
Abstract
Epilepsy in frontotemporal dementia is considered to be less frequent than in Alzheimer’s disease. We report two cases of patients with non-convulsive status epilepticus associated with behavioral variant frontotemporal dementia. In the first case, status epilepticus was the first symptom of the disease, and consisted of loss of consciousness and mutism. In the second case, status epilepticus led to a clinical worsening one year after the diagnosis. Our study highlights the importance of suspecting non-convulsive status epilepticus in patients with frontotemporal dementia, and including frontotemporal dementia within the differential diagnosis of new-onset seizures.
INTRODUCTION
The incidence of epilepsy in patients with neurodegenerative disorders is higher than in general population. Alzheimer’s disease (AD) has been associated with an increased risk of epilepsy in multiple research studies [1–4], and the probability of suffering an unprovoked epileptic seizure in AD is estimated at 8–22%, which is 5–10 times greater than in age-adjusted healthy controls [3, 6]. In frontotemporal dementia (FTD), it seems to be lower than in AD [1], although there are not many studies analyzing the presence of epilepsy in patients with FTD. An incidence between 2.2 and 3.0% of epileptic seizures in patients with FTD has been recently reported in the literature, representing a risk between four and six times greater than in the general population [7]. Likewise, the information regarding status epilepticus and its relationship with FTD is also scarce [8].
We present two patients with behavioral variant FTD (bvFTD). In the first, a non-convulsive status epilepticus (NCSE) was the first symptom of the disease, and in the other, NCSE conducted to severe clinical worsening.
CASE 1
A 68-year-old male with personal medical history of essential tremor was admitted to the emergency department with three episodes in the last 24 hours of pallor and loss of consciousness, among which the patient did not recover and associated mutism. In the previous months, he had suffered similar episodes of sweating and malaise, self-limited with full recovery, for which he had not sought advice. Although his vital signs and general examination did not show any remarkable findings, neurological examination showed inattention, confusion, and restlessness. There were no relevant findings on blood tests, ECG (electrocardiogram), and echocardiography. A 24-hour ECG Holter study performed in the first days of admission revealed unexplained episodes of sinus bradycardia. During the following hours in the emergency department, the patient suffered more episodes of loss of consciousness followed by mixed aphasia, while the inattention and confusion progressively increased. A 24-hour video-EEG recording was performed while the patient remained symptomatic. It showed focal persistent slowing, compounded by theta and delta low-voltage activity placed on the left anterior temporal region. Over this background activity, focal seizures were registered, with ictal EEG pattern characterized of high-voltage rhythmic theta activity evolving into rhythmic delta activity located in the left posterior temporal region (Fig. 1A). This clinical picture and EEG findings met criteria for NCSE [9]. Simultaneous ECG showed ictal bradycardia with a heart rate reduction from 80 to 50 beats per minute. He received 5 mg of midazolam and 100 mg of lacosamide during video-EEG recording, with progressive improvement in both the clinical and the EEG pattern. Blood, serology (syphilis and all the herpes virus) did not reveal remarkable findings. Cerebrospinal fluid (CSF) analysis showed mild increase in protein concentration (50 mg/dl, laboratory limits 15–45 mg/dl). A complete immunological study was normal including anti-neuronal nuclear antibodies (ANNA) type 1 (anti-Hu), type 2 (anti-Ri), anti-Yo, anti-CV2/CRMP5, anti-PNMA2, anti-amphiphysin (0 UI/ml all studied with indirect immunofluorescence and confirmed with western blot), and anti-GAD (<5 UI/ml, laboratory limits 0–12.5 UI/ml), studied with immunofluorescence and western blot) in CSF. MRI showed predominantly right-side fronto-temporal atrophy (Fig. 2). At the moment of seizure presentation, the patient did not take any neuroactive drug, including antidepressants, antipsychotics, and cholinomimetics [10].

Above: EEG recordings of Case 1 showing a high-voltage rhythmic theta activity located in the left posterior temporal region. Below: EEG recordings of Case 2 showing low-voltage delta activity placed in the right frontal-central-parietal region which evolves into a high-voltage rhythmic delta activity and lateralized periodic discharges over the right central parietal region.
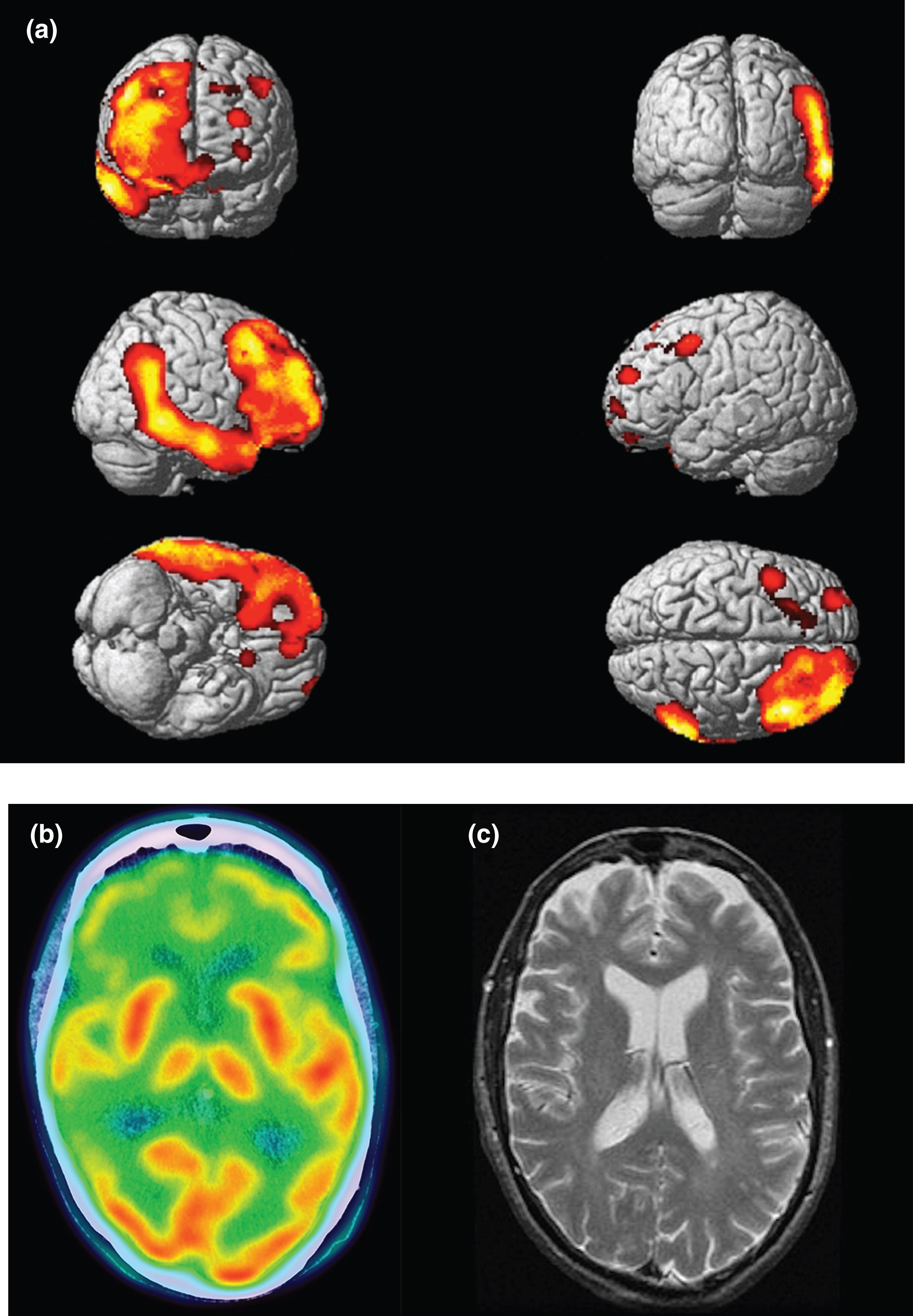
Neuroimaging of Case 1. A) SPM map showing regions of hypometabolism. FDG-PET image of Case 1 was compared with a healthy control group of 40 subjects, using age and sex as covariates. Clusters surviving an uncorrected p-value <0.001 and extent threshold k = 100 voxels are shown. SPM map shows predominant right frontotemporal hypometabolism. B) 18F-FDG PET-CT imaging of Case 1 demonstrating right predominant frontotemporal hypometabolism. C) MRI scan of Case 1 revealing mild frontal atrophy.
The patient was treated with intravenous steroids with no response. Family anamnesis confirmed the absence of previous cognitive or behavioral significant changes. Over the following months he developed progressive word-finding difficulties, and behavioral changes, such as irritability, apathy, and lack of inhibition.
Neuropsychological assessment performed after hospital discharge showed low performance in executive tasks (TMT-B, ratio TMT-B/A), social cognition (Story-Based Empathy Task) [11], language and semantic deficits (semantic verbal fluency, Boston Naming Test), and memory impairment (Free and Cued Selective Reminding Test, Complex memory at Rey-Osterrieth Complex Figure at 3 and 30 minutes). Results of neuropsychological testing are summarized in Table 1 [12]. An 18F-FDG PET-CT revealed right-dominant frontotemporal hypometabolism (Fig. 2). A new MRI performed at 15 months showed an increased in the frontotemporal atrophy.
Main results of neuropsychological testing
FCSRT, Free and Cued Selective Reminding Test; SS, Age- and education-adjusted scaled score (mean 10, standard deviation 3) according to the Neuronorma project [12].
CASE 2
A 75-year-old male was evaluated in our neurology clinic because of changes in social behavior, lack of inhibition, excessive expenses, hyperphagia, and hypersexuality in the last two years. His personal medical history was unremarkable with the exception of an isolated episode of generalized tonic-clonic seizure eleven years earlier. He was treated with valproic acid during 6 years after which the patient discontinued treatment and remained seizure-free for 5 years.
Neuropsychological examination revealed executive dysfunction (TMT-B, Tower of London, and Hayling test) (Table 1) [13]. Laboratory investigations did not show remarkable findings. 18F-FDG PET-CT imaging of the head showing bilateral parieto-temporal and frontal hypometabolism (Fig. 3) and normal values of AD biomarkers in CSF (amyloid-β42: 963 pg/mL; reference range [1058–2594 pg/mL], total tau: 348 pg/mL [146–410], phosphorylated tau: 34.3 pg/mL [21.5–59], and amyloid-β42/amyloid-β40 ratio: 0.118; [0.099–0.168]) led to the diagnosis of bvFTD. CSF analysis was performed in a Lumipulse® G1200 equipment, following the recommendations for handling and storage of samples, and with standardized values to certified reference material in the case of amyloid levels [14]. One year later, the patient sought care at our hospital for episodes of confusion and strange behavior. The day before the patient suffered multiple episodes of unresponsiveness followed by confusion and strange behavior. During his stay in the emergency room, he experienced an episode of unresponsiveness followed by a tonic-clonic seizure, and therefore, treatment with levetiracetam was started. At the moment of seizure presentation, the patient did not take any neuroactive drug.
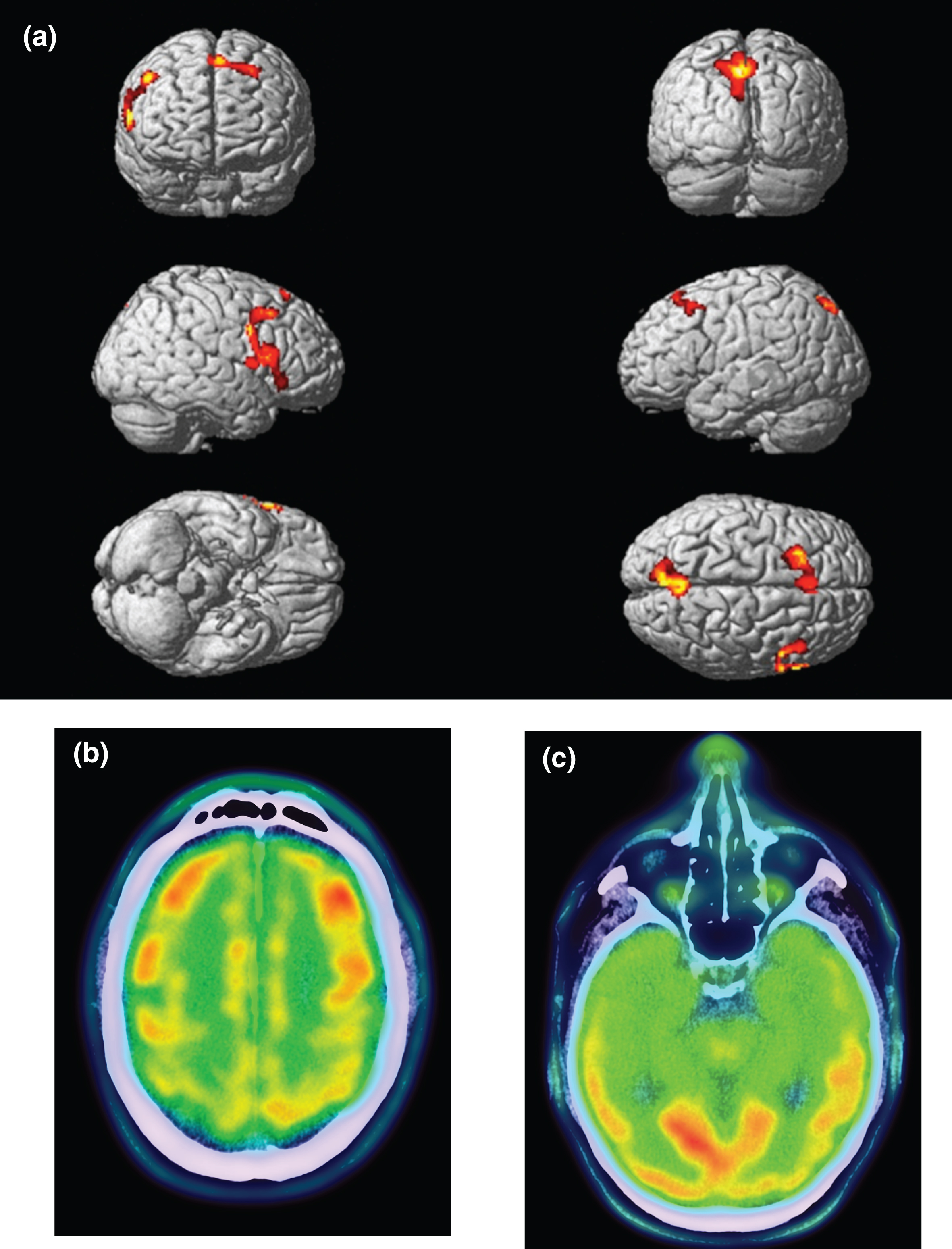
Neuroimaging of Case 2. A) SPM map showing regions of hypometabolism. FDG-PET image of Case 2 was normalized to the MNI space and smooth at 12 mm and then, compared with a healthy control group of 40 subjects, using age and sex as covariates. Clusters surviving an uncorrected p-value <0.001 and extent threshold k = 100 voxels are shown. SPM map shows a bilateral frontal lobe hypometabolism, and in the precuneus. B) 18F-FDG PET-CT imaging of Case 2 displaying also bilateral temporal hypometabolism.
A 24-hour video-EEG recording during hospital admission performed while the patient continued with confusion and inattention showed low-voltage delta activity placed in the right frontal-central-parietal region which evolved into a high-voltage rhythmic delta activity and lateralized periodic discharges at 1–2 Hz over the right central-parietal region (Fig. 1B). This activity stopped abruptly after 20 minutes and was recorded four times. The interictal EEG revealed spikes and sharp waves in both frontal regions. During the video EEG monitoring, the patient was treated with intravenous lacosamide (600 mg) and clonazepam (0.5 mg), and the seizures were controlled returning to baseline status.
DISCUSSION
We present two cases of bvFTD in which NCSE constituted the initial symptom, which led to diagnosis in one case, and a severe worsening in clinical situation in the second one. As NCSE is a reversible situation, and according to our findings, we highlight the importance of an early detection in order to lead to prompt treatment of seizures. In our cases, video EEG monitoring allowed NCSE diagnosis, facilitating treatment and clinical return to baseline status.
The etiopathogenesis of epileptic seizures in patients with dementia is controversial although the most accepted theories point to mechanisms of glutamatergic and gabaergic excitotoxicity produced by the neurodegenerative process [15]. The association of mutation p.P301S MAPT with FTD associated with parkinsonism and epilepsy has been described (FTDP-17) [16], and in a murine model of FTDP-17 an increase in epileptogenic activity and greater sensitivity to GABAa antagonists has been observed [15]. Another explanation could be the use of some neuroactive drugs, which may increase the risk of seizures in some cases, although the risk seems to be low [10].
Cognitive decline in elderly population with neurodegenerative disorders is frequently attributed to the underlying disease. However, acute pathologies, such as NCSE, can produce cognitive fluctuations or worsening in mental status [17, 18], as it occurred in our cases. The incidence of NCSE among patients with altered mental status and dementia is not well established, and the variability of data in the literature is high, estimated at 8–30% depending on the study [17–19]. A recent study has suggested that epilepsy could be more refractory in patients with non-AD dementia [20]. Due to the paucity of information, the relationship between altered mental status and status epilepticus in dementia patients has not been studied so far and the risk of developing epilepsy has not been extensively explored in this group of patients.
Another interesting aspect is the dissociation between right predominant atrophy in Case 1, and the left hemisphere ictal onset at EEG. We may hypothesize that this finding could be explained by some difficulties of the more damaged regions to recruit enough neurons to produce a visible scalp discharge until the propagation to the less damaged hemisphere. This may resemble the situation that occurs in the “burned-out hippocampus syndrome” in hippocampal sclerosis [21, 22]. However, further studies in patients with atypical dementia with asymmetric presentations and epilepsy are necessary to confirm this hypothesis.
In conclusion, although our sample is very small, we want to emphasize the need to consider NCSE in the differential diagnosis of significant clinical worsening of FTD, or even as the first symptom of the disease. In this context, we highlight the importance of performing a video-EEG monitoring to reach prompt detection and treatment of NCSE.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/20-0512r1).