
Abstract
Background:
Discordance among amyloid biomarkers is a challenge to overcome in order to increase diagnostic accuracy in dementia.
Objectives:
1) To verify that cerebrospinal fluid (CSF) Aβ42/Aβ40 ratio (AβR) better agrees with Amyloid PET (Amy-PET) results compared to CSF Aβ42; 2) to detect differences among concordant positive, concordant negative, and discordant cases, basing the concordance definition on the agreement between CSF AβR and Amy-PET results; 3) to define the suspected underlying pathology of discordant cases using in vivo biomarkers.
Method:
We retrospectively enrolled 39 cognitively impaired participants in which neuropsychological tests, apolipoprotein E genotype determination, TC/MRI, FDG-PET, Amy-PET, and CSF analysis had been performed. In all cases, CSF analysis was repeated using the automated Lumipulse method. In discordant cases, FDG-PET scans were evaluated visually and using automated classifiers.
Results:
CSF AβR better agreed with Amy-PET compared to CSF Aβ42 (Cohen’s K 0.431 versus 0.05). Comparisons among groups did not show any difference in clinical characteristics except for age at symptoms onset that was higher in the 6 discordant cases with abnormal CSF AβR values and negative Amy-PET (CSF AβR+/AmyPET–). FDG-PET and all CSF markers (Aβ42, AβR, p-Tau, t-Tau) were suggestive of Alzheimer’s disease (AD) in 5 of these 6 cases.
Conclusion:
1) CSF AβR is the CSF amyloid marker that shows the better level of agreement with Amy-PET results; 2) The use of FDG-PET and CSF-Tau markers in CSFAβR+/Amy-PET–discordant cases can support AD diagnosis; 3) Disagreement between positive CSF AβR and negative Amy-PET in symptomatic aged AD patients could be due to the variability in plaques conformation and a negative Amy-PET scan cannot be always sufficient to rule out AD.
INTRODUCTION
Current diagnostic guidelines for Alzheimer’s disease (AD) suggest the use of amyloid positron emission tomography scan (Amy-PET) as an alternative test to cerebrospinal fluid (CSF) analysis in order to identify amyloid-β (Aβ) pathology in a clinical or preclinical phase [1–3]. Nevertheless, in some circumstances, Amy-PET has failed to prove the presence of Aβ pathology in familial and sporadic AD cases [4]. While diagnostic recommendations exist in cases of discordant results between amyloid and neuronal injury biomarkers (interclass biomarkers incongruence) [2], no explicit recommendations exist in cases of intraclass biomarkers incongruence (IBI), as in cases of discordance between CSF and PET Aβ markers (Aβ IBI). Recently, in order to identify AD pathology in its preclinical stages, the National Institute on Aging and the Alzheimer’s Association Workgroup’s Research Framework proposed a biomarker classification scheme which divides the major AD biomarkers into three categories (A, T, N), defined on the basis of the corresponding pathologic change: “A” refers to Aβ pathology as measured either by PET or in the CSF as Aβ42 concentration or Aβ42/β40 ratio (AβR); “T” refers to Tau pathology as measured by Tau-PET or CSF phosphorylated Tau (p-Tau); “N” refers to neurodegeneration or neuronal injury and dysfunction, as measured by brain magnetic resonance imaging (MRI), by [18]F-Fluoro-deoxyglucose positron emission tomography (FDG-PET), or by CSF total Tau (t-Tau). While “A” and “T” biomarker categories are specific for AD diagnosis, “N” can reflect a neurodegenerative process in different neurological diseases. Moreover, “A” is essential in defining the initial “AD pathologic change”, and in the presence of other biomarkers is essential in confirming the trajectory in the “AD continuum” [5]. Thus, Aβ IBIs may represent a major limit to a precise diagnosis of AD. The percentage of Aβ IBIs ranges between 10% and 20% in both normal elderly and patients [6, 7] and it is higher at an earlier stage of disease [8–10]. Then it is possible that Aβ IBIs depend on the capability of CSF Aβ markers to detect earlier alterations in the AD trajectory but this supposition is still controversial [11]. Results from a quantitative PET data study reveal that the association between CSF and PET Aβ markers is nonlinear, it is modulated by the plasma apolipoprotein E (ApoE) genotype, and it is absent for their longitudinal changes [12]. More recent evidence recommends the use of CSF AβR rather than the absolute value of CSF Aβ42, to reduce Aβ IBIs and to improve AD diagnosis [7]. In this regard, many studies confirm the advantages in using CSF AβR instead of CSF Aβ42 alone in order to improve the agreement between CSF and Amy-PET results [13–19] and to better distinguish between AD and non-AD dementia [13, 20–23]. These findings have also been confirmed by neuropathology [24]; anyway, the accuracy of any CSF and PET Aβ marker shows some limitations in detecting Aβ plaques in comparison with neuropathology [24–28]. Since the current trend to define AD pathology using a “biological definition” instead of a “clinical definition” [5], it is essential to reduce Aβ IBIs and clarify how to interpret discordant results in dementia research and in clinical practice.
The aims of this study were 1) to verify whether CSF AβR differs from CSF Aβ42 in detecting Aβ pathology and to assess which of these two tests better agrees with Amy-PET results in a sample affected by cognitive decline; 2) to classify each case in the “concordant” or “discordant” group according to the absence/presence of Aβ IBI and to detect differences among groups; 3) to define the suspected underlying pathology of discordant cases using clinical data and available in vivo biomarkers (CSF AβR, CSF p-Tau, CSF t-Tau, FDG-PET, Amy-PET).
Overall, the scope of this study was to improve the diagnostic work-up with biomarkers in cognitive decline; other objectives such as to define the accuracy of each biomarker were not part of this project.
MATERIALS AND METHODS
Study design
This is a single-center, cross-sectional retrospective observational study that involves 39 participants affected by cognitive decline; the study was conducted at the University of Florence, Neurology Unit, between 2017 and 2019. This is a pilot study with the aim to obtain preliminary data about the level of agreement between CSF Aβ biomarkers and Amy-PET results. Study procedures and data analysis have been performed in accordance with the ethical standards of the Committee on Human Experimentation of our Institute and the study was approved by the local Institutional Review Board (reference 15691_oss).
The inclusion criteria were: 1) AD or mild cognitive impairment (MCI) due to AD had to be possible diagnoses (typical and atypical presentations both admitted); 2) participants had to have already performed an extensive diagnostic work-up as part of clinical routine, including neuropsychological tests, ApoE genotype determination, brain CT/MRI, FDG-PET scan, Amy-PET scan, CSF analysis; 3) CSF samples of participants had been stored at –80°C and had to be available, in appropriate quantity, to perform further analysis.
Participants (or their caregivers) gave informed consent for all procedures. Cases were not enrolled if a stroke was documented at the onset of cognitive symptoms or when a relevant vascular load was detectable on the brain CT/MRI (Fazekas score above 2) [29, 30]. With these criteria, 39 cases were consecutively enrolled.
Clinical procedures
Diagnoses have been made according to current diagnostic criteria for MCI [2], AD [1], and frontotemporal dementia (FTD) [31, 32]. For each case, we based the most likely diagnosis on the higher agreement among neuropsychology and available in vivo biomarkers (CSF AβR, CSF p-Tau, CSF t-Tau, Amy-PET, FDG-PET).
Imaging readers and laboratory staff were not blinded to neuropsychological data, whereas the blindness about the results of biomarkers different from those directly tested, was observed. In detail, all included participants were symptomatic and they had performed a standardized neuropsychological battery [33–41] in order to diagnose MCI or dementia. The majority of participants (69%) had also performed one or more specific test batteries to investigate language deficits; however, due to the variability of the tests used for this scope [37, 42–46], language performances were not directly comparable. A conventional CT/MRI scan had been performed in order to rule out secondary causes of cognitive decline (e.g., normal pressure hydrocephalus, subdural hematoma, or brain tumor). FDG-PET scan and Amy-PET scan had been carried out following the national and international guidelines and Manufacturers’ specifications of each radiopharmaceutical. According to guidelines [47], FDG-PET had been performed first in the diagnostic-work-up and a qualitative description of the metabolic pattern was provided by the readers. Then Amy-PET had been carried out to confirm/rule out AD in patients with dementia and to clarify whether MCI was due to AD pathology. Amy-PET had been performed with any of the fluorine18-labeled tracers commercially available (Florbetaben (FBB)-Bayer-Piramal, Florbetapir (FBP)-Ely-Lilly, Flutemetamol (FMM)-General Electric) and a binary positive/negative output was provided by two trained and certified readers in a consensus reading based on visual assessment. For the interpretation, rules provided by each manufacturer were observed.
Finally, due to the ability of FDG-PET in discriminating among dementia subtypes [48, 49], in cases of an Aβ IBI, FDG-PET was also evaluated with two different automated classifiers provided by the neuGRID web-portal (http://www.neugrid2.eu): the Meta-analytically derived Regions Of Interest (metaROI) and the Hypometabolic Convergence Index (HCI) [50–52].
Laboratory procedures
The ApoE genotype has been determined using standardized procedures and in cases of young-onset of cognitive symptoms or positive family history for dementia, genetic analysis for causative mutations has been also performed.
CSF samples had been stored at –80°C until the moment of the analysis that was performed with the automated Fujirebio Lumipulse system [53]. The cut-off values for CSF Aβ42, CSF AβR, CSF p-Tau, and CSF t-Tau were pre-determined following Fujirebio guidelines for the chemiluminescent enzyme immunoassay (CLEIA) Lumipulse method (Diagnostic sensitivity and specificity using clinical diagnosis and follow-up as golden standard. December 10, 2018) and were selected based on the Youden index method. Cut-offs indicative of AD pathology were for CSF Aβ42 < 874 pg/ml, for CSF p-Tau > 56.5 pg/ml, for CSF t-Tau > 404 pg/ml, and for CSF AβR < 0.1.
Statistical analysis and preliminary definitions
Statistical analysis was performed using MedCalc Statistical Software version 14.8.1 (MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org; 2014). First, we verified whether the agreement between CSF Aβ markers and Amy-PET results significantly differs utilizing CSF Aβ42 or CSF AβR as the reference CSF Aβ marker (McNemar’s test; the significant level was set at p < 0.05). Then we verified which of these two tests better agrees with Amy-PET results (unweighted Cohen’s K coefficient; K values less than 0.40 were indicative of low agreement, values between 0.41 and 0.60 were indicative of moderate agreement). We planned these two steps in sequence in order to estimate the number and type of discordant cases detectable with each CSF Aβ marker. On the basis of these first results, in the following only CSF AβR was used to classify each case as “concordant” or “discordant” referring to the absence/presence of an Aβ IBI. (A complementary analysis was conducted also basing the concordance definition on the agreement between CSF Aβ42 and Amy-PET results, data shown in the Supplementary Material). A participant was defined as “concordant” when both CSF AβR and Amy-PET were indicative of Aβ pathology or when both CSF AβR and Amy-PET excluded Aβ pathology; a participant was defined as “discordant” in case of disagreement between CSF AβR and Amy-PET in detecting the presence of Aβ pathology. Then, each case was assigned to one of the following four categories: 1) category with CSF AβR<0.1 and positive Amy-PET (CSFAβR+/Amy-PET+), also defined concordant+, that is inclusive of cases probably affected by AD dementia or MCI due to AD; 2) category with CSF AβR≥0.1 and negative Amy-PET (CSFAβR–/Amy-PET–), also defined concordant-, that is inclusive of cases probably unaffected by AD dementia or MCI due to AD; 3) category with CSF AβR < 0.1 and negative Amy-PET (CSFAβR+/Amy-PET–), that is inclusive of discordant cases possibly affected by AD dementia or MCI due to AD; and 4) category with CSF AβR≥0.1 and positive Amy-PET (CSFAβR–/Amy-PET+), inclusive of discordant cases possibly affected by AD or MCI due to AD. Then, in order to verify differences in demographic, clinical, and neuropsychological data and biomarker profiles, we compared cases of different categories, when numerically possible, with a statistical approach. Regarding discordant cases, due to the limited number in the CSFAβR–/Amy-PET+ group, only for CSFAβR+/Amy-PET– group was possible a statistical approach and it was compared with both concordant groups. Continuous variables were compared using a multiple comparisons test (Kruskal-Wallis) for independent samples and, whether statistically significant differences were detected, a test for pairwise comparisons of subgroups according to Conover was performed. Categorical variables were compared using Fisher’s test. According to Bonferroni correction, the significance level was set at p < 0.01. We used a non-parametric correlation test (Spearman’s Rank Correlation Coefficient) to assess the correlation between CSF Aβ markers and age and between CSF Aβ markers and ApoE genotype. For the study purpose, we defined a case to be in the “AD continuum” [5] in the presence of at least 1 positive Aβ marker (CSF AβR or Amy-PET) and when AD was a possible diagnosis; as such, to be in the “AD continuum” was not synonym of to be affected by AD pathology. Moreover, we defined an Amy-PET result as “false negative” when the scan was interpreted as negative by the two certified readers in the presence of other biomarkers all indicative of AD pathology (CSF AβR, CSF p-Tau, CSF t-Tau, FDG-PET). For all discordant cases, an AD pathology was initially hypothesized and each case was separately interpreted considering the possible impact of age and ApoE polymorphism on biomarker results. When the main suspected pathology was AD, but only the presence of neurodegeneration was in vivo confirmed, participants were classified as affected by suspected non-Alzheimer’s pathology (SNAP) [54]. In cases of all biomarkers within the normal range, participants were classified as affected by a non-neurodegenerative disease (NND).
RESULTS
Description of participants
As reported in Table 1, 39 cases are included in the study: 13 are affected by MCI (mean MMSE score 25.2±2.4) and 26 are affected by mild to moderate dementia (mean MMSE score 18.4±3.8). “Language presentation” is fairly represented (44%). Sixty-two percent of cases are females, 26% are at least 1 ApoE ɛ4 carriers. Genetic analysis revealed the presence of a missense variant Pro321Arg in PSEN2 gene in a patient with young-onset AD belonging to the category concordant+. The mean age is 62.8±7.2 and the young-onset of symptoms is frequent (62%). All participants are aged less than 80. The mean education is 11.7±6 years, the mean MMSE score for the total sample is 20.7±4.7. Sixteen cases had performed Amy-PET with the FBB, 8 with the FBP and 15 with the FMM. The mean time interval between CSF collection and Amy-PET execution is 9±13 months and CSF generally had been performed first (74%).
Characteristics of the total sample. n, number; MMSE, Mini-Mental State Examination; MCI, mild cognitive impairment; M, mean; SD, standard deviation; y, years; m, months; Time between exams, time interval between CSF collection and Amy-PET execution; FBB, Florbetaben; FBP, Florbetapir; FMM, Flutemetamol
CSF Aβ markers and Amy-PET agreement
McNemar’s test shows that the agreement between CSF Aβ markers and Amy-PET results does not significantly differ utilizing CSF Aβ42 or CSF AβR. Anyway, differences in the classification regard 6 cases that are classified as CSF Aβ positive using the CSF AβR (negative using the CSF β42), and 1 case in the opposite direction. The characteristics of discordant cases and the level of agreement between CSF Aβ markers and Amy-PET results are shown in Table 2. When the CSF Aβ42 marker is applied, the level of agreement with Amy-PET is weak (Cohen’s K 0.05) and the number of discordant cases is high: 13/39 (33%). In detail: 9 cases are CSFAβ42+/Amy-PET–, whereas 4 cases are CSFAβ42–/Amy-PET+. The level of agreement between CSF Aβ markers and Amy-PET improves from low to moderate (Cohen’s K 0.431) using CSF AβR as the reference CSF Aβ marker. Indeed, only 8 (21%) cases are confirmed as discordant by the AβR: 6 are CSFAβR+/Amy-PET–, whereas 2 are CSFAβR–/Amy-PET+. As reported in Table 3, each category of cases is evaluated in relation to the “AD continuum”: 34 out of 39 cases are within the “AD continuum”: 26 CSFAβR+/Amy-PET+ are probably affected by AD dementia/MCI due to AD, 6 CSFAβR+/Amy-PET– and 2 CSFAβR–/Amy-PET+ are possibly affected by AD dementia/MCI due to AD. On the basis of their biomarker profiles (CSFAβR–/Amy-PET–), 5 out of 39 cases are outside the “AD continuum” and are considered affected by different diseases (FTD n = 3, SNAP n = 1, NND n = 1).
The level of agreement between CSF and PET Aβ markers in 39 cases
Categorical variables of the 4 groups: CSFAβR+/Amy-PET+, CSFAβR–/Amy-PET–, CSFAβR+/Amy-PET–, and CSFAβR–/Amy-PET+. Fisher’s test was conducted for pairwise comparisons involving CSFAβR+/Amy-PET– group and both concordant groups; Bonferroni correction was applied. The significance level was set at p < 0.01. n, number; g, groups; p, presentation; n.p., not performed; FBB, Florbetaben; FBP, Florbetapir; FMM, Flutemetamol; n.s., not significant
Comparisons among groups
As previously specified, since the low number of cases (n = 2), the CSFAβR–/Amy-PET+ group was excluded a priori from the analysis, and the largest homogeneous group of discordant cases (CSFAβR+/Amy-PET–, n = 6) was compared with both concordant groups (CSFAβR+/Amy-PET+, n = 26, and CSFAβR–/Amy-PET–, n = 5). The comparison among groups does not show any significant difference in categorical variables as ApoE genotype and gender distribution, frequency of language presentation. A “young-onset” of symptoms is prevalent in the positive and negative concordant groups (69% and 80%, respectively) whereas dementia is highly represented in both concordant+ and CSFAβR+/Amy-PET– groups (69% and 83%, respectively); anyway, also these results are not statistically significant when compared to the remaining group. The percentage of young-onset participants is significantly different between concordant and discordant groups when all kind of concordant and discordant cases are merged together between them (CSFAβR+/Amy-PET+ with CSFAβR–/Amy-PET– and CSFAβR+/Amy-PET– with CSFAβR–/Amy-PET+) (71% and 25%, respectively, p = 0.04); 92% of young-onset participants belong to the merged concordant group.
The use of the three Amy-PET tracers is evenly distributed in all groups (Table 3). Regarding continuous variables (Table 4), age at symptoms onset is higher in the CSFAβR+/Amy-PET– group (72.2±5.5) compared to the CSFAβR+/Amy-PET+ (61.3±6.0) and CSFAβR–/Amy-PET– (59.2±7.9) group (p < 0.01). Again, age at Amy-PET execution is higher in the CSFAβR+/Amy-PET– group (74.7±5.3) compared to the CSFAβR+/Amy-PET+ group (64.3±7.0) and the CSFAβR–/Amy-PET– (63.8±8.8) group, but this result is not statistically significant after Bonferroni correction.
Continuous variables of the 4 groups: CSFAβR+/Amy-PET+, CSFAβR–/Amy-PET–, CSFAβR+/Amy-PET–, and CSFAβR–/Amy-PET+. All values reported as M±SD. The comparison among the first 3 groups was performed using the Kruskal-Wallis test and pairwise comparisons according to Conover; Bonferroni correction was applied. The significance level was set at p < 0.01. Neuropsychological tests corrected for age and education (only for the MMSE score raw data). n, number; g, groups; y, years; m, months; Time between exams, time interval between CSF collection and Amy-PET execution; RAVL-IR, Rey Auditory Verbal Learning Test-Immediate Recall; RAVL-DR, Rey Auditory Verbal Learning Test-Delayed Recall; FABit, Frontal Assessment Battery; CSF AβR, CSF Aβ42/40
The comparison among the three groups does not show any difference in years of education, in disease duration, in the main neuropsychological test results (mean MMSE score ranges from 19.7 to 23.4). The mean interval between CSF collection and Amy-PET execution is not significantly different even if wide (9±13 months for the total sample). All CSF markers are indicative of AD pathology in both CSFAβR+/Amy-PET+ and CSFAβR+/Amy-PET– groups and all CSF markers, except Aβ40 and Aβ42, are significantly different compared to the CSFAβR–/Amy-PET– group (p < 0.01).
A negative non-significant correlation between CSF Aβ markers and age, and between CSF Aβ markers and ApoE ɛ4 are found in the total sample.
The suspected underlying pathology of discordant cases detected using in vivo biomarkers
In the absence of a pathological confirmation, we tried to define the underlying pathology of discordant cases using in vivo biomarkers. To this aim, in all 8 discordant cases, FDG-PET was revised visually and with two different automated classifiers: both classifiers (metaROI and HCI) gives in all cases the same result. We reported separately data for each discordant case (Table 5). For case A, only the CSF Aβ markers are indicative of AD pathology, whereas Amy-PET, FDG-PET, and the other CSF marker are normal. Then, in this case, the underlying pathology is probably different from AD and CSF AβR is interpreted as a false positive result. For cases B, C, D, E, and F, despite a negative Amy-PET, both visual and automated assessment of FDG-PET together with all CSF markers (Aβ1–42, AβR, p-Tau, t-Tau) are suggestive of AD (imaging of case F is reported in Fig. 1). All these 5 cases, except case E, are ApoE ɛ4 non-carriers. The underlying pathology of case G and H remains undefined: in both cases, despite a positive Amy-PET, the majority of CSF markers and FDG-PET are not unequivocally indicative of AD; both cases are aged less than 75 and ApoE ɛ3/ɛ3 carriers; in this situation, a false positive Amy-PET result is less probable [47, 55]. Thus, even if only one biomarker (Amy-PET) is indicative of AD pathology, still AD may be a possible diagnosis for cases G and H. Additional considerations are necessary for discordant cases D, E, and H that show a neuropsychological profile compatible with the semantic variant of primary progressive aphasia (PPA) for whom a “mixed AD+FTD pathology” can be supposed.
Neuropsychology and biomarkers in discordant cases: case A, B, C, D, E, and F belong to CSF AβR+/Amy-PET– group; case G and H belong to CSF AβR–/Amy-PET+ group. In bold, results that suggest AD pathology. age, age at onset; ApoE, ApoE genotype; MMSE, Mini-Mental State Examination; NPSY, neuropsychology; Time between exams_months, time interval between CSF collection and Amy-PET execution; md, multiple domains; AD, Alzheimer’s disease; Logopenic v, Logopenic variant; bvFTD, behavioral variant of Frontotemporal Dementia; SDv-FTD, Semantic variant of Frontotemporal Dementia; FBB, Florbetaben; FBP, Florbetapir; FMM, Flutemetamol; AβR, Aβ42/40; co, cut-offs for AD; V, visual assessment; A, automated assessment (metaROI and HCI); n.p., not pathological
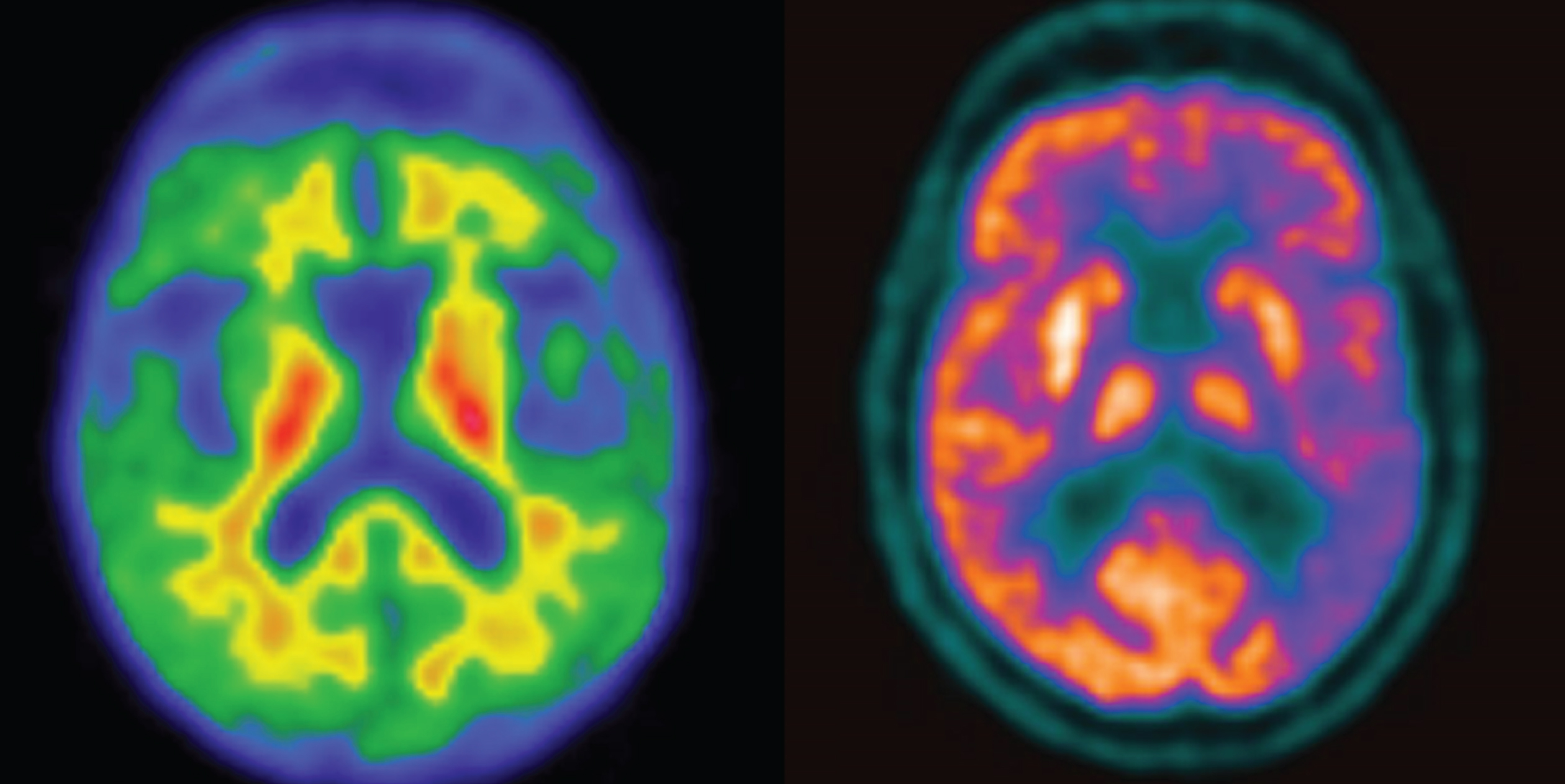
Transaxial sections of FBB negative Amy-PET represented on a color scale on the left side (no tracer uptake in cortical regions) and FDG-PET on the right side (severe left hemispheric hypometabolism mostly in the parieto-temporal regions). Imaging belongs to case F (CSF AβR+/Amy-PET– discordant case).
DISCUSSION
The in vivo differential diagnosis of dementia is one of the main challenges in the research field and clinical practice. For this reason, the development and use of biomarkers has become a main issue. The final scope of this study was to improve the diagnostic work-up in dementia, especially in cases of discordant results between CSF Aβ markers and Amy-PET. For this purpose, in the absence of a pathology confirmation of the underlying disease, for each case, we based the most likely diagnosis on the higher agreement among neuropsychology and available in vivo biomarkers (CSF AβR, CSF p-Tau, CSF t-Tau, FDG-PET, Amy-PET) of the present series.
Anyway, despite a wide availability of in vivo biomarkers, the underlying pathology can remain undefined in clinical practice.
Main findings and comments
The main characteristics of this series are a young age of participants and a high prevalence of language disturbances. Probably the first result is a consequence of that often younger cases affected by cognitive decline are more widely investigated than the older ones. The second consideration depends on the fact that cases affected by language disturbances can share similar symptoms and the clinical presentation may be an expression of different underlying pathologies [56]. For this reason, in case of language presentation, clinicians more often require biomarkers to support the diagnosis.
In our cohort, McNemar’s test shows that the agreement between CSF Aβ markers and Amy-PET results does not significantly differ utilizing CSF Aβ42 or CSF AβR; however, the use of CSF AβR is associated with a reduction of discordant cases from 13 to 8. CSF AβR allows to increase the agreement with Amy-PET from a low to a moderate level. Therefore, CSF AβR was chosen as the CSF Aβ marker of reference to establish Aβ concordance/discordance of each case. Probably the better level of agreement between CSF AβR and Amy-PET depends on the fact that AβR “normalizes” the CSF Aβ42 levels for the total CSF Aβ concentration mostly represented by the isoform Aβ40 [7]. For this reason, and considering that the presence of white matter lesions affects the levels of CSF Aβ42 but not those of CSF AβR [57], CSF AβR should be used to improve the percentage of appropriated diagnoses [7]. In consequence, we guess that the results of our study using CSF AβR in comparison with Amy-PET may be the most realistic and numerically optimized estimate of the agreement between CSF and PET Aβ markers. It is worth noting that in our series, the use of CSF AβR allows the reduction of both the number of cases falsely classified as normal and those falsely classified as pathological by the CSF β42 level. This is in line with results obtained by Janelidze and colleagues [13], while other authors reported an improvement in the classification performance only for cases that are classified falsely as normal by CSF β42 level [58]. In consequence of these two initial results, we guess that for the AD diagnosis there might be questionable an interchangeable use of CSF and PET Aβ markers, as well as an interchangeable use of the two CSF Aβ markers. We also highlight the importance that despite the use of CSF AβR to minimize the number of discordant cases, controversy still exists between CSF Aβ and Amy-PET results and at present, there is an unmet need for suggestions to manage Aβ IBIs. The number of discordances in the present series is higher of that found by other authors both with CSFAβ42 (33% versus 10–20%) [6, 7] or with CSFAβR (21% versus 16%) [19]. A possible explanation is a difference in the design of the studies. Indeed, several previous studies have been conducted using cut-offs specifically determined to optimize agreement between CSF and PET Aβ markers. Differently, in our study, we utilized external pre-determined cut-offs using clinical diagnosis and follow-up as golden standard. In this regard, applying the clinical diagnosis as golden standard, similar discordance values between CSFAβ42 and Amy-PET results (32.5%), have been reported by Weise et al. [59], using ELISA test.
Moreover, the estimation of Aβ IBIs in different studies may be affected by several factors as the use of different amyloid PET tracers, the use of different methods to interpret Amy-PET results (visual versus semiquantitative reading), the lack of a common standardized method to analyze CSF markers, the unavailability of universally pre-specified CSF Aβ marker cut-offs and the inclusion of cases with a different level of cognitive decline.
The comparison among concordant groups (CSFAβR+/Amy-PET+ and CSFAβR–/Amy-PET–) and the CSFAβR+/Amy-PET– discordant group does not show any difference in clinical, neuropsychological data except for age which is higher in CSFAβR+/Amy-PET–. Thus in the present series, the single factor that seems to influence the discordance of CSFAβR+/Amy-PET– cases is age. It is well known that, in normal aging, amyloid positivity increases both with age and according to ApoE ɛ4 genotype [60–62]. In this regard, a meta-analysis conducted by Ossenkoppele and colleagues revealed that also in non-AD dementias Amy-PET positivity increases with both age and ApoE ɛ4 genotype. Conversely, in symptomatic AD, the prevalence of Amy-PET positivity decreases from age 50 to 90 years in ApoE ɛ4 non-carriers (86% ⟶68%) and to a lesser degree in ApoE ɛ4 carriers (97% ⟶90%) [55]. Unfortunately, these PET findings have not been either compared to CSF biomarkers or confirmed by pathology. Thus, it is impossible to state whether in that series the negative Amy-PET scans in AD can be attributed to a clinical misclassification or to an actual false negative PET finding. In our cohort, possibly due to the limited number of cases, no significant correlation between CSF Aβ markers and age and between CSF Aβ markers and ApoE ɛ4 genotype are detectable. Our cohort is overall characterized by a lower prevalence of ApoE ɛ4 genotype compared to that usually detected in AD (26% versus 40%) [63] and this proportion is preserved also in the group of discordant cases (2/8 = 25%). As reported in Table 5, CSFAβR+/Amy-PET– cases are 6 in number: 1 is affected by MCI (case A) and 5 are affected by dementia (cases B, C, D, E, F). These 5 cases, characterized by a negative Amy-PET, show the classic CSF AD-like pattern, and 4 out of 5 are ApoE ɛ4 non-carriers. In this regard, data from recently completed clinical trials for AD documented from 36 to 42% of Amy-PET negativity in clinically probable AD ApoE ɛ4 non-carriers [64, 65]. However, even if also CSF is known to be very strongly related to ApoE genotype [8, 66], CSF markers are abnormal in the same group. It is not clear how ApoE genotype could affect only Amy-PET results interpretation instead of also CSF Aβ marker levels interpretation. In this regard, results from a previous study on the quantitative association between CSF and PET Aβ markers, showed a lower amyloid PET uptake for the same CSF Aβ42 levels in ApoE ɛ4 non-carriers, highlighting that ApoE does not necessarily influence one or the others Aβ markers, but instead it may influence their relationship [12]. No difference in clinical disease duration is present among groups. This information, altogether with high CSF t-Tau values and pathological MMSE scores, confirms that the CSFAβR+/Amy-PET– cases of our series are not at an initial stage of the disease that could have justified a negative Amy-PET result [8, 10].
Indeed, we believe that in our series, the cause of discordance in the CSFAβR+/Amy-PET– group cannot be explained with the assumption that CSF “changes” before Amy-PET, as conversely demonstrated by other authors in cognitively unimpaired-MCI cases [8, 10]. Thus, our results support the possibility that a negative Amy-PET, in and of itself, cannot always rule out the presence of Aβ pathology in the brain possibly as a consequence of some characteristics of the Aβ plaques (see below).
We tried to define in vivo the underlying pathology of discordant cases (8/39). We reported separately data of each discordant case (Table 5) and we evaluated the possible impact of age and ApoE at an individual level. In summary, 34 out of 39 participants, having positive at least one Aβ marker, are within the “AD continuum”: 26 CSFAβR+/Amy-PET+, 6 CSFAβR+/Amy-PET–, 2 CSFAβR–/Amy-PET+. In consideration of all the other available data, the main conclusion is that in 5 (case B, C, D, E, F of Table 5) out of the 34 cases (15%) Amy-PET provides probably false negative results; in one case, probably CSF AβR provides a false positive result (case A). As shown in Table 5, all other CSF biomarkers beyond AβR, i.e., p-Tau, t-Tau, and FDG-PET may contribute in defining in vivo the underlying pathology for cases B, C, D, E, and F, highlighting the advantage of using CSF analysis as it allows the simultaneously capture of the two degenerative processes specific for AD pathology (“A” and “T”) and neurodegeneration (“N”). In this regard, as reported in a consensus paper from the Alzheimer’s Biomarkers Standardization Initiative [67] and in one more recent consensus of the Task Force on Biological Markers in Psychiatry of the World Federation of Societies of Biological Psychiatry [68], if all classical AD CSF biomarkers are abnormal, the overall result should be interpreted as “neurochemically probable AD”. Moreover, FDG-PET, providing a well recognizable and specific AD-like pattern in these cases (B, C, D, E, F,) helps in the differential diagnosis, as expected [49]. Conversely, the underlying pathology of cases G and H remains undefined, probably due to the fact that CSF markers are negative and cannot be used to confirm another type of dementia [69]; additionally, in these cases, FDG-PET does not provide a well recognizable metabolic pattern of a specific disease.
Summing up in our cohort the use of multiple AD biomarkers seems to advantage in particular the diagnosis in the CSFAβR+/Amy-PET– compared to the CSFAβR–/Amy-PET+ discordant cases.
Overall, this data suggests the possibility of Amy-PET failures (15%) in detecting in vivo Aβ pathology in symptomatic sporadic AD cases, as it has been already shown, independently from age, in familial AD [70] and in sporadic AD autopsy confirmed aged patients [71, 72]. In this regard, a relevant finding that is worth noting, even if relative to a mutated population, is that Amy-PET was negative in all the cases of familial AD with the Arctic mutation [73]. The 15% of failures in detecting Aβ pathology might be due to biochemical reasons and linked to the conformation that Aβ can assume in the brain. As it is well known, Aβ pathology is characterized by the formation of deposits including diffuse and cored plaques; diffuse deposits are immature precursors of the cored plaques associated with AD [74]. Results from an autopsy-confirmed study showed that in AD brain tissue sections, 6-CN-PiB (highly fluorescent Pittsburgh compound B derivative) labeling was most robust in compact/cored plaques than in diffuse plaques [75]. Structural variations in Aβ fibrils have been widely described [76–78] and some authors affirm that different conformations of Aβ deposits in both familial and sporadic AD cases may affect the binding of Amy-PET tracers [4, 80]. Age and the percentage of AβR could also influence Amy-PET tracer uptake modifying the deposits and inducing conformational changes in Aβ plaques [74, 81]. Additionally, it is possible that some particular conformations of Aβ are partially resistant to the pyro-glutamation process needed to allow 6-CN-PIB (and probably also other tracers of the same class) binding [82, 83]. Hence, in our study, the disagreement between positive CSF Aβ and negative Amy-PET in symptomatic aged AD patients could be due to the variability in plaques conformation such as lower “fibrillarity” compared to standard AD plaques, corroborating the existence of different molecular AD subtypes.
Separate considerations deserve the discordant cases affected by the semantic variant of PPA (3 out of 8 cases in Table 5). Basing on the literature data [56] for these cases, a mixed pathology has been suspected (FTD+AD); in any case, we guess that this condition cannot explain the Aβ IBIs. Indeed, in mixed pathology (AD + Vascular Dementia and AD + Lewy Body Dementia) Amy-PET is expected to be positive [47], as well as in FTD when AD is the concomitant pathology [28, 84].
Moreover, we evaluated the time interval between exams as a possible cause of discordance: the overall time interval between CSF collection and Amy-PET execution is wide (9±13 months) but it shrinks to nearly coincide (3.5±3.4 months) in the CSFAβR+/Amy-PET– discordant group. Therefore, except for case G (time interval 24 months, Table 5), we guess that the Aβ marker discordances can hardly be thought to be dependent on that.
Finally, we also considered whether it was possible that brain morphological changes, atrophy in particular, might have determined discordances. Indeed, cortical atrophy can affect the visual differentiation between gray matter and white matter tracer retention, and generally, atrophy has been associated with false positive Amy-PET interpretation; anyway, a severe atrophy has been also associated with false negative Amy-PET interpretation [28].
Strengths, clinical implication, and possible application
According to recent recommendations [7], all participants of this series had performed an extensive diagnostic work-up comprehensive also of CSF AβR; moreover, CSF analysis was made utilizing the new validated automatic Lumipulse method that should be preferred to the manual method, in order to reduce inter- and intra-laboratory variability [85].
Regarding the level of agreement between Aβ markers, our results suggest the opportunity to apply a different diagnostic work-up in AD according to patient age: for cases with a young-onset of symptoms (age < 65), CSF AβR and Amy-PET seems to be nearly equally capable in detecting/excluding Aβ pathology (92% of young-onset cases are concordant in our study). Conversely in aging, both Amy-PET and CSF analysis are characterized by an increase in false positive results [60–62]. Moreover, since CSF analysis shows a high negative predictive value [67, 86], whereas, according to our and other findings [55], the number of false negative Amy-PET results seems to grow in AD dementia aged patients, CSF analysis might be preferable in aged AD suspected cases.
Limitations
A major limitation of our study, common to several previous clinical studies, is the lack of pathological confirmation of diagnoses; for this reason, the study was not designed as a test accuracy study. Moreover, even if the performances of the three fluorinated tracers are comparable [87], the use of various Amy-PET tracers might have influenced Amy-PET results [79].
It is possible that a quantitative approach to Amy-PET might in the future change the performance of this diagnostic technique. In our experience, this approach was not performed both for a lack of certified methods of quantification and for the use that we have done of various amyloid PET tracers.
Finally, our cohort is small and inclusive of cases with a widely different level of cognitive decline. Probably the sample size depends on the fact that Amy-PET is considered an alternative test to CSF analysis and not many cases usually perform both tests, and even fewer cases performed addition neuropsychological tests, ApoE genotype determination, FDG-PET that were, all together, conditions necessary for the inclusion in the study. Moreover, due to the retrospective design of the study, the fractional value of any class may be biased by several factors, as purely random events (e.g., CSF quantity left) or by difficult diagnoses and therefore worthy of the more extensive diagnostic effort. Anyway, thanks to the health care organization in Italy, different healthcare insurance or socioeconomic status did not influence the decision to request exams by clinicians.
Conclusion
1) Amyloid biomarker incongruences are the main challenge to overcome in order to improve in vivo AD diagnosis: our results suggest that an interchangeable use of CSF and PET Aβ markers in the AD diagnostic work-up may be questionable and support the implementation of CSF AβR in clinical practice; 2) the use of FDG-PET together with CSF p-Tau and t-Tau in symptomatic discordant CSFAβR+/Amy-PET– cases can support AD diagnosis; 3) finally, our findings, together with other reports, suggest that the variability in plaques conformation could affect the capability of Amy-PET in detecting Aβ pathology, challenging the concept that a negative Amy-PET scan always rules out AD, and supporting a comprehensive diagnostic work-up.
Further studies are needed to establish the capability and the limits of different tracers in detecting Aβ pathology in the brain. We recommend verification and replication of our findings in larger studies, with a prospective design, involving also participants at an earlier and more homogeneous stage of disease.