
Abstract
Background:
Obstructive sleep apnea (OSA) is associated with cognitive impairment and increased risks of dementia. However, the effect of continuous positive airway pressure (CPAP) on cognitive function in patients with OSA is still controversial.
Objective:
To evaluate the cognitive effects of CPAP treatment on OSA.
Methods:
We systematically searched PubMed, EMBASE, and Cochrane Library for randomized controlled trials (RCT) in the corresponding fields.
Results:
Totally 14 studies and 1,926 participants were included in our meta-analysis. Standardized mean difference (SMD) or weighted mean difference (WMD) were calculated for subjective sleepiness and cognitive domains including attention and speed of information processing, executive function, and memory. Individual cognitive scale and subgroup analyses according to OSA severity, length of trial, and RCT design type were further conducted. Significant treatment effect on attention and speed of information processing was only observed in severe OSA patients (SMD, 0.17; 95% CI, 0.02 to 0.31; p = 0.025; I2 = 0%).
Conclusions:
Therefore, our meta-analysis indicates that CPAP treatment can partially improve cognitive impairment in the population of severe OSA.
INTRODUCTION
Obstructive sleep apnea (OSA) is one of the most common types of sleep disorders characterized by repeated obstruction of upper airway during sleep [1–3], which leads to intermittent hypoxemia, sleep fragment, and daytime sleepiness [4, 5]. Mounting evidences have demonstrated that cognitive impairment is one of the core consequences of OSA [6], with a series of mechanisms proposed. Intermittent hypoxia may destroy the integrity of white matter as the result of systemic inflammation and altered permeability of blood–brain barrier, which leads to changes of synaptic plasticity and consequently cognitive impairment [7, 8]. At the same time, disturbed sleep in OAS may directly contribute to Alzheimer’s disease (AD) by increasing generation and deposition of amyloid-β (Aβ), promoting tau hyperphosphorylation, as well as decreasing Aβ clearance [9].
Continuous positive airway pressure (CPAP) is considered as an effective way to treat OSA via steady airflow supplement with devices worn during sleep [10, 11]. However, the cognitive effect of CPAP treatment on patients with OSA is still controversial. Some studies demonstrated that CPAP treatment could partly reverse the cognitive impairment attributed to OSA [12, 13], whereas others did not find sufficient improvement after CPAP treatment [14, 15]. Although two meta-analyses had been performed previously [16, 17], they included only a limited population or were performed a few years ago. Hence, we aim to comprehensively evaluate the effects of CPAP on cognition so as to provide an evidence-based clinical guidance for future treatment of OSA patients.
METHODS
Inclusion/exclusion criteria
Articles were included if they: 1) defined OSA by apnea-hypopnea index (AHI), oxygen desaturation index (ODI), or respiratory disturbance index (RDI); 2) were randomized controlled trials (RCTs) of CPAP compared with sham CPAP (or standard care) conducted in adults (aged≥18 years) with OSA; 3) were with outcomes of cognitive function assessed by effective neuropsychological tests. In addition, only articles with valid data or data that could be transformed into valuable information or obtained from authors were included.
Abstracts, comments, case reports, reviews, and meta-analyses were excluded from the research. We also excluded duplicate reports and those conducted in children. Language of publication was restricted to English, and the date of publication was updated to October 24, 2019.
Search strategy
Two investigators independently searched for the relevant articles through electronic databases, including PubMed, EMBASE, and Cochrane Library. We applied the same search terms associated with three major themes into the online databases, which were sleep-related breathing disorders, cognition, and treatment. The specific search terms were as follows: ((sleep disorder breathing) or (sleep apnea) or (upper airway resistance)) and (cognition or cognitive or dementia or memory or Alzheimer or neuropsychological or neuropsychology) and ((effect or treatment or improvement or therapy or management or (positive airway pressure)). Moreover, reference lists of the relevant articles and reviews were scanned by hand for additional articles.
Data extraction and quality assessment
Preliminarily included articles were independently identified by two investigators according to title and abstract. If the reviewer was uncertain about the eligibility, the article was read in full. Disagreements were discussed by two investigators in order to reach consensus. Major disagreements included the eligibility of a crossover trial with three different treatments and cognitive outcomes of some cognitive scales. Any disagreement was resolved by consensus discussion and consultation with a third investigator. Data were extracted independently by investigators with the following information: author, year of publication, sample size, definition of OSA, way of intervention, cognitive outcomes, etc. Insufficient data were solved by asking the author through E-mail or by transforming the data through statistical methods.
Quality of the included RCTs was performed by two investigators independently according to the Jadad scale, which assesses randomization procedure, blinding and description of dropout [18].
Statistical analysis
Data-analysis was performed with STATA. Means and standard deviation of cognitive change, as well as number of participants were used to calculate the effect size. Results were presented as standardized mean difference (SMD) when different scales were used to assess one cognitive domain, or weighted mean difference (WMD) when the cognitive domain derived from the same scales. Value of p < 0.05 was considered statistically significant. I2 statistics were used in conjunction with chi-square test to describe the percentage of variability and quantify the degree of heterogeneity. Random-effect model was used in our analysis considering the heterogeneity of the samples. Begg’s and Egger’s tests were conducted to evaluate the publication bias. Epworth sleepiness scale (ESS) was used to assess subjective sleepiness. Three cognitive domains, attention and speed of information processing, executive function, and memory were evaluated in the study. Subgroup analyses were further conducted according to OSA severity (mild to moderate or severe), length of trial (4 weeks or more than 4 weeks) and RCT design type (parallel or crossover).
RESULTS
Study identification and characteristics
Totally 1,149 articles were identified from the electronic databases. After applying the inclusion and exclusion criteria, inappropriate articles were excluded according to title and abstract. Thirty-eight articles were carefully read in full to verify the eligibility, and 15 articles were removed afterwards. We further excluded 9 articles for insufficient data, which cannot be transformed through statistical methods or acquired from authors. Eventually, 14 articles were included in this meta-analysis [12–15, 19–28]. The process was displayed in Fig. 1.
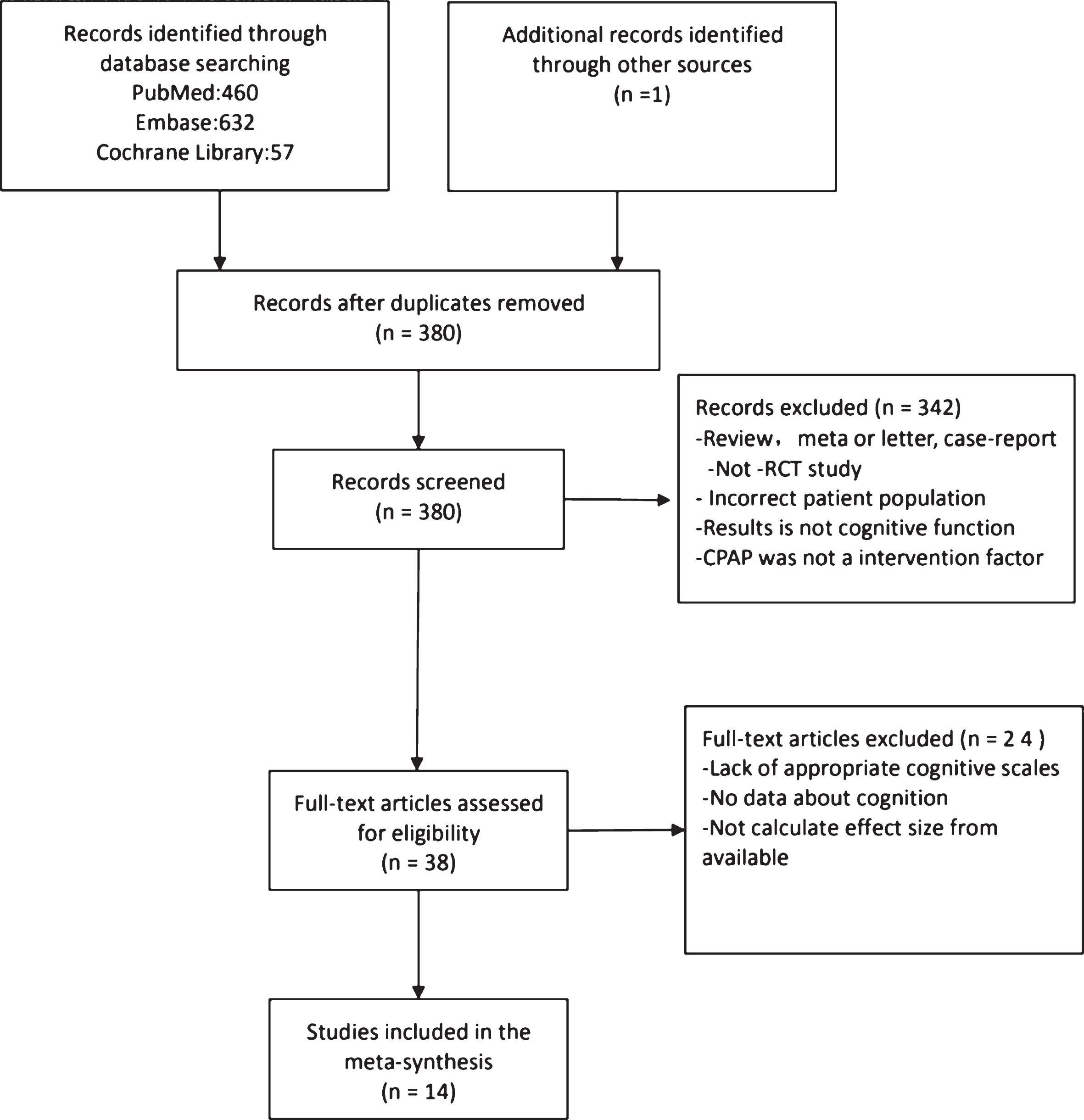
Flow diagram of systematic search and study selection.
All articles identified were published between 1998 and 2016, including 1,926 participants (mean age of 57.0 years) from 6 different countries. The sample size ranged from 23 to 843 participants, with 995 in the experimental groups and 931 in the control groups. Of the 14 RCTs, 11 were parallel trials and 3 were crossover trials; one was performed in the population of Parkinson’s disease, and one was performed in the population of stroke. The definition of OSA was based on AHI > 5 events/h, except for one article using oxygen desaturation index (ODI) > 7.5 events/h and one using respiratory disturbance index (RDI) > 15. Treatment adherence and duration ranged from 2.5 to 6.4 h per night and 1 to 24 weeks respectively. Study characteristics were listed in Tables 1 and 2.
Clinical characteristics of studies included in the meta-analysis
N, number of patients (E, experimental group; C, control group); BMI, body mass index; AHI, apnea-hypopnea index; CPAP, continuous positive airway pressure.
Comparison between groups, duration, design, country, and Jadad rating score of studies included in the meta-analysis
RCT, randomized controlled trial; CPAP, continuous positive airway pressure; Jadad, rating score for the quality of a randomized controlled trial-controlled trial.
Main results
No improvement of subjective sleepiness was observed in CPAP treatment group compared with controls (WMD, –2.36; 95% CI, –4.93 to 0.21; p = 0.07; I2 = 95.8%) (Fig. 2). Similarly, CPAP could not improve attention and speed of information processing (SMD, 0.05; 95% CI, –0.02 to 0.12; p = 0.15; I2 = 0%), executive function (SMD, 0.01; 95% CI, –0.11 to 0.11; p = 0.93; I2 = 0%), and memory (SMD, –0.02; 95% CI, –0.46 to 0.43; p = 0.95; I2 = 25.7%) (Fig. 3). However, subgroup analysis found that CPAP treatment could significantly improve attention and speed of information processing in patients with severe OSA (SMD, 0.17; 95% CI, 0.02 to 0.31; p = 0.025; I2 = 0%) (Fig. 4). No significant improvements were observed when patients were assessed with individual cognitive scale (Figs. 5 and 6), including Trail Making A (WMD, –2.58; 95% CI, –5.56 to 0.40; p = 0.09; I2 = 0%), Trail Making B (WMD, 0.09; 95% CI, –5.91 to 6.09; p = 0.98; I2 = 0%), Digit Symbol (WMD, 0.80; 95% CI, –0.25 to 1.86; p = 0.13; I2 = 20.5%), Digit Symbol Substitution (WMD, 0.52; 95% CI, –0.61 to 1.65; p = 0.37; I2 = 0%), Verbal Fluency (WMD, –0.67; 95% CI, –4.93 to 3.60; p = 0.76; I2 = 0%), Digit Span (WMD, 0.17; 95% CI, –0.21 to 0.54; p = 0.38;I2 = 0%), Digit Span Forward (WMD, 0.02; 95% CI, –1.54 to 1.58; p = 0.98;I2 = 55%), and Digit Span Backward (WMD, –0.16; 95% CI, –0.46 to 0.14; p = 0.30; I2 = 0%).
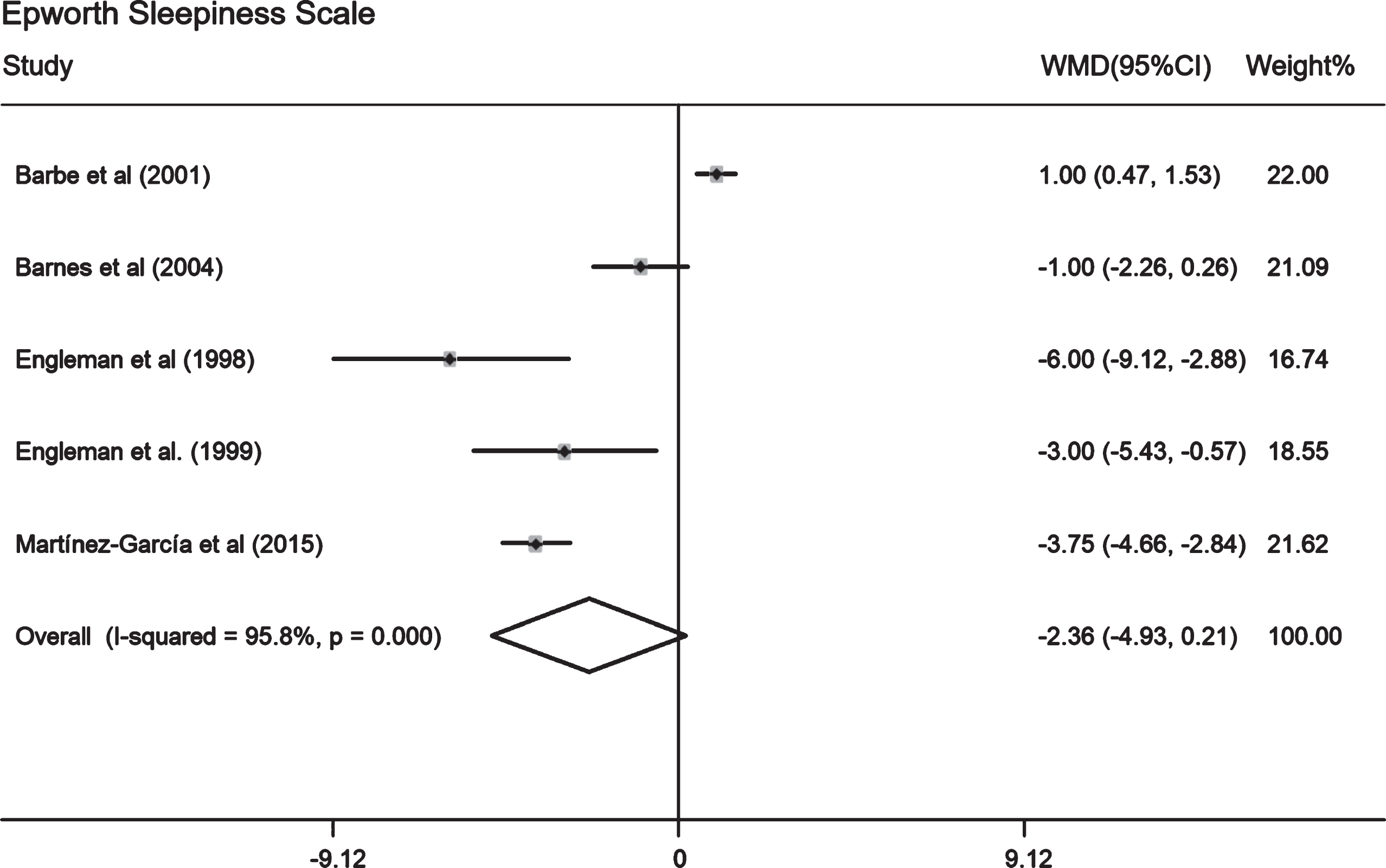
Forest plot of studies on association between CPAP and subjective sleepiness: Epworth Sleepiness Scale.

Forest plot of studies on association between CPAP and cognition: attention and speed of information processing, executive function, and memory.
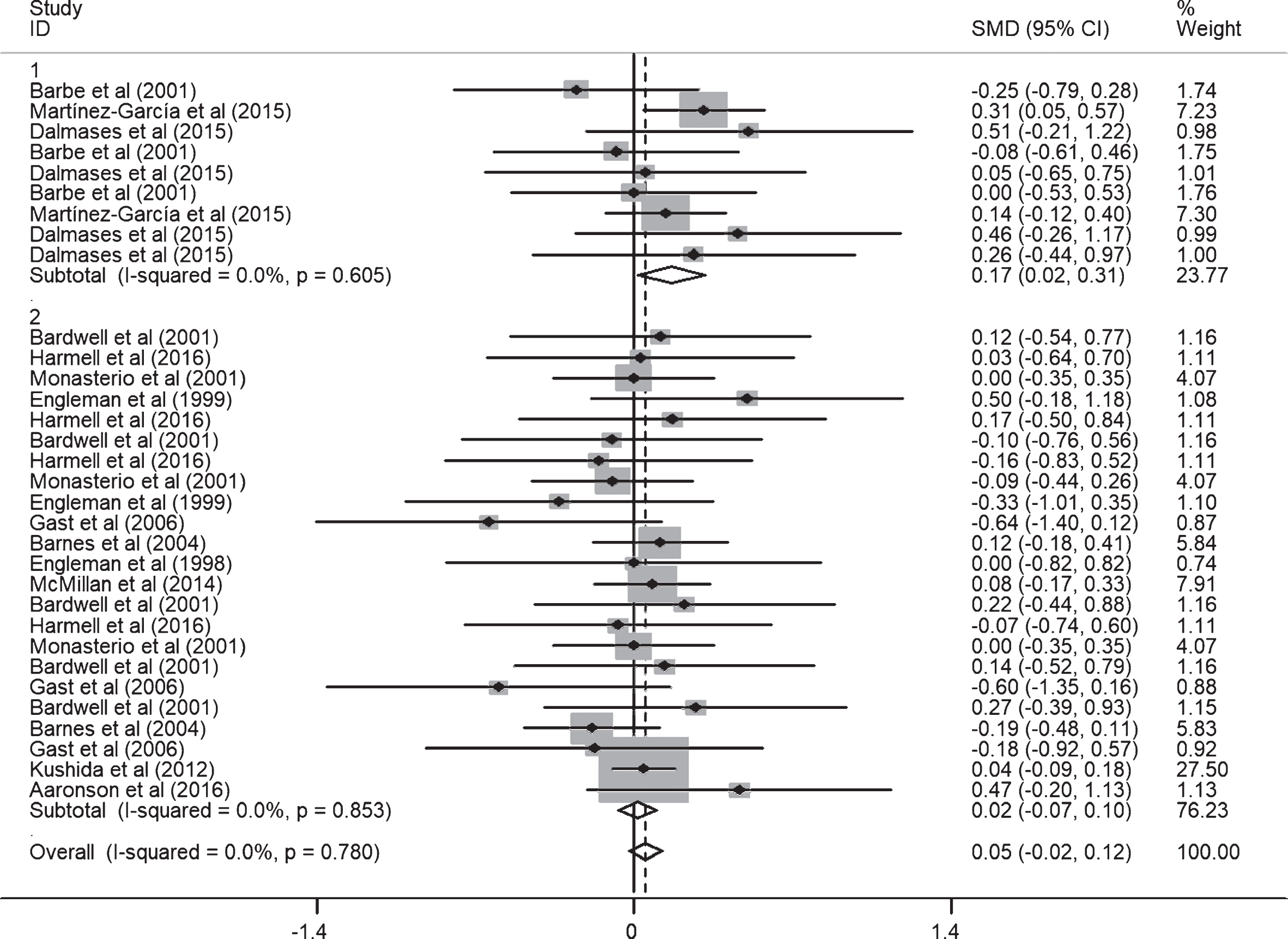
Forest plot of studies on association between CPAP and cognition: attention and speed of information processing (subgroup 1: severe OSA, subgroup 2: mild to moderate OSA).
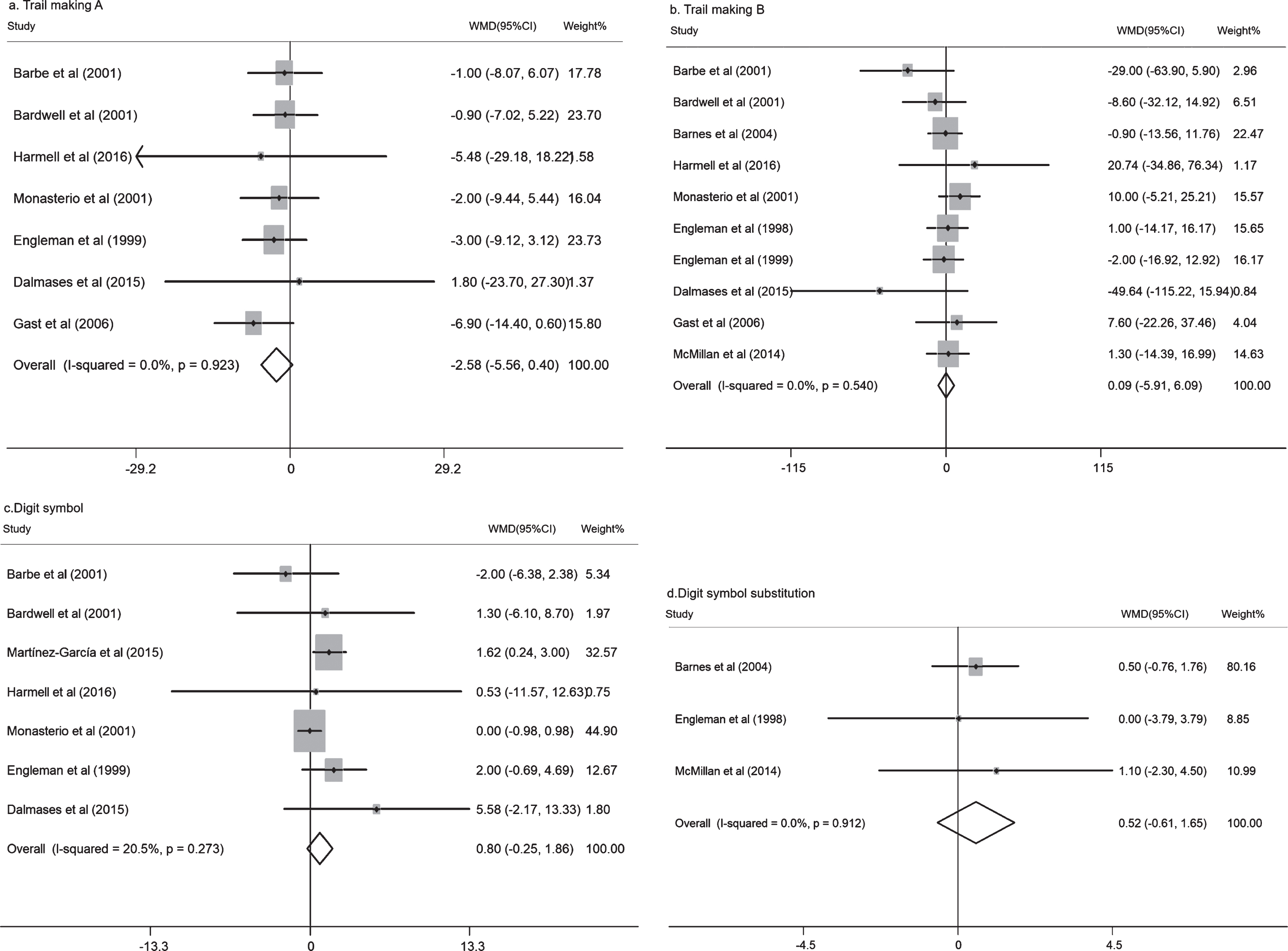
Forest plot of Studies on association between CPAP and cognition: Trail making A, Trail making B, Digit symbol, and digit symbol substitution.
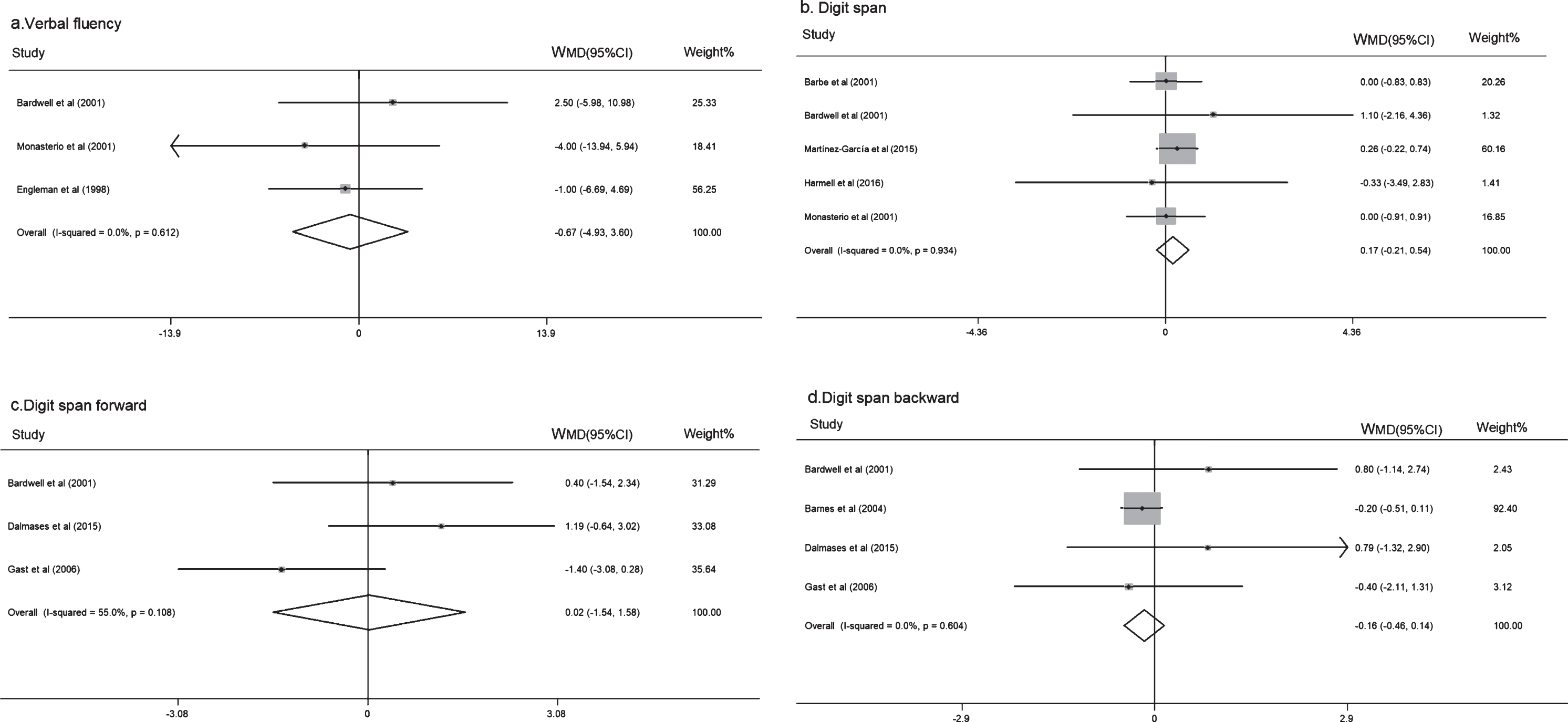
Forest plot of studies on association between CPAP and cognition: Verbal fluency, Digit Span, Digit Span Forward, and Digit Span Backward.
As there was significant heterogeneity in Epworth Sleepiness Scale (I2 = 95.8%) and Digit Span Forward (I2 = 55.0%), sensitivity analysis was performed to explore the sources of heterogeneity as well as the stability of the results. The heterogeneity of Epworth Sleepiness Scale was not improved when each study was removed sequentially, whereas that of Digit Span Forward decreased from 55.0% to 0% after removing Gast et al. [23]. No significant publication bias was found in our meta-analysis with Begg’s and Egger’s test. Funnel plot for attention and speed of information processing was displayed in Fig. 7.
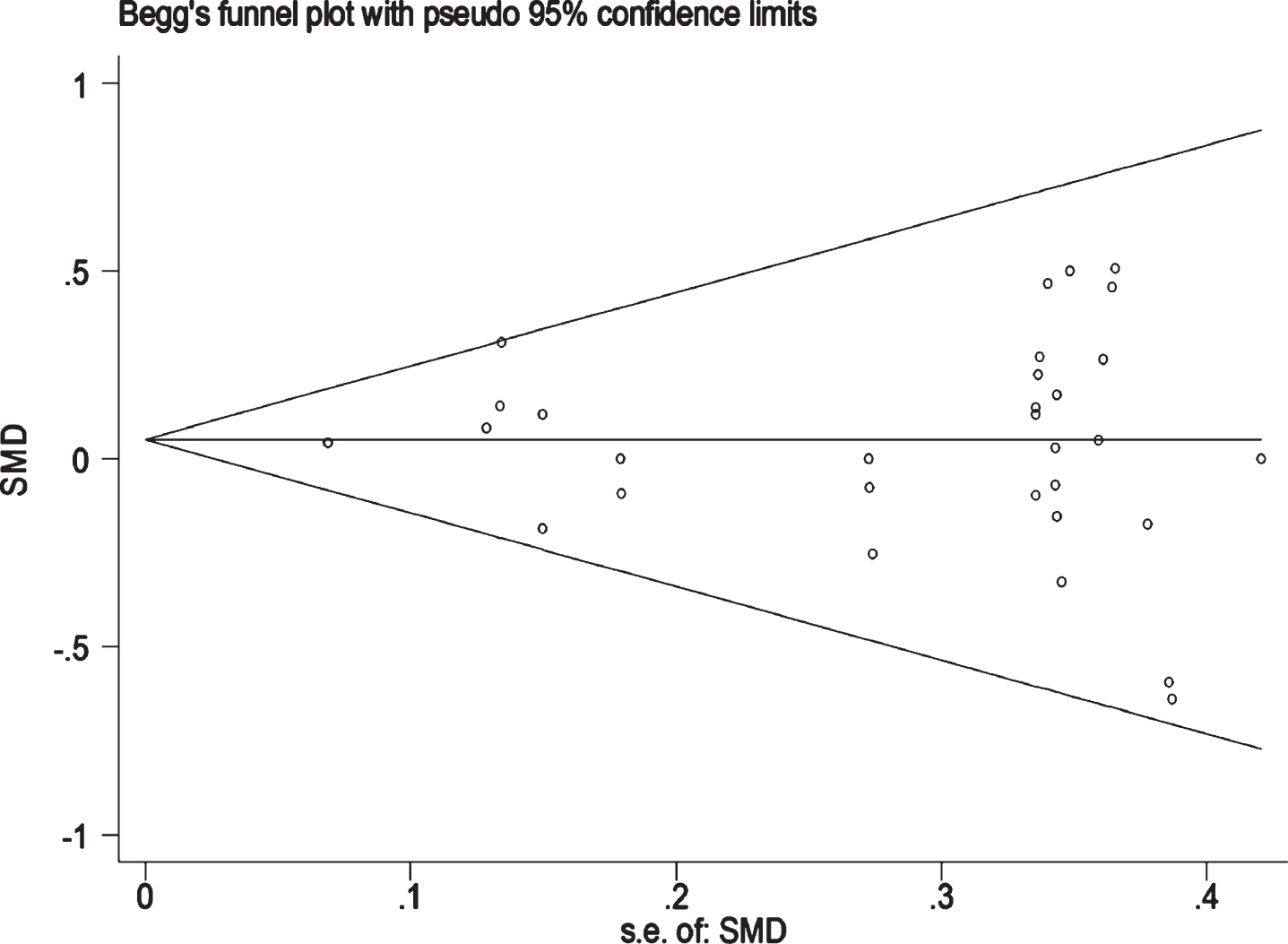
Funnel plot for attention and speed of information processing.
DISCUSSION
In this meta-analysis, CPAP treatment could significantly improve attention and speed of information processing in patients with severe OSA. However, the improvement was not observed in other cognitive domains. The results were in line with the previous meta-analyses conducted in all participants, which showed that CPAP could partially improve cognitive function, with a small but significant effect on attention and vigilance [16, 17].
It is known that the speed of information processing is essential to the downstream processes of attention and executive functions [29], all of which are associated with the function of frontal lobe [30, 31]. A previous meta-analysis revealed that frontal cortex is one of the lobes that are most likely to display atrophy in OSA patients [32], which could partially be reversed by CPAP treatment [33]. Although significant effect size of executive function in severe OSA patients was observed, only two clinical trials were included in the analysis, so we fail to make an exact conclusion. Hence, more observations are needed to verify the authenticity of the conclusions.
Interestingly, only patients with severe OSA benefit from CPAP treatments in the analysis. It was found that patients with mild OSA were less likely to be successfully treated than those with severe OSA syndrome [34]. It is recognized that the effectiveness of CPAP therapy is time-dependent [35] and associated with the compliance of CPAP [36]. Compared with those with mild and moderate OSA, patients with severe OSA were reported to have a better compliance to CPAP treatment [37, 38], and therefore, a longer treatment duration and better therapeutic effectiveness.
In the current meta-analysis, most cognitive domains did not achieve significant improvements, which might be due to the following factors. First, the treatment duration is not sufficiently long for the biological and structural recovery of the brain. Previous study has showed that continuous CPAP treatment for 3 months could significantly increase the connectivity of right middle frontal gyrus [20]. If the treatment lasted for 6 months, the change of Cho/Cr in the hippocampus could be reversed, whereas no change was observed in the frontal lobe [39]. Similarly, another study revealed that the change of white matter was very limited after 3 months’ treatment, whereas both the change of white matter and cognitive function could be completely reversed if the treatment lasted for 12 months [35], which indicates a time-dependent effect of CPAP treatment. Although mounting evidence have indicated that CPAP treatment could decrease Aβ42, normalized CSF Aβ42 and t-tau/Aβ42 ratio [40], there is still a long distance from pathological change to clinical improvement. In the current meta-analysis, the treatment duration in most of the studies were no more than 6 weeks; hence, treatment with longer duration is needed in the future to achieve obvious cognitive improvement. Second, the poor compliance of CPAP might dilute the effectiveness of treatment. Previous studies found that the effectiveness of CPAP treatment is closely related to the hours of treatment in routine clinical practice [41, 42]. The whole-night effective AHI < 5 could only be achieved when CPAP treatment lasted for more than 6 h per night, otherwise the effectiveness occurred only in non-supine position [43]. In fact, a great number of patients cannot tolerate the side effects of CPAP in spite of its effectiveness [44]. The average usage of CPAP in this meta-analysis was only 3.8 h per night, which indicates poor compliance and acceptance as well as limited improvement of cognition. Third, the clinical phenotypes and endotypes of OSA may affect the outcomes of CPAP treatment. It was found that if the patient had a lack of subjective daytime sleepiness, CPAP treatment could not improve their cognitive function in spite of the severity of OSA [14]. In addition, compared to patients with subjective daytime sleepiness, those without the symptom had mild hypoxemia, less sleep fragment, and poor CPAP compliance [45]. Therefore, treatment based on clinical phenotype is of great importance to the therapeutic effect and prognosis of OSA patients [46]. It is known that different pathogenetic mechanisms (endotypes) might lead to similar phenotype. Therefore, further exploration according to the endotypes of OSA might facilitate the precise treatment.
There are some limitations in our meta-analysis. First, we were unable to access all the outcome data from the studies even though we have transformed the data via statistical method or have asked the authors. We have contacted 8 authors for insufficient data; however, only 2 of them replied, which undermined the strength of the finding. Second, we tried to obtain information about relevant grey literature that has been completed but never been published through the following ways: 1) The International Clinical Trials Registry Platform Search Portal; 2) formal letters of request to colleagues for information about the unpublished studies. Unfortunately, we did not find the relevant grey literature that could minimize the bias of the meta-analysis. Third, the majority of the studies enrolled around 50 participants, whereas one study enrolled nearly 1,000 participants; thereby, the main effect may be partially driven by the results from the study. Finally, the cognitive function in the current meta-analysis was divided into several domains, each of which is evaluated by multiple scales and some of which may lack certain sensitivity and representativeness.
In summary, our meta-analysis found that CPAP treatment could only improve attention and speed of information processing in patients with severe OSA. Future studies need to pay more attention to the following aspects: 1) the effects of long-term CPAP treatment on cognitive function; 2) methods to increase the compliance and adherence of CPAP; and 3) precise therapy based on clinical phenotypes and endotypes.