
Abstract
Background:
Perioperative neurocognitive disorders (PND) are common complications in older adults associated with increased 1-year mortality and long-term cognitive decline. One risk factor for worsened long-term postoperative cognitive trajectory is the Alzheimer’s disease (AD) genetic risk factor APOE4. APOE4 is thought to elevate AD risk partly by increasing neuroinflammation, which is also a theorized mechanism for PND. Yet, it is unclear whether modulating apoE4 protein signaling in older surgical patients would reduce PND risk or severity.
Objective:
MARBLE is a randomized, blinded, placebo-controlled phase II sequential dose escalation trial designed to evaluate perioperative administration of an apoE mimetic peptide drug, CN-105, in older adults (age≥60 years). The primary aim is evaluating the safety of CN-105 administration, as measured by adverse event rates in CN-105 versus placebo-treated patients. Secondary aims include assessing perioperative CN-105 administration feasibility and its efficacy for reducing postoperative neuroinflammation and PND severity.
Methods:
201 patients undergoing non-cardiac, non-neurological surgery will be randomized to control or CN-105 treatment groups and receive placebo or drug before and every six hours after surgery, for up to three days after surgery. Chart reviews, pre- and postoperative cognitive testing, delirium screening, and blood and CSF analyses will be performed to examine effects of CN-105 on perioperative adverse event rates, cognition, and neuroinflammation. Trial results will be disseminated by presentations at conferences and peer-reviewed publications.
Conclusion:
MARBLE is a transdisciplinary study designed to measure CN-105 safety and efficacy for preventing PND in older adults and to provide insight into the pathogenesis of these geriatric syndromes.
Keywords
INTRODUCTION
Postoperative cognitive dysfunction (POCD; also known as neurocognitive disorder-postoperative, or NCD) and delirium each occur in up to 40% of the≥16 million adults age≥60 who undergo surgery each year, and both are associated with decreased quality of life, increased one-year mortality, and a possible increased dementia risk [1 –7]. Mild NCD refers to a 1 or 2 standard deviation cognitive decline (either from before to after surgery, or in comparison to population norms) that occurs between 1–12 months after surgery, coupled with either a subjective cognitive complaint (for mild NCD) or inability to care for oneself (NCD major) [8]. These perioperative neurocognitive disorders [8] (PND) pose a mounting public health concern as increasing numbers of older adults undergo surgery [1]. While there are several behavioral interventions such as the Hospital Elder Life Program (HELP) [9] and the ABCDEF bundle [10] that have demonstrated efficacy for reducing delirium incidence, there are no currently FDA-approved drugs for preventing delirium or other types of PND, likely due to our poor understanding of their pathogenesis.
Two mechanisms hypothesized to underlie PND are neuroinflammation and exacerbation of pre-existing Alzheimer’s disease (AD) pathology. The role of neuroinflammation in PND is supported by animal studies revealing postoperative increases in brain inflammatory cytokines [11] and microglial activation [12], and human studies demonstrating postoperative cerebrospinal fluid (CSF) inflammatory cytokine increases [13 –15]. Further, some surgical patients display postoperative increases in blood and CSF tau and amyloid-β (Aβ) levels and the tau/Aβ ratio [14, 16], similar to alterations seen in patients with AD [17 –19]. Low preoperative CSF and plasma Aβ levels and elevated preoperative CSF tau/Aβ have also been associated with increased POCD incidence [18, 20] and severity [21], respectively. Thus, AD neuropathology increases PND risk, and PND may be associated with postoperative worsening of AD pathology. Additionally, the relationship between AD pathology and neuroinflammation is complex: neuroinflammation plays both pathogenic and protective roles in AD [22 –24], and may interact with AD pathology in PND pathogenesis, suggesting an ideal PND prevention drug may need to act on both of these processes.
One potential target implicated in both neuroinflammation and AD pathology is the late-onset AD genetic risk factor APOE4 [25], whose protein product apoE4 increases glial activation and pro-inflammatory cytokine levels in animal models [26 –29]. Human APOE4 carriers have elevated systemic IL-1β, IL-6, and TNFα levels and increased postoperative IL-1β levels [30, 31], increased Aβ and tau pathology [32, 33], and have worsened long term cognitive trajectories after surgery [34, 35]. In murine models, blocking apoE4 with the apoE mimetic peptide drug CN-105 reduced neuroinflammation and improved cognitive, neurobehavioral, and motor outcomes in traumatic brain injury, ischemic stroke, and cerebral hemorrhage models [36 –38]. Additionally, a phase I trial found that CN-105 was safe at doses up to 20 times greater than those given in preclinical studies, with no serious adverse events (SAEs) [39]. Based on these data, we hypothesize that CN-105 will be safe and effective for preventing PND in older adults. Thus, we have initiated MARBLE, a phase II randomized controlled trial (RCT) to determine the safety, feasibility, and efficacy of perioperative CN-105 treatment in older surgical patients at risk for PND.
METHODS
Overview
MARBLE is a phase II escalating dose RCT that is registered with clinicaltrials.gov (NCT03802396). Since the MARBLE study drug (CN-105) was developed and patented by Duke University, MARBLE is overseen by an external IRB (Western Institutional Review Board) and monitored by an external Data and Safety Monitoring Board (DSMB+) comprised of five investigators external to Duke with no COI relative to CN-105 or AegisCN. In line with NIH recommendations, every attempt is being made to enroll a diverse group of study patients, in terms of race and ethnicity, as well as socioeconomic status in the MARBLE study, such that the results will be as broadly generalizable to the larger population of older adults as possible.
Eligibility
MARBLE has currently enrolled 40 of its 201-patient target. Inclusion criteria are: English-speaking, age≥60 years old, and scheduled to undergo non-cardiac/non-neurologic surgery of≥2 h with a planned postoperative hospital admission at Duke University Hospital. Duke University Hospital is a tertiary care academic medical center. Eligible patients are informed about the study via brochures (distributed to the preoperative screening and surgical clinics), phone calls as well as electronic messages sent to their online medical charts in accord with Duke’s patient recruitment and engagement policy for clinical research [40]. Exclusion criteria include incarceration, planned systemic chemotherapy between the baseline and 6-week postoperative study visits, and inability to undergo lumbar punctures (LPs), e.g., due to anticoagulation [41]. There are no preoperative cognitive exclusion criteria; secondary analyses will be performed on patients stratified by preoperative cognitive function. Participants who undergo significant head trauma between the baseline and 6-week postoperative study visits will be withdrawn from the study due to the confounding effects of head trauma on cognition. Written informed consent is obtained from all patients or their legally-authorized representatives before participation.
Study intervention
After enrollment, participants are randomized to receive CN-105 or placebo at a 3 : 1 ratio. There are three successive escalating dose groups of 67 patients; in each group, 50 patients receive CN-105 and 17 receive placebo. CN-105 dosage is 0.1 mg/kg, 0.5 mg/kg, and 1 mg/kg in the three groups, respectively. After complete enrollment for each dose level, the DSMB+ reviews the data and makes a recommendation (based on safety data in that dose level) for whether the study should be stopped or not. For each patient, CN-105 or placebo is given by intravenous infusion within 1 h before the scheduled or actual surgery start and then every 6 h±90 min after the start of surgery. Patients continue receiving drug (or placebo) until discharge orders are placed or until three days after surgery, whichever occurs first, for up to 13 doses per patient. The participants, study team, and hospital nurses are blinded to treatment randomization (i.e., to active drug versus placebo), thus the study is triple blinded. Randomization is tracked by the Duke hospital investigational drug service, and was designed electronically by an independent staff statistician.
Safety and feasibility assessments
Safety of perioperative CN-105 administration is assessed by AE rates in drug versus placebo-treated patients. Common terminology for classifying adverse events (CTCAE) criteria are used to assess and classify SAEs and AEs [42]. AEs are monitored by study staff that review participants’ clinical records, and by noting any symptoms reported directly by the participants to the study staff. All SAEs, even if unrelated to the intervention, are reported to the IRB in accordance with IRB and DSMB-designated reporting schedules. Since inflammation plays a role in both wound healing and postoperative infections, and CN-105 has been shown to modulate inflammation in animal studies [38], particular attention is payed to assessing for infection or delayed wound healing as AEs. As discussed above, our DSMB reviews the unblinded AE rate information after the enrollment of each 67-patient group (50 patients who receive drug, 17 who receive placebo), and then decides whether the study should be stopped or not (see section below on stopping rules). The primary study team, patients, and the PI remain blinded while the DSMB conducts these reviews of the un-blinded AE rate information.
The feasibility of perioperative CN-105 administration is assessed by tracking the percentage of doses given within the correct time window (i.e., within 1 h prior to the scheduled or actual start time of the surgery, and within a ±90 min time window for subsequent doses, which are administered every 6 h after the start of surgery).
At study completion and after un-blinding, we plan on assessing the characteristics of CN-105 treated patients who had AEs, particularly if overall AE rates or specific types of AEs are more common in drug versus placebo treated patients in this study. This analysis could potentially identify predictors of drug-related AEs if they occur, such as potential drug-drug interactions between CN-105 and other medications administered to study participants. Identifying such drug-drug interactions, if they occur, would be important given overall concerns about the detrimental effects of polypharmacy in older adults [43].
Blood and CSF sampling, assays
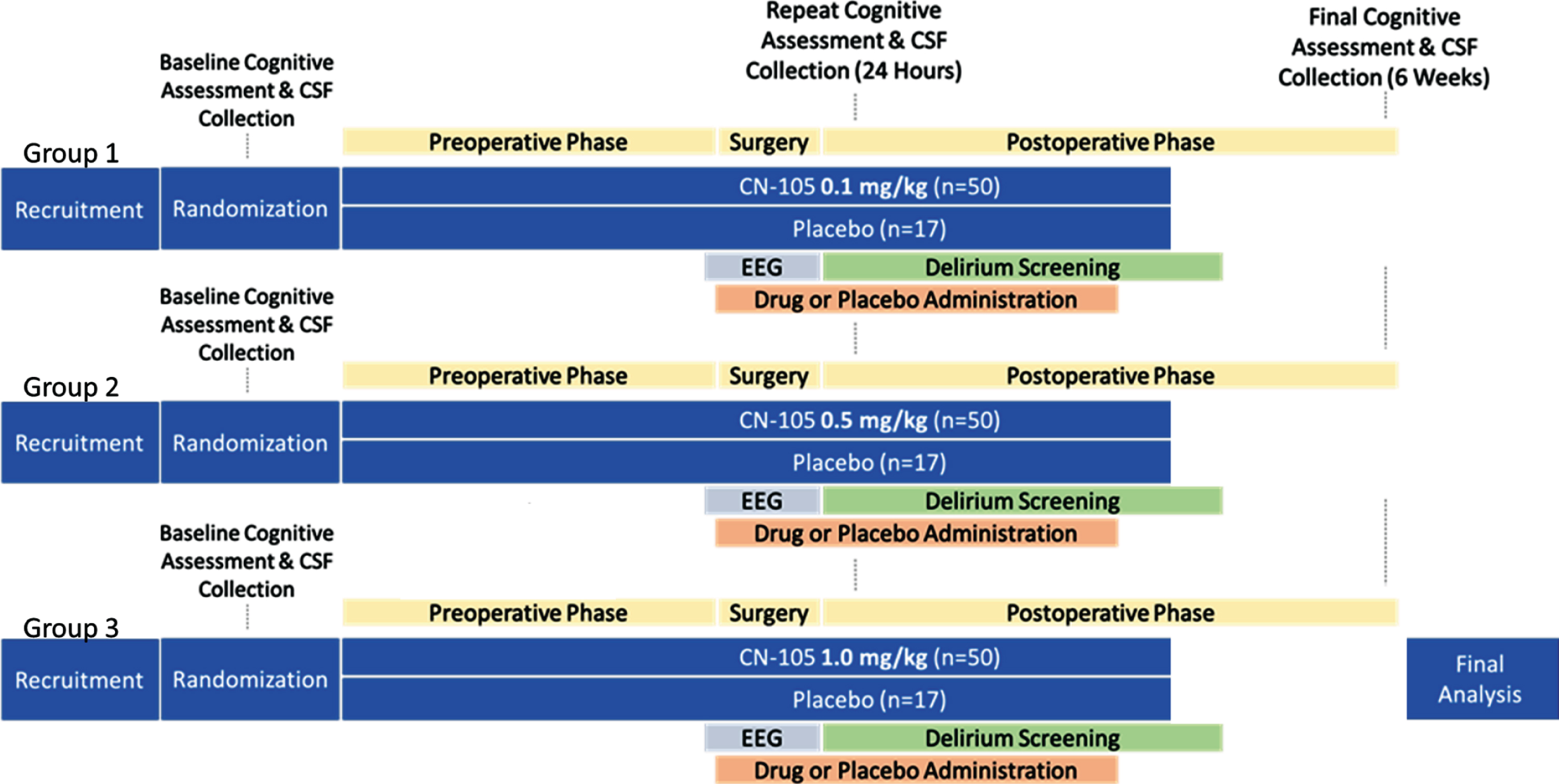
An overview of the MARBLE trial design. Precise time periods for each intervention or measurement are given in Table 1.
Activities and Timeline for MARBLE Study Participants
CSF, cerebrospinal fluid; EEG, electroencephalogram.
Participants undergo baseline CSF and blood sampling within two months prior to surgery; repeat CSF and blood samples are obtained 24±2 h after the start of surgery, and 6±3 weeks after surgery. Blood samples are centrifuged to separate plasma from the red cell pellet and buffy coat. CSF samples obtained using a 25 or 27 g pencil point needle, after topical benzocaine spray is sprayed on the patient’s back and allowed to soak in for 10 min. Then, up to 5 ml of 1–2% lidocaine is injected at the planned LP site, and 2 min is allowed to elapse before the LP needle itself is inserted, to allow the lidocaine to begin to work. We have recently shown that this protocol is effective for minimizing pain and AEs after LPs [44]. CSF samples are then centrifuged to obtain cell pellets, which are cryopreserved and stored according to our recently published protocol [45] for future studies. Blood components and CSF supernatant aliquots are stored at –80°C. CSF specimens are used to determine the effects of CN-105 treatments on levels of the cytokines IL-6, IL-8, G-CSF, and MCP-1 using Meso Scale Discovery multiplex assays [46]. Complete blood counts with differentials and serum chemistries are also obtained before and 24 h and 6 weeks after surgery, to evaluate potential off-target effects of CN-105. Blood samples are used for APOE genotyping [16]. These genotyping results will be used to perform stratified exploratory analyses to examine whether CN-105 treatment efficacy varies by APOE genotype.
Cognitive testing, NCD assessment
Cognition is assessed with a standard test battery [47, 48] (Table 2), by staff trained by a board-certified neuropsychologist within 2 months before and again 6 weeks after surgery. Individual test scores will be combined by factor analysis into cognitive domain factors, as previously described [2]. Our prior experience is that this approach typically results in a four-factor solution that accounts for the vast majority of the variance in the individual cognitive battery test scores [2]. The mean of these cognitive domain factor scores yields the Continuous Cognitive Index (CCI), a sensitive score used to quantify overall cognitive function which our group has used in multiple studies over the past 20 years [2 , 47–49]. CCI change from before to after surgery thus quantifies the degree of learning/cognitive improvement or cognitive decline. CCI change from before to after surgery will be compared between drug versus placebo treated patients as a secondary outcome, because this continuous measure (CCI change) provides significantly greater statistical power for determining differences between groups than comparing the between-groups difference in the incidence of a dichotomous outcome (such as the absence versus presence of NCD postoperative, mild or major). Further, examining the difference in CCI change between randomized groups (i.e., CN-105 versus placebo-treated) estimates the treatment effect of CN-105 after controlling for regression to the mean (since regression to the mean for cognitive test results over time should be similar in both groups), as described in [50]. Since the main purpose of this study is to simply compare outcomes (such as postoperative changes in cognition) between drug treated versus non-drug treated groups, this study does not contain a control group of non-surgical individuals.
The MARBLE Cognitive Testing Battery
Since changes in specific cognitive domains have been observed from before to after surgery [51], we will also examine the change in each the individual cognitive domain factor scores from before to 6 weeks after surgery between drug versus placebo treated patients. This is the first human study to measure cognitive change between CN-105 versus placebo treated patients; thus, we have no a priori hypothesis about which particular cognitive domain(s) will be affected the most or the least by CN-105 treatment. Accordingly, we will examine differences between drug versus placebo treated patients in each of the cognitive domain score changes (from before to after surgery) as an exploratory outcome.
The incidence of NCD-postoperative, mild and/or major [8], between drug- versus placebo- treated patients will also be examined as an exploratory outcome. NCD postoperative (mild) will be defined as a 1–2 standard deviation (SD) decrease in score on any one of the four cognitive domain factors (which are used in calculating the CCI as described above) combined with a subjective cognitive complaint. Major NCD, postoperative will be defined as a >2 SD drop in any of these four cognitive domain factors. Here, a 1 or 2 standard deviation in any one of the four cognitive domain factors refers to the standard deviation in each of these factors in the entire population under study here at the baseline/preoperative timepoint. Subjective cognitive complaints will be assessed using the Cognitive Difficulties Scale [52], which our group has previously used to examine the association between subjective and objective cognitive deficits after surgery [53]. The Cognitive Difficulties Scale is administered to MARBLE study patients both before and 6 weeks after surgery.
NCD postoperative (major) will be defined as a 2 SD decrease in any one of the four cognitive domain factors, combined with a postoperative deficit in ability to perform one or more activities of daily living (ADLs). Patients’ ability to perform ADLs will be assessed using the Duke Activity Status Index [54], which is administered to MARBLE study patients both before and 6 weeks after surgery.
Delirium screenings
Delirium is assessed at the initial baseline study visit and twice daily during postoperative days one through day five using the 3D-CAM in non-intubated patients and the CAM-ICU in intubated patients [55, 56]. Delirium assessors are trained with materials from the Hebrew SeniorLife Program/Harvard Medical School SAGES study group [57], and begin conducting delirium assessments on study patients only once they demonstrate≥90% agreement with standardized training assessments. To date, the accuracy of our delirium assessors measured using these standardized video-taped assessments [57] is 93%, and all assessors receive feedback to further improve their accuracy after this process. Delirium severity will be assessed by the 3D-CAM as well [58].
EEG recording
Baseline 32 channel EEG measurements are obtained just before surgery and CN-105 administration, and during anesthesia/surgery (i.e., after the initial CN-105 dose is given) as described [49]. These recordings will help identify potential intraoperative EEG markers of PND and/or neuroinflammation [59 –61], and whether CN-105 treatment prevents these intraoperative EEG patterns.
Physical and quality of life assessments
Physical function is assessed via Timed-Up-and-Go (TUG) [62] and Romberg tests, Duke Activity Status Index (DASI) [54], Elderly Falls Screening Test [63], Fall-Risk Screening Test, and the physical function subscale of the Short-Form-36 Health Survey (SF-36) [64]. QOL is assessed via the SF-36 [64]. These assessments occur within two months before and 6±3 weeks after surgery.
Stopping rules
MARBLE may be stopped if after any group of 67 patients the rate of grade III or higher SAEs (per 2018 CTCAE guidelines [42]) in drug-treated patients is > 10% and more than three times the rate of such events in the placebo-treated group. Considering the wide range of surgical procedures and patient comorbidities that could contribute to AEs in this study, the DSMB+ has been advised to use both this quantitative cutoff and its clinical judgement in considering whether to recommend that the study be stopped or not.
Statistical analysis
Based on prior studies, we expect≥80% of patients to complete all aspects of the study (drug administration, blood and CSF sampling, neurocognitive testing, EEG recording, quality of life assessments, and delirium screening), yielding≥117 CN-105-treated patients across the three dose groups and≥39 placebo-treated patients. We anticipate an AE incidence of 5% among placebo-treated patients, based on prior AE rates in older Duke non-cardiac surgical patients. Based on these parameters, this sample size provides > 80% power (with α=0.05) in a two- sample two-sided un-pooled variance chi-square test to detect an absolute difference of 14.8% between AE rates in placebo versus CN-105 treated patients. Missing data will be categorized by cause, and baseline characteristics of patients who do not complete the study will be compared to those who do, to evaluate for response bias. Multiple imputation will be pursued if found necessary for the analysis of efficacy endpoints. In the case that imputation is used, sensitivity analyses will also be performed using only actual data to ensure that the results are not biased by the imputation strategy.
The primary safety outcome will be compared between placebo and drug treated patients via chi-square tests and post-hoc logistic regression to investigate dose-response patterns or subgroup effects. The feasibility analysis will be performed via construction of confidence intervals for the rate of dose administration per protocol. Post-hoc analysis will be performed among drug treated patients and by dose level to determine if the drug itself or drug dose level affects feasibility. For our secondary efficacy endpoints, we will perform t-tests, Wilcoxon rank sum tests, or chi-square tests as appropriate to compare outcomes for drug and placebo treated patients. Subsequently we will use ANOVA or regression models to investigate potential dose-response and subgroup effects for each endpoint. Additional exploratory sensitivity analyses will be conducted for primary and secondary outcomes by stratifying patients based on baseline cognitive status. These additional exploratory analyses will be performed in case there are interaction effects between CN-105 effects (whether beneficial or harmful) and baseline/preoperative cognitive status.
Each study participant is assigned a unique study ID; all data and subsequent analyses are stored securely under this unique ID without patient identifiers in a redcap database. Data are to be analyzed using standard software packages including SAS and R.
DISCUSSION
MARBLE is a phase II clinical trial designed to evaluate the maximum safe dose of perioperative CN-105 administration in older non-cardiac, non-neurological surgery patients. It is secondarily intended to evaluate the feasibility and potential of CN-105 for preventing PND and reducing postoperative neuroinflammation.
We hypothesize that CN-105 administration at all dose levels will be well-tolerated by participants (i.e., with no significant increase in AE rates among drug versus placebo treated patients), based on CN-105’s phase I safety profile [39]. We expect CN-105 administration will mitigate postoperative neuroinflammation and AD pathology changes, as measured by CSF inflammatory cytokine and tau, p-tau, and Aβ levels, respectively. We also hypothesize that CN-105 will be effective for decreasing the incidence and severity of POCD/NCD.
MARBLE’s design allows for the identification of possible CN-105 response predictors for preventing POCD/NCD, delirium, and neuroinflammation, which could then be formally evaluated in future studies. For example, since apoE mimetic peptides have demonstrated differential efficacy for reducing neuroinflammation in APOE3 and APOE4 transgenic animals, [65, 66], we will also perform stratified exploratory analyses to examine whether CN-105 treatment efficacy varies by APOE genotype.
In conclusion, MARBLE is the first clinical trial to examine the effect of modulating presence of APOE4 on PND risk, severity and underlying mechanisms in older surgical patients. Its findings should guide future PND studies and may also assist in identifying predictors of susceptibility and resilience to these disorders. Finally, regardless of whether CN-105 is safe or efficacious, the data collected in MARBLE should further elucidate the role of neuroinflammation and AD pathology in PND.
Footnotes
ACKNOWLEDGMENTS
We would like to thank Tanya Bolton, Diane Edwards, Galen Murphy, and the rest of the perioperative nursing staff at Duke University Hospital for their enthusiastic support of our study and excellent care for its participants.
MARBLE is supported by a Program to Accelerate Clinical Trials (PACT) grant from the Alzheimer’s Drug Discovery Foundation (to Dr. Berger). Dr. Berger also acknowledges additional support from National Institutes of Health (NIH) grants 1K76AG057022 (to Dr. Miles Berger), R01DA043241 (to Dr. David Murdoch), the Physical Resilience Indicators and Mechanisms in the Elderly (PRIME) Collaborative UH2AG056925 (to Drs. Heather Whitson and Cathleen Colon-Emeric), and additional support from the Duke Claude D. Pepper Older American Independence Center (P30AG028716), a William L. Young neuroscience research award from the Society for Neuroscience in Anesthesiology and Critical Care (SNACC), and the Duke Anesthesiology Department. Dr. Devinney acknowledges support from a research fellowship grant from the Foundation for Anesthesia Education and Research. Dr. Laskowitz has received funding from CURE-AD for preclinical efficacy of CN-105 in murine AD models