
Abstract
Background:
Delirium is associated with dementia and thus biomarkers reflecting neurodegeneration are of interest. Fatty acid-binding protein 3 (FABP3) is a cytoplasmic neuronal protein that has been isolated from the brain. It is released following brain injury and concentrations in cerebrospinal fluid (CSF) are also higher in neurodegenerative disorders such as Alzheimer’s disease (AD).
Objective:
To examine the relationship between CSF FABP3 concentration and delirium in hip fracture patients compared to a group of cognitively normal controls.
Methods:
CFS FABP3 concentration was measured in 128 hip fracture patients with (n = 71) and without (n = 57) delirium, and in cognitively unimpaired adults ≥64 years (n = 124) undergoing elective surgery.
Results:
CSF FABP3 (pg/ml) concentration (median (IQR)) was higher in hip-fracture patients compared to cognitively normal controls (5.7 (4.2–7.7) versus 4.5 (3.4–6.1), p < 0.001). There was a significant weak correlation between age and CSF FABP3 (ρ= 0.3, p < 0.001). After adjustment for age, the association between CSF FABP3 and hip-fracture was no longer statistically significant (β= 0.05, p = 0.5). There were no significant differences in CSF FABP3 concentration between hip fracture patients with (5.4 (4.1–8.2)) and without (5.8 (4.2–7.2)) delirium. CSF FABP3 concentration correlated positively with CSF AD biomarkers p-tau (ρ= 0.7, p < 0.01) and t-tau (ρ= 0.7, p < 0.01).
Conclusion:
CSF FABP3 concentrations were higher in hip fracture patients compared with cognitively normal older adults, indicating ongoing age-related neurodegeneration in these patients. There were no differences of CSF FABP3 concentrations across delirium groups, suggesting that neuronal damage or degeneration reflected by FABP3 may not be directly linked to delirium pathophysiology.
INTRODUCTION
Despite the high prevalence and morbidity of delirium, the pathophysiological mechanisms are poorly understood [1, 2]. Epidemiologically and clinically, delirium is closely linked with dementia, and thus biomarkers of neurodegeneration are of interest [3, 4]. Associations between cerebrospinal fluid (CSF) concentrations of amyloid-β 1–42 (Aβ42), total tau (t-tau), and phosphorylated tau (p-tau) and delirium have been shown [5, 6], and the vulnerability to develop delirium increases with the degree of neuropathology, also in individuals without clinical dementia [5–7].
Fatty acid-binding protein 3 (FABP3) is a cytosolic protein found in various tissues, including heart, skeletal muscle, intestinal mucosa, liver, and kidney [8, 9]. It is also highly expressed in the adult brain, particularly in the pons, frontal lobe, and hippocampus [10, 11]. In the brain, FABP3 regulates the lipid composition of the membrane and transports fatty acids between different intracellular compartments [11]. It is released extracellularly after neuronal damage [10] and high CSF concentration of FABP3 is found in acute conditions, such as brain injury and stroke [12, 13]. CSF FABP3 concentration is also higher in conditions with neurodegeneration/neuronal damage, e.g., Alzheimer’s disease (AD) [14, 15], mild cognitive impairment (MCI) due to AD [15–18], dementia with Lewy bodies [19], and Creutzfeldt–Jakob disease [20]. CSF FABP3 concentration correlates with cognitive decline [19] and are associated with brain volume loss in areas selectively affected in early AD [21]. Thus, FABP3 is suggested to be a general marker of neuronal damage [8].
We wanted to test the hypothesis that CSF FABP3 is a marker of vulnerability for developing delirium. Thus, the aim of this study was to examine the relationship between concentration of FABP3 in CSF and delirium in hip fracture patients compared with a group of cognitively normal controls.
MATERIALS AND METHODS
CSF was collected from hip fracture patients recruited in the Oslo Orthogeriatrics trial and from cognitively normal patients admitted for elective surgery, at Oslo University Hospital and Diakonhjemmet Hospital, Oslo Norway.
The hip fracture patients were enrolled at Oslo University Hospital from 2009 to 2012, in a randomized controlled trial evaluating the effect of orthogeriatric care on cognitive function [22]. Participants with available CSF (N = 128) were included in the current study.
All hip fracture patients were screened for delirium once daily using the Confusion Assessment Method (CAM) [23] preoperatively and until postoperative day 5 (all) or discharge (patients with delirium). The study geriatrician or study nurses performed all assessments. The CAM scores were based on information from nurses, close relatives, and hospital records related to the preceding 24 h, as well as a 10- to 30 min interview with the patient, as earlier described.
For secondary analyses, delirium was further categorized as preoperative, incident (i.e., delirium not present preoperatively, but developed at any point until assessments stopped), or subsyndromal delirium (SSD, defined as two or more positive CAM items but never fulfilled criteria for full-scale delirium) (Fig. 1). Proxies were interviewed regarding prefracture activity of daily living (using Barthel ADL index [24]) and prefracture cognitive function using the Informant Questionnaire in Cognitive Decline in the Elderly (IQCODE) [25].
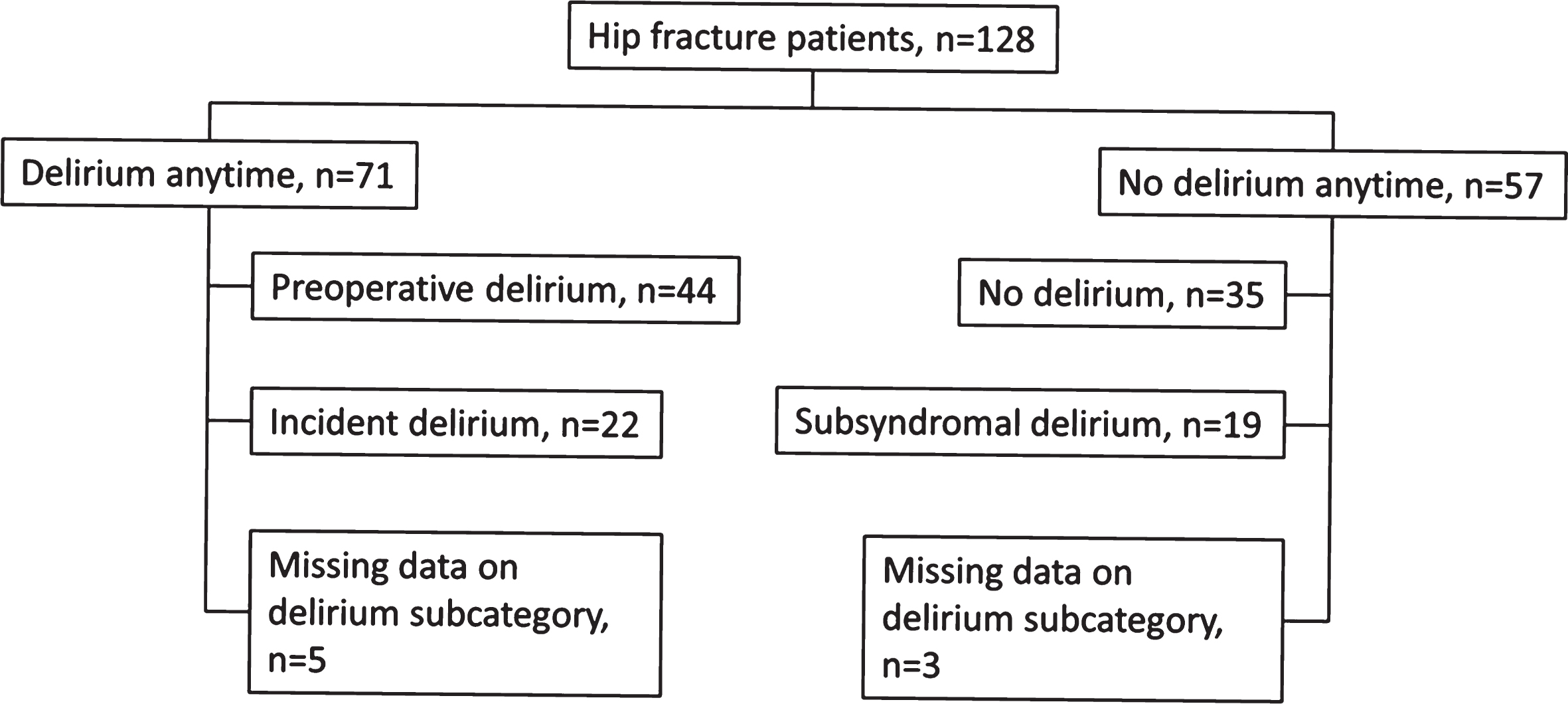
Delirium subcategories.
An experienced geriatrician and an experienced specialist in old age psychiatry independently assessed whether a patient fulfilled the ICD-10 criteria for dementia, based upon all available information except delirium status during hospital stay [26]. In case of disagreement, a consensus diagnosis was made.
The participants were also classified into biomarker groups according to the National Institute on Aging–Alzheimer’s Association (NIA-AA) criteria [27]. According to established cut-offs, the criteria for amyloid positivity (A+) was Aβ42 < 530 pg/mL and for tau positivity (T+) p-tau≥60 pg/mL [28]. T-tau was not used for classification of neurodegeneration (N+), because of a very strong correlation between t-tau and p-tau (ρ= 0.9, p < 0.001).
Cognitively normal participants (control group) were recruited to the COGNORM study from 2012 to 2013 at Oslo University Hospital and Diakonhjemmet Hospital, Oslo [29]. A total of 172 patients, aged 64 years or older, undergoing elective gynecological, orthopedic, or urological surgery in spinal anesthesia, were assessed with a multi-domain battery of cognitive tests prior to surgery and at annual follow-up assessments. Patients were excluded if they had dementia, Parkinson’s disease, previous stroke with sequela, or other acknowledged or suspected brain diseases likely to influence cognition. In the current study we excluded patients without CSF samples (n = 22), suspected undiagnosed dementia with referral to a memory clinic at any time point during 5 years of follow-up (n = 12), or a Mini-Mental State Examination score <28 at baseline (n = 14). All patients were free from delirium at the time of surgery. Delirium was not assessed postoperatively.
CSF sampling and handling
Up to 10 mL of CSF was collected in polypropylene tubules just before injection of the spinal anesthetic in both cohorts. The CSF was centrifuged shortly after collection, and the supernatant was stored in aliquots at –80°C. Samples were sent on dry ice for analyses at the Clinical Neurochemistry Laboratory at Sahlgrenska University Hospital (Mölndal, Sweden). CSF FABP3 concentration was measured on the MSD platform using the Human FABP3 Kit (Meso Scale Discovery, Rockville, MD). CSF Aβ42, p-tau, and total tau (t-tau) concentrations were measured using INNOTEST enzyme-linked immunosorbent assays (Fujirebio, Ghent, Belgium). All measurements were performed by board-certified laboratory technicians who were blinded to the clinical data.
Ethics
The study was conducted in accordance with the Declaration of Helsinki and approved by the Regional Committee for Ethics in Medical Research in Norway (REK 2009/450 and REK 2011/2052). Informed consent was obtained for participants or from substitute decision-makers if participants did not have capacity to consent.
Statistics
Statistical analyses were performed using SPSS Statistics version 25 (IBM Corp., Armonk NY). Figures were drawn in GraphPad prism version 7.02. Categorical data were analyzed using Chi-square tests. Because the distribution of the FABP3 concentrations was skewed, nonparametric statistics were used. Mann-Whitney U-tests were used to compare differences between two independent groups. Stratified analyses were performed according to prefracture dementia, as well as amyloid (Aβ42) and p-tau biomarker groups. Kruskal Wallis tests were used to detect possible subgroup differences. Spearman ρ was used for correlation analyses. In linear regression analyzes, standardized residuals were regarded to sufficiently approach the criteria of normal distribution.
RESULTS
FABP3 (pg/mL) was measured in the CSF of 128 hip fracture patients with and without delirium, and in 124 cognitively normal older adults undergoing elective surgery (Table 1).
Demographics and CSF concentrations of FABP3, Aβ42, and tau-proteins
Values are presented as n (%) or median (interquartile range). CSF, cerebrospinal fluid; FABP3, Fatty Acid Binding Protein 3; Aβ42, amyloid-β 1–42; p-tau, phosphorylated tau; t-tau, total tau. aHip fracture patients with delirium, versus without delirium. bAll hip fracture patients versus cognitively normal controls. ±Consensus in an expert panel. *Amyloid-positive if CSF Aβ42 < 530 pg/mL. **Tau-positive if CSF p-tau≥60 pg/mL.
The hip fracture patients were older than the cognitively normal controls. Hip fracture patients with delirium had a higher median IQCODE score, a higher percentage of dementia, and were older than hip fracture patients without delirium.
Comparison of CSF FABP3 concentration between the hip fracture patients and the cognitively normal controls
Median CSF FABP3 (pg/ml) concentration was higher in hip fracture patients compared with cognitively normal controls (5.7 versus 4.5, p < 0.001 (Table 1 and Fig. 2A).
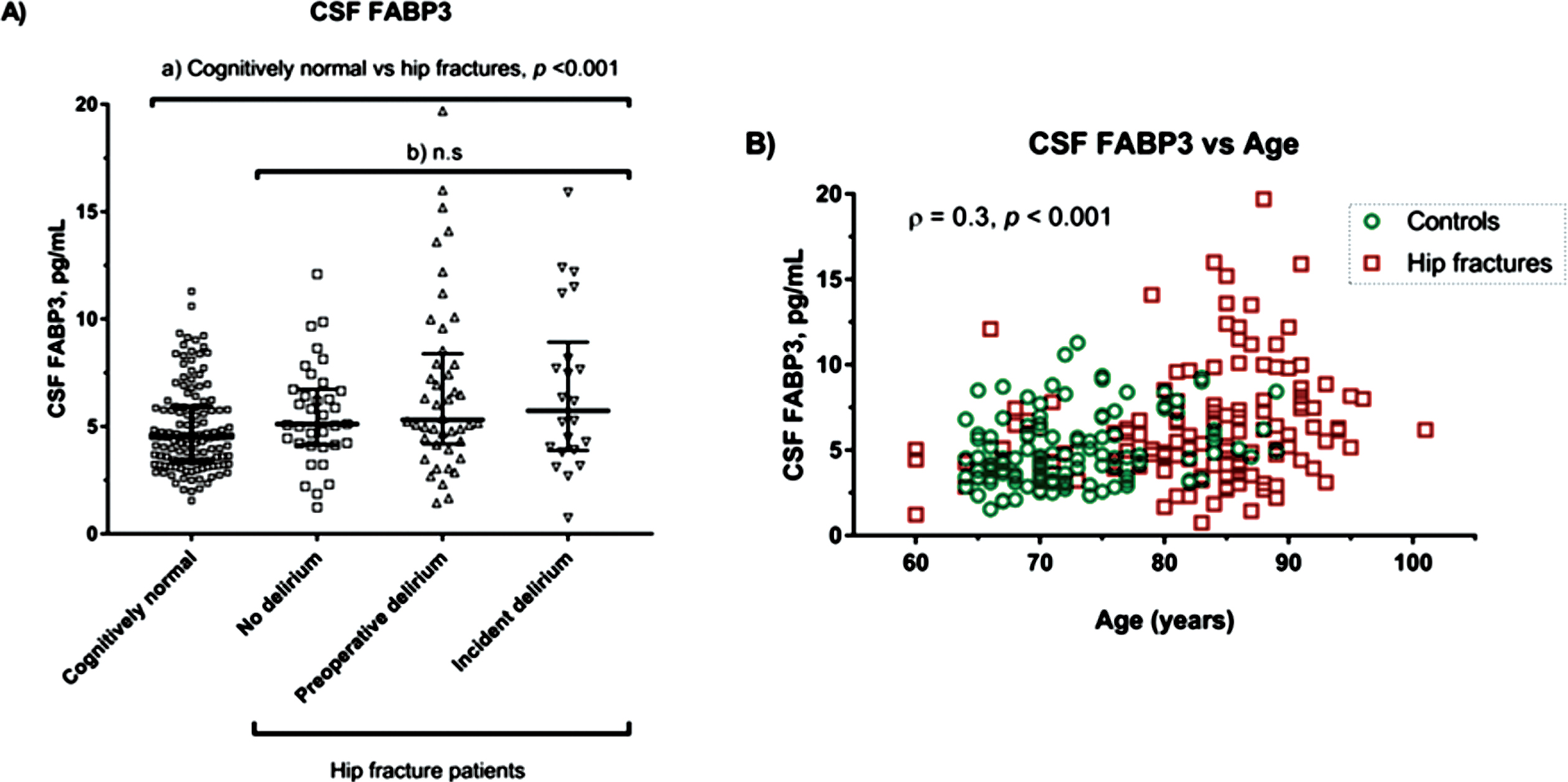
CFS FABP3 concentrations in cognitively normal patients and in hip fracture patients. A) CSF FABP3, according to delirium status in hip fracture patients (no delirium, n = 35; preoperative delirium, n = 44; incident delirium, n = 22) and in cognitively normal patients (n = 124). Participants with subsyndromal delirium (n = 19) were excluded. Data on delirium subcategory were missing for 8 patients. The black lines represent the median and interquartile range. The p values are from the (a) Mann-Whitney U test and (b) Kruskal-Wallis test. B) Relationship between CSF FABP3 concentrations and age. The Spearman’s ρ and p-value are for unadjusted analyses of the combined sample of cognitively normal patients (red squares, n = 124) and hip fracture patients (green circles, n = 128). CSF, cerebrospinal fluid; FABP3, fatty acid-binding protein-3.
There was a significant weak correlation between age and CSF FABP3 in the hip fracture group (ρ= 0.3, p = 0.004), in the group with cognitively normal controls (ρ= 0.2, p = 0.002), and in the combined sample (ρ= 0.3, p < 0.001) (Fig. 2B). After adjustment for age, the association between CSF FABP3 and hip fracture was no longer statistically significant (β= 0.05, p = 0.5).
Comparison of CSF FABP3 concentration across delirium groups, dementia groups, and dementia biomarker groups in the hip fracture cohort
There were no significant differences in median CSF FABP3 (pg/ml) concentration (median (IQR)) between hip fracture patients with (5.4 (4.1–8.2)) and without (5.8 (4.2–7.2)) delirium, or across delirium subgroups (no delirium 5.1 (4.1–6.7), preoperative delirium 5.3 (4.2–8.4), and incident delirium 5.8 (3.9–8.9), Fig. 2A).
There were no significant differences in median CSF FABP3 concentration between patients with and without dementia (consensus diagnosis), 5.5 (4.2–8.4) versus 5.8 (4.1–7.3), respectively.
There was no significant difference in median CSF FABP3 concentration between the amyloid-positive (A+) and amyloid-negative (A–) group (5.3 (3.9–7.7) versus 6.1 (4.6–7.8)). However, CSF FABP3 concentration was significantly higher in the tau-positive (T+) than in the tau-negative (T –) group (7.4 (5.9–10.0) versus 4.7 (3.2–5.9), p < 0.001), and in the A + T+ group (7.4 (5.9–10.6)) compared with all other hip fracture patients (5.0 (3.5–6.3)), p < 0.001.
The hip fracture patients were further stratified according to dementia status, as well as the presence of CSF amyloid or tangle pathology or both. There were no significant differences in CSF FABP3 concentration between patients with and without delirium in either strata (Table 2).
CSF concentrations of FABP3 (pg/mL) in patients with and without delirium, stratified according to dementia status or the presence of amyloid and tau positivity
Values are presented as median (interquartile range). CSF, cerebrospinal fluid; FABP3, fatty acid-binding protein 3. ±Consensus in an expert panel. *Amyloid positive if CSF Aβ42 < 530 pg/mL. **Tau positive if CSF p-tau > 60 pg/mL.
Correlations between CSF FABP3, age, and other biomarkers of neurodegeneration in hip fracture patients
In the hip fracture patients (n = 128), CSF FABP3 concentration correlated positively with all core CSF AD biomarkers Aβ42 (ρ= 0.2, p < 0.01), p-tau (ρ= 0.7, p < 0.01), and t-tau (ρ= 0.7, p < 0.01). These correlations, as well as the correlation between t-tau and p-tau were weaker for higher concentrations of t-tau.
DISCUSSION
This is the first study of CSF FABP3 concentrations in hip fracture patients with and without delirium. The study included a control group of cognitively unimpaired individuals and has three key findings: CSF FABP3 concentration was higher in the hip fracture cohort compared to the cognitively normal control group. This can be explained by correlation between CSF FABP3 and age. There were no significant differences in CSF FABP3 concentration between hip fracture patients with and without delirium, regardless of pre-fracture dementia status, amyloid positivity, tau positivity or both. CSF FABP3 concentration correlated with biomarkers of neurodegeneration and tau pathology, in particular t-tau and p-tau.
CSF FABP3 is considered a general biomarker of neuronal damage, and can reflect both acute and chronic disease [8]. It could thus be a marker of vulnerability for developing delirium, as well as reflecting an acute neuronal damage involved in the pathophysiological process in delirium. We did not find an association between delirium and CSF FABP3 concentration. Thus, our results suggest that the neuronal damage reflected by FABP3 is not directly involved in delirium pathophysiology. On the other hand, the hip fracture patients in our study, both those with and without delirium, may have so extended brain pathology that the abnormalities of biomarkers, including FABP3, have reached a plateau, and thus the between-groups differences are likely to be small. One argument for this is the significant age-related difference in CSF FABP3 concentration between the control group and the hip fracture group.
We found correlations between CSF FABP3 and core biomarkers of AD pathology in the hip fracture group. The fact that the correlations became weaker at higher t-tau concentrations could partly explain why t-tau differed significantly between the groups, while p-tau and FABP3 did not (Table 1). In the cognitively normal control group, CSF FABP3 concentration did not correlate with CSF Aβ42, but correlated positively with CSF p-tau and t-tau. These results have recently been published elsewhere [30]. Previous studies in cognitively unimpaired older individuals found higher CSF FABP3 concentration in Aβ positive individuals (low CSF Aβ), compared to negative individuals (high CSF Aβ) [31]. FABP3 concentration in CSF is also found to be higher in patients with MCI that progresses to AD dementia and in early clinical stages of dementia [14]. CSF FABP3 is therefore suggested to be a potential biomarker for predicting disease progression in early stages of AD and identifying individuals at risk of developing the disease [8, 31]. We found higher CSF FABP3 concentration in patients with biomarker defined AD (A + T+), compared to all other hip fracture patients. Our findings of strong, positive correlations of CSF FABP3 with t-tau and p-tau confirm previous reports in cognitively unimpaired adults [15, 30], as well as in patients with dementia [16, 19] and support FABP3 as a biomarker of neurodegeneration.
It is a strength of this study that we used a reasonably large sample, allowing for subgroup analyses. We included a cognitively normal control group as well as hip fracture patients both with and without dementia in order to present a wide neurodegenerative spectrum. The analyses were performed simultaneously in an expert laboratory. Delirium was assessed bedside daily. It is a limitation that the cognitively normal cohort was significantly younger than the hip fracture patients, and the control group should ideally be age-matched. We cannot rule out that the fracture or muscle damage might have contributed to higher CSF FABP3 concentrations in the hip fracture group. The subgroups are small, reducing statistical power. We did no longitudinal sampling of CSF.
In conclusion, CSF FABP3 concentration in hip fracture patients was higher compared to cognitively normal older adults, indicating ongoing age-related neurodegeneration in these patients. There were no differences of CSF FABP3 concentration across delirium groups, suggesting that the neuronal damage reflected by FABP3 may not be directly involved in delirium pathophysiology.
Footnotes
ACKNOWLEDGMENTS
We would like to thank the patients and staff at the Orthopedic Department, the Gynecology Department, the Urology Department, and the Anesthesiology Department at Oslo University Hospital and the Surgery Department and the Anesthesiology Department at Diakonhjemmet Hospital in Oslo. We also thank the laboratory technicians at the Clinical Neurochemistry Laboratory, Sahlgrenska University Hospital, for skillful technical analyses.
The research was funded by grants through the South-Eastern Norway Regional Health Authorities, the Norwegian Health Association and the Medical Student Research Program in Norway. HZ is a Wallenberg Scholar supported by grants from the Swedish Research Council (#2018-02532), the European Research Council (#681712), and Swedish State Support for Clinical Research (#ALFGBG-720931). KB is supported by the Swedish Research Council (#2017-00915), the Alzheimer Drug Discovery Foundation (ADDF), USA (#RDAPB-201809-2016615), the Swedish Alzheimer Foundation (#AF-742881), Hjärnfonden, Sweden (#FO2017-0243), the Swedish state under the agreement between the Swedish government and the County Councils, the ALF-agreement (#ALFGBG-715986), and European Union Joint Program for Neurodegenerative Disorders (JPND2019-466-236).
The sponsors had no role in the design of the study, subject recruitment, collection, analysis or interpretation of the data, or the preparation of the manuscript.