
Abstract
Background:
Obstructive sleep apnea (OSA) is associated with cognitive disorders, but little is known about prevalence of co-occurring OSA and mild cognitive impairment (MCI) as well as about co-occurring OSA and Alzheimer’s disease (AD). Pathophysiological models integrating OSA, cognitive deficits and neurodegeneration remain speculative. Findings in this area could contribute to the knowledge about pathophysiological processes in cognitive disorders and neurodegenerative processes, be helpful for the diagnosis of cognitive disorders and provide approaches for the treatment of cognitive disorders.
Objective:
Examining the prevalence of OSA and patterns of cognitive deficits as well as AD biomarker profiles associated with OSA in a cohort of 104 MCI patients.
Methods:
Assessments used include: respiratory polygraphy, The Consortium to Establish a Registry for Alzheimer’s Disease Neuropsychological Battery (CERAD NB), Tau, phosphoTau181, amyloid-β-1–42/1–40, 18F-fluorodeoxyglucose positron emission tomography (F18-FDG-PET).
Results:
Prevalence of OSA of any severity: 58,7% (Apnea Hypopnea Index (AHI)≥5/h), OSA in a moderate-to-severe extent (AHI≥15/h): 25%. Only 13.1% of MCI patients with OSA reported daytime sleepiness. MCI-OSA patients showed no specific neuropsychological pattern. Presence of OSA was not associated with specific AD biomarker profiles in the whole study group besides a positive association between AD positivity in an AD biomarker sub cohort.
Conclusions:
OSA is highly prevalent in patients with MCI. It might often remain undiagnosed as only a small number of MCI-OSA patients report daytime sleepiness. OSA could contribute to MCI symptoms and even to AD pathology. Further research is needed to validate these findings and to investigate possible pathophysiological relationships between OSA and MCI as well as between OSA and AD.
INTRODUCTION
Prevalence of obstructive sleep apnea (OSA) as well as of mild cognitive impairment (MCI) increases with high age and will continue to rise due to the demographic change. Epidemiological findings suggest a relationship between the two syndromes but pathophysiological models about possible connecting mechanisms remain speculative [1–3]. MCI has multiple underlying etiologies including toxic, cerebrovascular, and neurodegenerative causes such as Alzheimer’s disease (AD) [4–6]. The clinical relevance of MCI is enormous due to its high prevalence of 7.7 to 32.9% [7–11] among patients aged >65 years and an annual progression rate to dementia due to AD of 5–15% [10, 13]. Thus, it is crucial to identify potentially reversible causes for MCI. OSA is a sleep-related breathing disorder associated with older age as well as higher body mass index (BMI) and high prevalence rates from 6% to 46% among the general population [14–16]. The standard therapy for OSA is nocturnal continuous positive airway pressure (CPAP) therapy [17].
Mounting evidence suggests an epidemiological link between OSA and MCI. Worldwide studies found prevalence rates of OSA among MCI patients between 9.9% and 55.3% for Apnea Hypopnea Index (AHI)≥15/h and between 13.8% and 70.8% for AHI of ≥5/h [18–23]. Vice versa, some authors found OSA patients at increased risk of suffering from MCI as well as for developing dementia [24, 25]. Osorio et al. found that patients suffering from sleep-related breathing (SDB) had an earlier onset of both MCI and dementia and that the treatment of SDB with CPAP can delay the progression of cognitive impairment in patients with SDB and MCI [26].
OSA primarily affects the cognitive domains vigilance, attention, and executive functions in cognitively healthy probands [27–34]. Terpening et al. investigated cognitive profiles in patients with OSA and comorbid MCI and found associations between higher AHI, increased sleep duration, reduced nocturnal oxygen saturation, and slower processing [35].
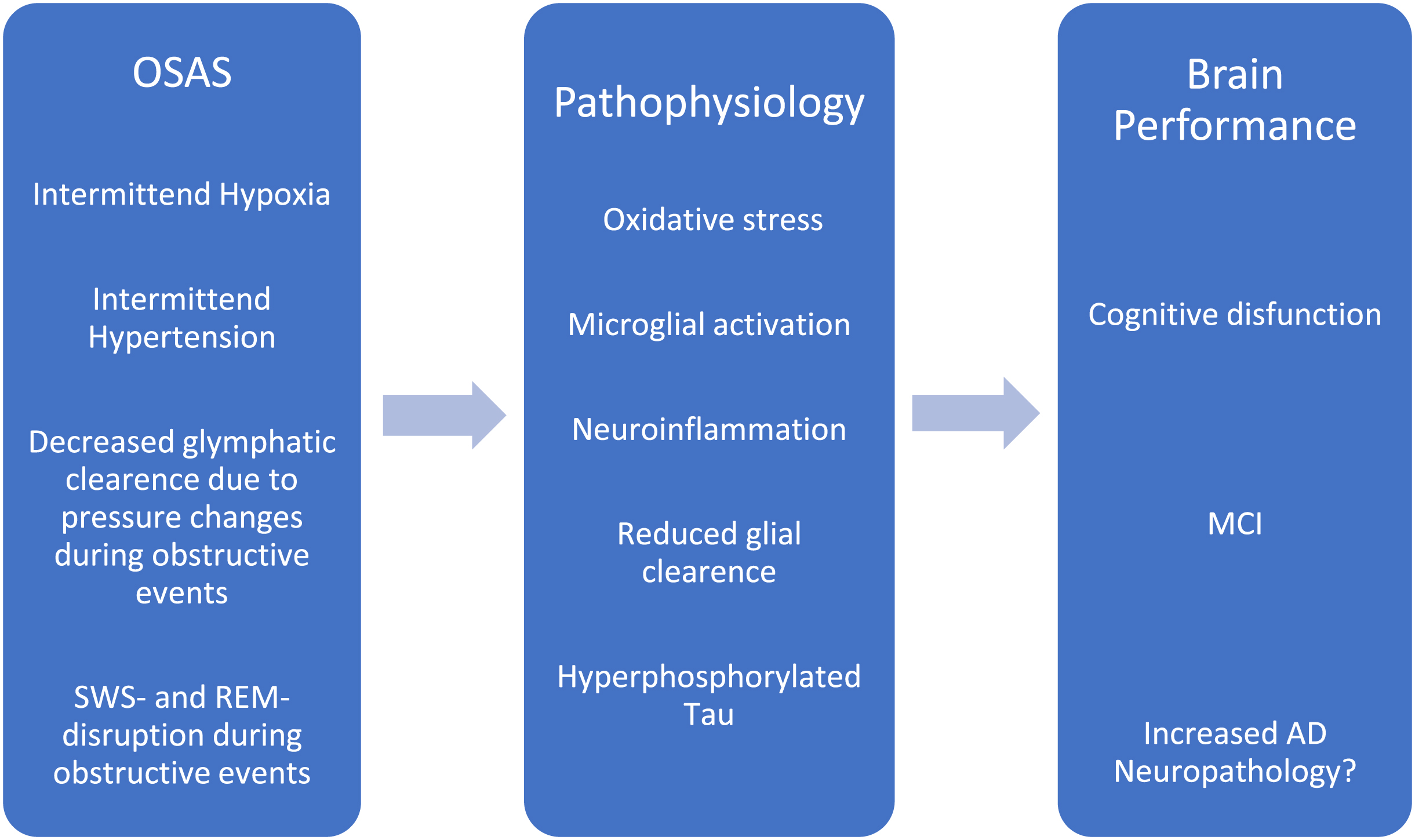
Most models assume disrupted sleep and intermittent hypoxia as probable factors facilitating the development of MCI and/or AD in OSA [3, 37]. Polsek et al. hypothesized a shared pathophysiology of AD and OSA with oxidative stress, neuroinflammation, reduced glial clearance and increased amyloid-β (Aβ) production as pathological mechanisms [38]. Figure 1 shows possible pathophysiological links between OSAS, cognitive dysfunction and neurodegeneration.
Several studies found associations between OSA respectively OSA severity and biomarkers of neurodegeneration. Sharma et al. found an association of higher OSA severity and significantly decreased cerebrospinal fluid (CSF) Aβ levels in 208 initially cognitively normal participants over the course of 2.42±0.88 years (r = –0.24; p < 0.05) but no significant correlation of OSA and pTau181 or tTau levels in CSF [39]. Bubu et al. found a significantly faster decrease of Aβ42 levels (B = –2.62; 95% CI: –3.23, –2.03; p < 0.001) as well as an accelerated increase of pTau181 (B = 1.74; 95% CI: 1.22, 2.27; p < 0.001) and tTau (B = 2.21; 95% CI: 1.58, 2.86; p < 0.001) in 103 OSA patients in comparison to 695 MCI patients without OSA over the course of 2.52±0.51 years [40]. Diaz-Roman et al. (2020) retrieved a positive correlation between tTau and AHI (r = 0.463; p < 0.01) as well as between pTau and AHI (r = 0.425; p < 0.01) in a cross-sectional study on 57 patients with MCI [41].
Ju et al. found significantly lower Aβ42 levels in CSF of 10 OSA patients as compared to 31 patients without any sleep-related breathing disorder (SDB) (717±143 pg/ml versus 914±224 pg/ml; p = 0.013) [42]. Ligouri et al. described significantly lower levels of CSF Aβ42 in untreated OSA patients (n = 25; 484.0±159.9 pg/ml) in comparison to CPAP-treated OSA patients (n = 10; 881.4±174.33 pg/ml) or to patients without OSA (n = 15; 888.4±147.88 pg/ml). The authors observed no significant differences in CSF tTau or pTau181 levels between these groups [43].
Bubu et al. used Florbetapir positron emission tomography (PET) to quantify brain amyloid burden in 516 cognitively normal, 798 MCI, and 325 AD patients with and without OSA and found significantly higher amyloid burden in cognitively normal with OSA (B = 0.06; 95% CI: 0.02,0.11; p < 0.001) and in MCI patients with OSA (B = 0.08; 95% CI: 0.05, 0.12; p < 0.001) in comparison to individuals of those groups without OSA [40]. Sharma et al. examined 208 cognitively normal subjects and showed a positive correlation between AHI and change in amyloid pathology measured by amyloid PET with Pittsburgh Compound B (PiB) after 2.50±0.88 years (r = 0.374; p < 0.05) [39]. Jackson et al. found significantly higher amyloid burden (measured by PiB PET) in 34 OSA patients in comparison to 12 age- and gender-matched controls that were free from OSA (F1,43 = 10.8; p = 0.002; Cohen’s d = 0.12) [44].
There are several clinical implications of examining the association between OSA severity and biomarkers of AD (CSF or F18-FDG-PET) in patients with MCI: Previous studies point to a possible bidirectional interaction between OSA and AD. This implies that OSA could be a risk factor for AD and AD could be a risk factor for OSA. Furthermore, both OSA and AD could result in cognitive impairment and therefore lead to a diagnosis of MCI. Therefore, it is necessary to specify the extent to which OSA severity contributes to AD risk. In particular, it is important to define AHI cutoff values of OSA severity that are associated with increased risk of MCI due to AD. This could lead to the development of guideline recommendations for OSA in patients suffering from MCI due to AD. Considering the two-way interaction of OSA and AD, another clinical implication of this association could be routine screening for sleep-related breathing disorders in AD patients.
Further studies found positive effects of CPAP treatment of OSA in patients with MCI and with AD. Ancoli-Israel et al. found improvement of cognition already after three weeks of CPAP therapy in 52 OSA patients with dementia due to AD [45]. Ligouri et al. examined 24 OSA patients suffering from MCI or dementia due to AD and found a significant slower decline on the Clinical Dementia Rating scale (CDR) in subjects adherent to CPAP therapy [46]. Further studies also point to a potentially improved cognition [47–49] as well as a reduced risk for dementia in OSA patients after applying CPAP therapy [50].
Study aim and objective
This cross-sectional study aimed to determine the prevalence of (undiagnosed) OSA in a cohort of 104 patients with MCI as prevalence estimates for OSA in MCI patients are still scarce and study results heterogenous. We compared cognitive performance, thoroughly assessed using the Consortium to Establish a Registry for Alzheimer’s Disease Neuropsychological Battery (CERAD-NB), between MCI patients with and without OSA (objectively assessed using polygraphy) in order to identify a specific cognitive profile of MCI-OSA patients. Finally, we investigated associations between presence and severity of OSA and AD biomarker profiles (CSF and F18-FDG-PET) in patients with MCI for the purpose of specifying the association of OSA severity and AD pathology on cognitive impairment.
We hypothesized a high prevalence of OSA among MCI patients, differing cognitive patterns in the CERAD-NB between MCI patients with and without OSA as well as differences in AD biomarker profiles of MCI patients with and without OSA.
This study is one of the first to examine the prevalence of OSA objectively assessed by polygraphy among MCI patients, examining a memory clinic cohort and additionally taking detailed cognitive testing (CERAD-NB) and AD specific biomarkers (CSF, F18-FDG-PET) into account.
MATERIALS AND METHODS
Participants
109 consecutive patients diagnosed with MCI in a German university-based memory clinic (Centre for Cognitive Disorders, TU Munich) between April 2017 and December 2020 underwent at-home polygraphy within 180 days of the MCI diagnosis. In three patients polygraphy data was not evaluable due to insufficient recorded sleep duration (<4 h) and in two patients the MCI diagnosis was withdrawn (CDR≥1). Finally, 104 patients were included in the study. MCI was diagnosed using standard diagnostic criteria, namely the Albert 2011 clinical core criteria [51]. Cognitive impairment was defined as deviation of ≥1.5 SD in at least one category of the CERAD-NB [52, 53]. Results of the CERAD-NB are depicted using age-, sex-, and education-adjusted z-scores.
CERAD-NB was available for 101 of 104 subjects. 50 subjects (48.1%) were characterized as single-domain amnestic type, 34 subjects (32.7%) as multi-domain amnestic, and 17 subjects (16.3%) as non-amnestic type. Characterization of 3 subjects (2.9%) was not possible due to missing CERAD scores.
Inclusion criteria were a diagnosis of MCI, CDR global score of 0.5, and willingness to participate. Exclusion criteria were a diagnosis of dementia (CDR≥1), insufficient language skills and inability to consent. See Fig. 2 for the flowchart of patient selection.
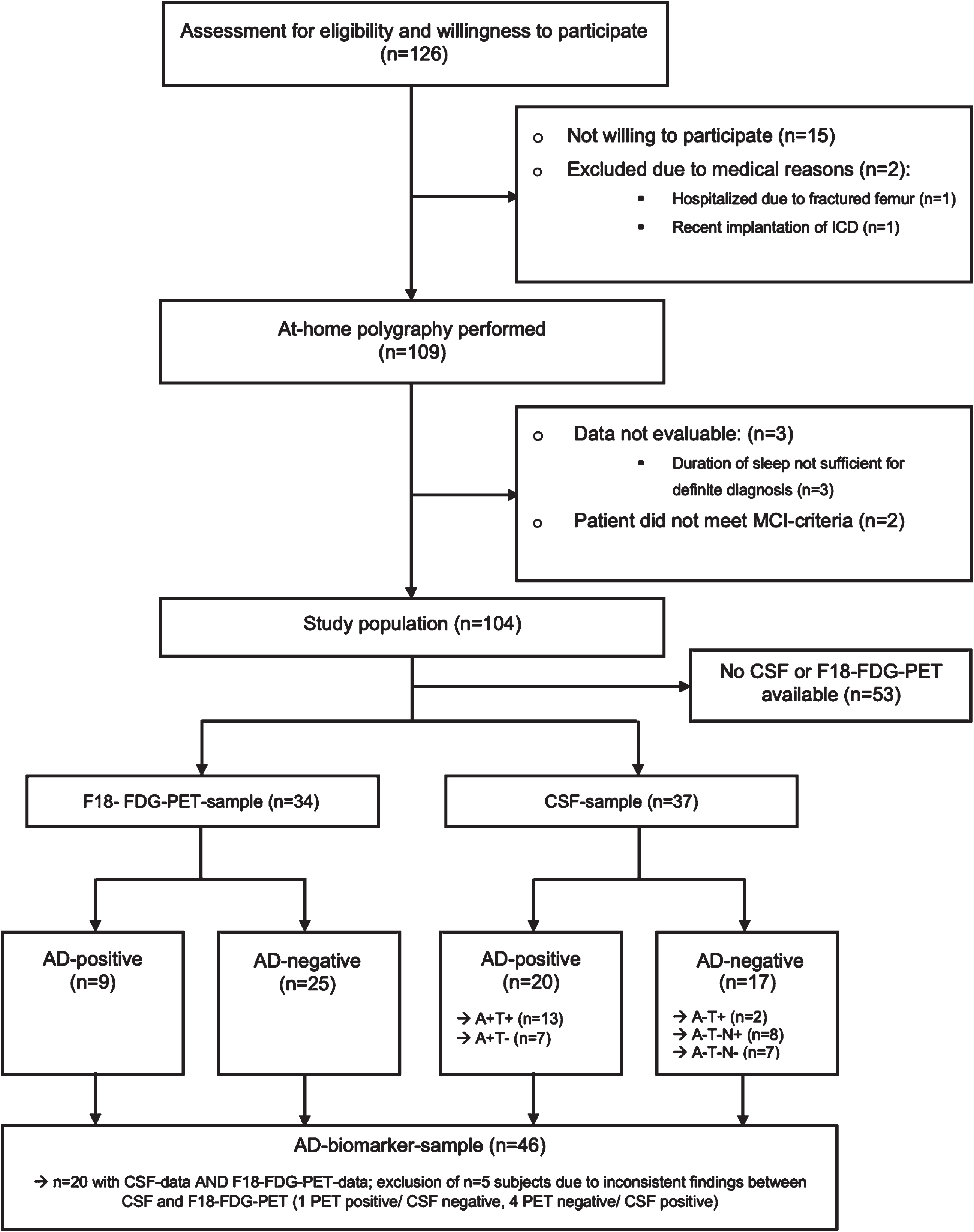
Consort 2010 Flow Diagram of patient selection.
All human subjects included in the study provided written and informed consent and were fluent in German. The study design was approved by the ethics committee of the Technical University of Munich (project code: 45/17). All clinical investigations were conducted in accordance with the Declaration of Helsinki 1964 and its amendments and followed the Guidelines of Good Clinical Practice (GCP).
Assessments and procedures
See Table 1 for the description of the used assessment tools.
Assessments
CERAD-NB, Consortium to Establish a Registry for Alzheimer’s Disease Neuropsychological Battery; CSF, cerebrospinal fluid; t-tau, total-tau; p-tau 181, phosphorylated tau 181; Aβ, amyloid-β; F18 FDG PET, F18 fluorodeoxyglucose positron emission tomography.
Overnight at-home polygraphy was performed using “MiniScreen Plus” devices by “Löwenstein Medical” (Bad Ems, Germany). Several guidelines (The American Academy of Sleep Medicine/-guideline, German S3-guideline) state that single-night at-home testing is acceptable in uncomplicated patients with a high pretest probability of OSA [54–56]. As subjects undergo polygraphy at home, no adaption night is needed. This is clinical routine in diagnosing OSA. On the day of their scheduled polygraphy participants were instructed on how to use the polygraphy devices or, if proper use could not be guaranteed, devices were attached to the patients by trained study group members. All sleep examinations were manually scored in 2-min steps by a trained study group member according to the scoring guidelines of the AASM [57]. If total sleep time was below the accepted minimum of 4 h or any sleep data was missing (e.g., nasal flow, breathing excursion, SpO2), the examination was not included in theanalysis.
Apnea was defined as a nasal airflow reduction of ≥90% lasting for at least 10 s, hypopnea as a nasal airflow reduction of ≥30% combined with a blood oxygen desaturation of ≥3% lasting for at least 10 s. AHI is calculated by summing apneas and hypopneas and dividing them by total sleep time.
Performing several nights of sleep apnea testing might have increased diagnostic accuracy [58]. After weighing the advantages of single-night polygraphy (increased rate of acceptance by subjects) against the risk of underestimating OSA prevalence we decided to perform single night polygraphy. Indeed, OSA prevalence among MCI patients might be even higher than stated in this study.
Subjects were stratified into different OSA severity subgroups: no OSA (AHI < 5/h), mild OSA (AHI≥5/h<15/h), moderate OSA (≥15/h < 30/h), severe OSA (≥30/h). Additionally, the cohort was dichotomized according to the International Classification of Sleep Disorders (ICSD) criteria of OSA (AHI≥5/h and daytime sleepiness or AHI≥15/h), referred to as ICSD-OSA [59].
Daytime sleepiness was measured using the Epworth Sleepiness Scale (ESS), an established screening tool for daytime sleepiness [60]. An ESS Score of ≥10 was considered a pathological finding [61]. Patients were informed about their results via phone call or in writing.
Comorbidities such as depression or hypertension were extracted from the patients’ files at the memory clinic.
Lumbar puncture (LP) was performed by trained physicians following the current diagnostic standard [62]. F-18-FDG-PET scans were performed at the TUM university hospital and evaluated by a trained physician. The accepted time span between MCI diagnosis and LP or PET scan was 180 days. The AD biomarker sub-sample included patients with CSF, FDG PET or both, excluding patients with inconsistent findings between PET and CSF. LP and CSF analysis was performed in 37 patients and F18-FDG-PET in 34 patients as a part of the clinical routine diagnostic procedure. Subjects with AD compatible results in F18-FDG-PET or CSF were classified as AD+(AD positivity) while subjects without AD compatible results were classified as AD– (AD negativity).
Statistical analyses
Data was analyzed using the statistical software “Statistical Package for the Social Sciences 27 (SPSS 27)” (IBM, Armonk, New York, US). Normal distribution was tested graphically and using Kolmogorov-Smirnov Test. As the collected data did not turn out to be within normal distribution, non-parametric tests were used. Subgroups were compared by applying Mann-Whitney U Test and Kruskal-Wallis Test. Correlation was tested using Spearman correlation analysis. Furthermore, univariate, multivariate and logistic regression analyses were performed. All analyses were exploratory, consistently p-values<0.05 were considered statistically significant. Due to the exploratory nature of the study the multiple analyses were not corrected for multiplicity so that statistically significant associations cannot be considered confirmatory.
RESULTS
Patient characteristics
See Table 2 for description of the study population.
Sociodemographic and clinical characteristics of study population (n = 104)
BMI, body mass index; AHI, Apnea-Hypopnea-index; AI, Apnea-Index; HI, Hypopnea-Index; ESS, Epworth Sleepiness Scale; MMSE, Mini-Mental State examination; CDR SOB, Clinical Dementia Rating scale, Sum of Boxes; CDR Global, Clinical Dementia Rating Scale Global score; *CDR was assessed in 102 of 104 patients.
Comparison of patients with MCI and OSA and patients with MCI without OSA
See Table 3 for sociodemographic, clinical and neuropsychological parameters stratified by OSA severity. In particular, there was no significant effect of OSA severity on any cognitive test result.
Sociodemographic and clinical parameters stratified by OSA-severity
BMI, body mass index; AHI, Apnea Hypopnea Index; ESS, Epworth Sleepiness Scale; MMSE, Mini-Mental State examination; CDR SOB, Clinical Dementia Rating scale Sum of Boxes; CDR Global, Clinical Dementia Rating Scale Global score.
See Table 4 for comparison of demographic and cognitive parameters of the total cohort dichotomized into OSA+ and OSA– using ICSD criteria for diagnosing OSA (OSA– : AHI < 5/h or AHI≥5/h and <15/h & ESS < 10; OSA+: AHI≥15/h or AHI≥5/h and <15/h & ESS≥10). In particular, there was no significant difference between the OSA+ and OSA– MCI group on any cognitive test result but constructional praxis.
Comparison of OSA+and OSA- subjects dichotomized by ICSD-criteria
BMI, body mass index; AHI, Apnea Hypopnea index; ESS, Epworth Sleepiness Scale; MMSE, Mini-Mental State examination; CDR SOB, Clinical Dementia Rating scale Sum of Boxes; CDR Global, Clinical Dementia Rating Scale Global value.
AD biomarker sub-sample
AD biomarkers were available for 51 subjects, either CSF (n = 37) or F18-FDG-PET scan (n = 34) or both (n = 20). 5 of 20 patients who underwent LP as well as PET scan had inconsistent results (1 PET positive/CSF negative, 4 PET negative/CSF positive) and therefore were excluded from the AD biomarker sub-sample. The final AD biomarker sample consisted of 46 subjects. The sociodemographic and clinical parameters of the AD biomarker sub-sample did not differ significantly from the rest of the cohort (not depicted). For comparison of sociodemographic and clinical parameters of AD-positive (n = 19) and AD-negative (n = 27) subjects of the AD biomarker sub-sample see Table 5.
Comparison of AD-positive and AD-negative subjects
BMI, body mass index; YOE, years of education; MMSE, Mini-Mental State examination; CDR SOB, Clinical Dementia Rating Scale Sum of Boxes; AHI, Apnea Hypopnea Index; ESS, Epworth Sleepiness Scale; Mean O2, Mean nocturnal peripheral O2-Saturation; T90, Percentage of nocturnal time spent below 90% peripheral O2-saturation; AD-positive, CSF or PET compatible with AD
The main findings of the comparison of clinical parameters of AD+ and AD– patients were significantly higher BMI (p < 0.001) and significantly lower mean SpO2 levels (p = 0.01) in AD– subjects.
Additionally, we analyzed associations of AD biomarkers and parameters of disordered breathing within subjects suffering from ICSD-OSA (diagnosed according to ICSD criteria: AHI≥5/h and daytime sleepiness or AHI≥15/h) in the AD biomarker sub-sample (n = 12).
Besides from age and BMI, AHI was correlated with AD positivity (r = 0.615; p = 0.033) in this subgroup.
We conducted further univariate and multivariate regression analyses and investigated correlations between sleep-related (AHI, T90, mean SpO2) and sociodemographic parameters (BMI, age, sex) with total Tau as well as between AD– positivity and sociodemographic parameters (BMI, age, sex) with AHI (please see Supplementary Tables 1–6). While none of the above-mentioned regression models predicts the influence of any independent variable on the dependent variable AHI (see Supplementary Tables 2 and 3), the independent variable BMI was inversely associated with total-Tau (see Supplementary Table 4). A regression model including BMI, age, years of education and AHI as independent variables suggests potential influence on the dependent variable total Tau (adjusted R-squared 0.182; p = 0.045). It has to be noted that BMI is the only significant independent variable within this model (see Supplementary Table 1).
DISCUSSION
Research question, study objectives, and main findings
The research question of this study was the association between OSA and AD pathology in MCI. The study objectives were prevalence of OSA and the association of OSA with patterns of cognitive deficits and AD biomarkers in older adults with MCI. The main findings were that 58.7% of adults with MCI of this study group had OSA and only 13.1% of them reported daytime sleepiness. There were no significant associations between presence of OSA and neuropsychological test results or AD biomarkers. However, a positive association between AD biomarkers and AHI was found in a small group (n = 12) with MCI and ICSD-OSA (AHI≥5/h and daytime sleepiness or AHI≥15/h).
OSA prevalence in this study compared to the general population, to elderly populations and to MCI cohorts
This study is one of the few to estimate the OSA prevalence among MCI patients in a memory clinic cohort. The overall OSA prevalence was 58.7% (AHI≥5/h) and 25.0% for moderate-to-severe OSA (AHI≥15/h), respectively 27.9% applying to ICSD criteria (taking daytime sleepiness into account).
Table 6 presents the rates of mild and of moderate-to-severe OSA of our study in comparison to other studies in the general population, in elderly populations and in MCI patients.
Comparison of OSA prevalence rates: own results, general population, elderly, MCI patients
PSG, polysomnography; PG, polygraphy; f, female subjects.
Comparability of OSA prevalence rates of different studies is complicated by varying diagnostic and selection criteria as well as diverging cut-offs for both OSA and MCI [63, 64]. Consequently, studies about OSA prevalence often provide heterogenous results. Consistent with that, a systematic review by Senaratna et al. found varying prevalence rates for OSA from 9% to 38% in the general population [16].
The high prevalence of 58.7% for OSA of any severity and 25% for mild-to-moderate OSA within our study cohort is higher than the prevalence rates in the general population and higher than in studies among elderly, cognitively normal groups [65]. It is comparable to another elderly study group of cognitively normal subjects with higher mean BMIs and a higher obesity rates (35% versus 13.5% in our cohort) as additional factors causing OSA and might additionally entail selection bias as 71% of this cohort did not consent to in-laboratory polysomnography [14].
Reliable data about OSA in MCI patients remain scarce. In comparison to the inconsistent findings of 13.8% –70.8% OSA prevalence in different MCI cohorts the OSA prevalence of our study ranges in the high section of those OSA rates, while the generalizability of two comparator studies is reduced due to a small sample size (n = 30) in one investigation [22] and a higher BMI rates (27.5±5.5 kg/ m2) as a promoting factor for OSA in the other one [21].
A review by Mubashir from 2019 investigating five studies found varying OSA prevalences of 11%–71% among MCI patients and interpreted this as due to heterogenous cohorts and different diagnostic criteria [23]. Further studies estimating OSA prevalence in MCI patients found numbers ranging from 4.4% to 58.7% [19, 66].
OSA/MCI and daytime sleepiness
One of the most frequent symptoms of OSA is daytime sleepiness, former studies mostly quantified daytime sleepiness using the Epworth Sleepiness Scale (ESS).
In our cohort only 13.1% of all OSA patients and 19.2% of moderate-to-severe OSA patients showed considerable daytime sleepiness in the ESS (Score≥10). The ESS could not discriminate between OSA and non-OSA in this MCI cohort. This finding is consistent with previous studies that also showed weak associations between OSA and pathological ESS scores [14, 68]. In addition, it might be possible that MCI patients have difficulties describing OSA daytime symptoms due to cognitive deficits. Consequently, OSA might often remain undiagnosed in MCI patients when using the ESS as a screening tool. This might be an argument for early or even routine polygraphy in MCI patients.
OSA and cognition
Former studies found different effects of OSA on cognitive function among non-demented subjects, mainly influencing vigilance, attention and executive functions [27–34]. In this cohort of MCI subjects, we did not find significant effects of OSA presence or severity on specific cognitive domains of the CERAD-NB, indicating that there is no specific neuropsychological pattern in patients with MCI and OSA.
This might have several reasons:
Firstly, the patients with OSA from this cohort had only moderately elevated mean AHIs with most of them suffering from mild-to-moderate OSA (median AHI: 12.3/h mean 16.08/h). In contrast, several studies which showed significant effects of OSA on cognition, examined patients with higher AHI values [27, 69].
Secondly, the AHI as a singular parameter determining the severity of OSA may not be sufficient. Cognitive effects of OSA might not only be influenced by the number of apneas but also by further parameters such as desaturations, total length of apneas or sleep microarchitecture [70]. In order to evaluate the complex association of AHI and cognitive domains more specific parameters might be needed. Such an approach was used by Kulkas et al. They tried to distinguish OSA severity and evaluated further parameters like “obstruction severity”, “desaturation severity”, “obstruction duration”, and “desaturation duration”. Interestingly this study found differences in mortality between two subgroups with similar AHI but diverging parameters of apnea and desaturation severity and duration [71]. We also performed regression and correlation analysis within the total cohort taking mean SpO2 and T90 into account (data not shown). In contrast to AHI, T90 correlated with the clock drawing test (Spearman correlation; r = 0.223; p = 0.02) indicating that there might be an association of OSA parameters and cognition besides AHI. We therefore propose to consider further parameters such as the severity and duration of desaturations/apneas when examining the association of sleep related breathing and cognition in the future.
Thirdly, the cross-sectional design might not be suitable to evaluate the effect of OSA on cognition. Consistent with our findings a meta-analysis by Bubu et al. found little effects of OSA on cognitive parameters in patients aged older than 60 years using cross-sectional designs [2].
Fourthly, MCI can be caused by different etiologies and pathophysiological processes with varying effects on single cognitive domains, making it hard to discriminate effects of OSA.
OSA and CSF biomarkers for neurodegeneration
Prevalence of OSA among AD patients is sparsely investigated [72, 73]. Although some studies suggest associations between OSA and CSF AD biomarker profiles, we did not find significant associations between OSA parameters and CSF AD biomarkers in this MCI cohort. This might be due to the fact that former studies predominantly examined the association between OSA and CSF biomarkers in patients suffering from OSA of higher severity. Mean AHI in our OSA cohort was 16.08/h whereas mean AHIs in other studies cohorts examining correlations between OSA and AD biomarkers ranged from 25.56 to 36.34/h [41–43]. Focusing on subjects with OSA according to ICSD criteria within our cohort, we found a positive association of AHI with AD positivity (r = 0.615; p = 0.033; n = 12; see Table 6). Within this small subgroup AD+ subjects had significantly higher AHI than AD- subjects (28.45/h versus 19.9/h; p = 0.048; see Supplementary Table 5). Given the small numbers among this subgroup, this finding has to be interpreted with caution but could hint to a pathophysiologic connection between OSA and AD pathology. Undoubtedly, further longitudinal studies examining larger cohorts are needed to evaluate CSF biomarkers among OSA-MCI patients with at least moderate-to-severe OSA.
AD+ and AD– subjects did not differ statistically in AHI or T90, whereas a significantly lower nocturnal mean SpO2 in AD-negative subjects was observed (94.0 versus 92.63%; p = 0.01). This might be related to higher mean BMIs of the AD-negative subjects (27.26 versus 22.5 kg/m2; p < 0.001; see Table 4) as obesity is linked to impaired oxygenation and reduced SpO2 values [74, 75].
OSA, AD positivity, and BMI
Subjects with AD positivity had significantly lower BMI than patients with AD negative status. This finding is in line with other studies linking lower BMI to higher amyloid burden and higher AD prevalence [76–79]. Guo et al. (2022) additionally suggested that weight decline precedes MCI and dementia by many years [80]. Since OSA is associated with higher BMI we examined a possible statistical association between AD positivity and BMI in the context of OSA but did not find any statistical hints for this relationship in our study group.
OSA and education
Consistent with the former studies presence of OSA was associated with lower educational level in this cohort [81].
Strengths and limitations
This study has several strengths: OSA was measured using validated at-home polygraphy devices instead of screening questionnaires. Conducting polygraphies at the subjects’ homes resulted in greater acceptance of the method in comparison to in-laboratory diagnostics and consequently reduced a possible recruitment bias. Detailed neuropsychological data of the CERAD-NB was available in almost all subjects (101 of 104 subjects).
Limitations
In comparison to the diagnostic gold standard of in-laboratory polysomnography, a polygraphy offers less diagnostic accuracy. CSF and PET data was not available for all subjects resulting in smaller subsamples. Due to the exploratory nature of the study, the multiple analyses were not corrected for multiplicity so that statistically significant associations cannot be considered confirmatory.
Conclusion
In conclusion, OSA is highly prevalent among MCI patients. A high number of those patients did not report any daytime symptoms in the ESS which indicates a high number of subjectively asymptomatic MCI patients with OSA and that the ESS is not a rational screening tool for OSA in MCI patients. Using a cross-sectional design, we were not able to identify specific cognitive profiles of OSA-MCI. Our findings indicate that there may be an association between AD pathology and OSA of higher severity.
Future studies linking OSA and AD should therefore focus on moderate-to-severe cases of OSA. We recommend that OSA screening should be implemented in routine diagnostic work-up of MCI.
Reasons for the high frequency but apparently mild importance of OSA in the subjects of this study could be: 1) the influence of OSA on cognition and AD pathology may be less than initially assumed; 2) the influence of OSA on cognition and biomarkers only becomes relevant with more severe OSA; 3) the influence of OSA on cognition and biomarkers only becomes relevant in more severe cognitive disorder; 4) OSA-associated cognitive impairment is not appropriately reflected in the CERAD; and 5) the cross-sectional design of the study is not ideal for examining the association of OSA and AD but hints towards a possible interaction of OSA and AD. Still, this exploratory pilot study might pave the way for further (longitudinal) research concerning this question.
AUTHOR CONTRIBUTIONS
Dirk Schwerthöffer (Conceptualization; Methodology; Supervision; Validation; Writing – original draft; Writing – review & editing); Timo Grimmer (Conceptualization; Project administration; Supervision; Formal analysis; Writing – review & editing); Tim Haselwarter (Data curation; Formal analysis; Writing – original draft).
Footnotes
ACKNOWLEDGMENTS
We would like to thank all patients willing to participate in this study. Furthermore, we thank all psychiatrists of the Centre for Cognitive Disorders, Technical University Munich for supporting this project.
FUNDING
Polygraphy devices were provided free of charge by Löwenstein Medical (formerly “Heinen & Löwenstein”).
CONFLICT OF INTEREST
Prof. Grimmer received consulting fees from AbbVie, Alector, Anavex, Biogen, Cogthera, Eli Lilly, Functional Neuromodulation, Grifols, Iqvia, Janssen, Noselab, Novo Nordisk, NuiCare, Orphanzyme, Roche Diagnostics, Roche Pharma, UCB, and Vivoryon; lecture fees from Biogen, Eisai, Grifols, Medical Tribune, Novo Nordisk, Roche Pharma, Schwabe, and Synlab; and has received grants to his institution from Biogen, Eisai, and Roche Diagnostics.
DATA AVAILABILITY
The datasets generated and/or analyzed during this study are available from the corresponding author on reasonable request. However, due to the nature of pseudonymized patient data, a material transfer agreement is required to meet ethical standards and data privacy laws of Germany.