
Abstract
Background:
Non-pharmacological therapies for persons with dementia (PWD) are needed.
Objective:
To develop and test the Paired Preventing Loss of Independence through Exercise (PLIÉ) program, an integrative group movement program for PWD and care partners (CPs).
Methods:
Participants were randomized to immediate or delayed start to Paired PLIÉ in community-based classes (1 hour, 2 days/week, 12 weeks, 3 home visits). Co-primary outcomes included standard measures of cognition, physical function,and quality of life (PWD) and caregiver burden (CPs) assessed by blinded assessors, analyzed using linear mixed models to calculate effect sizes for outcome changes during Paired PLIÉ, controlling for randomization group. Anonymous satisfaction surveys included satisfaction ratings and thematic analysis of open-ended responses.
Results:
Thirty dyads enrolled, 24 (80%) completed. PWD (mean age 80; 55% female) experienced significant improvement in self-rated quality of life (Effect Size+0.23; p = 0.016) when participating in Paired PLIÉ, while CPs experienced a non-significant increase in burden (–0.23, p = 0.079). Changes in physical and cognitive function in PWD were not significant. All CPs returning the satisfaction survey (n = 20) reported being moderately-to-highly satisfied with the program. Thematic analyses identified physical (e.g., sit-to-stand, more energy), emotional (enjoyment), and social benefits (peer-to-peer interaction) for PWD and CPs; challenges were primarily related to getting to the in-person classes.
Conclusion:
Paired PLIÉ is a promising integrative group movement program that warrants further study. It is feasible and may improve self-rated quality of life in PWD. Although CPs may experience increased burden due to logistical challenges, most reported high satisfaction and physical, emotional, and social benefits.
INTRODUCTION
Alzheimer’s disease dementia is a major public health challenge for our century: By the year 2050 the number of people with dementia in the United States is expected to rise from 5.8 to nearly 14 million [1]. Research into pharmaceutical therapies has been disappointing and not provided any medications that can halt the disease trajectory of decline in the cognitive, functional, emotional, and social capabilities of persons with dementia (PWD) [2]. In the absence of disease-altering medications, it is critically important to study non-pharmacological strategies for enhancing quality of life and function in PWD.
For non-pharmacological approaches, multi-domain programs that address several of the declining capabilities in an integrated way have shown the strongest promise for their ability to slow the decline [3]. One such program is the Preventing Loss of Independence through Exercise (PLIÉ) program, a systematically developed integrative group movement program developed for adult day centers [4, 5]. PLIÉ targets abilities and neural mechanisms that are relatively well-preserved in people with Alzheimer’s disease and related dementias. Key elements include building procedural memory [6] for basic activities of daily living (such as transitioning between sitting and standing), improving focus and attention through mindful body awareness, and increasing well-being through social and emotional connection with others. The overall structure of PLIÉ was developed by integrating ‘best practices’ from a wide range of movement modalities including physical therapy, occupational therapy, recreation therapy, dance movement therapy, yoga, tai chi, Feldenkrais, and Rosen Movement. The Guiding Principles, based on these practices, are shown in Table 1. The PLIÉ program has been studied and successfully implemented in adult day centers and has been evaluated with encouraging results using standard dementia outcome measures of function, cognition, and quality of life that allow comparison to pharmacological studies [4, 5].
Guiding Principles of the Preventing Loss of Independence through Exercise (PLIÉ), Paired PLIÉ Themes and Goals
However, there are substantial barriers in the community to enrolling in adult day centers: Most people in the community do not have access to a center in their immediate area, and many perceive enrollment as stigmatizing or cost prohibitive [7]. Only a small minority of PWD enroll in adult day centers, while the majority are cared for by family members in the community or are placed in nursing homes [8–10]. In 2014, we sought to identify unmet needs in PWD and CPs in our community by convening a local stakeholder meeting and performing semi-structured interviews with representatives from senior care facilities, county health officials, caregivers, and home care service representatives. We learned that PWD and CPs wanted access to effective programs that they could do together to maintain functional status and quality of life. Caregivers asked for guidance on how they can employ a home-based exercise program with their family member with dementia. This need was also emphasized by behavioral health providers at Kaiser Permanente Northern California (KPNC), the largest health care system in the region. Consequently, we thought that CPs and PWD living together in the community are functional dyads that may benefit from a paired exercise program.
Few studies have examined paired home exercise programs for PWD. A recent systematic review of 20 studies of dyadic psychosocial interventions [11] included only three studies that utilized exercise as the primary intervention for PWD and only one with truly paired exercise for PWD and their CPs [12, 13]. Another recent review described four additional randomized controlled trials of home visit-based paired exercise interventions for PWD and CPs. However, a limitation of one-on-one home-based interventions is that they do not provide social engagement among peer dyads. Yet, Cochrane reviews of prior studies have found that social engagement improves quality of life and cognitive function in persons with dementia [14, 15].
The objectives of this study were to: 1) develop Paired PLIÉ—an adapted version of the original PLIÉ program that can be practiced in dyads of persons with mild to moderate dementia together with their CPs in a community-based group environment; and 2) test the efficacy of Paired PLIÉ in a mixed-method Phase I clinical trial.
MATERIALS AND METHODS
Development of the Paired PLIÉ intervention
We first convened a daylong internet-based video conference with national experts and exercise instructors from various modalities including physical and occupational therapy, music and dance therapy, and movement practices from integrative health as well as our team of PLIÉ instructors to discuss how we might adapt the original PLIÉ program (which includes only PWDs) to include dyads (PWDs and CPs). Subsequently, the research team and the PLIÉ exercise instructors explored and practiced dyadic and group movements that led to a multimodal interactive program based on implicit procedural learning and using the same general principles as the PLIÉ program (see above) [4, 5]. The final Paired PLIÉ program includes movements performed as a full group (e.g., seated or standing in a circle) as well as dyadic (paired) movements (usually with a family member or paid CP). Movements focus on physical function such as balance, include personalized music choices and singing, support positive affect, and use language to cognitively enhance the experience of mind-body integration [5, 16]. Our aim was to promote a non-judgmental supportive atmosphere to foster a sense of embodied personhood in PWD through joyful and playful social interaction with an empowered CP. We prepared a script for ten Paired PLIÉ Themes taught briefly at the beginning of each class, with each theme designed to roughly correspond to the original PLIÉ Guiding Principles (Table 1). In addition, we developed a protocol for monthly home visits to help integrate the movements that were practiced in class into the dyad’s home environment and to tailor the program to address each dyads’ individual needs.
We conducted two pilot tests of Paired PLIÉ at a regional memory facility (Alzheimer’s Services of the East Bay, ASEB, Oakland, CA) for an iterative refinement process. Based on participant feedback, we adjusted the timing of classes and number of home visits (original PLIÉ: 2 to 3 days/week for 18 weeks; first Paired PLIÉ pilot: 2 days/week over 4 weeks+3 monthly classes, 11 classes total and one home visit; second Paired PLIÉ pilot: 2 days/week over 16 weeks and four home visits; final Paired PLIÉ design: 2 days/week for 12 weeks and three home visits). We created home support materials: a handout brochure with a few core exercises and a 20-minute video to be used with the exercises.
Following several minor modifications and the thorough training of new exercise instructors, we established a cooperation between the University of California San Francisco (UCSF) and the Division of Research of KPNC at its Medical Center in Oakland, which was the site of our clinical trial.
Ethics statement
This trial was approved by the Institutional Review Board (IRB) of the University of California, San Francisco (IRB# 15–17641) and the KPNC IRB (IRB# CN-15-2151) and is registered at ClinicalTrials.gov (pilot trial: NCT02403752; full trial: NCT02729311).
Overview of clinical trial study design
We tested Paired PLIÉ by performing a 12-week randomized controlled trial (Fig. 1) at the Kaiser Permanente Medical Center in Oakland. We enrolled participants in sequential cohorts of 10 dyads (PWD and CPs). These were randomized to either an immediate start intervention group (five dyads receiving Paired PLIÉ) or a delayed start control group (five dyads continuing usual activities that subsequently received the Paired PLIÉ intervention after 12 weeks of being waitlisted). When dyads were participating in the 12-week Paired PLIÉ program, they attended classes for 1 hour, 2 days/week, for 12 weeks and also had 3 monthly visits to provide targeted exercise instruction and better assess participants’ personal goals and interests. The immediate start intervention group participated in the program from weeks 1–12, while the delayed start control group participated in the program from weeks 13 to 24. Standardized assessments were performed in all participants at baseline, 12 and 24 weeks by trained research assistants who were blinded to group assignment. Caregivers in both groups were called monthly to assess for adverse events throughout the study period. An anonymous satisfaction survey with pre-paid return envelope was sent to all caregivers after program completion or withdrawal.
Eligibility and enrollment
Study participants were recruited using a variety of strategies. We gave presentations at local caregiver support groups offered by KPNC in Oakland, and caregivers were invited to contact the study team at UCSF by phone. In addition, we distributed study flyers and brochures to psychiatrists, neurologists, and caregiver support managers at KPNC, gave presentations at Medical Center Grand Rounds for attending physicians, and posted fliers in community settings and on social media (e.g., Facebook).
Participants and caregivers were enrolled as dyads. Inclusion criteria for the PWD were: a diagnosis of dementia of any type of mild to moderate severity (defined as Clinical Dementia Rating [17] of 0.5, 1 or 2 during phone screen); being ambulatory and able to take 2 steps without cane or walker; living in the community in a private home; and English language fluency. Exclusion criteria were behavioral or physical issues that would be disruptive or dangerous to themselves or others (e.g., active psychosis, drug abuse, severe behavioral issues determined by interview); planning to move to a facility before the end of the study period; terminal illness (life expectancy <1 year); non-stable dementia medication dose; or current participation in another research study. Their CPs needed to meet the following inclusion criteria: motivated to participate with PWD; able to answer study questions related to the PWD’s functional status, mood, behaviors, quality of life and their own feelings regarding caregiving; and English language fluency. Exclusion criteria were identical to those for PWD
Sample size calculation
Our sample size of 30 was selected based on effect size estimates from our pilot study of the original PLIÉ program [5], which ranged from 0.34 for physical performance to 0.83 for quality of life. We estimated that a sample size of 30 would provide 80% power to detect an effect size of 0.57 using a repeated measures design with 1 pre and 2 post measures and correlation between measures.
Screening/consent/assent
We contacted the legally authorized representative (LAR) for all potential PWD participants and collected standard demographic and medical history information to assess eligibility. Those who were eligible and interested were scheduled for an in-person consent visit. We assessed the PWD’s capacity to consent for themselves using standard procedures, and if they did not demonstrate capacity to consent, they were asked to provide assent. PWDs and CPs provided outcome data in separate rooms so that their answers did not influence each other.
Randomization
The randomization sequence was created in advance using a random number generator. Randomization was performed in blocks of 10. The randomization sequence was stored separately and securely and was accessible only to the intervention team. Research staff involved with enrollment and assessment were blinded and unaware of the randomization sequence.
Paired PLIÉ intervention
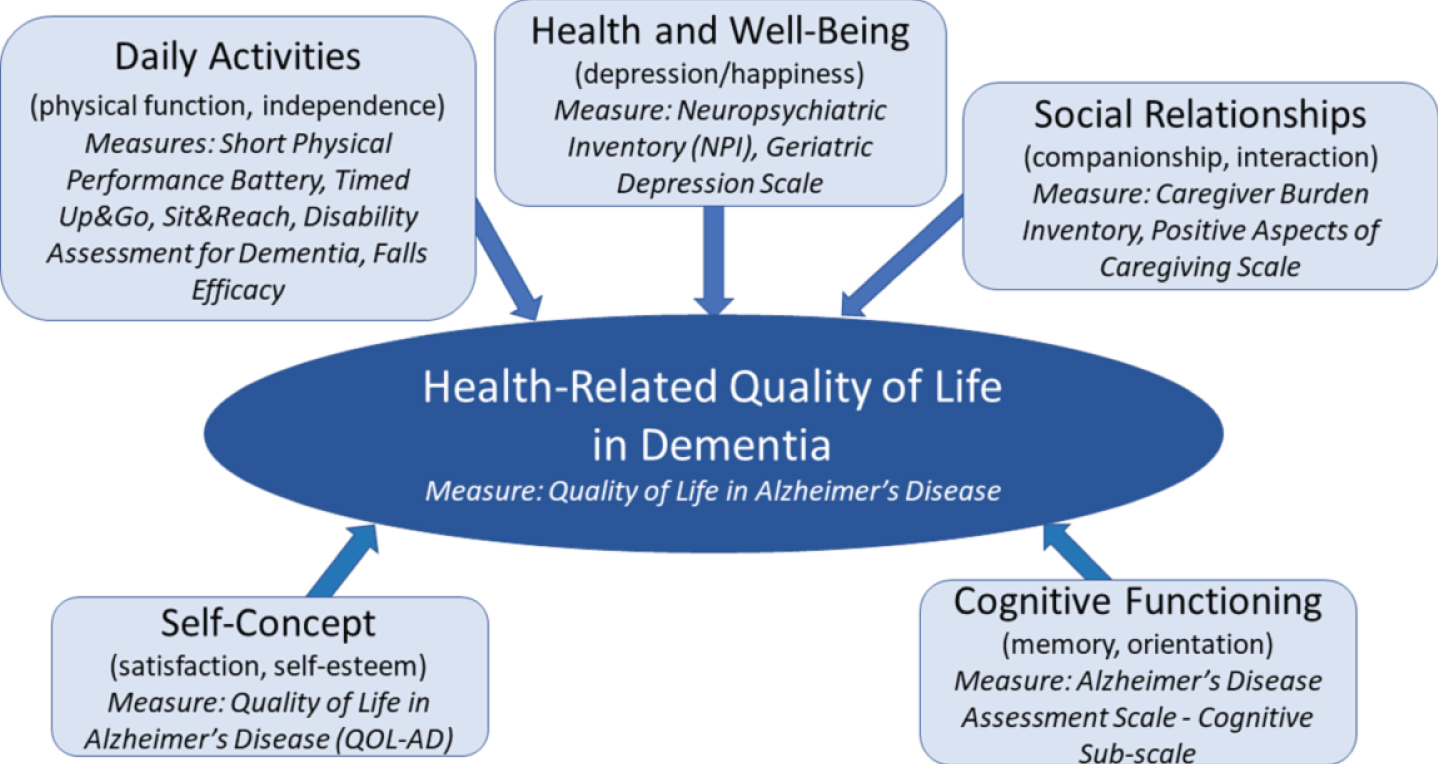
Instructors followed the same Guiding Principles as the original PLIÉ program and also used the Paired PLIÉ Themes to help make these principles memorable for CPs (Table 1) [4, 16]. Consistent with the conceptual framework for health-related quality of life for persons with dementia developed by Smith et al. [18], the Guiding Principles and Class Themes are used to target five key domains: daily activities, health and well-being, social relationships, cognitive functioning, and self-concept (Fig. 1).
Class format
Participants met as a group for 1 hour, 2 days/week for 12 weeks. Each class began with participants seated in a circle and followed a basic class structure that included greetings, body awareness warm-up, and breathing exercises to bring focus to and acceptance of the present moment (cognitive function). After this beginning, which opened every class, a series of progressively more challenging movement sequences were introduced to promote daily function and social connection (e.g., to support smooth transitions between sitting and standing and balancing while standing and walking) (daily activities). All movements are performed slowly and purposefully, so that persons with dementia are able to follow and participate successfully (self-concept). In addition, many movements involve interactions between class participants, such as turning to face one’s neighbor and holding hands in a circle (social relationships). Classes closed with body awareness and breathing exercises and sharing of appreciations (health and well-being). Adherence to the protocol was monitored through class visits by the principal investigator and co-investigators; review of daily class reports; viewing of class videos; logs of the specific exercises taught at each class; and weekly team meetings. CPs were asked to practice these movement exercises with their dyad partners between classes at home. For the home practice we provided a printed booklet and access to online videos.
The first group of dyads to receive the intervention was asked to keep a daily practice log, record weekly reflections, and were provided with a Fitbit to wear during home practice and group classes in order to motivate and monitor home practice. Although we were able to confirm that the Fitbit data highly correlated with the log entries, use of the Fitbit and these daily practice logs were eliminated in subsequent groups because CPs reported that completing them was too burdensome [16].
During an initial phone interview before classes started, exercise instructors made an individual goals assessment and queried CPs and PWD about personally meaningful music, which was incorporated into classes. The exercise instructors were certified and well trained educators for movement practices in yoga, Feldenkrais [26–28], or Rosen method [29]. They were thoroughly trained in the Paired PLIÉ program and in working with individuals with dementia. In addition to the classes, exercise instructors called CPs monthly to ask about potential adverse events and address any logistical issues. The exercise instructors also made three monthly home visits, during which they assisted dyads in applying the movement practice to the individual home environment. These home visits occurred during the 12 weeks of the intervention. In addition, participants received an illustrated brochure with the movement exercises practiced in class to support potential home exercises after the end of the 12-week program.
Measures
Participant demographic information (age, sex, race, education) was determined for both PWD and CPs based on CP report. CPs also were asked about the PWD diagnosis (Alzheimer’s disease, vascular dementia, other/unknown), the number of years they had been providing care, their relationship with the participant (spouse, child, paid, other) and their marital status.
Primary outcome measures
Primary and secondary outcome measures were selected based on our Conceptual Framework (Fig. 1). We had three a priori co-primary outcomes for PWD to reflect the domains of daily activities/physical function, cognitive function and quality of life. A single primary outcome of caregiver distress was specified a priori in CPs.
Physical function (PWD –direct assessment). The Short Physical Performance Battery (SPPB) was developed by the National Institute on Aging to provide an objective tool for measuring physical performance in older adults [30]. It includes direct assessment of lower body strength, balance and gait speed that provide a summary score (range 0–12). Higher scores indicate higher performance ability. Individual components were examined as secondary outcomes (see below).
Cognitive function (PWD –direct assessment). The Alzheimer’s Disease Assessment Scale –cognitive subscale (ADAS-cog) [31] was used to directly assess cognitive function in PWD. It is one of the most commonly used outcome measures in dementia drug treatment trials. It includes direct assessment of learning (10-word list), naming (objects), following commands, constructional praxis (figure copying), ideational praxis (mailing a letter), orientation (person, time, place), recognition memory and remembering test instructions. The ADAS-cog has shown high consistency and test-retest reliability [32]. Higher scores (range 0–70) indicate worse cognitive function.
Quality of life (PWD –self-report). The Quality of Life Scale in Alzheimer’s Disease (QOL-AD) asks PWDs to rate their current quality of life on a 4-point Likert scale (poor, fair, good, excellent) in 13 areas: physical health, energy, mood, living situation, memory, family, marriage, friends, self as a whole, ability to do chores around the house, ability to do things for fun, money, and life as a whole. Internal consistency is excellent with a Cronbach’s alpha coefficient of 0.82 [33]. Higher scores (range 4–52) indicate higher quality of life.
Caregiver burden (CP –self-report). The Caregiver Burden Inventory (CBI) is a standard 24-item measure that includes questions about the CPs feelings about caregiving on a 5-point Likert scale with 5 domains. This measure has good internal consistency [34]. Higher scores (range 0–96) indicate higher burden.
Secondary outcome measures
We included a wide range of secondary outcome measures that were considered exploratory and hypothesis-generating to inform future studies.
Balance (PWD –direct assessment). Balance was assessed as part of the SPPB based on ability to stand with feet side-by-side together, in semi-tandem or tandem stance (range: ordinal variable 0–4). Higher scores indicate better performance.
Chair stand (PWD –direct assessment]). Lower body strength was assessed as part of the SPPB based on the time to stand up from a chair five times without using arms (range: ordinal variable 0–4). Higher scores indicate better performance.
Usual gait speed (PWD –direct assessment). Gait speed was assessed as part of the SPPB based on 3 meter walk (time in seconds) [35]. Higher scores indicate worse (slower) performance.
8-foot Timed Up & Go (TUG) (PWD –direct assessment). TUG assessed mobility based on the time to get up from a chair, walk 8 feet around a cone and return to sit back down (time in seconds). Higher scores indicate worse (slower) performance.
Flexibility (PWD –direct assessment). Flexibility was assessed using the Sit & Reach test, which involves reaching toward the toes of one leg with knee extended while sitting (inches) [36]. Higher scores indicate better performance.
Falls efficacy (PWD –self- and CP-report). We administered a modified version of the Falls Efficacy Scale (FES) to assess concern about falling for the PWD in 10 different scenarios. Response categories used a 4-point Likert scale (range: 10 to 40), with higher scores indicating greater concern about falling (i.e., lower efficacy). Although the FES has been validated in individuals with cognitive impairment [37], the questionnaire was administered separately to PWD and CPs to obtain their independent perspectives.
Behaviors (PWD –CP-report): The Neuropsychiatric Inventory (NPI) was administered to assess the number (NPI-N), frequency/severity (NPI-FS), and level of caregiver distress (NPI-CD) caused by 12 common dementia-related behaviors (delusions, hallucinations, agitation/aggression, depression/dysphoria, anxiety, elation/euphoria, apathy/indifference, disinhibition, irritability/lability, aberrant motor behavior, sleep, and appetite/eating) by CP report and has good test-retest reliability and internal consistency [38]. NPI-N scores range from 0–12. NPI-FS was calculated by multiplying the frequency*severity of behaviors, which had a range of 0–144. Finally, NPI-CD range from 0–60. Higher scores indicate worse outcomes (i.e., more behaviors, greater frequency/severity and greater distress).
Independence (PWD –CP report). The Disability Assessment for Dementia (DAD) [39] is a standard measure that asks CPs to rate the participant’s disability with 17 basic and 23 instrumental activities of daily living over the past 2 weeks. The DAD has high established validity and high test-retest reliability, inter-rater reliability, and internal consistency. Scores represent the percentage of activities performed independently during the past two weeks of those applicable (total number of questions answered yes/total questions applicable)*100 with the range from 0 to 100. Higher scores indicate greater independence.
Quality of life (PWD –CP-report). The Quality of Life Scale in Alzheimer’s Disease (QOL-AD) also asks CPs to rate the PWD current quality of life on the same scale as the PWD QOL self-report (see above).
Caregiving (CP –self-report). The Positive Aspects of Caregiving (PAC) scale includes 9 questions about the benefits of caregiving noticed by the CPs about themselves, which are rated on a 5-point Likert scale. This measure has high internal consistency [40] and can improve with CP training interventions [41]. Total scores range from 11 to 55 with higher scores indicating more positive feelings.
Mood (PWD and CP –self-report). The Geriatric Depression Scale (GDS) is a standard measure that includes 15 yes/no questions assessing depressive symptomatology over the past week. PWD and CP answered separately regarding their own mood. This scale ranges from 0 to 15 and has been validated in people with and without cognitive impairment [42]. Higher scores indicate more depressive symptoms.
Other outcomes
We also assessed both adverse events and adherence to the intervention. Specifically, we assessed adverse events by asking caregivers to report any adverse events on a monthly basis. We assessed adherence by class attendance logs completed after each class by instructors.
The Montreal Cognitive Assessment (MoCA) [43] was only assessed at baseline to further characterize our study sample. It is a 30-point performance test assessing visuospatial abilities, multiple aspects of executive functions, attention, concentration, working memory, language and orientation to time and place. Scores of 25 or below indicates cognitive impairment.
Satisfaction survey
An anonymous satisfaction survey was sent by mail to all CPs after study completion or withdrawal with a pre-paid return envelope. The survey asked CPs to rate their satisfaction with all study components (enrollment and assessment: consent visit, baseline assessment, mid-point assessment, final assessment; intervention: initial goals assessment, weekly classes, monthly check-in calls, home visits) and overall on a 5-point Likert scale (highly satisfied, moderately satisfied, neutral, moderately unsatisfied, highly unsatisfied). They also were asked how likely they were to recommend the program to others on a 0 to 10 scale, with 0 being ‘not at all likely’ and 10 being ‘highly likely.’ In addition, five open-ended questions were asked to assess the qualitative effects of the program, challenges and suggestions for improvements. The questions were: 1) What changes did you notice in your loved one when they were participating in our program? 2) What changes did you notice in yourself when you were participating in our program? 3) What did you enjoy the most about the study? 4) What did you find most difficult about your participation in the study? 5) Do you have any other comments or suggestions for us?
Analyses
Characteristics of the immediate and delayed start groups were compared using t-tests for continuous variables and Chi-square tests for categorical variables. Means were calculated for all continuous outcome measures at each time point by group (immediate versus delayed start). Linear mixed models were used to examine changes in outcome measures between groups and over time. This analytic approach enables inclusion of all study participants regardless of their completion status (intent-to-treat) while also accounting for baseline differences between the groups and correlation between repeated measures over time. Three model specifications were explored. First, we performed traditional linear mixed models and tested for overall group-by-time differences with time modeled as categorical to allow for non-linearity of change over time. However, this modeling approach does not take into account the effect of the intervention in the waitlist group. Therefore, to capitalize on the waitlist design in which all study participants ultimately received the intervention, we examined time as a binary variable that indicated whether a participant had received or not received the intervention at a given assessment visit. Thus, in the immediate start group, time was classified as 0 at baseline and 1 at the 12-week assessment, so that a 1-unit change reflected change during Paired PLIÉ controlling for baseline values. We considered two alternative specifications of time for the 24-week assessment in the immediate start group to reflect either a persistent effect (time = 1) or return to baseline (time = 0) and selected the best-fitting model for each outcome variable based on the lowest Akaike Information Criterion (AIC) value [44]. In the delayed start group, time was modeled as 0 for the baseline and 12-week assessments and 1 for the 24-week assessment, so that a 1-unit change reflected change during Paired PLIÉ compared to baseline and midpoint values. Finally, we used the best fitting model to estimate standardized effect sizes using the marginal estimated mean change during Paired PLIÉ (i.e., change from time = 0 to time = 1 combining data from the two groups) divided by the baseline standard deviation. Signs were reversed for measures in which lower scores reflect better outcomes, so that positive effect size values indicate improvement during Paired PLIÉ and negative values reflect decline. p≤0.05 was considered statistically significant for all analyses of prespecified primary outcomes. We decided a priori not to adjust for multiple comparisons for our three co-primary outcomes in PWD to minimize the risk of Type II error given our relatively small sample size and because we believe that all three reflect clinically meaningful outcomes [45]. We defined effect sizes of 0.20 SDs or greater as ‘clinically meaningful’ based on prior studies of effect sizes for current dementia medications [46]. Results with effect sizes ≥0.20 but p > 0.05 are described as ‘non-significant’ changes. Results with effect sizes <0.20 and p > 0.05 are described as no evidence of clinically meaningful change. We also performed a sensitivity analysis repeating the analyses described above but restricting to the first two time points (i.e., change from baseline to 12 weeks in the immediate and delayed start groups).
For anonymous satisfaction surveys, we report mean (SD) values for satisfaction ratings. We employed applied thematic analysis of the free written responses in the surveys. Applied thematic analysis is an inductive and analytical methodology used to develop a theory of the phenomenon being studied [47]. Applied thematic analysis allows core problems and processes to emerge from the analysis, as opposed to applying external concepts to the data [47]. We began with the overarching domains identified in our prior studies PLIÉ, which included physical, cognitive, and social/emotional function [5, 16]. The themes were then refined in an iterative process that allowed for continual modification to best explain the meaning of the data. Two members of the research team (TS, WM) independently coded the transcribed responses. Codes were compared and differences were discussed among three team members (TS, WM, DB) until consensus was reached.
RESULTS
From May 5, 2016 to June 30, 2018, we screened 92 dyads over the phone. Reasons for exclusion (n = 62) were not meeting inclusion criteria (n = 14), declining to participate (e.g., due to inconvenient timing for working CPs and transportation challenges; n = 47; and one “other” reason) (see flow diagram Fig. 1). Thirty eligible dyads (30 PWD and 30 CPs) were enrolled and randomly assigned to immediate start (n = 15) or delayed start (n = 15). One dyad in the immediate start group dropped out before classes began because of declining health, resulting in 29 dyads and a total of 58 participants. Classes were held in waves that started August 23, 2016 and were completed June 7, 2018. Of the 14 dyads in the immediate start group, two withdrew during the intervention period (lack of time, n = 1; unspecified personal reasons, n = 1) and 12 completed the intervention and the 12-week (mid-point) assessment. Two additional dyads withdrew during the follow-up period (death, n = 1; unspecified personal reasons, n = 1), and 10 completed the 24-week (final) assessment. Of the 15 dyads in the delayed start group, one withdrew due to moving to a care facility because of declining health, and 14 completed both the 12- and 24-week assessments and the intervention. There were no statistically significant differences between those who withdrew from the study and those who completed, although power was somewhat limited to detect differences due to the relatively small number of withdrawals (n = 5, 17%).
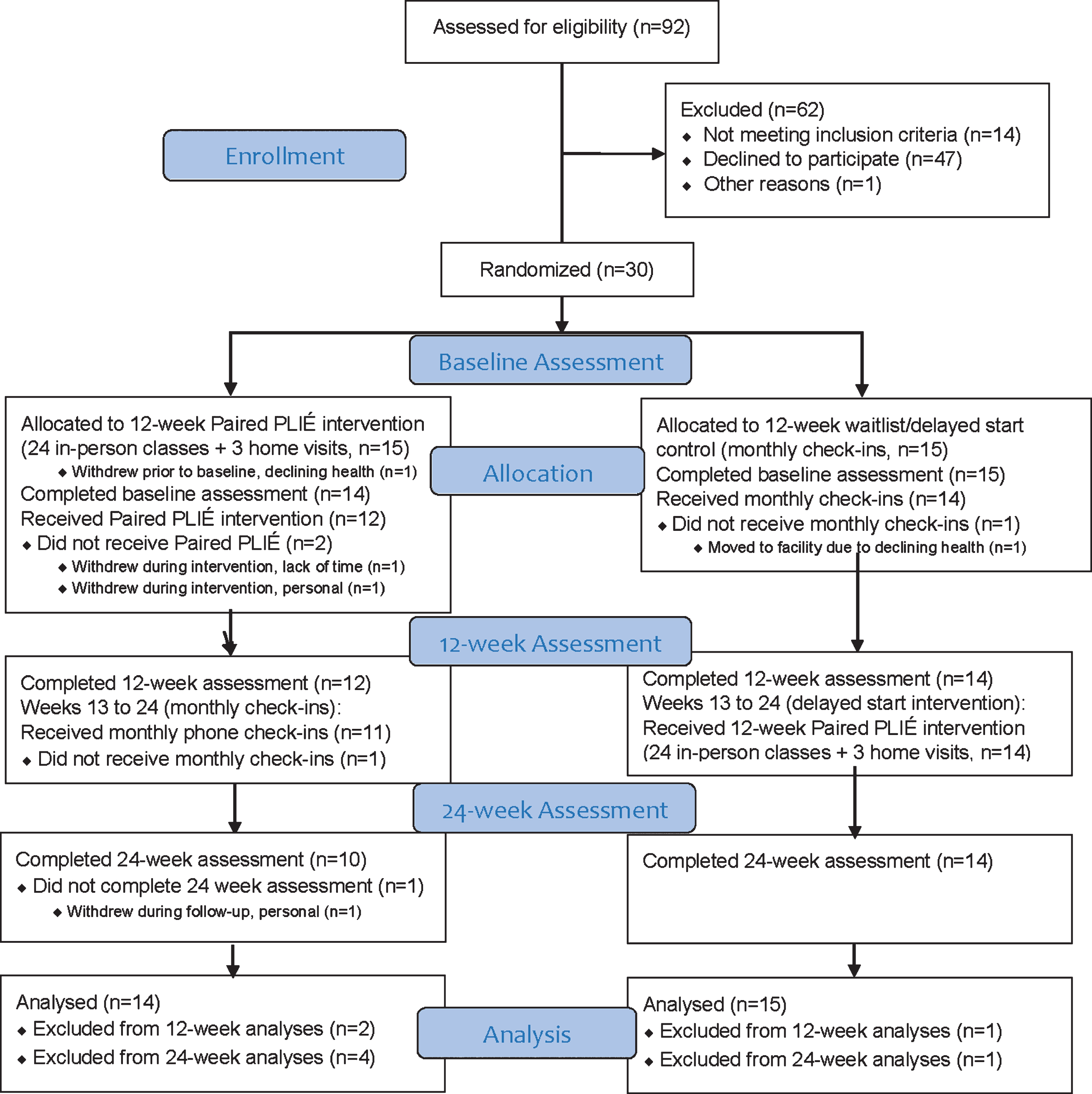
Flow Diagram.
Overall, the PWDs were predominantly white (n = 22, 73%) with slightly more females PWD (n = 16, 53%) than males. The PWD were approximately 80 years old (SD = 6.18) on average and attained slightly more than a college education on average (M years = 16.47, SD = 3.65). The CPs were also predominantly white (n = 18, 60%), mostly female (n = 21, 70%), and also attained slightly more than a college education on average (M years = 16.87, SD = 2.93), and were approximately 66 years old (SD = 15.13) on average. Dementia severity based on the Clinical Dementia Rating global score was similar between groups and was rated as 11 questionable, 13 mild, and 6 moderate, and the mean MoCA score was 13.6 (SD = 6.3). CPs were spouses/partners (n = 18), daughters/sons (n = 8) and others/paid (n = 4). Baseline demographic characteristics were similar between both groups except both PWD and CPs were older in the immediate start group (see Table 2).
Participant Characteristics
Means (SD) for continuous variables, and n for categorical variables. *p<0.05 by independent samples t-tests for continuous variables and χ2 for categorical variables
Each group had 24 classes, except one group 1 that had 23 classes due to a break over holidays. Excluding participants who withdrew during the intervention for reasons noted above, 9 of 12 dyads in the immediate start group and 10 of 14 dyads in the delayed start group attended at least 18 (75%) of the 24 classes; almost all dyads, 11 immediate start and 14 delayed start dyads, attended at least 12 (50%) of the 24 classes. The most common reasons for missing classes were doctor visits, non-study-related injuries, respiratory infections during the winter season, a gout attack, heart problems, travel (e.g., for a child’s wedding or planned vacation), and CPs’ difficulties with the schedule or transportation.
Unadjusted mean scores at baseline, 12-weeks, and 24-weeks for both groups are shown in Table 3 for primary outcomes and in Table 4 for secondary outcomes. Baseline values were similar between groups with some exceptions: delayed start CPs reported higher levels of current depressive symptomatology (M = 2.9, SD = 2.3) than those in the intervention group (M = 1.2, SD = 1.5) at baseline (t = 2.4, p = 0.02, d = 0.89). Also mean scores for caregiver burden (CBI) and dementia-related behaviors (NPI) at baseline appeared to be slightly worse in the delayed start group (although this did not reach statistical significance; see Tables 3 and 4, respectively).
Change in Primary Outcomes and Standardized Effect Size Estimates
ADAS-cog, Alzheimer’s Disease Assessment Scale—cognitive subscale; QOL-AD, CBI, Caregiver Burden Inventory; Quality of Life in Alzheimer’s Disease; SPPB, Short Physical Performance Battery; ahigher scores better; blower scores better Difference and effect size estimates calculated using the marginal estimate of mean change from the linear mixed model with the best fit (lowest AIC). +values indicate improvement during Paired PLIÉ and –values indicate decline. Bolded effect size was statistically significant (p = 0.016).
Change in Secondary Outcomes and Standardized Effect Size Estimates
CP, care partner; DAD, Disability Assessment for Dementia; FES, Falls Efficacy Scale; GDS, Geriatric Depression Scale; NPI, Neuropsychiatric Inventory (-N: number; - FS, frequency severity score; -CD, caregiver distress score); PAC, Positive Aspects of Caregiving Scale; PWD, person with dementia; QOL-AD, Quality of Life in Alzheimer’s Disease; SFT, Senior Fitness Test; SPPB, Short Physical Performance Battery; TUG, Timed Up & Go. ahigher scores better; blower scores better. Difference and effect size estimates calculated using the marginal estimate of mean change from the linear mixed model with the best fit (lowest AIC). +values indicate improvement during Paired PLIÉ and –values indicate decline.
We documented 19 adverse events during study enrollment. These were mostly mild events, including six unprovoked falls. None of the adverse events were study-related.
Traditional linear mixed model analyses suggested no significant group-by-time differences for any of our primary or secondary outcomes. However, because this analytic approach does not account for the waitlist design, we focused our analyses on examining change during Paired PLIÉ (combining both immediate and delayed start groups). For our primary outcomes, we found statistically significant and clinically meaningful improvement in participant self-rated quality of life (ES, 0.23; p = 0.016); no evidence of clinically meaningful change in physical performance (ES, –0.07; p = 0.512) or cognitive function (ES, –0.14; p = 0.0754); and non-significant worsening of caregiver burden (ES, –0.23; p = 0.079).
For exploratory analyses of secondary outcomes, analyses of change during Paired PLIÉ suggested a trend for improvement in mobility (8-foot Timed Up & Go; ES, 0.27; p = 0.10) that did not reach statistical significance. In addition, we found non-significant worsening of flexibility (ES, –0.25; p = 0.154), PWD reported significantly more concern about falling (ES, –0.45, p = 0.009), and CPs reported a non-significant decline in quality of life for PWDs (ES, -0.27; p = 0.133). All other changes were not statistically significant and unlikely to be clinically meaningful. Results were similar in sensitivity analyses restricted to the first 12 weeks of the study (see Supplementary Tables).
Anonymous satisfaction surveys
Twenty (60%) CPs returned the anonymous satisfaction survey. Quantitative survey results are shown in Table 5. All respondents were satisfied with the study overall (78% highly, 22% moderately). Mean ratings ranged from 4.3 to 4.8 on a 5-point Likert scale for specific study components, with an overall study rating of 4.8. CPs also indicated a high likelihood of recommending the program to others (mean 9.2, SD = 1.4, 0 to 10 Likert scale).
Anonymous Satisfaction Survey Results
Thematic analysis of CP’s open-ended responses revealed themes in several key domains: 1) physical functioning, 2) cognition, 3) emotional functioning, 4) social functioning, and 5) issues regarding study logistics. These were further classified based on whether they were referring to the PWD or the CP.
CP reporting about PWD
Physical functioning
CPs made statements about the PWD balance, mobility, and physical strength, but also other aspects of physical health such as energy, activity, and exercise. Several CPs mentioned that their dyad partners’ learned some basic techniques they had practiced in class and were able to apply at home, such as getting up from a chair, car seat, or toilet (n = 5). Even when balance deteriorated (n = 1), CPs perceived their partners as more active and energized (n = 5), and they expressed witnessing improvements in PWDs bodily awareness (n = 4). “[my mother, with whom I participated in the Paired PLIE program] started incorporating many of the movements that we practiced. She uses some of them when getting up out of a chair or off of the toilet. She also taps her feet and moves her hands when listening to music, and occasionally dances, to the extent that she is able.” (CP #8)
Emotional functioning
Many CPs reported that PWDs enjoyed and looked forward to the classes and appeared happy (n = 6). “[He] like[d] the activity, not really realizing he was exercising.” (CP #19)
Social functioning
There were consistently strong statements reported by the CPs regarding the positive experience of social interactions within the group of PWD (n = 4) and with exercise instructors among PWD (n = 1). “He loved the social interaction with others.” (CP #19)“Enjoyed going. Participated in activities. Engaged with participants and leaders.” (CP #12)
Cognitive functioning
Only one of the CPs reported an observation regarding changes in their partners’ cognition (e.g., focus, attention, memory, etc.), which was that the exercises supported the PWD’s ability to focus and maintain attention.
“My loved one is almost always difficult to handle but the exercise took the tension down and created a focus.” (CP #10)
Although most CPs reported observing some physical, emotional, social, or cognitive changes in their loved ones, three reported no changes in PWD (See Supplementary Table 3 for additional quotes of CPs reporting on PWDs).
CPs reporting about themselves
Physical functioning
Changes the CPs observed for themselves in physical functioning included techniques, such as getting up from a seated position more efficiently (n = 2), consistent practicing of some of the exercises at home (n = 2), feeling more energized (n = 2), and one CP stated that she became more aware of her body.
“I enjoyed the class. I use the exercises every day. The trainers were the best. Thankful ... ... ” (CP #10)
“I have learned some techniques for getting out of chairs more efficiently.” (CP #8)
They appreciated the slow movements but also expressed boredom from these activities. “Small movements great for them, but sometimes too slow (boring) for me.” (CP #18)
Emotional functioning
CPs made numerous statements about their own emotional functioning, using words representing emotions (e.g., happy, glad) and/or psychological topics such as coping (n = 4), relaxation (n = 3), and acceptance (n = 1). Several CPs reported that they became less stressed and more patient with their partners and stated that they enjoyed joint activities with their partner and others (n = 6).
“I enjoyed spending time with my mom doing something that gave her great pleasure.” (CP #2)
“Assurance that my husband’s illness & our relationship was not unique.” (CP #6)
However, it clearly was not easy for every CP to have patience with their PWD partner. “I was totally surprised and caught off guard by how difficult and challenging this process was for me.” (CP #9)
Social functioning
Many positive statements about CPs social functioning were made including interactions within the dyads (n = 5), with other CPs (n = 9) and PWD (n = 8), and with the exercise instructors (n = 3). When asked what they enjoyed the most, for most it was the social interaction. “The group aspect. We built a real community in a short period of time.” (CP #10) “I enjoyed meeting & having fun with others with dementia & their caregivers.” (CP #2) “It was good to have an activity we could do together.” (CP #17)
However, there was also a statement that one relatively shy CP did initially have some difficulty:
“I am not a very outgoing person and it took some effort to get over the initial barrier to opening up, and to participating in some of the activities that seemed goofy and fun, but required suspending a certain amount of shyness.” (CP #8)
(See SupplementaryTable 4 for additional quotes of CPs reporting about themselves)
Logistics and overall study views by CPs
Another topic that came up frequently in the satisfaction surveys with CPs was around the logistics, statements mentioning logistical challenges, such as time commitment, distance and travel, and issues with research procedures or dynamics within the dyad. For several CPs it was difficult to get the PWD motivated to leave the house for the class (n = 2). Transportation issues, the distance to drive to classes, and finding parking were frequently mentioned challenges (n = 6). The time commitment was another challenge (n = 4).
“Mostly getting there could be tough. But once you are there, it is great.” (CP #10)
However, overall CPs were very pleased with the study and voiced their gratitude about the overall study and its facilitators (See SupplementaryTable 5 for additional quotes from CPs about logistics and overall study views).
“Thank you for this study. I still feel I can do more than before we began the study & for that I’m grateful.” (CP #7)
“Great movement teacher < name> . Loved the paired dancing.” (CP #18)
DISCUSSION
The present study reports findings from a randomized controlled study of Paired PLIÉ, a novel integrative group movement program that can be practiced in dyads of persons with mild to moderate dementia together with their care partners. Paired PLIÉ was adapted from the Preventing Loss of Independence through Exercise (PLIÉ) program [4, 16], which was originally developed for people in adult day facilities, for use at home, or in a community-based setting. This is one of the first randomized controlled studies of a community-based, multimodal, group exercise intervention for both PWD and CPs.
Our quantitative results suggest statistically significant and clinically meaningful improvement in self-rated quality of life for PWD, which was one of three pre-specified primary outcome measures. This is important because quality of life is often identified as the most important outcome for PWD and CPs [48], and current dementia medications and most non-pharmacologic programs show at best questionable effects on quality of life [49–51]. This result is supported and further explained by qualitative statements made by the CPs that indicated notable satisfaction with physical, emotional, and especially social aspects of the Paired PLIÉ intervention for both the PWD and for the CPs themselves. These encouraging findings are in line with our previous studies [4, 16] and a prior dyadic exercise study for PWD and their CPs [12]. This suggests that Paired PLIÉ could potentially be combined with medications or other programs to maximize benefits across multiple outcome domains.
However, the other two co-primary outcomes in PWD suggested no meaningful change. These quantitative results are markedly different from our small pilot study with PWD (without CPs) in day care [6], in which we observed larger, positive effect sizes for all of these outcomes. The most likely explanation for this difference is the smaller ‘dose’ of the intervention in the current study compared to the pilot study: the original PLIÉ program was offered 3 days/week for 18 weeks (up to 54 classes), while the Paired PLIÉ program was offered 2 days/week for 12 weeks (up to 24 classes). Other potential explanations include: 1) spurious results in the much smaller pilot study (n = 11); 2) regression to the mean in the intervention group of the pilot study, in which participants of the intervention had worse cognitive values at baseline compared to the usual care controls; or 3) involvement of caregivers in Paired PLIÉ, which could have resulted in a program that was less tailored to meet the needs of PWD because it also accommodated the needs of CGs.
In addition, our primary outcome of caregiver burden in CPs—although not statistically significant—was consistent with worsening while participating in Paired PLIÉ. This finding also is consistent with our qualitative results in which caregivers reported many logistical challenges with bringing PWD to the classes and being asked to practice home exercises.
Our exploratory analysis of secondary outcomes suggested potential improvement in mobility based on the Timed Up&Go task. This secondary quantitative finding is important and encouraging and is further illustrated by qualitative statements from CPs about their partners’ ability to get up from sitting in a chair. Again, these findings are consistent with our previous reports of the PLIÉ intervention [4, 16] as well as those of another dyadic exercise study [12].
Other findings of our exploratory analyses suggested potential decline or worsening during Paired PLIÉ in some standard measures, including flexibility and fear of falling in PWD and caregiver ratings of quality of life in PWD. We acknowledge that our qualitative survey data do not invalidate our direct assessment findings, but they raise concerns regarding the face validity of some of our measurements. It is important to note that the physical performance measures for balance and flexibility that are commonly used in research and were applied in this study have important shortcomings. The balance tests of the SPPB require foot positions that bring the feet close together and do not allow a hip-wide distance from each other in the frontal plane. This is contrary to the way the Paired PLIÉ program–and any occupational or physical therapy program–teaches balance skills by training to place the feet hip-distance apart to provide a stable stance. Similarly, the SFT flexibility measure requires the seated participant to bend forward and try to reach with their hands towards the toes with fully straightened knee. In contrast, the Paired PLIÉ program encouraged participants to bend their knees when reaching forward to minimize risk of discomfort or injury. Therefore, these measures contradicted the teachings of our program and may have confused participants. It is possible that concerns about falls may increase when participants learn to become increasingly aware of their balance during movement exercises.
We were surprised that we did not observe any evidence of change on our quantitative measure of chair stands since statements made by CPs about PWD indicated that physical functioning, particularly sit-to-stand, was notably improved in several ways. This is in contrast with one particularly relevant and more recent uncontrolled (N = 10; N = 22 dyads) pilot study by Yao et al. using six ‘sticky hands’ movement variations based on Tai Chi, music, and exercise incentives that found improvement in sit-to-stand time [12, 13].
Our qualitative results also suggest that future studies should include measures of social engagement, given strong qualitative statements about the joy and great benefits from the social interactions among the participants in the group classes.
Another important finding from the qualitative data was that, in establishing a community-based group program, issues around transportation are quite challenging for CPs and had an undeniable impact on recruitment and class adherence. The need to individually help the PWD out of the house into a private car or to public transportation in order to be able to join the class in a downtown location with major freeway traffic congestion was the biggest hurdle and challenge for participating in the Paired PLIÉ program. Therefore, we are now developing and testing an internet-based interactive virtual group class, where the instructor teaches in front of a video camera and dyads participate from their homes via two-way live-streaming video, with positive feedback. The recent COVID19 epidemic already demonstrated the growing need for internet-delivered and home-based interventions. Technology may offer an option for future research directions and a broader implementation of the intervention.
An apparent limitation of our study is the small sample size that limited our power to detect statistically significant results and may have led to imprecision in our effect size estimates. We also cannot exclude the possibility of chance findings. Generalizability of our results may be limited, because the study was conducted at a single site with mostly white and well-educated participants. Although participants were randomly assigned to the immediate or delayed start (waitlist) of the group intervention, the intervention group participants were statistically significantly older than controls. As advanced age brings additional health issues around physical fitness, joint degeneration, and other health issues, this may have diminished our chances for finding benefits from our program. This concern was offset by using the mixed models to examine change during Paired PLIÉ in both groups combined. Furthermore, as discussed above, standard measures for balance and flexibility may need modification, as they do not reflect best practices in fields such as physical therapy. Dyadic exercises in classes and at home require an extra effort by CPs, which may increase burden while also providing physical, social, and emotional benefits.
Future studies should consider examining changes in physical activity levels, in addition to changes in physical performance, to determine whether they are associated with retention, outcomes, or responses to participation. In addition, further study of the effect of such programs on the CPs and the relationship with the PWD should be considered for future research. Clearly there is a need for more studies of comprehensive integrative multi-modal dyadic group interventions with rigorous assessments.
In conclusion, our findings suggest that the Paired PLIÉ program may improve self-rated quality of life in PWD. Although some care partners may experience an increase in burden, most expressed high levels of satisfaction with the program and reported benefits in physical function and social/emotional well-being in themselves and their loved ones. Community movement classes that involve and engage both PWD and their CPs appear to be a treatment option, particularly for those who do not have access to—or are not ready for—a daycare facility. These results are encouraging and suggest further study, e.g., with interactive virtual group video conference adaptation, in a larger sample is warranted.
Footnotes
ACKNOWLEDGMENTS
This study was supported by (1) an intramural grant from the University of California, San Francisco (Resource Allocation Program, RAP, with funding from the UCSF Pepper Center (P30AG044281) and Tideswell at UCSF to Dr. Mehling and Dr. Barnes) and (2) funding from the Alzheimer’s Association to Dr. Barnes (NPSASA-15–364656). We are deeply indebted to the participants for volunteering; Alzheimer’s Services of the East Bay, ASEB, in Berkeley, CA, for providing space and support; the staff of Kaiser Permanente Oakland Medical Center for logistical support; the exercise instructors for assisting with developing and applying the intervention: Jennifer Lee, Deborah Marks, Robin Woodstock, Kristyn Marshman, and Janet Hetherington; the evaluation and assessment team: Tatiana Dannenbaum, Jason Flatt, Maria Ventura, Sienna Williams, Jennifer Wu; Leah Hotchkiss and Nicole Matouk; and Gary Tarasovsky for data management.
Dr. Mehling, Dr. Barnes, and Dr. Chesney are co-inventors of the Paired PLIÉ program and have the potential to earn royalties from Paired PLIÉ. The intellectual property for Paired PLIÉ is assigned to the University of California, San Francisco, and the Department of Veterans Affairs.