
Abstract
In October 2018, the Texas Tech University Health Sciences Center (TTUHSC) held its first annual Healthy Aging and Dementia Research Symposium. The symposium was conceived and organized by the TTUHSC Garrison Institute on Aging. Its overall objective was to bring together scientists, healthcare professionals, interns, graduate students, postdoctoral fellows, faculty members, and NIH officials in order to share research results on aging and dementia associated with Alzheimer’s disease and to discuss possible lines of research that may be productive in reducing dementia associated with Alzheimer’s disease and, ultimately, associated with other neurological diseases. Another objective of the symposium was to share information, through formal and informal presentations, on whether and how unmodifiable factors, such as aging, and modifiable lifestyle factors, such diet and physical activity, impact dementia specifically and other chronic and neurological diseases, including diabetes and Alzheimer’s disease. Discussions of the relationship across aging, dementia, and chronic and neurological diseases, and of the impact of lifestyles on these diseases mainly focused on populations living in the rural areas of West Texas counties since these areas are known to have populations of extremely different lifestyles. This introduction gives background on research of dementia associated with Alzheimer’s disease, on populations and lifestyles of persons in rural West Texas, and on lifestyle factors known to affect progression of dementia and neurological diseases.
Keywords
INTRODUCTION
Dementia is increasing worldwide except in a very few countries that are undergoing changes in everyday lifestyles, such as the United States. This introduction addresses what researchers in the field of dementia can do to help stop the rising numbers of persons worldwide who are developing dementia. Dementia is a characterized by memory problems, impaired communication abilities, and impaired reasoning faculties. Alzheimer’s disease (AD) is the most common disease associated with dementia. AD worsens over time, with a concomitant worsening of dementia [1]. The purpose of this article is to highlight findings of ‘Healthy Aging and Dementia Research Symposium’.
Types of dementia
There are many different types of dementia, including Lewy body dementia, frontotemporal dementia, vascular disorders, mixed dementia, or a combination of types. In addition, age-related changes in the brain may harm neurons and contribute to cognitive dysfunction in AD. These age-related neuronal changes include atrophy of learning and memory regions of the brain, inflammation of the brain, increased production of free radicals, and reduced production of energy within cells [1].
Signs of dementia
There are few definitive early warning signs of dementia. Consequently, dementia begins and usually worsens before a certain diagnosis is made. Early warning signs include memory loss, difficulty in planning or solving problems, difficulty in performing such familiar daily tasks of living as putting on shoes or opening and heating a can of soup, difficulty in determining spatial and temporal orientation, confusion in attempts to understand visual information, and misplacing things [1].
Deterioration of the brain ultimately happens to everyone as they grow older, but it occurs more quickly in aged people with dementia that is associated with AD. Advanced aging is the most known, non-modifiable risk factor for the pathogenesis of dementia that is associated with AD. The number of people over the age of 65 who are diagnosed with dementia and AD doubles every 5 years, and about half of all people 85 years and older are believed to have dementia in association with AD [1].
Factors associated with dementia
In addition to aging, there are other non-modifiable risk factors for developing dementia, such as genetics, family history, Down syndrome, genetic mutations and polymorphisms in the genome, and gender [2–5]. In contrast, there are also modifiable factors associated with the onset and progression of dementia, such as socioeconomic status, diet, physical activity, smoking and alcohol use, type 2 diabetes mellitus 2 (T2DM), traumatic brain injury, cardiovascular reserve, and cognitive reserve [2–6].
Prevalence of dementia
Statistics from the 2018 World Alzheimer Report indicate that 50 million people worldwide are living with diagnosed AD, and this number is expected to increase worldwide to 82 million by 2030 and to 131 million by 2050 [7]. The 2015 World Alzheimer Report described alarming rates of dementia that are increasing in African countries [7] and also reported that global healthcare costs associated with persons diagnosed with AD were about 1 trillion US dollars in 2018. It is estimated that this figure will reach 3 trillion by 2030. According to the 2015 World Alzheimer Report, a new case of dementia is diagnosed every 3 seconds worldwide [7]. Increases in AD will no doubt be accompanied by increases in dementia. Such high healthcare costs are huge societal burdens and are indicative of healthcare problems that all countries need to urgently address.
Research into the non-modifiable risks of aging and onset of AD are continuing to better understand dementia, but researchers are also turning their attention to determining the contribution of modifiable risk factors to dementia, such as diet and nutrition, smoking, weight, and access to healthcare. Research in this latter line of research is well underway not only worldwide but also at the Garrison Institute on Aging (GIA) at the Texas Tech University Health Sciences Center (TTUHSC). In October 2018, the GIA organized and hosted a symposium on the TTUHSC campus in Lubbock, Texas, with the focus on sharing current lines of research into dementia in terms of 1) factors associated with dementia, 2) biological aspects of dementia, 3) blood-based biomarkers of dementia, 4) drug discovery to reduce symptoms of dementia, 5) educational, and community outreach programs to educate people about lifestyle decisions and their impact on dementia and public heath, and 6) funding opportunities to study dementia and modifiable and nonmodifiable risk factors [8]. At this 2-day Regional Healthy Aging and Dementia Research Symposium, researchers, interns, graduate students, postdoctoral fellows, geriatricians, social workers, and others involved in dementia research met to share their research results and to discuss possible lines of research that may be productive in reducing dementia worldwide. Since this article is focused on lifestyle factors and risks associated with dementia in rural West Texas population, it is important to discuss historical development, topology, and demographic features of Texas for the last 100 years.
HISTORICAL DEVELOPMENT OF TEXAS
The population of Texas grew rapidly from 1,591,749 in 1880 to 3,048,710 in 1900. In addition to the natural growth of Texas population, a steady migration came from southern states, and foreign-born migrants (from Mexico and Germany), also contributed with a large number 179,357 to the population. Most Texans lived and labored in rural areas—90.8% in 1880, still 82.9% in 1900. The expanding population spread westward to complete settlement of the state by establishing communities on the South Plains, in the Panhandle, and beyond the Pecos River. Figure 1 shows geographic locations of early Texans [9].
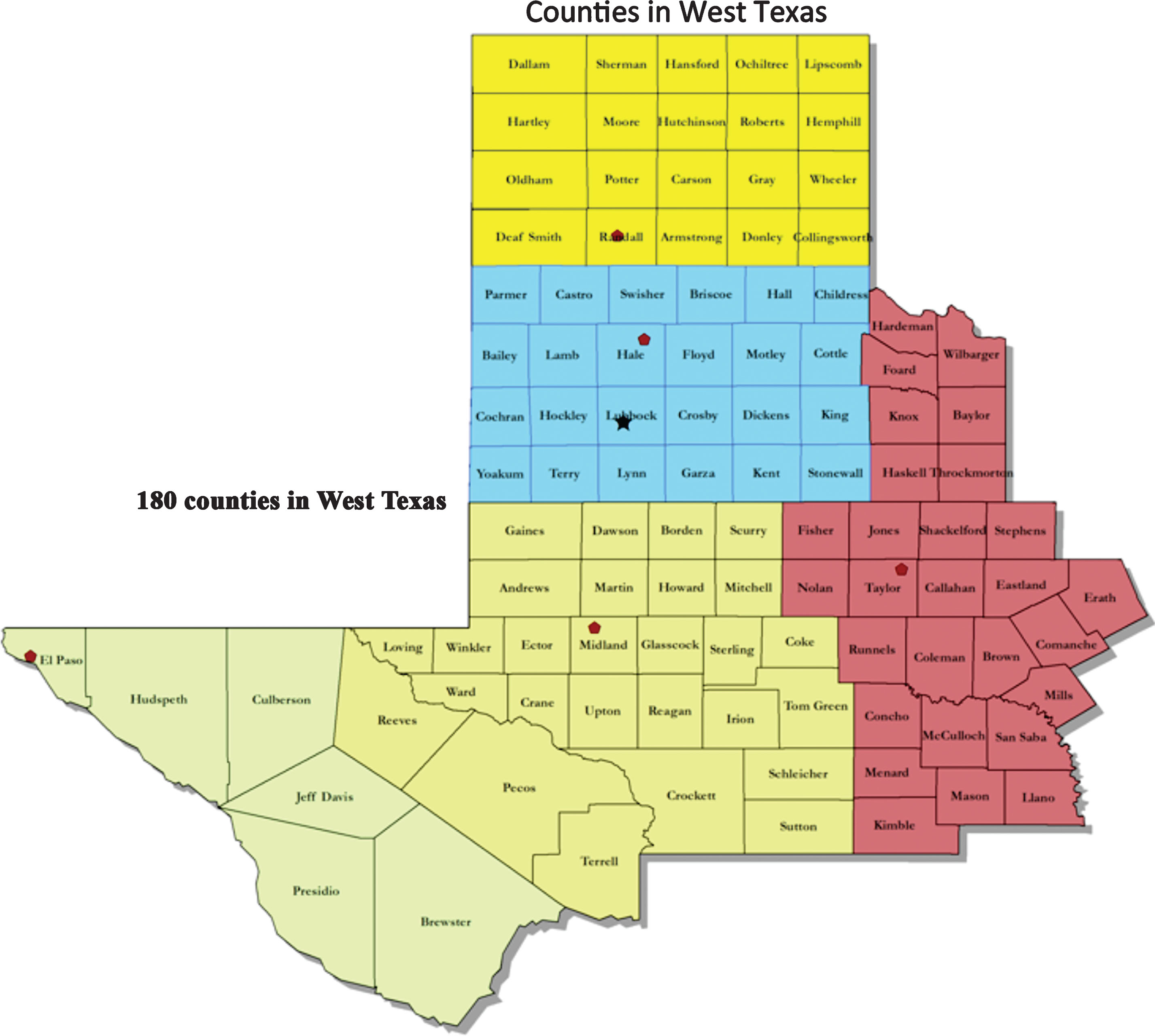
Total number (180) of counties in West Texas.
The Texas economy markedly increased in the late nineteenth century. Agriculture continued to dominate the state economy, with a majority of Texans engaged in farming or ranching. The number of farms and ranches grew from 174,184 in 1880 to 2,506,212 in 1900—more than in any other state. Corn, the most significant food crop, increased from 29,065,172 bushels in 1880 to 109,970,350 in 1900. The value of Texas farms increased because they grew in size.
Ranching, like farming, experienced impressive growth, as Texans drove more than three million cattle north to the railroads in Kansas between 1875 and 1885, after the Indians had been forced from the plains. Major ranchers in West Texas joined those in South Texas in raising the largest herds in the nation, which grew from 4,894,698 cattle and 3,651,633 sheep in 1880 to 8,543,635 cattle and 4,264,187 sheep in 1890. Prices began to fall because supply outran demand, disease led to quarantines, harsh winters and drought-killed animals.
The development of commercial farming and ranching received important stimulation from the growth of railroads. Spurred on by state land grants of over thirty million acres, railroads grew from 1,650 miles of track in 1875 to 9,867 in 1900. The new track, more than half of which was laid between 1875 and 1885, crossed the state both east-west and north-south to provide faster and cheaper transportation for people and products. Between 1880 and 1900 the number of women in the work force increased from 58,943 to 140,392, an advance from 11% to 13% of all employed persons.
The development of industries, primarily in urban areas, stimulated the growth of Texas towns in the late nineteenth century. The number of Texans living in urban centers grew from 115,396 in 1880 to 454,926 in 1900, an increase from 7.2% to 14.9% of the population. The patterns of urban growth shifted, however, as newer interior towns expanded more rapidly with advancing settlement.
In 1910, 24.1% of the Texas population resided in urban areas. By 2010, the urban share of Texas population had risen to 84.7%. Conversely, in 1910, 75.9% of Texans lived in rural areas compared to 15.3% in 2010. Its eastern boundary has been defined as far west as the Pecos River and as far east as the Brazos River. The concept of west Texas is based on the five principal metropolitan areas it contains: El Paso, Lubbock, Abilene, Midland/Odessa, and San Angelo [9].
PHYSICAL TOPOLOGY OF RURAL WEST TEXAS
Texas’s major physiographic divisions are the Gulf Coastal Plain in the east and southeast; the North Central Plains, covering most of central Texas; the Great Plains, extending from west-central Texas up into the panhandle; and the mountainous trans-Pecos area in the extreme west [9].
DEMOGRAPHY OF RURAL WEST TEXAS
The area in rural West Texas is a 131,000 square mile service area that is divided into 180 counties (Fig. 1). This area comprises 50% of the landmass and 11% of the population of Texas. The cities of Lubbock, Midland, Odessa, and El Paso are located in rural West Texas. This area has a population of 2.7 million persons who have been highly underserved by health care professionals and health care facilities, despite the substantial and meaningful contributions made by Texas Tech University Health Sciences Center and other research and educational institutions in Texas to reach the rural West Texas population. As shown in Fig. 2, Texas has 254 counties with a population of 29.09 million and area of 268,597 square miles [10].
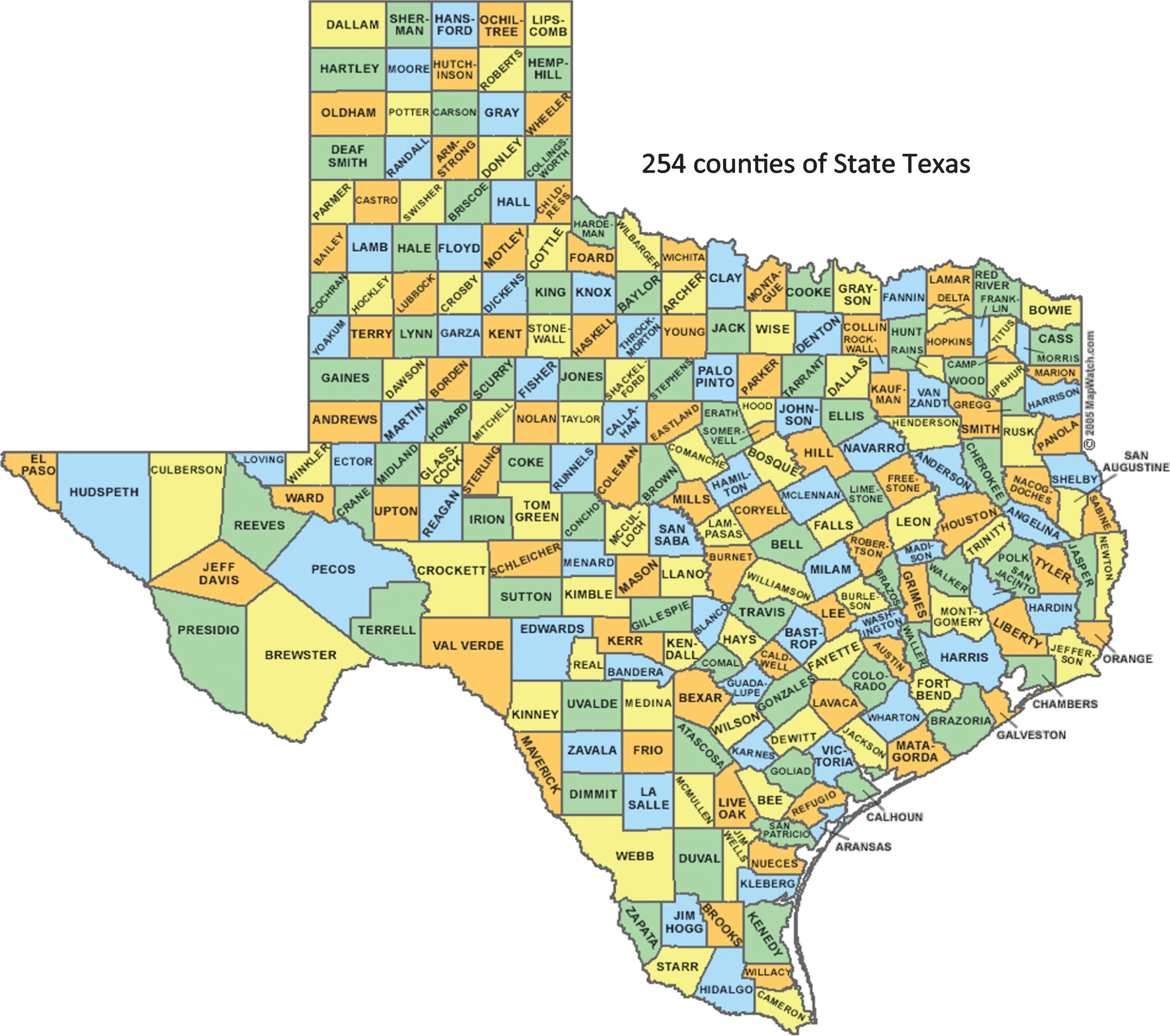
Total number (254) of counties in Texas.
From 1980 to 2018, there have been major demographic shifts in rural West Texas populations, as well as socioeconomic and epidemiologic characteristics of its sub-groups, creating major and specific demands on healthcare services.
As shown in Table 1, the per capita income is low in Texas compared to overall US per capita income; however, per capita income of rural West Texas is even lower than Texas. These numbers indicate that low economy in rural West Texas—in other words, most residents live rural West Texas are below the poverty line. Percent of poverty also increased in children and persons above 65 years of age in rural West Texas.
Per capita income and poverty comparisons for Texas
Source: Most recent data available. Income information from the Bureau of Economic Analysis, 2002 data. Poverty data from the U.S. Bureau of the Census, 2000 Census [11].
HEALTH STATUS OF HISPANIC POPULATIONS IN RURAL WEST TEXAS
Health care is a major economic industry in rural area. In communities that still have a local hospital or nursing home, health-related businesses are often the largest employers. One rural physician can generate more than five full–time jobs and $233,000 in local economic activity. For every health care dollar generated locally, an estimated 1.5 dollars are brought into the community economy. Therefore, immigration of Hispanic persons from rural counties in rural West Texas to more urban areas to cities in other Texas cities is a major contributor to the loss of local revenues, which ultimately reduces the funds available to spend on health care in rural West Texas, and 70 to 80% of out–migration is due to the availability of care facilities [12]. Throughout West Texas, population density is low, making it difficult to maintain health care services since there are not enough persons to support a medical practices and institutions. The general population of rural West Texas is too low to support adequate medical care, whether the population is comprised of Hispanics or non-Hispanics, people who are homeless or own homes, whether they are single or married mothers of young or adolescent children, whether they are poor or middle-income, whether they are living with chronic diseases and disabilities or not [13].
CHRONIC NEUROLOGICAL DISEASES
According to the Center for Disease Control & Prevention, rates of heart disease are higher in rural West Texas, particularly in Hispanic populations. Physical inactivity and unhealthy diets are part of the lifestyle of Hispanics in rural West Texas. As shown in Figs. 3 and 4, percentage of Hispanic Population based on geographical location and age.

In some counties of rural West Texas, 50–80% of the population is of Hispanic heritage. Healthcare for persons with chronic diseases, including T2DM, obesity, cardiovascular disease, and dementia are urgently needed in rural West Texas populations.
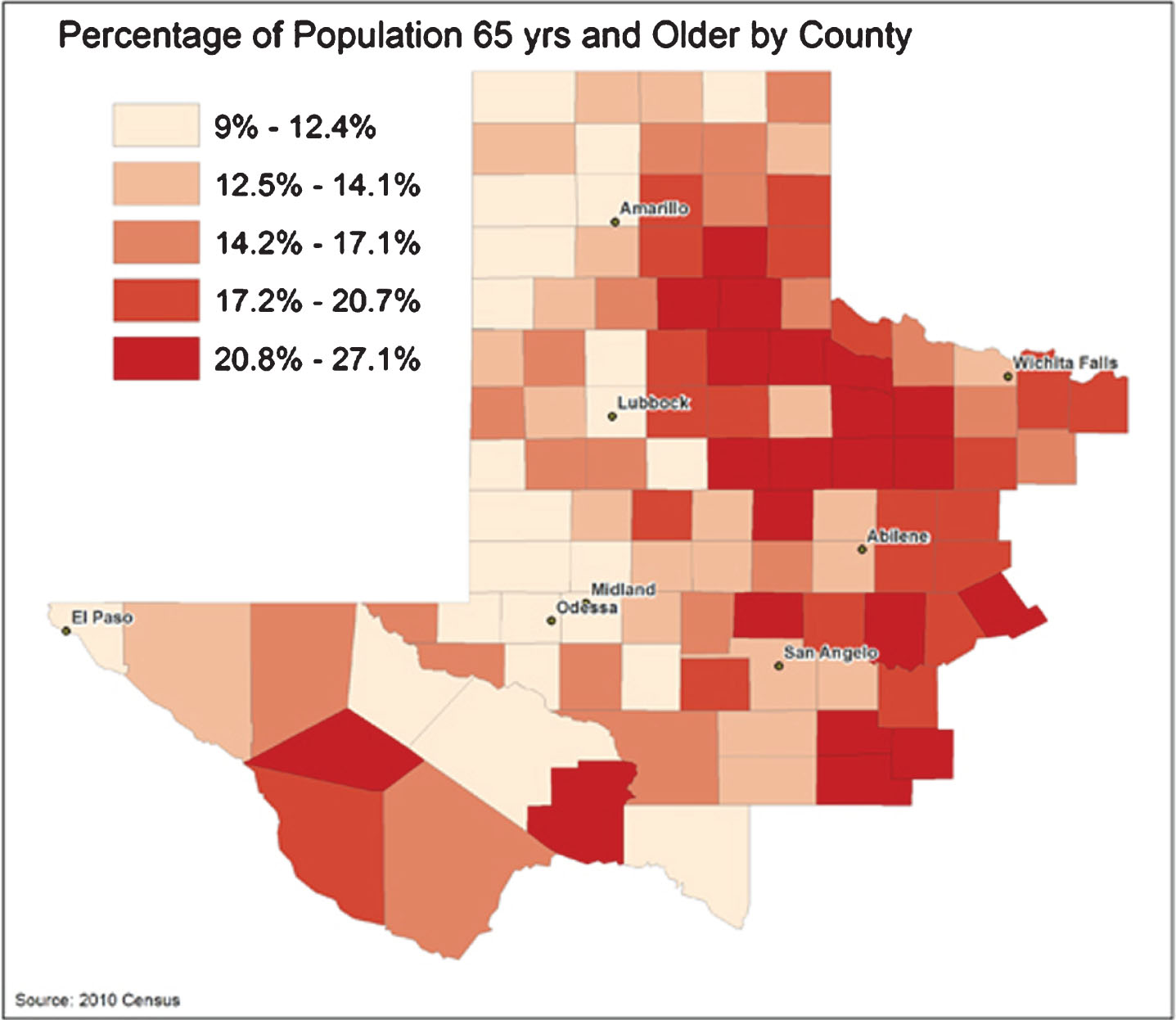
Percentage of population 65 years and older in the counties comprising rural West Texas. As shown in this figure, most of the population in rural West Texas.
Although there is no research on the prevalence of AD with dementia in Hispanic populations in rural West Texas, there has been research on Hispanics and stroke, a disease that has modifiable lifestyle risk factors, similar to dementia. In 2005, the CDC reported that in the United States in the last decade of the 20th century, 1 out of 4 Hispanic men died of stroke, greater than the 1 out of 10 non-Hispanic men who died of stroke. The CDC also found that Hispanic men are also more likely to have their first stroke at younger ages than non-Hispanic white: the average age for a first stroke among Hispanic men was 67, far younger than the age of first stroke for non-Hispanic whites, the average age of which was 80 years. Studies are underway are needed to determine socioeconomic status, lifestyle, and genetic influences that may account for differences between Hispanic men and non-Hispanic white men in terms of stroke.
According to the CDC, Hispanic men and women in the United States are at greater risk for kidney disease than are non-Hispanic white men and women, and are also 1.5 times more likely to have kidney failure compared to non-Hispanic white men and women. In 2015, the CDC reported that 13% of new kidney failure patient were Hispanic, compared to 5% of non-Hispanic whites, but it is as yet not fully understood why. Researchers have speculated that these differences may be due to the higher percentage of Hispanic men and women who have T2DM, which is the leading cause of kidney disease: 10% of Hispanics were determined to have T2DM, compared to 3% of non-Hispanic whites [14].
Lifestyle features influencing the onset of such diseases as stroke, T2DM, and kidney disease—and of dementia—have also not been researched in Hispanic and non-Hispanic white populations in the United States. It has been hypothesized that the lifestyle of Hispanic men in rural West Texas impacts not only the prevalence of dementia, stroke, T2DM, and kidney disease on this population, but their lifestyle also impacts the age at which they develop the diseases.
SUMMARIES OF PUBLISHED ARTICLES IN SYMPOSIUM TOPIC
In the October 2018, the TTUHSC symposium focused on the latest research of the relationship between healthy aging and dementia, public health trends related to neurodegenerative diseases of aging, and community-based programs and research into nutrition and cognition. There were formal presentations, special addresses, oral presentations, and poster presentations by researchers from across the United States [8]. Nine of these presenters wrote full-length articles to accompany their presentations. Brief summaries of the articles that were accompanied by written articles are given here:
Oliver and Reddy (2019) summarized their research on the molecular basis of AD, with a particular focus on mitochondria [15]. They discussed recent developments in the research of mitochondrial structure, function, physiology, dynamics, biogenesis, mitophagy, and mitochondrial DNA changes in healthy and diseased states. They also discussed factors, including age, gender, lifestyle, epigenetic factors, and T2DM, that are involved in late-onset AD. They highlighted morphological and pathological studies that are associated with the loss of synapses, defective mitochondria, and the proliferation of reactive astrocytes and microglia in AD, in addition to the presence amyloid-β (Aβ) and phosphorylated tau in learning and memory regions of the brain in AD patients. They compared early-onset familial and late-onset sporadic AD in terms of functional aspects of mitochondria and synapses. They discussed the involvement of genetic mutations in APP, PS1, and PS2 loci causing familial AD. They reported on multiple factors that they found to be involved in late-onset AD, including APOE4 genotype, polymorphisms in several gene loci, T2DM, traumatic brain injury, stroke, and age-related factors, including increased reactive oxygen species production and dysfunction in mitochondria [13].
George and Reddy (2019) summarized others’ research into the role of healthy diets and regular exercise on delaying the progression of dementia in elderly mice and humans [16]. They presented evidence on how antioxidant-enriched diets and regular exercise reduced toxic radicals, enhanced mitochondrial function and synaptic activity, and improved cognitive function in elderly populations. They also summarized others’ research into antioxidants that were added to the diet of mouse models of AD and antioxidant supplements added to the diets of elderly persons with AD. They also assessed research that used antioxidants in the diets of AD patients. Their survey suggests that antioxidant diets delay the progression of dementia in elderly individuals. George and Reddy cautiously concluded that diets rich in antioxidants and regular exercise appeared to delay the progression of dementia and appeared to reverse mild cognitive impairment in individuals to the point that they ultimately returned to a non-demented state [16].
Ramasubramanian and Reddy (2019) discussed the role of T2DM as a risk factor for AD. In patients with diabetes, increased blood glucose levels are reported to induce multiple complications, such as heart disease, stroke, kidney failure, foot ulcers, and damage to the eyes. However, they noted that the molecular basis of T2DM is not completely understood [17]. Further, there are no accurate animal models that mimic both type 1 and T2DM found in humans. Multiple polygenic models are being used to study T2DM, including the Goto-Kakizaki rat, the Otzhka Long-Evans Tokushima fatty rat, the Nagoya Shibata Yasuda mouse, the New Zealand obese mouse, the Tsumura-Suzuki obese diabetes mouse, the leptin-deficient ob/ob, and the leptin receptor deficient db/db mouse models. They extensively discussed about TallyHo mice that represents many features of T2DM in humans. In this mouse model, only the male mice develop hyperglycemia and the females exhibit features of obesity. Thus, this model can be used to study both diabetes and obesity. Ramasubramanian and Reddy assessed whether TallyHo mice are a true mouse model for T2DM and AD [16].
Kumar and Reddy (2019) summarized their own research that investigated blood-based microRNAs as peripheral biomarkers for AD [18]. They discovered therapeutic relevance of miR-455-3p to biomarkers in AD. Their global microarray analysis of serum samples from AD patients, individuals with mild cognitive impairment, and healthy subjects found high levels of miR-455-3p in the AD patients relative to mild cognitive impairment individuals and healthy controls. Their findings also confirmed the role of miR-455-3p in AD with different AD samples such as serum, postmortem brains, AD fibroblasts, AD B-lymphocytes, AD cell lines, AD mouse models, and AD cerebrospinal fluid confirmed the biomarker potential of miR-455-3p. They determined the mechanistic link between miR-455-3p in AD miR-455-3p regulate amyloid-β protein precursor (AβPP) and Aβ levels. The luciferase reporter assay validated AβPP as a target of miR-455-3p. Their study on mouse neuroblastoma cells revealed the protective role of miR-455-3p against Aβ-induced toxicities [18]. They also found that miR-455-3p enhanced cell survival and extended the lifespan of cells. High levels of miR-455-3p reduced Aβ toxicity, enhanced mitochondrial biogenesis and synaptic activity, and maintained healthy mitochondrial dynamics. Based on these findings, they speculated that miR-455-3p may be a promising peripheral biomarker and therapeutic candidate for AD.
Sawant and Reddy (2019) assessed the role of phosphorylated tau in Huntington’s disease (HD) progression and pathogenesis [19]. Although the HD gene was discovered 26 years ago, it is still unknown how mutant huntingtin (mHTT) selectively targets medium spiny projection neurons in the basal ganglia of patients with HD. Several years of intense research by scientists revealed that multiple cellular changes are involved in the HD disease process, including transcriptional dysregulation, mitochondrial abnormalities and impaired bioenergetics, defective axonal transport, calcium dyshomeostasis, synaptic damage, and caspase and NMDAR activations. Sawant and Reddy reported on recent research in which phosphorylated tau and defective GSK3β signaling were found to be strongly linked to HD progression. They also summarized recent findings in cellular and pathological changes in HD progression, namely that mutant Htt aggregates and GSK3β activation [19].
Khan and colleagues (2019) studied the current status of chronic diseases, including dementia and hypertension, in rural West Texans [20]. They analyzed the risk factors of dementia data collected by Project FRONTIER for rural West Texas counties. They found that hypertension, neurologic diseases, and muscle strength were associated with males and females older than 60. Hypertension was significantly associated with cognitive disorders and T2DM in both males and females [20]. Females but not the males in this age group also had with a prevalence for parkinsonism, stroke, reflexes, and sensory intact, Hypertension in females was significantly associated with cardiovascular disease and depression. Both males and females in Hispanic and non-Hispanic groups were found to be significantly associated with AD. They concluded that gender-specific differences in dementia risk factors exist and integrating such variables may guide relevant policymaking to reduce dementia incidence in rural West Texas.
Hegde and colleagues (2019) discussed research into risk factors of T2DM, including hyperinsulinemia and insulin resistance, in an effort to determine whether these same factors may be risk factors in the development of mild cognitive impairment and AD [21]. Recent findings have shown that hyperinsulinemia and insulin resistance can coexist or be independent events. They emphasized that there is an urgent need to determine the impact of each of these conditions on AD.
Kang and Woo (2019) discussed research into cofilin, a master node that regulates cytoskeletal pathogenesis in AD, to determine the role of cofilin and phosphorylated tau in AD [22]. Hirano bodies and cofilin-actin rods are extensively found in AD brains; both are associated with the actin cytoskeleton. The actin-binding protein cofilin, known for its actin filament that severs, depolymerizes, nucleates, and bundles activities, has emerged as a significant player in AD pathogenesis. Kang and Woo reported on their research into the regulation of cofilin by multiple signaling events that impinge on LIM kinase-1 and/or Slingshot homolog-1 downstream of Aβ [22]. Such pathophysiological signaling pathways impact actin dynamics to regulate synaptic integrity, mitochondrial translocation of cofilin to promote neurotoxicity, and the formation of cofilin-actin pathology. They also found other intracellular signaling proteins, such as β-arrestin, RanBP9, Chronophin, PLD1, and 14-3-3 that impinge on the regulation of cofilin downstream of Aβ. They discussed the role of activated cofilin as a bridge between actin and microtubule dynamics by displacing tau from microtubules, thereby destabilizing tau-induced microtubule assembly, missorting tau, and promoting tauopathy [22].
Morsy and Trippier (2019) highlighted currently known and emerging pharmacological targets for the treatment of AD [23]. They discussed the use of these targets in terms of therapeutic strategies. The first approach targets pathological hallmarks of AD, namely Aβ oligomers and hyperphosphorylated tau tangles which primarily focus on reducing formation and aggregation, and/or inducing the clearance of Aβ [23]. The second approach modulates neurotransmitter signaling. Comprising this strategy are cholinesterase inhibitors and treatments to block N-methyl-D-aspartate receptor blockade, both of which have been approved by the FDA to reduce AD symptoms. Additional targets under investigation are those that aim to stabilize neuron signaling through modulation of neurotransmitters and their receptors. The third approach uses a collection of ‘sensitive targets’ to indirectly influence Aβ or tau accumulation. These targets are proteins that, upon Aβ accumulation in the brain or upon their direct interaction with Aβ accumulation, modify the target’s function. They also discussed changes in Aβ levels that occur in AD progression [23]. This strategy aims to restore normal target function to alleviate Aβ-induced toxicity in neurons. Overall, they discussed drug targets that have emerged in the last decade and targets that have been validated using small molecules in in vitro and/or in vivo models [23].
CONCLUSIONS
Chronic diseases, including dementia and neurological diseases, are increasing in Texas, the United States, and globally. Chronic diseases are highly prevalent in Hispanic males and females, particularly in rural West Texas. Even with clinicians, healthcare professionals, and researchers in rural West Texas, many more resources are needed to provide the health care and education to change lifestyle factors known to impact the development of dementia in elderly persons. These challenges can be addressed to a certain extent by 1) developing more healthcare clinics, 2) developing more community outreach centers to increase awareness in Hispanics’ about healthy lifestyle choices and dementia, 3) develop centers for excellence on aging, and dementia, 4) introduce biology of aging and dementia in educational curriculum in graduate and medical programs, 5) develop and establish Alzheimer’s Disease Research Centers, and 6) developing statewide dementia and chronic diseases data management cores to keep records of residents of rural West Texas.
This issue of the Journal of Alzheimer’s Disease provides timely resources for students, scholars, clinicians, and basic science researchers who are seeking a basic understanding of chronic diseases of rural West Texas.
I sincerely thank all of our contributors for their outstanding articles and to our reviewers who provided cogent evaluations of our articles. Special recognition is given to Beth Kumar, Managing Editor of this issue; George Perry, Editor-in-Chief of the Journal of Alzheimer’s Disease; Rasjel van der Holst, publisher at IOS Press; and all of the IOS Press production and printing staff for their professional support.