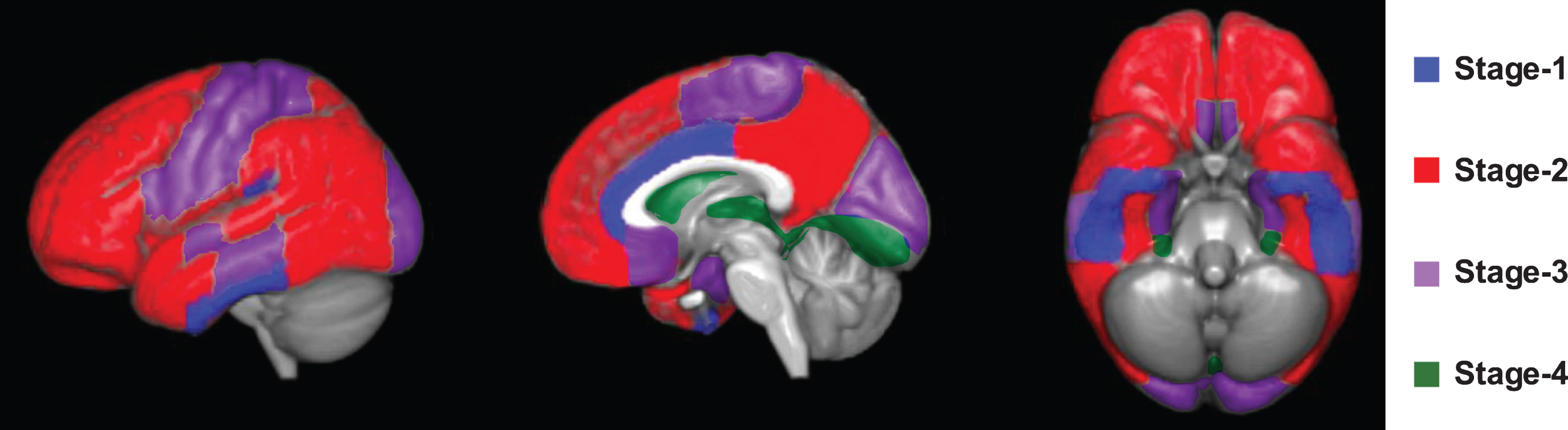
Staging systems for amyloid-PET. Spatial mapping of amyloid stage-specific ROIs that were used to determine regional AV45 amyloid-PET uptake.
Statistical analysis
We tested the differences in demographic characteristics between APOE ɛ4 carriers and APOE ɛ4 non-carriers using t tests for continuous variables and Chi-squared tests for dichotomous variables. We evaluated whether increased global or regional (i.e., four ROIs corresponding to Amyloid stages I–IV) AV45 amyloid-PET SUVRs were associated with the loss of WM integrity (i.e., global MD or global FA) using linear regression models, controlling for age, gender, educational level, and APOE ɛ4 status (Model 1). To test whether the above associations were independent of WMH volume, we further included WMH volume as a covariate (Model 2). Considering that the accurate definition of a clinically meaningful cutoff value of SUVR in CN population remains unclear [31, 32] and using different cutoff values of SUVR may result in different findings [33], our study treated the level of Aβ deposition as a continuous variable. MD, FA, and AV45 amyloid-PET SUVR scores were log transformed prior to this analysis in order to approximately fit the normal distribution. Both the log-transformed independent and dependent variables in linear regression models were converted into normalized z scores. Estimated effects of AV45 amyloid-PET SUVR on WM integrity are reported as β coefficients. Since all outcome variables were converted into normalized z scores, β coefficients refer to standardized effects. All statistical analyses were performed using a software program (R, version 3.6.0; The R Foundation). The criterion for statistical significance was p < 0.05. We did not correct for multiple comparisons because we expected to see differences only in ROIs affected at early Amyloid stages and included later-stage ROIs as control regions.
RESULTS
A total of 71 CN individuals were enrolled in our study, 40 of them were women and 31 of them were men. The mean age and education level of the entire CN cohort was 72.82±5.59 and 16.37±2.70 years, respectively (see Table 1 for sample characteristics). Of the total, 48 had no APOE ɛ4 allele, 22 had one, and 1 had two alleles. Subjects with at least one copy of the APOE ɛ4 allele were categorized as APOE ɛ4 carriers, and the others were classified into non-carriers. APOE ɛ4 non-carriers with a mean age of 73.77±6.08 years were older than carriers with a mean age of 70.82±3.79 years (p < 0.05). No statistical differences in gender, education, and WMH volume were found between this two groups (p > 0.05).
In a first step, we tested the hypothesis that the increased Aβ deposition would be associated with the loss of WM integrity. We averaged Aβ tracer uptake across four cortical regions (frontal, anterior/posterior cingulates, lateral parietal, and lateral temporal) as global Aβ load that are commonly used for classifying subjects into Aβ-positive or negative [24]. Our results indicated that higher global AV45 amyloid-PET SUVR was associated with higher MD in the entire CN group (p = 0.023), and with both higher MD (p = 0.015) and lower FA (p = 0.026) in APOE ɛ4 carriers when testing via linear regression models controlled for age, gender, education, and APOE ɛ4 genotype (see model 1 in Table 2). To test whether the above associations were independent of WMH volume, we further included WMH volume as a covariate and the results did not alter (see model 2 in Table 2).
Aβ, amyloid-β; APOE, Apolipoprotein; SUVR, standard uptake value ratio; WM, white matter. Model 1: p-values are based on linear regression models controlled for age, gender, education, and APOE ɛ4 genotype. Model 2: p-values are based on linear regression models controlled for age, gender, education, APOE ɛ4 genotype, and WMH volume. Bold text indicates p < 0.05.
We next tested whether the effects of Aβ deposition on WM integrity were regionally specific. For this, we assessed the AV45 amyloid-PET SUVR within four brain regions corresponding to Amyloid stages I–IV (Fig. 1) that recapitulate the spatial Aβ-spreading pattern from early-to-late-stage Aβ pathology [18]. The subregion analysis showed that the above positive findings only existed within regions corresponding to Amyloid stages I-II, which indicated that the higher regional AV45 amyloid-PET SUVRs in stage-1 and stage-2 ROIs were associated with higher MD (Stage-1: p = 0.030; Stage-2: p = 0.016) in the entire CN group, and with both higher MD (Stage-1: p = 0.004; Stage-2: p = 0.010) and lower FA (Stage-1: p = 0.022; Stage-2: p = 0.014) in APOE ɛ4 carriers when controlling for age, gender, education, and APOE ɛ4 genotype (see model 1 in Table 2). When additionally controlling for WMH volume, these above associations remained fully consistent again (see model 2 in Table 2).
There were no significant associations in APOE ɛ4 non-carriers or in regions corresponding to Amyloid stages III-IV. The associations of global and regional Aβ deposition with MD and FA were shown in Figs. 2 and 3, respectively. Detailed β coefficients and p-values in total CN group including APOE ɛ4 carriers and APOE ɛ4 non-carriers were listed in Table 2.
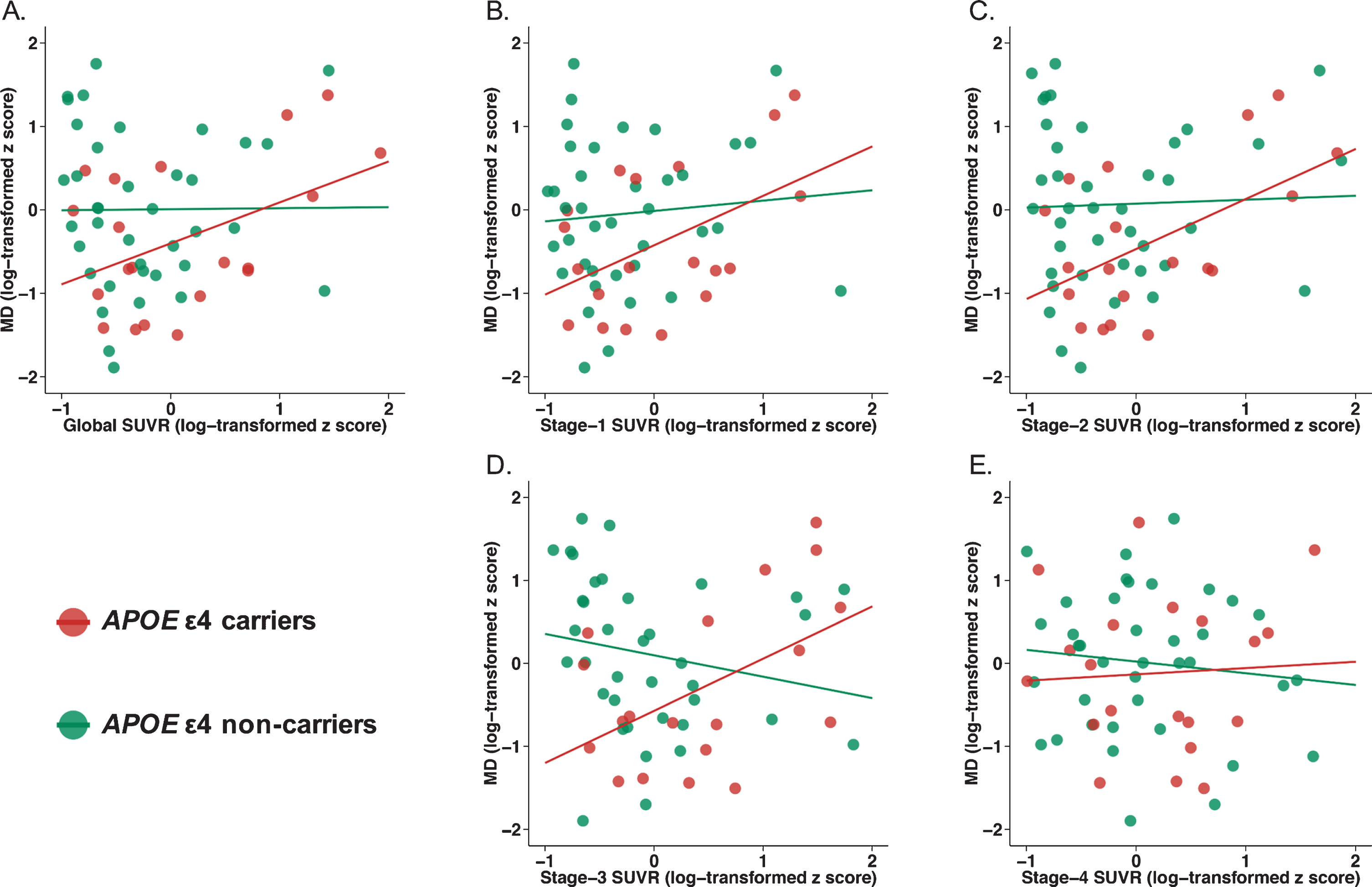
Associations of global and regional Aβ burden with MD assessed by DTI. Global and regional (i.e., four ROIs corresponding to Amyloid stages I–IV) AV45 amyloid-PET SUVRs for each subject were plotted on the X axis, and MD for each subject assessed by DTI was plotted on the Y axis. AV45 amyloid-PET SUVR scores and MD were log transformed prior to this analysis in order to approximately fit the normal distribution. Both the log-transformed independent and dependent variables in linear regression models were converted into normalized z scores. The regression line is drawn separately for APOE ɛ4 carriers and APOE ɛ4 non-carriers for ease of comparison. Aβ, amyloid-β; ROI, region of interest; SUVR, standard uptake value ratio.
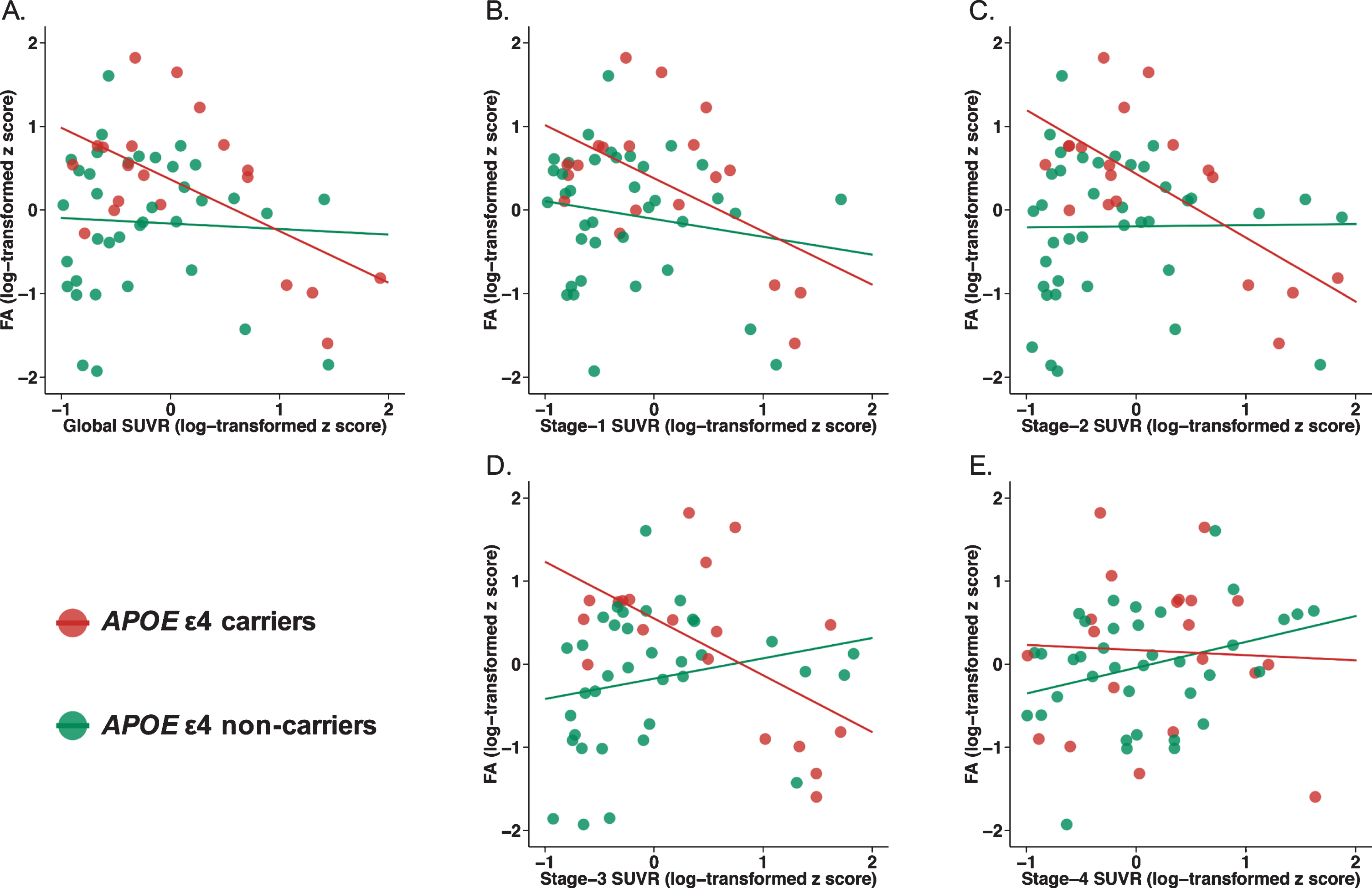
Associations of global and regional Aβ burden with FA assessed by DTI. Global and regional (i.e., four ROIs corresponding to Amyloid stages I–IV) AV45 amyloid-PET SUVRs for each subject were plotted on the X axis, and FA for each subject assessed by DTI was plotted on the Y axis. AV45 amyloid-PET SUVR scores and FA were log transformed prior to this analysis in order to approximately fit the normal distribution. Both the log-transformed independent and dependent variables in linear regression models were converted into normalized z scores. The regression line is drawn separately for APOE ɛ4 carriers and APOE ɛ4 non-carriers for ease of comparison. Aβ, amyloid-β; ROI, region of interest; SUVR, standard uptake value ratio.
DISCUSSION
Here, we adopted a hierarchical model of in vivo amyloid staging proposed by Grothe and colleagues [18] and applied it to explore possible associations of Aβ deposition assessed by AV45 amyloid-PET with WM microstructure assessed by DTI in a cohort of CN individuals from the ADNI database. Our results indicated that: 1) the effects of Aβ load on WM integrity were regionally specific: basal temporal and medial frontal cortices, and the remaining associative neocortices (Amyloid stage I-II), which were the first to develop Aβ pathology, showed greater effects than primary sensory-motor regions and medial temporal areas, and the striatum (Amyloid stage III-IV), which only accrued Aβ plaques during symptomatic phase of AD; and 2) the aforementioned effects only existed in APOE ɛ4 carriers, which indicated that the effects of Aβ load on WM integrity were modulated by APOE ɛ4 status.
Our results provided supportive evidence for recent findings, which demonstrated that increased Aβ load was associated with the loss of WM integrity before the onset of dementia [10–13]. A preliminary study by Kalheim et al. compared subjects with low (Aβ positive) and normal CSF Aβ (Aβ negative) in a cohort of non-demented elders consisting of MCI or subjective cognitive decline (SCD) and found that increased MD in subjects with low CSF Aβ [10]. Another study compared FA on DTI between subjects with higher Aβ load (Aβ positive, Amyloid PET SUVR > 1.69) and subjects with lower Aβ load (Aβ negative, Amyloid PET SUVR < 1.40) in a cohort of non-demented elders consisting of CN and MCI subjects. They found that higher Aβ burden was associated with lower FA in the presence of neurodegeneration (by hippocampal atrophy on MRI and hypometabolism on fluorodeoxyglucose PET) [13]. However, previous studies grouped participants into “Aβ positive” and “Aβ negative” based on CSF Aβ level or global Aβ deposition on amyloid PET [10, 13], which might fail to explore whether the effects of Aβ load on WM integrity showed regional differences. In addition, since conventionally defined “Aβ positive” usually corresponds to relatively late stages of Aβ pathology [31, 34], previous studies [10, 13] might fail to explore the potential associations between early stages of Aβ pathology and WM integrity.
In our study, we treated the level of Aβ deposition as a continuous variable, considering that the accurate definition of a clinically meaningful cutoff value of SUVR in CN population remains unclear [31, 32] and using different cutoff values of SUVR might result in different findings [33]. Compared with previous studies, our study could detect the early stages of Aβ pathology below the threshold of conventionally defined “Aβ positive” by treating the level of Aβ load as a continuous variable.
We explored whether the potential associations between Aβ load and WM integrity showed regional differences by assessing regional AV45 amyloid-PET SUVR within four brain regions that recapitulate the spatial Aβ-spreading pattern from early-to-late-stage Aβ pathology [18]. Our results indicated that the higher regional AV45 amyloid-PET SUVRs in stage-1 and stage-2 ROIs were associated with higher MD in the entire CN group, and with both higher MD and lower FA in APOE ɛ4 carriers. We selected later-stage ROIs (Amyloid stage III-IV) as control regions and did not find any associations between Aβ load and WM integrity in stage-3 and stage-4 ROIs. Although the p-value of stage-3 SUVR in the regression model regarding MD for the APOE ɛ4 carriers subgroup approached the significance level (p = 0.065), we did not find any associations between stage-3 SUVR and MD/FA in the entire CN group and the association between stage-3 SUVR and MD in the APOE ɛ4 carriers subgroup also failed to achieve the significant level (p < 0.05). These findings suggested that the associations between Aβ load and WM integrity in brain regions corresponding to Amyloid stages I-II were more significant than those in brain regions corresponding to Amyloid stages III-IV. The results were also in agreement with previous reports that Aβ deposition in neocortices, which correspond to Amyloid stages I-II, was associated with WM integrity in CN individuals [12, 19]. Since Amyloid stages I-II ROIs in vivo correspond to Thal amyloid phase 1 at autopsy [14], the similar findings in our study and previous studies [12, 19] suggested that the associations between Aβ accumulation and WM integrity starting from a very early stage and WM integrity assessed by DTI may be an early marker of Aβ pathology. We restricted the present analyses to CN individuals, whereas Aβ deposition in regions corresponding to Amyloid stages III-IV started from symptomatic phase of AD, which led to reduced variability in AV45 amyloid-PET levels in these brain regions and might be the reason for the negative results. Additionally, the results of our study were required based on rather small sample size, which might attribute to the negative results as well. In our study, the p-value of stage-3 SUVR regarding MD approached the significance level. Future studies with larger sample size are needed to explore the effect of Aβ deposition in later-stage ROIs (Amyloid stage III-IV) on WM integrity in a mixed population consisting of CN, MCI and AD patients. The association between Stage-3 SUVR and MD/FA may be stronger on a larger cohort.
Our second major finding was that increasing Aβ load in early Aβ-associated brain regions, occurred only in APOE ɛ4 carriers. We therefore hypothesized that the effect of Aβ load on WM integrity was modulated by APOE ɛ4 status. This was consistent with the findings of recent studies exploring the effects of APOE ɛ4 alleles on WM integrity. A study by Lee et al. found that APOE ɛ4 carriers showed lower FA values in a cohort of SCD when compared with non-carriers [35]. Another study by Williams et al. [36] examined the interactive effects of vascular burden and APOE ɛ4 status on WM integrity in CN elders and found APOE ɛ4 carriers had greater decline in FA when compared to non-carriers. Given the small sample size of our study, the significant associations should be interpreted cautiously.
The above findings did not alter when additionally controlling for WMH volume, suggesting that the associations between Aβ load and WM integrity were independent of WMH volume. Recent studies have indicated that small vessel disease (SVD) may play an important role in the pathology of AD [37, 38], and SVD mainly affects subcortical WM. For WMH were often thought to be one of markers of SVD [39], we hypothesized that the effects of Aβ load on WM integrity might be independent of SVD. However, WMH are only one aspect of SVD, and many other manifestations are often detected in patients with SVD (e.g., cerebral microbleeds and lacunar cerebral infarction). Future studies are needed to determine whether the relationships between Aβ load and WM integrity are mediated by SVD.
Limitations
The present study has some limitations. Firstly, the sample size of the study was rather small, which may reduce the testing efficiency of whole and subgroup analyses to some extent. Secondly, majority participants in our study were relatively old (mean age: 72.82 years). Previous study indicated that middle-aged adults may be an optimal target for early intervention. However, it remains unclear whether Aβ deposition is associated with WM integrity in middle-aged adults. Thirdly, as a cross-sectional study, we did not detect longitudinal associations between Aβ load and WM integrity. Finally, the p values in our study were just on the significant edge and the associations may be stronger on a larger cohort. There is a need to conduct a follow-up study with larger sample size and broader age range in the future.
Conclusions
In summary, the main finding of our current study was that increased Aβ load in basal temporal and medial frontal cortices, and the remaining associative neocortices (Amyloid stage I-II) might be associated with the loss of WM integrity in absence of cognitive impairment. The effects were more obvious with the presence of APOE ɛ4 alleles.
Footnotes
ACKNOWLEDGMENTS
This study was supported by grants from the National Natural Science Foundation of China (91849126, 81571245, and 81771148), the National Key R&D Program of China (2018YFC1314700), Shanghai Municipal Science and Technology Major Project (No.2018SHZDZX01) and ZHANGJIANG LAB, Tianqiao and Chrissy Chen Institute, and the State Key Laboratory of Neurobiology and Frontiers Center for Brain Science of Ministry of Education, Fudan University. Data collection and sharing for this project was funded by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). Data used in the preparation for this article were derived from the ADNI database (http://adni.loni.usc.edu/). The authors express appreciation to contributors of Alzheimer’s Disease Neuroimaging Initiative (ADNI) database. ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (![]() ). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.