
Abstract
Background:
Motoric cognitive risk syndrome (MCR) and mild cognitive impairment (MCI) are two pre-dementia stages with an overlap, which may influence the risk for dementia.
Objective:
The study aims to examine the association of MCR, MCI, and their combination with incident dementia in Quebec community-dwelling older adults.
Methods:
1,063 older adults (i.e., ≥65) were selected from a population-based observational cohort study known as the “Nutrition as a determinant of successful aging: The Quebec longitudinal study” (NuAge). Participants were separated into four groups at the baseline assessment: those without MCR and MCI (i.e., cognitively healthy individual; CHI), those with MCR alone, those with MCI alone, and those with MCR plus MCI. Incident dementia was recorded at each annual visit during a 3-year follow-up.
Results:
The prevalence of CHI was 87.2%, MCR 3.0%, MCI 8.8%, and MCR plus MCI 0.9%. The overall incidence of dementia was 2.4% and was significantly associated with MCR alone (Odd Ratio (OR) = 5.00 with 95% Confidence interval (CI) = [1.01;24.59] and p = 0.049), MCI alone (OR = 6.04 with 95% CI = [2.36;15.47] and p≤0.001), and the combination of MCR and MCI (OR = 25.75 with 95% CI = [5.32;124.66] and p≤0.001).
Conclusion:
Combining MCR and MCI increased the risk for incident dementia. These results also demonstrated that this combination is a better predictor of dementia than MCI or MCR alone.
INTRODUCTION
In Canada, over half a million individuals are living with dementia, and this figure is expected to double in the next decade [1, 2]. Screening individuals at risk for dementia and acting on their modifiable risk factors represent an effective strategy to slow down the incidence of dementia [3]. The past two decades have been characterized by an increased interest in identifying and validating biomarkers for detecting early stages of dementia [4–7]. Although biomarkers have greatly contributed to improving the diagnosis of pre-dementia stage, their use may be limited and should be restricted to individuals screened at risk for dementia after appropriate clinical assessments [5–8].
Mild cognitive impairment (MCI) and motoric cognitive risk syndrome (MCR) are two pre-dementia stages [9–15]. MCI is characterized by subjective cognitive complaint with objective impairment in cognitive performance, without interference with daily life autonomy [8, 12]. MCR is characterized by an association of slow waking speed with subjective cognitive complaint [11]. Overlaps between these two clinical syndromes have been reported and, thus, their continuum between normal aging and the first stage of dementia (i.e., mild dementia), is a matter of debate [14]. Recently, it has been suggested that the combination of MCI and MCR is a stage associated with the greatest risk for developing dementia compared to MCR and MCI alone [14]. To test this hypothesis, we used information collected in the “Nutrition as a determinant of successful aging: The Quebec longitudinal study” (NuAge), which is population-based observational cohort study [16]. The aim of this study is to examine the association of MCR, MCI, and their combination, with incident dementia in NuAge participants.
MATERIALS AND METHODS
Study design and population
The NuAge study is a 3-year follow-up observational and prospective cohort study which enrolled Quebec men and women aged 67–84 years, living independently, without cognitive impairment at baseline (defined as a Modified Mini-Mental State (3MS) score > 79/100), without major mobility disability (defined as being able to walk 300 meters and climb 10 stairs without rest), who agreed to commit to 3-years of follow-up and the use of their data [16, 17]. For this study, we excluded participants with missing information at baseline for walking speed, the 3MS score or the use of a walking aid. Participants without 3MS score and items of the Functional Autonomy Measurement System (SMAF) reporting instrumental activities of daily living (IADL) abilities during the follow-up period, and those who withdrew their agreement to use their data were also excluded [18–20]. SMAF is a 29-ltem scale developed according to the WHO classification of disabilities. It measures functional ability in 5 areas: activities of daily living (ADL) [7 Items], mobility [6 Items], communication [3 items], mental functions [5 items], and IADL [8 items]. For each item, the disability is scored on a 5-point scale: 0 (independent), 0.5 (with difficulty), 1 (needs supervision), 2 (needs help), and 3 (dependent). In addition, we excluded participants with MCI and abnormal IADL score (i.e.,≤6/8) at baseline and those who were diagnosed with dementia over the first year of follow-up to prevent misclassification bias of the subgroups of participants (see below). The procedures of recruitment, assessment and follow-up have previously been described in detail [16]. A total of 1,063 (60.6%) participants from the full set of NuAge participants were selected for this study.
Study baseline assessment
At baseline, age, sex, and number of medications taken daily were collected. Polypharmacy was de-fined as≥5 drugs taken daily. Overweight and obesity were defined as body mass index (BMI) ≥25kg/m2. The level of physical activity was quantified using the Physical Activity Scale for Elderly (PASE) [21]. Low physical activity was defined to be below the lowest tertile of PASE score (i.e., < 69.1 for female and < 87.7 for male). Based on the Older Americans Resources and Services Multidimensional Functional Assessment (OARS) questionnaire information, the presence of musculoskeletal diseases was noted [22]. Walking speed was measured over a 4-meter distance. Time was measured between the second and the fourth meter with a stopwatch and the best time of two trials was used.
Definition of participant groups
Cognitively healthy individuals (CHI) were de-fined as participants without MCI or MCR. This group of participants was used as the reference group. Different methods have been used for the diagnosis of MCI using objective cognitive deficits relative to norms in memory or others cognitive domains, as well as in cognitively driven everyday function. We had two variables to make a diagnosis of MCI in the NuAge study: The 3MS score assesses cognitive performance and the IADL score assesses instrumental everyday function. Thus, we followed the Winblad et al. criteria for defining participants with MCI alone: absence of dementia (i.e., 3MS score > 79/100) and impairment of cognitive performance defined as one SD or more below the mean value of 3MS score established in the present cohort (i.e., < 90/100) [12]. Participants with MCR alone were defined according to criteria described by Verghese et al. [13]: a combination of subjective cognitive complaint, defined by the response “yes” for the item “Do you feel you have more problems with memory than most?” of the 30-item GDS, in combination with slow walking speed at baseline assessment as described in a previous publication [23]. The cut-offs for slow gait speeds were: for male < 1.09 m/s for age group 67–72, < 1.00 m/s for age group 73–77, < 0.97 m/s for age group 78–84 and < 0.93 m/s for age group ≥85; and for female < 1.04 m/s for age group 67–72, < 0.97 m/s for age group 73–77, < 0.91 m/s for age group 78–84 and < 0.81 m/s for age group ≥85. The last group of participants were those with a combination of MCI and MCR criteria.
Follow-up assessment
Cognitive status was monitored at each annual visit (T2, T3, and T4) using the 3MS score [20]. From T2 to T4, incident dementia was defined by a combination of abnormal scores of 3MS score (i.e., ≤79/100 as described by Teng & Chui in their publication which showed that 3MS compared to the Mini-Mental State Examination was a more sensitive screening test for dementia) and of IADL score (i.e., ≤6/8) [24].
Standard protocol approvals, registrations, and patient consents
Participants were enrolled in the NuAge study only after obtaining written informed consent for research. The NuAge study was approved by the Research Ethics Boards (REB) of the University Institutes of Geriatrics of Sherbrooke and the “Institut universitaire de gériatrie de Montréal”. The NuAge Database and Biobank were approved by the REB of the Centre Intégré Universitaire de Santé et de Services Sociaux-de-l’Estrie-Centre hospitalier universitaires de Sherbrooke. The present study was approved by the REB of the Jewish General Hospital (Montreal, Quebec, Canada).
Statistics
The participants’ characteristics were summarized using means, SD, frequencies, and percentages, as appropriate. Analysis of variance (ANOVA) with Bonferroni correction or Chi square test were used for group comparisons. Multiple logistic regressions were performed to examine the association of the overall incident dementia (used as dependent variables in separated model) with MCR, MCI, and the combination of MCR with MCI (used as independent variable, all variables in the same model). The reference group of participants for all regressions was CHI. All models were adjusted for the participant’s baseline characteristics. For between group comparisons, threshold of p-value significant was p≤0.001 because of multiple comparisons (n = 42). p-values less than 0.05 were considered as statistically significant for logistic regressions. The NuAge data set used in this study was transferred by the NuAge Database team on May 7, 2019.
RESULTS
The prevalence of CHI was 87.2%, MCR 3.0%, MCI 8.8%, and MCR plus MCI 0.9%. Age differed significantly between groups (p≤0.001), individuals with MCI being older than CHI (p≤0.001) (Table 1). CHI had the highest 3MS score compared to the other groups of participants (p≤0.001). Individuals with CHI had a greater 3 MS score compared to MCR, MCI, and MCI + MCR (p≤0.001), and those with MCR had greater 3MS score than MCI and MCI + MCR (p≤0.001). The lowest prevalence of abnormal IADL score was observed in CHI compared to the other groups of participants (p≤0.001). There was no other significant difference between groups for the baseline characteristics of participants. The overall incidence of dementia was 2.4% (n = 25) and significantly differed between groups (p≤0.001). CHI had the lowest incidence of dementia (p≤0.001) compared to participants with MCR, MCI, or those with both MCI and MCR.
Baseline characteristics of participants grouped according to their motor and cognitive status \centerline (i.e., motoric cognitive risk, mild cognitive impairment and association of motoric cognitive risk and mild cognitive impairment) and the 3-year incident cognitive impairment and dementia (n = 1,063)
MCR, Motoric Cognitive Risk defined as a combination of subjective cognitive complaint with slow walking speed at baseline assessment; MCI, mild cognitive impairment defined as Modified Mini mental Status score one standard deviation (SD) or more below mean values established in the present cohort (i.e., 3MS score < 90/100); SD, standard deviation; 3MS, Modified Mini-Mental State; *Comparison based on analysis of variance or Chi-square test, as appropriate; †Defined as number of therapeutic drugs daily taken ≥5; ‡Body mass index ≥25 kg/m2; ||Score of Physical Activity Scale for Elderly below the lowest tertile (i.e., < 69.1 for female and < 87.7 for male); ¶Based on the Older Americans Resources and Services questionnaire information; §Instrumental activity daily living score≤6/8; **3MS score was ≤79/100 and abnormal (i.e., ≤6/8) instrumental activity daily living score during the 3-year follow-up; Threshold of p-value significant was ≤0.001 because of multiple comparisons (n = 42) indicated in bold.
Logistic regressions showed that the overall incident dementia was significantly associated with MCR alone (Odd Ratio (OR) = 5.00 with 95% Confidence interval (CI) = [1.01;24.59] and p = 0.049), MCI alone (OR = 6.04 with 95% CI = [2.36; 15.37] and p≤0.001), and the combination of MCR and MCI (OR = 25.75 with 95% CI = [5.32; 124.66] and p≤0.001) (Fig. 1).
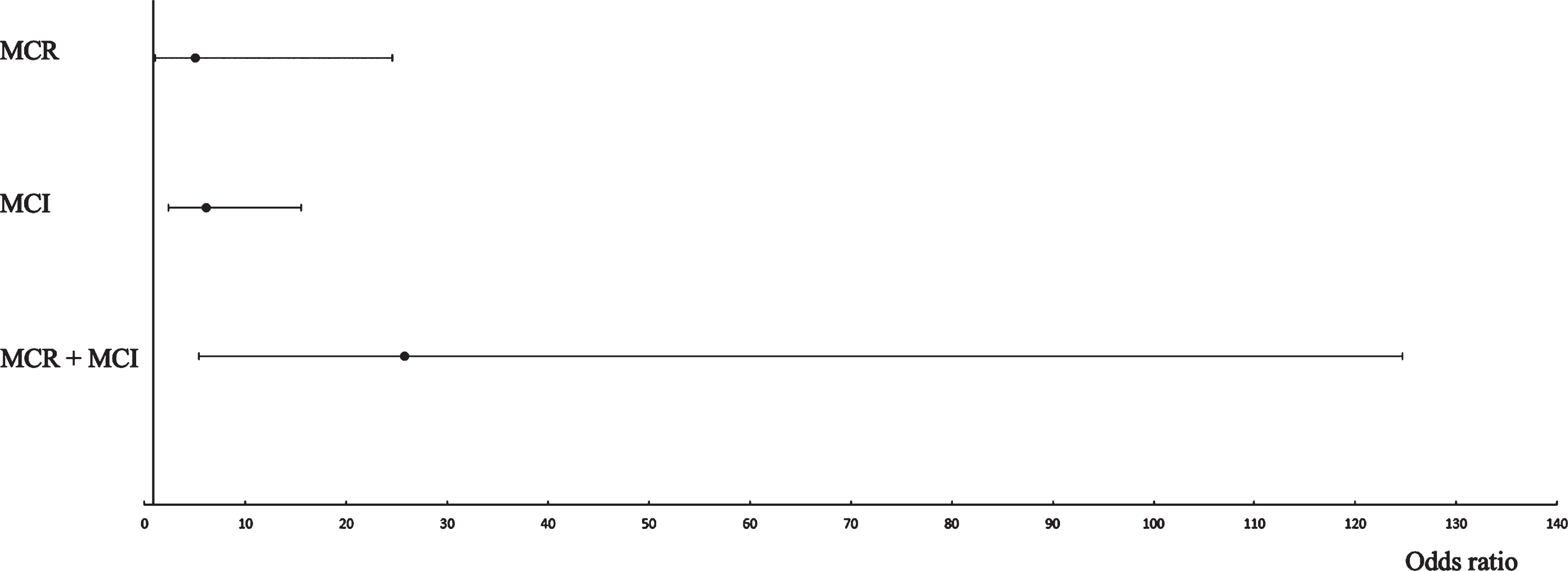
Logistic regressions showing the association of motoric cognitive risk, mild cognitive impairment and the combination of motoric cognitive risk with mild cognitive impairment with the 3-year incident dementia adjusted for participant’s baseline characteristics (n = 1,063). MCR, Motoric Cognitive Risk defined as a combination of subjective cognitive complaint with slow walking speed at baseline assessment; MCI, mild cognitive impairment defined as Modified Mini mental Status score one standard deviation (SD) or more below mean values established in the present cohort (i.e., 3MS score < 90/100); Dementia defined as a 3MS score ≤79/100 and abnormal (i.e., ≤6/8) instrumental activity daily living score over the 3-year follow-up.
DISCUSSION
The findings show that MCR, MCI, and the combination of MCR and MCI were significantly associated with the overall incident dementia. In addition, the highest risk for incident dementia was observed with the combination of MCR and MCI.
The combination of MCR and MCI was associated with the highest risk for incident dementia compared to MCR or MCI alone in our study. To the best of our knowledge, it the first time that this finding is reported. It has been noted that individuals with MCR syndrome are a non-homogenous group in terms of cognitive performance and status. Indeed, they can have normal cognitive performances, amnestic or non-amnestic MCI [14]. In addition, it was observed a higher prevalence of MCI in individuals with MCR compared to those without MCR (47.2% versus 39.5%) [14]. It was also reported that individuals with MCI and MCR had poorer cognitive performance in all domains compared to those with MCI alone and to participants with MCR alone [14]. Thus, it has been suggested that worst cognitive performance in individuals combining MCR and MCI may expose to a greater risk of dementia [14]. Our present finding is consistent with this hypothesis.
The second finding of our study is that MCI and MCR were associated with incident dementia, a greater OR being shown for MCI compared to MCR. MCI is an intermediate stage in the trajectory from normal cognition to dementia and, thus, it is a condition which exposes individuals to a higher risk of dementia compared to be cognitively healthy individuals [24]. The risk for dementia among those with MCI is higher compared to the risk reported in our study [24–26]. One explanation may be related to the low prevalence of MCI at baseline, which was 8.8%. This prevalence is below the range of prevalence of MCI reported in North America (ranged from 9.9% to 35.2%) [27]. The risk for dementia in MCI individuals may vary across different studies with clinical samples showing a higher rate of conversion than community-based samples. That is consistent with our population-based sample of older community dwellers [28]. There is limited data that examined the risk of both MCI and MCR converting to dementia. Only one study explored this risk in individuals with MCI and MCR separately [29]. This study showed that both MCR and MCI were associated with significant incident dementia like our study, the highest risk being reported with MCR Hazard ratio (HR) for MCR = 1.63[1.39; 1.89] versus HR for MCI = 1.36[1.19; 1.1.89] [30]. Our study showed a different result. An explanation may be related to the limitation of this previous study, which did not specify whether individuals with MCR also had MCI [30]. The difference with our study’s findings may also be related to the number of participants and the duration of follow-up. In the Verghese’s study, 4,555 older community-dwellers were recruited from three different prospective and observational cohort studies, which were merged together and followed for a longer period, in comparison to our study. Indeed, the range of follow-up was from 5.1 to 9.3 years, whereas, in this current study only 1,063 individuals were followed over 3 years. In our study, the fact that the association of MCR alone with incident dementia is borderline significant, suggests that objective cognitive impairment as observed in MCI is required to make a stronger link with dementia. This borderline result for MCR may also be explained by the fact that the NuAge population was in relatively good health condition at baseline, contributing to a low incidence of dementia. On the other hand, this good health condition of NuAge participants limited the potential effects of morbidities on the studied association but residual confounding factors are still possible. Another limitation of our study is the strategy used to classify the population in MCI and dementia groups. We used the 3MS test for this classification that may expose to misclassification. Diagnosis of dementia and MCI is usually based on an exhaustive cognitive multidisciplinary assessment. In addition, there is a growing body of evidence that deficits in IADL may be present in individuals with MCI [30]. That is why we made the choice to exclude participants combining MCI status and abnormal IADL score in order to prevent misclassification of NuAge participants in our study.
Our study showed that combining MCR and MCI increased the risk for incident dementia. This result highlights that, within the spectrum of pre-dementia stages, there is stratification of the risk for incident dementia. These results also demonstrated that this combination of MCR and MCI is a better predictor of dementia than MCI and MCR alone.
DATA STATEMENT
Access to NuAge Database can be obtain by contacting the NuAge team via E-mail:
Footnotes
ACKNOWLEDGMENTS
The authors gratefully acknowledge the voluntary participation of all study participants and the NuAge team for its assistance.
The NuAge Study has been funded by the Canadian Institutes of Health Research (CIHR; MOP-62842). The NuAge Database and Biobank are supported by the Fonds de recherche du Québec (FRQ; 2020-VICO-279753), the Quebec Network for Research on Aging funded by the FRQ-Santé and by the Merck-Frosst Chair funded by La Fondation de l’Université de Sherbrooke.
Olivier Beauchet and Gilles Allali were supported by National Institutes on Aging grant number R01 AG057548-01A1.