
Abstract
Background:
Gender differences have been noted in studies linking blood pressure to all-cause dementia, and the two most common forms of dementia: Alzheimer’s disease (AD) and vascular dementia (VaD). However, how gender modifies the relationship between blood pressure and dementia remains unclear.
Objective:
To review evidence for a gender modifying effect on the link between blood pressure and all-cause dementia.
Methods:
A systematic review was conducted according to PRISMA guidelines. Sixteen out of 256 reviewed articles met inclusion criteria.
Results:
For women, higher midlife systolic blood pressure (SBP) and hypertension were both associated with greater risk of all-cause dementia, AD, and VaD, in six out of seven studies. Two of these studies reported higher midlife SBP/hypertension were associated with greater risk for all-cause dementia in women, but not men. One study reported higher midlife SBP associated with greater AD risk in women, but not men. However, another study reported that midlife hypertension associated with AD risk in men, but not women. No clear gender differences were reported in the relationship between late-life high blood pressure/hypertension with all-cause dementia or AD.
Conclusion:
Studies rarely, and inconsistently, analyzed or reported gender effects. Therefore, interpretation of available evidence regarding the role of gender in blood pressure associated dementia was difficult. Several studies indicated higher midlife SBP was associated with greater risk of all-cause dementia for women, compared to men. Future studies should evaluate women-specific aging processes that occur in midlife when considering the association between blood pressure and dementia risk.
Keywords
INTRODUCTION
Recently, studies have begun to identify prominent differences in disease manifestation between men and women [1]. Recognizing the need for representation of both men and women in clinical research, the National Institutes of Health (NIH) have revised guidelines regarding inclusion of women in research, and have formed specific guidelines requiring investigators to outline an analytic strategy for examination of sex as a biological variable in human and animal research [2, 3]. The increased recognition of gender differences in risk factors and symptomology of dementia—and specifically the two most common forms of dementia: Alzheimer’s disease (AD) dementia and vascular dementia (VaD)—has also resulted in a call to action for further attention toward sexually dimorphic neurology [4–8]. While both men and women are affected by AD and VaD, growing evidence indicates that risk mechanisms differ between men and women and further studies are warranted [9].
Women comprise two-thirds of people living with AD [10]. This gender disparity in prevalence of AD and other forms of dementia was previously attributed to age and survival bias. More recently, biological and environmental mechanisms of risk are increasingly thought to convey differences in dementia risk between men and women [11]. While it is still unclear whether there is also a gender difference in dementia incidence, several studies in European and Asian populations show that incidence diverges by gender after age 80 [12, 13]. In the U.S., women tend to live longer than men (mean life expectancy for men: 76.1 years; for women: 81.1 years) [10, 11]. One proposed explanation for the gender disparity in AD prevalence is that men who live longer exhibit superior cardiovascular health, and subsequently less AD risk [12]. Mounting evidence suggests that cardiovascular risk factors play an important role in both VaD and AD [13, 14]. Notably, AD with mixed neuropathology, including multiple neuropathologic comorbidities that most commonly include cerebrovascular disease, is the most frequent neuropathological finding in dementia [15]. Indeed, there is increasing consensus that “pure” AD with no other comorbid non-AD pathology is fairly uncommon in autopsy studies [15]. Whether cardiovascular disease represents a key pathway in which men and women differentially progress to dementia remains poorly examined, despite evidence that men and women differ in prevalence and biomarkers of cardiovascular diseases that have been identified as risk factors for AD and VaD [1, 16–18]. Vascular risk factors are more commonly reported in men for various reasons such as poor awareness, under-recognition of clinical symptoms, and lack of female representation in clinical trials. However, cardiovascular disease is also the leading cause of death in women worldwide, accounting for ∼22% of deaths [19–21]. Furthermore, women are more at risk of dying from cardiovascular disease than men [22]. In contrast, breast cancer, which has greater perceived risk for women, only accounts for ∼8% of deaths [23–25]. Thus, understanding gender differences in cardiovascular disease profile throughout adulthood may also shed light on the AD gender imbalance [18, 26].
Sex versus gender distinction
It is important to note that sex and gender are two separate, though related, concepts. Sex refers to the biological differences that arise from sex chromosome expression (e.g., XX and XY) [27, 28]. The terms “male” and “female” are used to refer to biological or physiological sex features, including gonads, sex hormones, external genitalia, and internal reproductive organs [29]. Gender is a separate construct defined by socio-cultural expectations and attitudes that shape behaviors, lifestyle choices and experiences [29]. Therefore, “gender” refers to individuals belonging to a social group [27, 28]. Though gender and sex often covary, making their distinct effects difficult to study, there are circumstances in which one’s gender and sex are not aligned [29, 30]. The studies reviewed here rely on self-report, which may include both an individual’s sex assigned at birth and/or gender identity. As we are unable to make the distinction between sex and gender, we choose to use the descriptive term “gender” in this review. However, future studies may find these definitions useful when choosing an accurate descriptive term.
The aforementioned NIH guidelines for clinical research encourage investigators to consider how their variable of interest specifically affects women, and require clinical trials to submit an analytic plan addressing sex differences [2, 3]. However, past AD clinical research has often covaried for sex without describing sex differences [31]. Moreover, even when differences between men and women are reported, studies have rarely expanded on findings by measuring sex-specific factors like sex hormones and history of pregnancy, or gender-specific factors like career choice, education, or marital history [31]. One example that underscores the importance of clearly defined sex and gender differences in clinical research is the study of hormonal oral contraceptive use. Usage of hormonal oral contraceptives has been linked to small increases in blood pressure in some women [32, 33]. More specifically, hypertension is more common in women who take oral contraceptives that combine estrogen and progestin [34]. To study whether oral contraceptive use is associated with AD risk, it would be important to consider how sex-specific factors, such as menstrual cycle and exogenous sex hormones (e.g., estrogen and progestin), might affect a woman’s brain structure and function. For example, studies have noted that oral contraceptive users show reduced hippocampal volume [35–37]. However, it would also be important to further consider the potential effects of the prevalence, typical duration of usage, and type of oral contraceptive commonly used by the cohort being studied. These factors are largely dictated by the current gender roles and expectations [38, 39]. The lack of literature outlining differential effects of sex versus gender factors bars robust theory-building and confuses the interpretation of currently reported differences between men and women.
Gender differences in dementia presentation and neuropathology
Despite the potential importance of gender survival bias in the aging population, increasing evidence suggests that gender differences in dementia risk and underlying pathology are not entirely attributed to age. For example, men and women show differential effects of the apolipoprotein E4 (ApoE4) allele, the strongest genetic risk factor for AD [40, 41]. ApoE4 carrier women between ages 65–75 have greater AD risk than ApoE4 carrier men of the same age [42, 43]. Compared to men, ApoE4 carrier women also exhibit more cortical thinning, rapid cognitive decline, episodic memory deficits, and conversion from healthy aging to both mild cognitive impairment (MCI) and AD [40, 44]. ApoE4 also conveys higher risk of mortality due to both dementia and cardiovascular disease for women compared to men [44]. Despite these intriguing clinical and pathological observations, the mechanisms underlying the interaction between gender and ApoE4 remain unclear.
Independent of ApoE4, there are many reported differences in both AD clinical symptom and biomarker presentation. Both in vivo and postmortem investigations have observed subtle, but detectibly higher AD-related neuropathological burden at the molecular level in older women [45, 46]. For example, women, compared to men, exhibit greater flortaucipir F18 positron emission tomography (PET), independent of ApoE4 status, and largely attributable to higher level of tau-tangle density [45]. Clinically, the rate of cognitive decline is twice as fast for women than for men with MCI [5]. In contrast, women with amnestic MCI tend to exhibit relatively more preserved verbal memory compared to men [47]. This relative preservation of verbal memory aligns with reports that women in the general population tend to perform better than men in verbal memory tasks across the lifespan [48]. However, women diagnosed with AD have also shown worse verbal memory performance compared to men with matched disease severity and ApoE4 carrier status, potentially reflecting the difference between men and women in rate of cognitive decline [49]. Women diagnosed with AD are also more likely to exhibit depressive symptoms [50]. Women in the general population are more likely than men to experience depression across much of the lifespan, and depression itself may convey independent risk for AD [51, 52]. Identification of gender differences in risk profile as well as symptom and biomarker progression may highlight important treatment targets that are specific to women.
Gender, blood pressure, and dementia risk
High blood pressure is a cardiovascular condition linked to increased risk for both AD and VaD in samples that include men and women. High blood pressure demonstrates links to both cognitive decline and cerebrovascular disease, findings that have been reviewed extensively elsewhere [53–59]. Higher blood pressure has also been linked to AD-related changes such as increased brain amyloidosis [60, 61], higher CSF phosphorylated tau (P-tau) [62], reduced gray matter and hippocampal volume [63, 64], greater white matter lesion volume [65], and worse cognitive performance [66]. However, many aspects of the association between high blood pressure and AD or VaD risk remain unclear.
As a risk factor, high blood pressure is worthy of consideration because it affects the majority (86%) of adults over age 65 [67] and is modifiable through lifestyle or pharmaceutical treatment [68–71]. In fact, aggressive treatment for systolic hypertension older adults with vascular risk has been shown to attenuate incidence of MCI, a major risk for AD [72]. While some studies have reported a “J” shaped association (e.g., only very high blood pressure predicts AD), others have identified a “U” shaped association (e.g., both low and high blood pressure predict AD), and still others have seen no relationship [73–77]. Men tend to develop hypertension approximately 10 years earlier than women [78]. Women, on the other hand, become more at risk for cardiovascular disease post-menopause [1, 79]. In fact, men have higher incidence of high blood pressure than women throughout the lifespan until women reach menopause [80]. As the average age of menopause is approximately 51 years old [81], this may represent a crucial window of risk for development of AD or VaD later in life. The mechanisms that help maintain steady blood pressure across different levels of sympathetic nervous system activation differ between women and men, such that younger women tend to show several protective effects against hypertension [82, 83]. Therefore, hypertension may develop via distinct pathways for women compared to men [83]. Further research is needed focusing on how women-specific pathways to hypertension may also impact brain health and dementia risk.
In terms of blood pressure-related autoregulation, women, compared to men, also have shown higher cerebral blood flow velocity, cerebral vasomotor reactivity, and cerebrovascular reactivity [84–86]. One study demonstrated women over age 70 exhibited better cerebral autoregulation, or maintenance of cerebral blood flow during sit-to-stand postural changes [87]. Reduced cerebral blood flow is particularly implicated in VaD, and higher cerebral blood flow in older women may explain why VaD is more prevalent in men [88].
The current review
The current systematic review investigates the role of gender in the relationship between blood pressure and all-cause dementia risk, with a sub-focus on dementia due to AD and/or vascular disease. Female subjects, both human and animal, have historically been underrepresented in scientific research, and particularly within the realm of cardiovascular disease [89]. Despite evidence of gender differences in AD presentation and progression, studies infrequently focus on gender as a modifying variable. Previous reviews have examined links between menopause and cognition, as well as hypertension and cognition in menopausal women [90–92]. However, no reviews to-date have examined gender differences in the relationship between blood pressure and dementia risk. Of note, there are multiple types of dementia with distinct clinical presentation and putative differences in etiology, including AD and VaD, but also Lewy body dementia (DLB), Parkinson’s dementia, (PDD), frontotemporal dementia (FTD), and other less common forms of dementia such as chronic traumatic encephalopathy (CTE) [93, 94]. Men are more likely to experience certain types of dementia, such as PD, DLB, and CTE [95, 96]. However, women exhibit greater overall dementia burden, including AD [97]. VaD is the second most prevalent form of dementia, and vascular brain injuries such as cerebral infarctions and hemorrhages are found in about 40% of brains from individuals with dementia [97–99]. We chose to focus this review on all-cause dementia, and to include AD and VaD as they represent the two most common forms of dementia, have high rates of comorbidity, and are most frequently studied.
MATERIALS AND METHODS
We conducted a qualitative systematic review of the literature rather than a meta-analysis for this study due to lack of uniformity of methods across the selected studies. The key variables of sex/gender, blood pressure, and dementia were all defined differently across studies. Furthermore, studies varied in analytic approach for testing sex differences. The primary goal of the present study is to review studies that test and report sex or gender differences in the relationship between blood pressure and dementia risk. As more rigorous and uniform testing of sex differences is a developing area within this topic of study, this may partially contribute to the variability of study methodologies reviewed here.
Database search
Using PRISMA guidelines [100], a systematic review of the literature concerning the relationship between blood pressure and risk of dementia, with a focus on gender-differences and female population, was conducted in October 2019. Eligible papers were published research articles and unpublished dissertations. Results were limited to human subjects. No lower limit was applied for date published. Both cross-sectional and longitudinal studies with variable length of follow-up were included. The primary author (AB) identified and gathered articles using the following electronic databases: PubMed, Ovid MEDLINE, and Web of Science. Search results were uploaded into Mendeley Desktop for record management (e.g., avoiding duplicate records) and organization. The following Boolean search terms, with three categories of words linked with the “AND” operator, were considered: 1) “blood pressure” OR “hypertension” 2) “sex” OR “gender” 3) “dementia”. The search yielded 1,641 results.
Inclusion criteria
Selection criteria included English language, peer-reviewed, original research articles that examined the association between blood pressure and risk of all-cause dementia diagnosis and reported gender-specific analyses or otherwise focused on women. If specified, gender differences in risk for AD or VaD were also reviewed. Unique citations from papers published prior to October 2019 in the combined results from the three database searches were reviewed. The primary author (AB) also reviewed citations from relevant articles, and publication archives from well-known cohorts. Ancestry and descendancy searches yielded 4 additional articles [76, 101–103].
Exclusion criteria
Articles were excluded when the subject population did not include women, the subjects were a clinical population without focus on AD or VaD diagnosis (e.g., stroke, kidney failure, Parkinson’s or Huntington’s diseases), or the study reported on dementia caregivers. Clinical trials were excluded. Articles with “cognitive impairment” as the outcome were also excluded, as cognitive impairment is not exclusive to dementia. While MCI is an established risk factor for dementia, not all patients with MCI progress to dementia, and many revert back to normal cognition [104, 105]. Therefore, the present review chose to focus dementia as an outcome, more definitively reflecting pathophysiological changes. Articles investigating dementia risk related to “vascular risk factors” as a composite variable or “metabolic syndrome” that did not report specific associations for hypertension/blood pressure were not included. Studies reporting on measures derived from blood pressure (e.g., pulse pressure or blood pressure variability) were also excluded as they relate somewhat differently to vascular function (e.g., arterial stiffness) and may be considered independent risk factors [106–109]. Finally, studies that did not test sex or gender differences in the relationship between blood pressure and dementia were excluded.
RESULTS
Study characteristics
The flow diagram in Fig. 1 illustrates the review process. Initial search results were imported into Mendeley for organization and deletion of duplicates, yielding 1,645 records. Review of titles to exclude unrelated topics resulted in 256 records. After review of abstracts, 67 records were determined to be relevant to the scope of this paper. Finally, the author (AB) reviewed methods and results sections, excluding papers that lacked focus on blood pressure, or that did not indicate any testing for sex/gender differences. For those that met these criteria, the author also reviewed record references as well as works that cited the selected record, resulting in 4 additional articles. A total of 16 publications met selection criteria. All studies reviewed were observational and prospective in design. The study populations ranged from 707 to 848,505 participants. Blood pressure was modeled in a variety of ways, including cross-sectional measurement on a continuous scale, two or more categories of blood pressure range, or diagnosed hypertension. Studies also varied in choice of outcome measures which included all-cause or total dementia, AD, and VaD. One study differed such that blood pressure on a continuous scale was modeled as the outcome variable for three distinct dementia classification groups [76]. We report here the models that examined differences between men and women, or that were specific to one gender. The following publication characteristics are reported in Tables 1 and 2: study population, first author, year, country, number of participants, measurement and definition of sex or gender, % women, mean age (years), age range, mean follow-up (years), outcome measure, dementia type, diagnostic criteria, hypertension definition (if reported/applicable), and covariates.
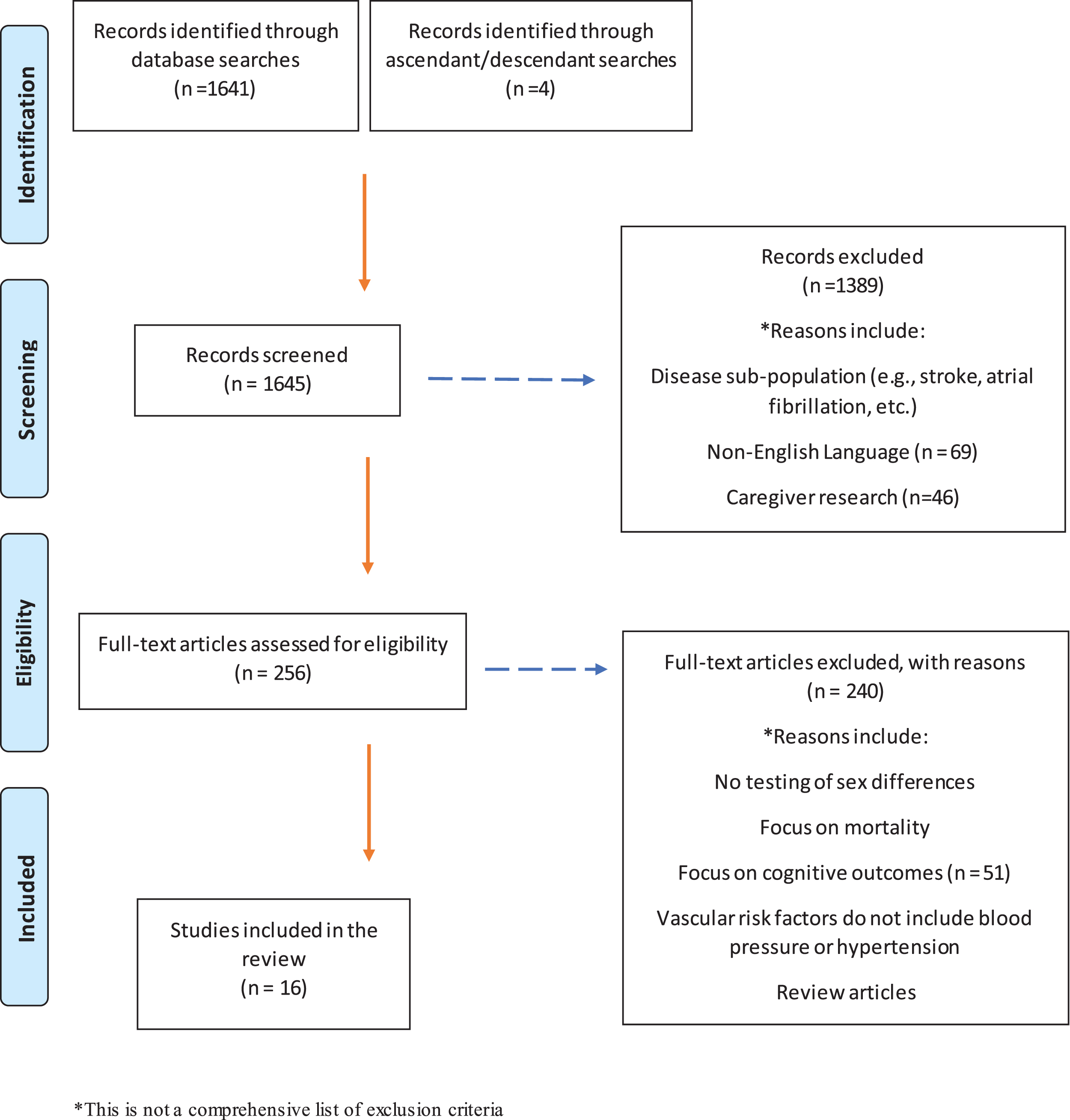
PRISMA flow diagram describing article selection process.
Study characteristics: Midlife blood pressure and risk of dementia
SBP, systolic blood pressure; DBP, diastolic blood pressure; BP, blood pressure; AD, Alzheimer’s disease; VaD, vascular dementia; TX, treatment.
Study characteristics: Late life blood pressure and risk of dementia
SBP, systolic blood pressure; DBP, diastolic blood pressure; BP, blood pressure; AD, Alzheimer’s disease; VaD, vascular dementia; TX, treatment.
Organization of findings
Age may modify the relationship between high blood pressure and both AD and VaD [53]. Several studies have, in fact, demonstrated a stronger association between high systolic blood pressure measured in midlife (e.g., <60 years old), and later risk of both AD and VaD [53, 110–113]. Research has been limited by inconsistent findings that may be due to cross-sectional study design, possible confounding effects of age, cohort, or type of blood pressure treatment, as well as variable quality of measures (e.g., number of blood pressure measurements) [114, 115]. However, as older individuals are subject to many more comorbidities that may complicate or mask diagnosis, the effect of high blood pressure on AD risk may be underestimated [116].
The studies reviewed here have been organized and synthesized in two groups: seven articles, with results summarized in Table 3, had a mean study participant age of <60 years or reported on midlife cardiovascular risk factors, and nine articles, with results summarized in Table 4, had mean study participant age of 60+. Although the mean age of the study by Whitmer et al. (2005) [111] was >60 years, the authors included midlife measures of cardiovascular risk (including hypertension), and thus are included in the midlife section. The reasons for this separation of studies include the distinction in the literature between mid- and late-life high blood pressure as a risk factor for AD or VaD, and the documented shift in blood pressure levels pre- and post-menopause. Study findings are further organized by diagnosis (e.g., AD versus VaD), if specified by the study.
Summary of midlife blood pressure and risk of dementia results
SBP, systolic blood pressure; DBP, diastolic blood pressure; BP, blood pressure; AD, Alzheimer’s disease; VaD, vascular dementia.
Summary of late life blood pressure and risk of dementia results
SBP, systolic blood pressure; DBP, diastolic blood pressure; BP, blood pressure; AD, Alzheimer’s disease; VaD, vascular dementia.
Age and education were the most commonly reported covariates included in analyses. Race, antihypertensive treatment, vascular risk factors (e.g., smoking status, diabetes), cardiovascular comorbidities, and ApoE4 carrier status were inconsistently reported and included in analyses. Tables 1 and 2 provide further details on covariates adjusted for in each study.
Gender differences in links between blood pressure in midlife and risk of dementia
Five out of seven studies treated hypertension as a categorical variable [102, 117–119]. Two of the seven studies analyzed systolic and diastolic blood pressure as continuous variables [120, 121]. Definition of dementia encompassed AD, VaD, and other dementia etiologies in six out of seven studies [111, 122]. One study provided further analyses for specific dementia types [121]. One study defined dementia as “Probable AD,” and provided further analyses for “Pure AD,” excluding cardiovascular or other pathological contributions to dementia [120]. Information detailing individual study definition of exposure and outcome are outlined in Table 1. Overall, six out of seven studies reported an association between high blood pressure in midlife and increased risk of dementia in samples that included both men and women.
Six out of seven midlife studies reported that women with high systolic blood pressure or hypertension diagnosis had increased risk of dementia [102, 121]. Two studies observed that women with high midlife systolic blood pressure or hypertension diagnosis had higher dementia risk, and not men [117, 121]. On the other hand, three studies did not see a difference in dementia risk between men and women with elevated midlife blood pressure [102, 123]. One study, conducted by Joas et al. (2012), did not include men in their sample and no gender comparison could be made [120].
Three studies had higher average ages (Kimm et al. (2011) [119]: 51.9 for men, 53.6 years for women; Gottesman et al. (2017) [118]: 54.2 years; Alonso et al. (2009) [102]: 56.4 years) than the two studies reporting a gender x blood pressure interaction (Gilsanz et al. (2017) [117]: 44.3 years; Gabin et al. (2017) [121]: 51.8 years).
Two studies examined the relationship between blood pressure changes over time and dementia risk. Blood pressure trajectories tend to differ between women and men over the lifespan, which may affect dementia risk [124]. Gilsanz et al. (2017) reported that women who had developed hypertension in their 40s had a 65% higher risk of dementia, compared to men with midlife hypertension and individuals who had not developed hypertension during early-to-middle adulthood [117]. In another study, Joas et al. (2012) used linear mixed models to examine blood pressure changes between 1968 and 2006 in women with or without treatment for hypertension [120]. Authors adjusted for potential confounding effects of education, smoking, stroke, cardiovascular disease, diabetes mellitus, midlife stress, and cholesterol at baseline. The non-treatment group did not exhibit any difference in systolic blood pressure trajectory between women who developed AD or VaD/mixed, and those who did not. Women who developed dementia exhibited higher baseline systolic blood pressure, measured during midlife. Women taking antihypertensive medication who developed dementia experienced a larger increase in systolic blood pressure over the study period.
Gender differences in links between blood pressure in midlife and AD and VaD dementia types
Two studies reported on AD and VaD separately. Kimm et al. (2011) reported that midlife hypertension was associated with increased risk VaD in both men and women. Midlife hypertension was only associated with increased risk of AD for men who were <65 years old [119]. Gabin et al. (2017) [121] reported that women <60 years old with higher systolic and diastolic blood pressure exhibited greater risk for dementia and AD, compared to men. One study showed that elevated midlife systolic blood pressure was associated with AD in both men and women who used antihypertensive medication [121]. Joas et al. (2012) reported that women who had higher systolic blood pressure during midlife and were not undergoing antihypertensive treatment had greater risk for AD [120].
Gender differences in links between later life blood pressure and risk of dementia
Two studies conducted analyses stratified by age (e.g., midlife versus late life), and are therefore included in both age group sections of this review [119, 121].
Seven out of nine studies examined hypertension or blood pressure as a categorical variable of risk for dementia [101, 125–129]. One study examined blood pressure as a continuous variable [55]. One study reported analyses with both hypertension as a categorical variable and blood pressure as a continuous variable [76]. Eight out of nine studies included all-cause or “total” dementia (e.g., both AD and VaD) as a main outcome variable [55, 130]. Five of nine studies provide further analyses for AD and VaD separately [119]. One study only included analyses for participants who met criteria for “Probable” or “Possible” AD [129]. Definition of exposure and outcome for each study are provided in Table 2. Overall, in four out of nine studies higher blood pressure or hypertension was associated with decreased risk of dementia in samples that included men and women [55, 121]. Three of nine studies reported that in the whole sample, greater decline in late life blood pressure was associated with greater risk of dementia [55, 125].
Five studies reported no association between high blood pressure and dementia risk in samples containing both men and women, as well as no evidence of gender effects. Most studies tested for gender differences using a gender x blood pressure interaction term in their models, while Kimm et al. (2011) [119] and Ruitenberg et al. (2001) [55] conducted gender-stratified analyses. Two studies with samples composed entirely of women also reported no relationship between high blood pressure and dementia risk [127, 128]. While authors Israeli-Korn et al. (2010) do report that individuals with hypertension during late-life exhibited increased AD risk, no gender x hypertension interaction was found [130].
Three studies examined blood pressure change over time in relation to diagnosis of dementia [55, 125]. In a study of older women, systolic blood pressure increased less in women who developed dementia [76]. The same study of older women also found that diastolic blood pressure decline more in older women who developed dementia [76]. Both Ruitenberg et al. (2001) [55] and Qiu et al. (2004) [125] reported greater blood pressure decline among all older adults who developed dementia or AD compared to those who did not. The effect of declining blood pressure on dementia, AD, and VaD risk was stronger for systolic blood pressure. There was no evidence of woman-specific blood pressure changes in relation to dementia, AD, or VaD risk.
Gender differences in links between later life blood pressure and AD and VaD dementia types
One study reported that late life hypertension in both men and women was associated with increased risk of VaD [119], with an attenuated effect for older versus younger men. Another study reported that hypertension was associated with increased VaD risk only in women [126]. In line with these results, Yamada et al. (2009) also report hypertension was associated with increased risk of VaD in an all women sample [128]. Gabin et al. (2017) reported that both men and women ≥60 years old with higher systolic blood pressure were at lower risk for dementia, mixed AD/VaD, and AD, but not VaD [121]. Obesity in women, another vascular risk factor, was associated with an increased risk of AD and not VaD [126].
DISCUSSION
This review summarizes existing literature regarding how the relationship between blood pressure and dementia may differ in men and women. Several studies provided evidence that high midlife systolic blood pressure or hypertension was associated with later risk of AD or dementia [102, 131]. Out of these, some studies indicated that the effect of high midlife systolic blood pressure or hypertension on risk of AD or dementia was present in women, and not men [117, 121]. In participants ≥60 years old, there was no strong evidence of a gender interaction for the effect of high systolic blood pressure or hypertension on risk of AD or dementia.
A limited number of studies reported results for VaD risk alone. In one study, high midlife systolic blood pressure or hypertension was associated with greater risk of VaD in both men and women <60 years old [119, 128]. One study reported that high late life systolic blood pressure or hypertension was associated with greater risk of VaD in women, specifically [126].
Sex-specific factors in hypertension and high blood pressure
While it is typically observed that premenopausal women demonstrate protection against hypertension, many premenopausal women still develop hypertension [83]. There are several notable factors specific to women that influence blood pressure including oral contraceptive usage, pregnancy, and menopause [132–134]. For example, during normal pregnancy, cardiac output and blood volume, and vasodilatation increase, while blood pressure decreases [135]. Resistance to pressor agents, such as norepinephrine and angiotensin II, is also characteristic of normal pregnancy [136]. Hypertension affects 10–15% of pregnancies, and the prevalence rates of a range of hypertensive disorders (e.g., gestational hypertension, pre-eclampsia, eclampsia, post-partum hypertension) during and after pregnancy are rising [137]. Several studies suggest that hypertensive pregnancy may increase risk of AD, cognitive decline, white matter lesion burden, and brain atrophy [138, 139]. Despite this, it is unclear the extent to which hypertensive pregnancy disorder might influence AD or VaD pathways to risk.
Menopause is a stage defined by the cessation of menstruation and ovarian follicular activity and is accompanied by a large shift in production of the female sex hormone estrogen, or estradiol [140, 141]. Women typically enter menopause around age 50, with a subsequent spike in risk of cardiovascular disease and, sometimes, cognitive impairment [142, 143]. The prevalence of hypertension is higher in post-menopausal women compared to men of the same age, and hypertension is associated with greater risk for cardiovascular disease for women in their 50s, compared to men of the same age [144, 145]. Climacteric refers to the approximately 2–8 years over which a woman experiences menopause-related changes, including the decline in ovarian activity through ovarian function cessation, and one year following final menses [146]. This time period is linked to numerous changes in cardiovascular function, including impaired endothelial function, atherosclerosis, autonomic function, and changes in adiposity [147–150]. Moreover, post-menopausal women experience steeper increases blood pressure [151]. The studies reviewed here provided evidence that high blood pressure during midlife—consistent with the age at which most women begin to experience menopause changes—was associated with greater dementia and AD risk in women. Menopause-related estrogen depletion and subsequent cardiovascular outcomes, such as endothelial dysfunction, may therefore represent a distinct pathway by which high blood pressure affects risk of dementia in women.
Estrogen may play an important role in the mechanism behind sex differences in blood pressure and risk for dementia. Endogenous estrogen, specifically 17β-estradiol (E2), has been shown to increase levels of nitric oxide, which is necessary for blood vessel dilation, and reduce levels of endothelin, necessary for blood vessel constriction [152–156]. E2 also influences the amount of elastin and collagen, necessary for flexibility of vessel walls [157–160]. Furthermore in premenopausal women, blood vessels tend to show attenuated constriction response to release of norepinephrine [82, 161]. After menopause, and the subsequent loss of endogenous estrogen, there is an observable increase in sympathetic activity and in adrenergic vasoconstrictor responsiveness that may explain the spike in hypertension seen in post-menopausal women [82]. Estrogen depletion may also accelerate arterial stiffening, thought to precede blood pressure changes, which is linked to increased cerebrovascular damage and may also provide insight into why women appear to show higher levels of AD-related neuropathologies [162, 163]. Women experience transitions in endogenous estrogen levels, including E2, at several different stages of life, and exogenous sex hormones can vary widely as hormonal contraceptive therapy is widely used from an early age. Despite evidence that estrogen depletion potentially plays an important role in development of hypertension and risk of AD or VaD, no study reviewed here, and few studies overall, measure endogenous estrogen levels. Given the hypothesized protective effects against hypertension for premenopausal women [146], it is particularly important to understand the mechanisms which contribute to high blood pressure in this age group, as they may also signify risk for AD or VaD. Improved understanding of the biological changes associated with large shifts in hormone levels experienced by women may offer critical insights into how men and women may differ in terms of AD risk and treatment response.
Gender-specific risk factors for dementia
The most commonly cited gender-specific risk factor for dementia is education [6, 164]. Higher educational and occupational attainment are thought to be protective factors in the context of dementia [165]. Education and occupation opportunities have traditionally been more limited for women, particularly those in the current older adult cohorts [31, 167]. Even though these differences have greatly shifted over time, men and women still tend to differ in lifestyle factors such as occupation history and exercise, which also interact with educational attainment and socioeconomic status [168]. For example, studies of maternal employment in the U.S. reported that mothers with less than high school education have higher rates of unemployment than those with more years of education during the 10 years after giving birth [168]. The choices and timing of women leaving and re-entering the workforce after birth depend heavily on country of residence, education, and race/cultural expectations [169]. Furthermore, women are more likely to fulfill caregiving roles within their family units which may provide challenges for occupational attainment earlier in life and may actually convey risk later in life, as it is well documented that women are more likely to take on caregiving burden with dementia patients and caregiving may increase risk of dementia [170].
Treatment implications
More tailored treatment plans, also referred to as precision medicine, consider as many factors as possible that may be contributing to disease pathogenesis, expression, and progression. It is necessary to provide education to combat the common belief that women are not at great risk of cardiovascular disease compared to men [171]. In fact, this cultural misconception has played out in detrimental ways as women have been underrepresented in cardiovascular research, women have been found to underreport cardiovascular symptoms, and cardiovascular disease is often underdiagnosed women [172–176]. Greater health awareness for women may improve clinician ability to diagnose, treat, and prevent negative outcomes.
Data from the Framingham Heart Study indicates that pharmaceutical control of blood pressure is more difficult to achieve in older women compared to men [177]. Furthermore, pattern of anti-hypertensive prescription differs between men and women, as it was widely debated for several years whether women who were pregnant could safely use angiotensin-converting enzyme inhibitors and angiotensin receptor blockers due to risk of fetal developmental abnormalities [178]. Therefore women are more likely to be prescribed diuretics regardless of pregnancy status, whereas men are prescribed beta-blockers, angiotensin-converting enzyme inhibitors, or angiotensin receptor blockers [179–181]. As angiotensin receptor blockers may decrease risk of dementia, attenuate age-related changes in cerebral amyloidosis, and have significant cognitive benefits when compared to other anti-hypertensive medications, this could be an important factor driving increased dementia risk for women with high blood pressure as observed in the studies reviewed here [72, 182–184]. Although sex is a common covariate in clinical trial studies, it is unclear whether men and women differ in potential benefits of antihypertensive treatment.
Menopause is an important treatment target to consider due to the potentially neuroprotective effect of estrogen in the brain. For example, higher levels of estrogen are associated with increased dendritic spine density in the hippocampus, and estrogen plays a regulatory role in inflammation regulation [185, 186]. Treatment of menopause symptoms in older women using hormone replacement therapy (e.g., estrogen plus progestin) was previously shown to lower cognitive function and increase AD risk, in addition to other harmful health outcomes [187]. Researchers have revisited the potentially beneficial effects of hormone replacement therapy with careful consideration of timing, dosage, and method of hormone synthesis [186, 188]. However, many have shown no benefit, or neutral effects, of hormone treatment for cognitive function [189–193]. Therefore, there are substantial limitations and wide gaps of knowledge that need to be addressed the use of hormone therapy in relation to dementia and related cognitive changes [194].
Limitations
A clear limitation of this review is the dearth of studies sufficiently evaluating how men and women differ in risk for AD. Furthermore, in several of the studies reviewed here, even when gender difference analysis was reported in the methods, the results were not reported. In some cases, even when a significant sex interaction was reported, the topic was not included in the paper discussion. Another limitation is that although there are many more large extant studies addressing the role of blood pressure in dementia risk, they have not yet published analyses addressing gender or sex differences and could not be included in this review [195–198]. Therefore, it is unclear whether the existing literature is an accurate report of existing investigations on the differential effect of the gender x blood pressure interaction on dementia risk. Furthermore, even in those studies testing for gender differences, it is difficult to draw meaningful conclusions due to lack of power. For example, in the study by Kimm et al. (2011) only 37 patients were diagnosed with VaD [119]. Future investigation into gender differences will require larger sample sizes in order to generate enough power to conduct both stratified analyses and interaction analyses to determine whether gender is a modifying factor. Gender difference research has often received criticism for underpowered analyses, small effect size, and lack of theoretical basis [199]. Therefore, it will be important for future gender-based models to include key variables that represent different paths by which men and women arrive at an AD diagnosis (e.g., sex hormone levels). Furthermore, increased attention is needed on covariates that are highly relevant to either men or women, such as hypertensive disorders of pregnancy.
Recent work suggests that women underestimate their risk of cardiovascular disease, leading to poor outcomes, underreporting, and serving as a potential confound in research studies examining gender differences [175, 176]. In the studies reviewed here, years of follow-up (range: 12.8–37.0 years) and diagnostic criteria of both AD and hypertension could be considered as possible confounding variables. Studies focused on midlife blood pressure as a risk factor for dementia may be particularly vulnerable to bias due to long period of follow-up, during which the study population may experience changes to risk factors and attrition, as high blood pressure is also risk factor for cardiovascular events and mortality [200]. Furthermore, measurement of blood pressure as a risk factor was inconsistent across studies. One study treated blood pressure as a continuous variable, whereas the others used a standard cutoff for categorization of hypertension (e.g., systolic blood pressure of at least 140 mmHg or a diastolic blood pressure of at least 90 mmHg). An advantage of examining blood pressure as a continuous variable is that it is inclusive of individuals with subthreshold cardiovascular disease (e.g., prehypertension) who still accumulate cerebrovascular damage. In fact, midlife prehypertension was a significant risk factor in the Atherosclerosis Risk in Communities (ARIC) study [122].
Another limitation is the variability across studies in outcome definition. Most studies used ICD-9 or ICD-10 discharge codes for AD and VaD along with varying quality of neurological examination. Whitmer et al. (2005) note that a significant limitation to their study is heavy reliance on self-report and patient charts for cardiovascular risk and dementia diagnosis [111]. They indicated that this may have resulted in underestimation of the effect of cardiovascular risk factors. In turn, this may have underestimated the effect of gender on the relationship between hypertension and dementia due to poor record keeping or undiagnosed dementia. Another study reviewed here that did not note gender differences operationalized “risk” as evidence of hospitalization due to dementia [102]. While the authors justify their use of this proxy with evidence, several problems may affect the interpretation of their results. As they note, individuals with cardiovascular risk have a higher risk of hospitalization [102].
Future directions
More high-quality research is needed to discover whether vascular risk factors and cerebrovascular pathology differ between men and women over time. More specifically, future studies should evaluate the role of hypertension in pregnancy, menopause, estrogen levels in relation to dementia risk. It is unclear whether women are particularly vulnerable to the cumulative effects of vascular and AD pathologies, leading to differences in prevalence and progression. It is also unclear to what extent genetic and sex hormone differences between men and women play a role in dementia development. Finally, it is possible that higher mortality for men may influence the estimated effect of reported risk factors, a factor that also warrants further clarification [201].
Notably, low blood pressure and orthostatic hypotension have also been examined as risk factors for dementia, especially in very old or frail individuals [202–205]. Orthostatic hypotension is prevalent in older adults [206]. Women may be at greater risk for orthostatic hypotension, but differing prevalence between men and women has been inconsistently reported [207, 208]. Relatedly, orthostatic hypotension can reflect autonomic dysfunction which can also result in greater blood pressure variability, another emerging area of risk for dementia [209–212]. To our knowledge, sex differences in the associations between orthostatic hypotension or blood pressure variability and dementia have yet to be investigated and represent an important area of future research.
It is worthwhile to examine how sex-specific factors (i.e., sex hormones, neurological underpinnings, menopause, puberty) contribute to changes in AD pathophysiology (e.g., amyloid and tau accumulation) and related brain changes (e.g., cerebrovascular pathology, changes in cerebral autoregulation, etc.) [8]. Further interpretation of how these factors interact with socio-cultural variables related to gender, such as education, occupation, and social roles may shed light on the evident disparity in dementia frequency between men and women. It may be particularly important to consider whether any of the relationships between risk factors, such as blood pressure, and dementia risk show distinct age-dependent effects for men and women. Finally, since menopause typically occurs between ages 50–52 it may be important to stratify analyses at this point in a woman’s life [213].
Conclusion
This systematic review seeks to highlight the importance of considering both sex and gender-specific aspects of aging and dementia risk, which are largely overlooked and often poorly defined in the literature. The studies reviewed here point to midlife blood pressure as a risk factor for dementia, AD, and mixed AD/VaD, particularly for women. Findings further highlight the importance of age in consideration of the links between gender, blood pressure, and dementia. The past five years have seen increasing reviews and opinion pieces calling for the prioritization of gender/sex differences in the context of AD and dementia [8, 201]. With more rigorous testing of gender differences, we may be able to draw better conclusions that will inform clinical trial research, potentially improving efficacy of AD treatment, and aid clinicians in providing more precise diagnoses.