
Abstract
Background:
Previous studies have shown an association between disruption of the blood-brain-barrier (BBB) and dementias of different etiologies. The protein concentration of cerebrospinal fluid (CSF) can be used as an indirect measurement for the permeability of the BBB using the CSF/plasma albumin quotient (Q-Alb) or total CSF protein.
Objective:
In the current study, we wanted to investigate Q-Alb and CSF protein concentration in dementias of different etiologies and the possible confounding factors.
Methods:
A total of 510 patients and healthy controls were included in the current study. The patients were diagnosed with Alzheimer’s disease (AD), dementia with Lewy bodies (DLB), vascular dementia (VaD), or frontotemporal dementia (FTD).
Results:
We found that Q-Alb was significantly different between the groups (p = 0.002, F = 3.874). Patients with DLB and VaD showed the largest Q-Alb. Although not significant for CSF total protein, we found the same overall pattern for DLB and VaD. When examining confounding factors, we found a positive association with age and a lower Fazekas score in DLB as compared to VaD.
Conclusion:
These results suggest that Q-Alb can contribute to our understanding of the pathophysiological mechanisms in DLB, and Q-Alb may serve as a supplementary diagnostic marker. Furthermore, we found a positive association with age, which may be due to differences in vascular co-morbidities. In addition, in patients with DLB, the increased Q-Alb is not due to vascular lesions. Studies are needed to validate the possible diagnostic value of Q-Alb in a larger cohort.
Keywords
INTRODUCTION
Studies have reported that there is a connection between disruption of the blood-brain-barrier (BBB) and dementia due to different etiologies [1, 2]. The BBB is a diffusion barrier composed of continuous non-fenestrated vessels and sealed cell-to-cell contacts within the central nervous system (CNS). The BBB is essential for normal neuronal function and regulates the homeostasis of the CNS by for example protecting the CNS from toxins, pathogens, and inflammation [3]. Consequently, an increased permeability of the BBB may thereby lead to pathological changes seen in neurodegenerative diseases and furthermore reflect the vascular pathology in dementia [4].
The quantification of the cerebrospinal fluid (CSF) protein concentration can be used as an indirect measurement for the permeability of the BBB since proteins pass the barrier at different rates, depending on, for example, the hydrodynamic radii of the protein [5]. An analysis of CSF/plasma albumin quotient (Q-Alb) serves as a standard measurement and is an ideal parameter for the permeability of the BBB since the CSF’s total protein concentration depends on a plethora of different variables. Albumin is exclusively synthesized in the liver, and consequently the albumin in the CSF originates from the blood and is only transported to the CNS through passive diffusion [6]. For that reason, abnormal elevations of Q-Alb can function as an indirect measurement for an increased permeability of the BBB, and has previously been investigated in multiple neurological diseases including multiple sclerosis [7] and stroke [8].
The role of Q-Alb as a diagnostic marker in dementia is not well understood. However, in patients with dementia with Lewy bodies (DLB) and vascular dementia (VaD), studies have found an increased Q-Alb [2, 10]. In patients with Alzheimer’s disease (AD), the results have been more varied [10–13], and a recent meta-analysis showed that Q-Alb was not a suitable biomarker for AD [11]. Furthermore, Q-Alb has previously been shown to be affected by age and may therefore be a confounding factor when differentiating between AD and younger healthy controls. Furthermore, vascular pathology, body mass index (BMI), and co-existing degenerative spine disorders have been shown to influence Q-Alb [14], which may explain the increased Q-Alb and CSF protein in DLB and VaD.
In order to investigate the potential role of Q-Alb and CSF total protein concentration as biomarkers for BBB integrity in dementias of different etiologies, the present study analyzed concentrations of Q-Alb and CSF protein concentration in a broad spectrum of dementia diagnoses and healthy controls. Furthermore, we investigated the association between Q-Alb and age, as well as CSF protein and age in both healthy controls and patients with AD. Lastly, we examined the potential confounding effects of spine disorders, BMI, and vascular pathology in patients with DLB and VaD.
METHODS
Data for this study were retrieved from the Danish Dementia Biobank (approved by the Danish Data protection agency case no RH-30-0284/00622). Patients who underwent diagnostic evaluation for dementia at the Memory Clinic, Rigshospitalet, gave informed consent for their data and biological samples to be used for research purposes. This project was approved by the Danish Data Protection agency VD-2018-62/6279.
The Danish Dementia Biobank database contains results of routine blood and CSF analyses, and consensus diagnoses, which were reached at a multidisciplinary team consisting of neurologists and psychologists. All participants gave written informed consent to participate in the biobank. The database uses RedCap software (Vanderbilt University, Nashville, TN, USA) and is hosted on a secure server at the IT department of the Capital Region of Denmark.
Participants
The first source of data was the healthy controls (HC), which were recruited as a part of the DemProg cohort [15, 16]. The HC group was recruited through public advertisements. Inclusion criteria were: 1) age between 50–90 years, 2) Mini-Mental State Examination score≥26, 3) Addenbrooke’s Cognitive Examination≥85, 4) normal neurological and clinical examination, 5) normal or age-related brain atrophy measured on a computed tomography (CT) scan, 6) normal routine blood tests. Exclusion criteria were: 1) an inability to participate (including impaired vision or hearing), 2) cognitive symptoms including memory complaints, 3) signs of major neurological, psychiatric or other severe diseases, which potentially could elicit cognitive impairments, including signs of major depression or a geriatric depression scale score > 7, 4) pregnancy, 5) had undergone general anesthesia, 6) received electroconvulsive therapy in the past 3 months, 7) received sedatives, or 8) had any past or current addictions to alcohol or medications. Two participants from the DemProg cohort were excluded due to missing data.
The following groups were included from the Danish Dementia Biobank. The patients with AD fulfilled the NIA-AA criteria or the NINCDS-ADRDA criteria for AD [17, 18]. The patients with DLB fulfilled the criteria for DLB from the third report of the DLB consortium, the VaD fulfilled the criteria from International Society for Vascular Behavioral and Cognitive Disorders [19] or the NINDS-AIREN criteria [20], and the patients with FTD fulfilled the criteria for either behavioral variant [21, 22], semantic variant or non-fluent aphasia [22, 23]. The group of neurological controls (NC) were all referred to the memory clinic and were included in this study using the following criteria: 1) Did not meet the criteria for dementia or mild cognitive impairment as determined by cognitive screening tests, and 2) age between 40–90 years old. The NC were excluded if they had: 1) a history of major neurological or psychiatric disease, except for mild depression within a year before and two years after the final visit at the memory clinic, or 2) excessive alcohol intake or drug abuse within the previous 2 years at the time of diagnosis.
Measurements
All analyses were performed as part of the clinical routine diagnostic assessment of the patients between February 2008 and September 2017. All analyses were performed on Cobas 8000 (Roche diagnostics) instruments at the Department of Clinical Biochemistry at Rigshospitalet using commercial and validated kits. Plasma albumin levels were analyzed by absorption, and CSF albumin levels were analyzed by an immunoturbidimetric assay. CSF protein levels were quantified by turbidimetry. All patients were classified as having either a presence or an absence of a pathological Q-alb according to the clinical reference limits at Rigshospitalet, which are 13.9 for Q-alb and 0.5 g/L for CSF protein.
To assess the BMI, white matter hyperintensity, and whether patients suffered from spine disorder, we retrospectively collected information from patient files. To assess the amount of white matter hyperintensity, we used the Fazekas scale [24], which is a scale ranging from 0 (no white matter disease) to 3 (high white matter disease) with either CT or MRI. Due to the retrospective design of the study, we were only able to retrieve CT or MRI scans from 43 patients with VaD, but for all 28 patients with DLB. In eight of the patients with VaD the underlying etiology of dementia was large vessel disease, whereas the remaining 35 patients suffered from small vessel disease. We reported the Fazekas score from the patients with small vessel disease.
Statistics
All statistics were performed in MATLAB (vR2017b). To compare BMI, Fazekas score, gender, and age, we performed a one-way ANOVA. Since we found a significant difference for gender and age between the groups, and both gender and age has been shown to have an impact on Q-Alb and CSF protein [25], we performed an ANCOVA with age and gender as covariates when comparing all six groups. If we found a significant interaction, we performed post-hoc t-tests between the groups. The p-values from the post-hoc tests were corrected for multiple comparisons using the false discovery rate. When comparing the FTD subgroups, we performed a Kruskal-Wallis test due to the non-normal distribution.
To investigate a potential effect of age on both Q-Alb and CSF protein, we first compared the older and younger patients with AD using a t-test. This was done since the AD group was the largest (n = 289), and both Q-Alb and CSF protein were lower than in patients with DLB and VaD. Since both Q-Alb and CSF protein are affected by vascular load, we investigated the correlation between age and CSF protein, as well as age and Q-Alb using Spearman’s correlation in HC.
Furthermore, to investigate a potential correlation between Fazekas score and Q-Alb in DLB, we performed a Spearman’s correlation.
RESULTS
Demographics
For a full overview of the demographics, see Table 1. A significant difference was found for age and gender between the groups (p < 0.05), where the patients with AD, VaD, and DLB were significantly older than the HC, NC, and FTD. Furthermore, see Table 1 for the percentage of patients in each group classified as having a presence of an increased Q-alb or CSF protein.
Demographic characteristics of the study. Mean and standard deviation for age, CSF protein and Q-Alb along with the percentage of participants, who had high Q-Alb (>13.9) and CSF protein (>0.5), number of males/females and the number of participants who had values for Q-Alb
HC, Healthy controls from the DemProg cohort; NC, Participants who had been referred to the memory clinic for diagnostic assessment of cognitive symptoms but found to be cognitively intact; AD, Alzheimer’s disease; DLB, Dementia with Lewy bodies; VaD, Vascular dementia; FTD, Frontotemporal dementia.
CSF/plasma albumin quotient
We found a significant difference between the groups for Q-Alb when including age and gender as covariates (p = 0.002, F = 3.874; Fig. 1 and Table 1). For the post-hoc analysis after correction for multiple comparisons with the false discovery rate, we found that Q-Alb was significantly higher in both VaD and DLB as compared to NC, HC, and AD (Table 2). In addition, we found that VaD showed a significantly higher Q-Alb as compared to FTD. Furthermore, HC showed a significantly lower Q-Alb than all other groups. No significant differences were found between the FTD subgroups (p = 0.958). When investigating the difference in Q-Alb between older (mean (SD)=7.65 (3.88)) and younger (mean (SD)=6.68 (3.73)) patients with AD, we did not find a significant difference (p = 0.079, t = 1.763). No significant correlation was found between Q-Alb and age in HC and age (p = 0.250, ρ=0.203).
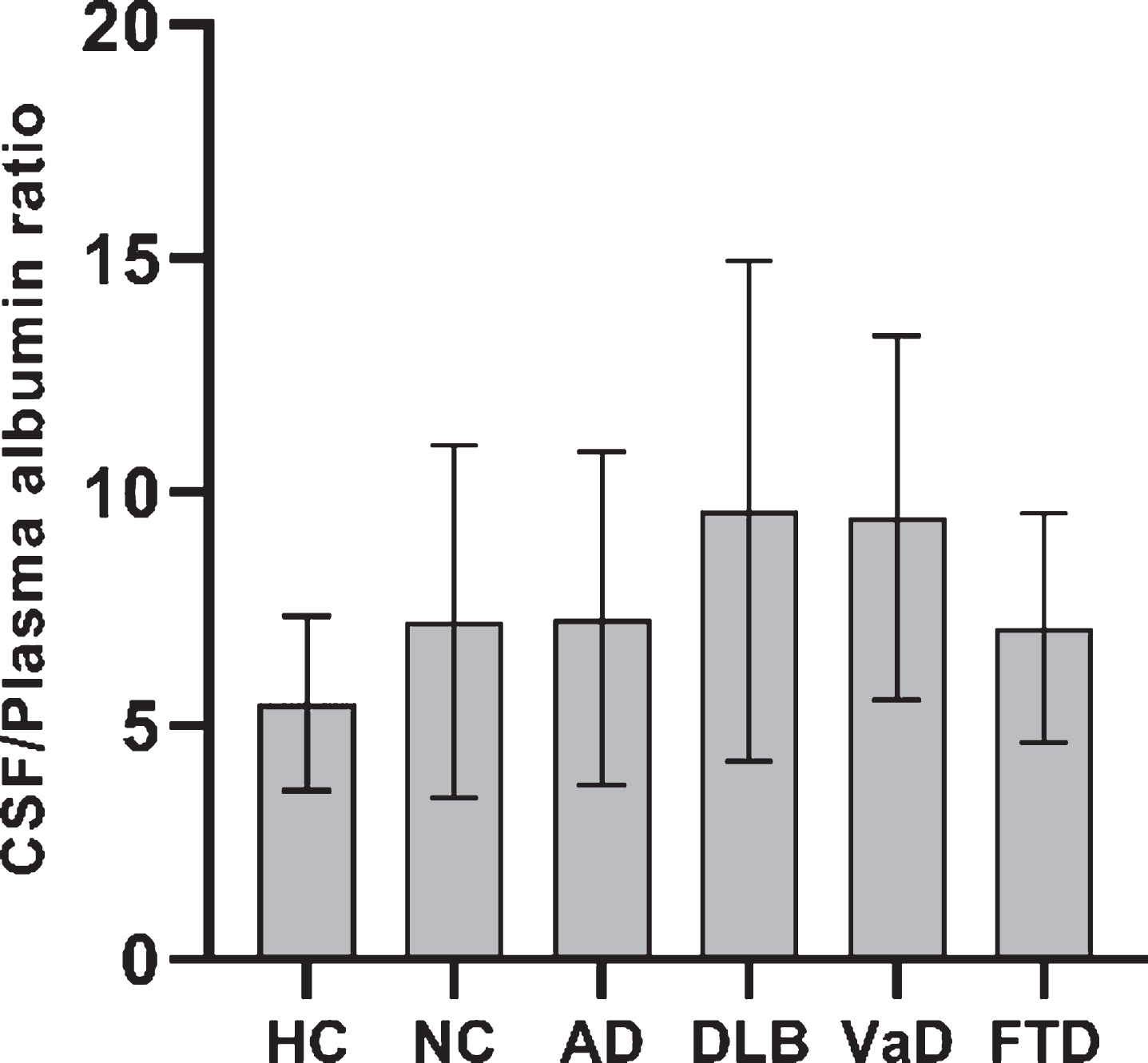
Mean and standard deviation of Q-Alb between the groups (HC, NC, AD, LBD, VaD, and FTD). The post-hoc t-test results can be found in Table 2.
P-value, t-value, and FDR corrected p-value for the post-hoc tests between groups for Q-Alb
FDR, False Discovery Rate; HC, Healthy controls from the DemProg cohort; NC, Participants who after diagnostic work-up did not suffer from a neurodegenerative disease; AD, Alzheimer’s disease; DLB, Dementia with Lewy bodies; VaD, Vascular dementia; FTD, Frontotemporal dementia; n.s., not significant.
CSF Protein
No significant differences were found for CSF protein between the groups (p = 0.245, F = 1.34; Fig. 2 and Table 1). We did not find any significant differences (p = 0.762) between the FTD subgroups. However, we found a significant difference between the older (mean protein (SD)=0.47 (0.19)) and younger patients (mean protein (SD)=0.40 (0.13)) with AD (p = 0.009, t = 2.636). When performing Spearman’s correlation between CSF protein in HC and age, we did not find a significant correlation (p = 0.082, ρ=0.298).
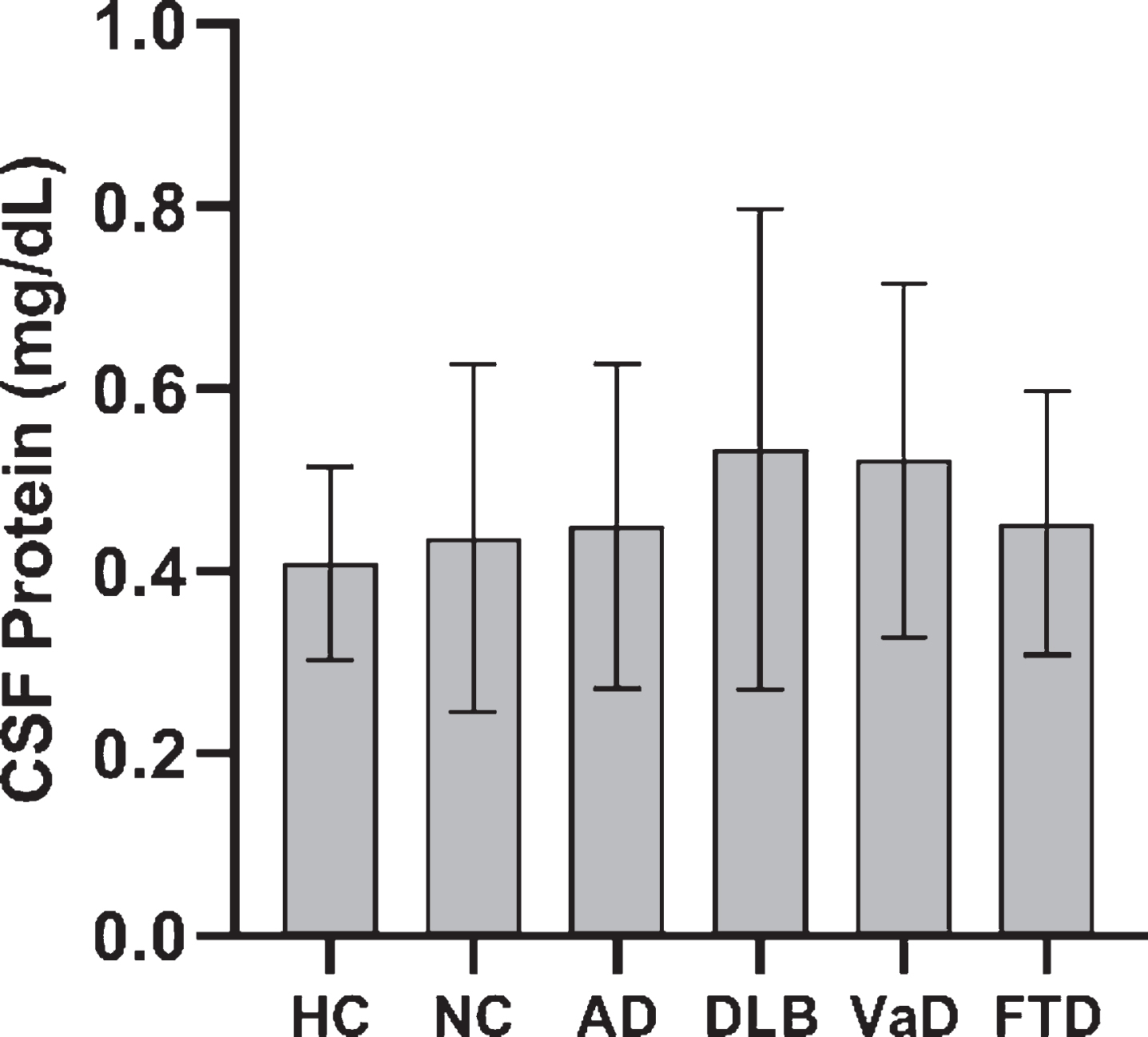
Mean and standard deviation of CSF protein between the groups (HC, NC, AD, DLB, VaD, and FTD).
Confounding factors
The main confounding factors for increased Q-Alb and CSF protein investigated in this study were vascular pathology, spine disorders, and obesity. As expected, we found that the Fazekas score was significantly higher in VaD (mean (SD)=2.86 (0.36)) as compared to DLB (mean (SD)=0.79 (0.92)) (p=<0.001, t = 12.280), and no correlation was found between Fazekas score and Q-Alb (ρ=0.226, p = 0.266) in patients with DLB. Due to the retrospective design, we were only able to retrieve BMI from 71.43% of patients with DLB and 61.70% of patients with VaD. We found that the BMI was not different between VaD (mean (SD)=23.83 (5.58)) and DLB (mean (SD)=24.46 (3.41)) (p = 0.657, t=–0.447) with two patients with DLB having a BMI between 30–35, while only one patient with vascular dementia had a BMI between 30–35. None of the patients with DLB and VaD had a BMI above 32.8. Four of the patients with VaD had a previous history of spine disorders, while none of the patients with DLB had any history of spine disorders.
DISCUSSION
In the current study, we found that Q-Alb was significantly higher in patients with DLB and VaD, compared to both HC, NC, and AD. Furthermore, we found that Q-Alb in patients with AD was significantly higher than in HC but not compared to NC. Although not significant for total protein, we found the same pattern of increased protein in CSF, especially for DLB and VaD. The percentage of high Q-Alb and CSF protein were also higher in both DLB and VaD. When examining the potential confounders, we found that younger patients (<65 years) with AD had lower Q-Alb and protein concentration than older patients with AD. In addition, a trend for increasing CSF protein in older age was found in HC. Furthermore, we found that the Fazekas score was significantly higher in patients with VaD as compared to DLB. Spine disorders were reported more frequently in VaD than DLB.
The results indicate that Q-Alb is especially increased in DLB when compared to the other diagnoses. DLB is characterized by the deposition of Lewy bodies, which are abnormal deposits of the protein alpha-synuclein inside neurons [26]. The cause of the accumulation of Lewy bodies is largely unknown, but studies have suggested that a high concentration of albumin increases the fibrillation of alpha-synuclein, which consequently leads to the formation of Lewy bodies [27, 28]. One might speculate, in the case of DLB, that albumin in the CSF not only serves as a measurement for the permeability of the BBB but might also be a part of the mechanism of the formation of Lewy bodies. However, other studies have reported the opposite. Two studies found that human plasma albumin (HSA) significantly decreased the aggregation and fibrillation of alpha-synuclein, and it was even proposed that HSA had a chaperone-like capacity against amyloid aggregation, which is a key parameter in the pathology of AD [29, 30]. More studies should be conducted in order to verify which explanation reflects the results found on Q-Alb in DLB in this study. In addition, we found the same overall pattern for CSF protein, which suggests that the majority of protein in the CSF is due to albumin [31, 32]. Furthermore, we found that the increased Q-Alb and CSF protein could not be attributed to confounding factors including vascular pathology, obesity or spine disorders in patients with DLB.
The results obtained on VaD indicate that this group, like the group with DLB, had a higher Q-Alb and CSF protein than the healthy controls and most other patients. BBB disruption is an important part of the pathophysiology of VaD [2], and several studies have reported that patients with VaD exhibit increased Q-Alb when compared to patients with other dementia diagnoses [33]. VaD can be caused by infarcts or white matter lesions with the latter particularly prevalent in our VaD subjects (Fazekas score (mean (SD)=2.86 (0.36)). These white matter lesions can in turn lead to degenerative changes in the endothelial cells of the intracerebral capillaries and arterioles of the BBB. Consequently, a dysfunction in the endothelial cells leads to an increased permeability of the BBB, which may explain why Q-Alb is increased in patients with VaD [9]. Since no significant difference between VaD and DLB was found, we suggest that Q-Alb as a marker of BBB integrity together with imaging modalities (CT or MRI) may serve as a suitable biomarker for DLB since a significant difference in Fazekas score was found between the two groups (p=<0.001, t = 12.28). However, recent evidence has suggested that CSF platelet-derived growth factor receptor-β, which is associated with pericyte damage, may serve as a biomarker of BBB integrity [34, 35]. Future studies should therefore investigate the potential role of platelet-derived growth factor receptor-β as a diagnostic marker for DLB.
When analyzing the association with age in HC, we found a trend toward an association between increased CSF protein and age (p = 0.082, ρ=0.298). Younger patients with AD showed a lower CSF protein than older patients with AD (p = 0.009, t = 2.636). Previous studies have shown that the load of vascular co-morbidities increase with age [36, 37]. We hypothesize that the difference in vascular load is the reason for the difference in CSF protein between the younger and older patients with AD. Furthermore, the positive association with age could potentially be explained by the increasing prevalence of degenerative spine disorders in older participants, which is known to impair spinal CSF circulation. Since previous studies have found a positive association between Q-Alb and age in healthy controls [38, 39], the lack of association in the current study may be due to the low sample size in HC.
The HC group was recruited for research purposes and did not suffer from severe co-morbidities, and therefore form a group that is probably healthier in a general sense. On the other hand, NC showed a higher Q-Alb than HC, which may be due to vascular disease or undiagnosed psychiatric disorders [40], for example, depression [41].
The current study has some limitations. The data were collected retrospectively, which means that some of the patient data were missing and further characterization of the patients was not possible. In addition, albumin is a large protein with a molecular weight of 66 kDa, which means that it cannot be used to determine if patients have micro-leaks of protein. Therefore, future studies investigating smaller molecules are needed. Furthermore, the low number of patients with DLB may influence the findings. Therefore, larger studies are needed to investigate the role of Q-Alb and CSF protein as a supplementary diagnostic marker.
Conclusions
In conclusion, Q-alb was significantly higher in both patients with DLB and VaD, but the underlying pathological processes in these diseases have previously been shown to differ. Furthermore, there seems to be a positive association between both CSF protein and age, as well as Q-Alb and age, which may be related to the load of vascular co-morbidities. However, the patients with DLB showed high Q-Alb and CSF protein, but a significantly lower Fazekas score than VaD. These results suggest that Q-Alb can contribute to our understanding of the pathophysiological mechanisms of DLB and suggest a disruption of BBB integrity, and Q-Alb may serve as a supplementary biomarker in the diagnosis of DLB in a memory clinic setting.