
Abstract
Background:
Social functioning is an important parameter for the early detection and diagnosis of dementia, as well as the description of its course and the assessment of intervention effects. Therefore, valid and reliable instruments to measure social functioning in individuals with dementia are needed.
Objective:
We aimed to provide an overview of such instruments including information on feasibility and psychometric properties.
Methods:
The review is informed by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Relevant literature was identified using a pre-specified search string in the databases MEDLINE, PsycINFO, and Web of Science. Information on the characteristics, feasibility, and psychometric properties of the identified instruments were extracted, summarized, and discussed.
Results:
Out of 5,307 articles, 8 were selected to be included in the study, describing a total of three instruments for measuring social functioning in individuals with dementia: the Nurses’ Observation Scale for Geriatric Patients (NOSGER; dimension “social behavior”), the Socioemotional Dysfunction Scale (SDS), and the Social Functioning in Dementia Scale (SF-DEM). The validity of all the three instruments was overall acceptable. Reliability was high for the NOSGER scale “social behavior” and the SF-DEM. Information on the usability of the instruments tended to be scarce.
Conclusion:
There are a few valid and reliable instruments to assess social functioning in individuals with dementia. Further considerations could comprise their feasibility with regard to measuring changes in social functioning over time, in additional target groups, e.g., different types and stages of dementia, and adaptions to different languages and cultural backgrounds.
Keywords
INTRODUCTION
Dementia is a neuropsychiatric syndrome that mai-nly occurs as a result of a degenerative disease of the brain. It is one of the most common and most severe disorders in old age and shortens the life span considerably [1]. The number of people living with dementia worldwide is constantly increasing [2]. In 2015, there were 46.8 million dementia cases [3], and the number is projected to increase to 152 million by 2050 [4]. This development will pose major challenges for public health and old age care systems in countries all over the world [5]. There is no effective treatment or cure for dementia yet. In the course of demographic changes that drive population aging, higher costs for health care systems will emerge [3]. Therefore, the importance of dementia prevention and early detection is growing.
The core symptom of dementia is acquired cog-nitive impairment that limits the independent performance of everyday functional activities. In addition to cognitive decline and functional loss, changes in so-cial functioning (SF) frequently occur in the course of dementia [6].
By showing repeated inappropriate social beha-vior—typically being unaware of it—people around individuals with dementia often withdraw from relationships with them. This reduces the individuals’ social contacts and social activities. Social behavior comprises “the readily observable interactions between an individual and other people, while “social functioning” is broader than social behavior in that it consist in the long-term and contextualized ability of an individual to interact with others” [7]. It is about how someone interacts in relationships with others, in social relationships, “how individuals associate and interact, both in society at large and their own personal environment”, such as loss of interest in previously valued hobbies or changes within close relationships [8]. Therefore, impairments in SF, showed as a disengagement from social activities that lead to impoverished interpersonal relationships, can contribute to increased psychiatric symptoms and worse mental health [6]. Behavioral problems such as disinhibition, apathy, or loss of empathy do not belong to SF by our definition. They are neuropsychiatric symptoms and are rather a prerequisite for SF. Supplementary Table 1 gives an overview of the definitions of the terms social cognition, social behavior, and social functioning.
SF needs to be differentiated from similar terms, such as social activities, social participation, or social engagement, which are frequently measured, for example, by collecting information on the frequency of contacts or meetings with family and friends or attending events [9]. Also, closely related is the construct of social network. It can be defined as “the web of social relationships that surrounds an individual” [10]. The assessment of the social network includes network size, the relationship between members and their frequency of contact [9]. These constructs are also important in surveys about individuals with dementia, and have been studied extensively [11, 12].
Changes in SF can occur early in the course of cognitive decline [13], in various types of dementia [14], including dementia due to Alzheimer’s disease (AD) [15], behavioral variant frontotemporal dementia (bvFTD) [16] and Lewy body dementia (LBD) [17]. In bvFTD, changes in SF are best described, because associated changes occur specifically in brain areas such as frontal lobes, anterior temporal lobes, and the amygdala being pivotal for SF [16, 18]. Studies also have shown that SF is already perceptibly altered in dementia pre-stages, e.g., in mild cognitive impairment [14]. In addition to cognitive and functional impairment, SF is thus not only an important criterion in the prediction and diagnosis of dementia but also a significant target variable for assessing treatment effects in prevention and intervention studies [8].
The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) also takes into account new research findings on the development and course of dementia which are explicitly reflected in expanded diagnostic criteria [19]. In addition to key characteristics, i.e., cognitive and functional impairment, social cognitive changes are now part of the diagnostic criteria of dementia, which are referred to as major neurocognitive disorder in the DSM-5. This is based on the observation that typical neuropathological changes in the brain trigger not only increasing impairment of cognitive and everyday functions, but also SF disorders [20]. Social cognition includes, e.g., aspects of social perception, social memory processes, socially influenced emotions, and thinking and acting [7, 15] and can be tested with standardized tests (for an overview, see [21]). SF needs to be assessed through self- and other-report questionnaires.
The significance of assessing SF in dementia consists in its usefulness for a better understanding of changes in relationships and associated outcomes in patients, relatives, and caregivers. It can be useful in the evaluation of intervention effects. As such, it can facilitate the development of effective psychosocial therapies and prevention interventions. This presumes valid and reliable measures of SF.
Therefore, the aims of the study were: To systematically review the literature to identify instruments for assessing SF in individuals with dementia; to provide an overview of the characteristics of the identified instruments and the feasibility of their application in individuals with dementia; to provide an overview of the psychometric properties (e.g., reliability, validity, and responsiveness) of the identified instruments; to provide recommendations for future research regarding instruments for assessing SF in individuals with dementia.
METHODS
Literature search
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [22]. We performed a systematic search for eligible articles in October 2019 in the electronic databases MEDLINE, PsycINFO, and Web of Science. The search included the following search algorithm: (question-naire OR instrument OR tool OR measure OR scale OR assessment* OR inventory) AND (dementia OR “cognitive function*” OR “cognitive imp-airment*” OR “cognitive decline” OR “neurocognitive disorder*” OR Alzheimer) AND (“social fun-ction” OR “social behavior” OR “social activity” OR “social life” OR “social participation” OR “social co-gnition” OR “social impairment” OR “social res-ources” OR “social appropriateness” OR “social inappropriateness” OR “socioemotional function”). The search was not limited regarding years of publication.
Eligibility criteria
Published articles were included if 1) the studies explained the development or psychometric testing of an instrument designed to assess SF in 2) individuals with dementia and 3) were published in English or German language in a peer-reviewed journal.
Single items were assigned to the domain of SF if the overall questionnaire, subscales of a questionnaire, or individual items addressed aspects of SF in the broader context of social interactions of individuals with dementia.
Study selection
The search results were uploaded to a reference management software (Citavi 6). First, duplicates we-re removed. Two reviewers (JG, SR) independently assessed the titles and abstracts of all identified articles in order to check their relevance for the study. Articles selected based on title and abstract screening were then read in full, specifically if the eligibility criteria were not clear yet. In case of disagreement, both reviewers discussed the articles until a consensus was reached.
Data extraction and data synthesis
The data were extracted by one researcher (JG). The following data were inventoried and described: 1) characteristics of the instrument (e.g., domains, number of items, scoring), 2) feasibility (administration, duration of application, ease of use, the latter indicating the ease with which the items are understood by or explained to the person with dementia, caregiver, or the interviewer and the availability of the instruments), and 3) psychometric properties (reliability, validity, and responsiveness, the latter defined as the ability to reflect changes in cognitive functions).
RESULTS
The search in the MEDLINE, PsycINFO, and Web of Science databases revealed 5,296 references. In total, 1,667 duplicates were eliminated. Additionally, 11 potentially suitable articles were identified after checking the reference lists of potentially eligible full-text articles. Finally, the study selection resulted in 8 articles describing three relevant instruments. Figure 1 illustrates the selection process.
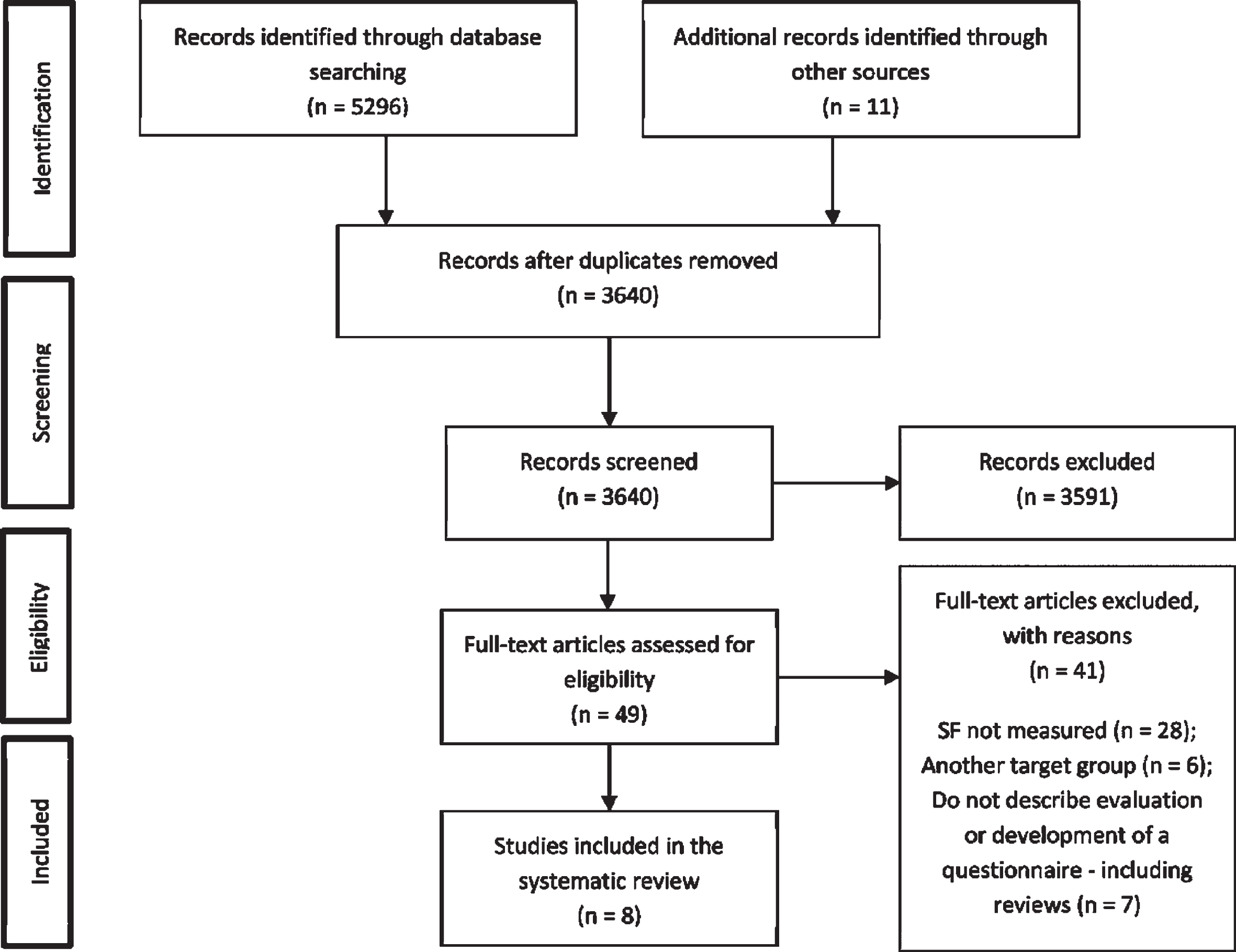
PRISMA flow chart of literature references on instruments for social functioning (SF) included in the review.
In addition to the three relevant instruments, a number of other instruments were identified, which included single items of relevance as part of other constructs. Such instruments were not the focus of the study; however, Table 1 provides a brief overview of these instruments. Moreover, Supplementary Table 2 lists further instruments that were not included in the systematic review with reasons for exclusion.
Instruments that include items to assess social functioning in individuals with dementia
SF, social functioning; # Domains and/or subscales are listed in numbered order. Below them, items relevant for SF are listed in italics. Individual items are separated by a semicolon. If an instrument has no subscales, only the items are listed (in italics). Subscales that contain relevant items are printed in bold; *in minutes; X: indicate quality criterion was tested; 1No information about the number of answer categories of the other items; 2qualitative question; 3121 main questions and 66 nested questions; 4detailed list of items is not freely available.
Instruments for assessing social functioning in individuals with dementia
Characteristics and feasibility of the instruments
The identified instruments for assessing SF in individuals with dementia were the Nurses’ Observation Scale for Geriatric Patients (NOSGER) [23], the Social Functioning in Dementia Scale (SF-DEM) [8], and the Socioemotional Dysfunction Scale (SDS) [24]. Table 2 shows the characteristics and feasibility of the instruments.
Characteristics and feasibility of instruments for assessing social functioning in individuals with dementia
Psychometric properties of instruments for assessing social functioning in individuals with dementia
1Refers to Brunner and Spiegel (1990); 2from the Geriatric Rating Scale; 3from the “semantic differential”; 4from the Götestam scale; 5SCAG factors which are similar in meaning and content to social behavior; 6PLUT scale “Reduced bodily care behavior”, atime between both interviews: 2 weeks. *Results from variance component analysis. α, Cronbachs Alpha; ADL, Activities of Daily Living; bvFTD, behavioral variant frontotemporal dementia; CDR, Clinical Dementia Rating Scale; DEMQOL, Dementia Quality of Life Scale; DKEFS, Delis-Kaplan Executive Function System; EOAD, Early onset Alzheimer’s Disease; FrSBe, Frontal Systems Behavior Scale family version; H, Kruskal-Wallis H test; ICC, Interclass correlation coefficient; MMSE, Mini-Mental Status Examination; NPI, Neuropsychiatric Inventory; PmD, Person with Dementia; PLUT, Geriatric observation scale of Plutchik; QoL-AD, Quality of Live in Alzheimer Disease (three social questions); r, Pearson’s correlations coefficient; rs, Spearman’s Rank coefficient.
The NOSGER is a 30-item questionnaire which is completed by a close caregiver. The screening tool was developed for outpatients and inpatients with suspected age-related dementia to detect behavioral changes in clinically relevant areas. Each area is assessed by one domain: memory, instrumental activities of daily living (IADL), activities of daily living (ADL), mood, social behavior, and disturbing behavior. Only one of the six domains, social behavior, taps into SF with five items (e.g., “Is interested in what is going on around him/her”, “Makes contact with people around”; cf. [25]). The scale is scored on a five-point Likert scale (1 to 5; “all the time” to “never”). The questions apply to the last four weeks.
The SDS is a 40-item scale for socioemotional dysfunction that can be completed by an informant (spouse, family member, caregiver, or other). The questionnaire reflects social interpersonal phenomena and socioemotional changes. Collective clinical features (disinhibition, apathy, social disengagement, poor social awareness, and difficulty discerning negative feelings in others) are represented in the content of the SDS items. This makes it especially relevant for clinicians, because these are the most promising discriminatory clinical markers of bvFTD [24]. Thirty-one items of the SDS were modified from the Social Competency Questionnaire (SCQ) [26]. The items are scored on a five-point Likert scale (1 to 5; “very inaccurate” to “very accurate”). A higher score indicates greater social dysfunction.
The SF-DEM assesses SF as the main construct and was developed specifically for individuals with dementia. It can be completed as a face-to-face interview with the individuals with dementia or with a proxy (e.g., caregiver or clinician). Both versions (self- and proxy report) consist of four domains: 1) Spending time with other people (e.g., “gone on trips or events like cinema or talks” or “seen friends and family in your own home”), 2) Communicating with other people (e.g., “talk to other people about your feelings or concerns” or “found it difficult to think of something to say to others”), and 3) Sensitivity to other people (e.g., “been very outspoken about what you really think” or “had argument or shouted at other people”). Altogether, the questionnaire includes 17 items. They are scored using a four-point Likert scale (0 to 3; “Very often” to “Never”) with a higher score indicating better SF. Three unscored summary questions assess overall impressions of SF in the individuals with dementia. These questions include recent change and willingness to make future social changes. Recent changes are recorded by comparing the current SF with the situation one year ago. Changes can be rated using a five-point ordinal scale. The will to change is assessed by asking if the individual desires to change their SF on a three-point Likert scale. The SF-DEM refers to the past four weeks.
Information on the instruments’ ease of use for individuals with dementia were found for NOSGER and SF-DEM. Regarding the NOSGER, short interviews with 42 relatives and caregivers were conducted to determine user acceptance and feasibility. In short discussions, it was determined to what extent the format of the NOSGER was acceptable and whether there were concerns or objections to individual terms. No concerns were expressed about the scale “social behavior” [23]. Wahle et al. (1996) confirmed these findings. The percentage of positive feedback given by individuals with mild dementia (87% acceptance) and individuals with moderate dementia (79% acceptance) was very high [27]. Regarding the SF-DEM, based on a survey of 30 dyads, consisting of a person with dementia and a relative each, Sommerlad et al. (2017) showed that 62% rated the SF-DEM acceptable and 38% very acceptable. There were no floor or ceiling effects, and all study participants were able to answer the questions of the self- and proxy version, respectively [8]. The acceptance of the proxy version of the SF-DEM was confirmed in a second study [28].
Psychometric properties
Psychometric properties concerning reliability, validity, and responsiveness were available for all three instruments in regard to the application in individuals with dementia. Details are given in Table 2.
The validity (concurrent) and reliability (test-retest and interrater) of the NOSGER scale “social behavior” have been tested. Spiegel et al. (1991) show high and meaningful correlations of the “social behavior” scale with external criteria measuring the same or related areas indicating concurrent validity [25], as summarized in Table 3. The interrater and the test-retest reliability showed high values in very diffe-rent settings and groups of patients. Wahle et al. (1996) showed significant differences in the results of the scale “social behavior” between healthy older individuals, individuals with mild dementia, individuals with serve dementia and elderly patients with depression [27]. The classification rate was at an acc-eptable level for this scale [29]. Responsiveness of individuals with dementia was demonstrated for the NOSGER. The study of Tremmel and Spiegel (1993) showed a moderate correlation between changes in the NOSGER scale “social behavior” and independent physicians’ overall assessments of treatment efficacy following a multicenter drug trail. In addition, they reported a moderate correlation between changes in the scale “social behavior” and the Mini-Mental Status Examination (MMSE) score, a test for cognitive impairment, assessed at baseline and at least three months later [30]. The rather short follow-up period may indicate that several different factors rather than the cognitive decline contribute to change in SF in individuals with dementia.
There was evidence for the validity (convergent and divergent) and reliability (internal consistency) of the SDS. The scale demonstrated preliminary evidence for discriminating between individuals with bvFTD and early-onset Alzheimer’s disease (EOAD). Furthermore, the SDS correlated strong with measures of conceptually similar constructs like judgment, community involvement, personal care, behavior, personality, apathy, disinhibition, elation, agitation, and irritability, which indicates convergent validity. The SDS also shows divergent validity as it can be differentiated from other concepts such as depression, anxiety, and delusion. The SDS total score did not correlate with proxy reports of measures of memory or orientation. Furthermore, the SDS did not significantly correlate with the majority of a range of cognitive tests except for one subscore of repetition errors on design fluency [24].
There was evidence for the validity (convergent, construct, content, and concurrent) and reliability (test-retest, interrater, and internal consistency) of the SF-DEM (see Table 1 for an overview). Sommerlad et al. (2017) found a moderate positive correlation between the SF-DEM total score and questions that measure a conceptually similar construct for both, the self-report and the proxy version [8]. This finding is an indication for convergent validity of both versions of the SF-DEM. Testing the construct validity of the proxy version, the domains “spending time with other people” and “communicating with other people” were correlated with levels of dependence as measured by the Bristol Activities of Daily Living (B-ADL) scale. All three domains were inversely correlated with neuropsychiatric symptoms. Only the item “sensitivity to others” was significantly correlated with quality of life. But this correlation was inversely as expected. Content validity was measured for both versions of the SF-DEM. They have shown to be good and reasonable, respectively based on qualitative opinions by interviewing study participants, both individuals with dementia and caregivers, in a focus group. Sommerlad et al. (2017) reported a moderate correlation between the patient or caregiver rated total score of the SF-DEM and their overall impression of the person’s “social life” indicates SF-DEM’s concurrent validity [8]. The agreement between patient and caregiver ratings supports the validity of the instrument. Moreover, they found pre-liminary evidence for the responsiveness of the instrument to measure changes in SF over time (repeated testing after an average of 7.2 months). In addition, there were indications that the question of the change in SF compared to a year ago predicts the SF-DEM score. However, changes in MMSE scores, i.e., cognitive impairment, in persons with dementia were not associated with changes in SF-DEM scores.
Instruments with relevant items
In addition to the three instruments presented, we have identified a number of other instruments that include SF as part of more comprehensive constructs, such as neuropsychiatric symptoms, problem behavior, and inappropriate behavior. These instruments cover SF either with single items or a number of items. Mostly, single items cover aggressive behavior. In all but one instrument, SF only plays a minor role. Table 1 provides an overview about these instruments with emphasize on the SF items.
DISCUSSION
We systematically reviewed the literature for ins-truments that are applicable for the assessment of SF in individuals with dementia. Such instruments are important in order to support a timely diagnosis of dementia and to better understand the course of the disorder. Reliable and valid instruments are also important for evaluating the effectiveness of different interventions.
Our systematic review identified three instruments to assess SF in individuals with dementia (NOSGER Scale “social behavior” [23, 30], SDS [24], and the SF-DEM [8, 28]). Detailed information regarding the feasibility and the psychometric properties of the instruments were provided, if available.
The scale “social behavior” from the NOSGER is short, which allows for quick assessments. Furthermore, the NOSGER was psychometrically tested (concurrent validity, test-retest, and interrater reliability) in different settings with different groups of elderly, which supports a broad application. It can be used to assess SF in individuals with any degree of dementia and is particularly helpful for individuals with AD. However, SF is not assessed as comprehensive as in the other two questionnaires: First, the SF-DEM consists of various subscales that comprehensively assess SF. It is the only questionnaire that can be completed by the individual with dementia or a proxy. In addition, it is the only questionnaire that also records changes in SF over time and asks about satisfaction with social life and the desire for change. This instrument was developed for individuals with dementia of any subtype. Specifically, it has been tested in individuals with mild dementia in regard to the self-report version, while the proxy-report version has also been tested in moderate to severe dementia. Comprehensive information about validity (convergent, construct, content, and concurrent) and reliability (test-retest, interrater and internal consistency) is available. The SF-DEM can be used for and the evaluation of interventions. It is also possible to track decline in SF in the context of disease progression. In addition to the SF-DEM, the SDS also provides comprehensive coverage of SF, whereby some of its items rather represent prerequisites for SF by covering socio-emotional changes including theory of mind. It can be used to assess SF in individuals with mild dementia. Therefore, it is possible to distinguish between individuals with EOAD and bvFTD on the basis of the results from SDS, which is not feasible using the SF-DEM. The SDS questionnaire is thus primarily relevant for clinical and diagnostic use. Currently there are estimates on the convergent and divergent validity and internal consistency, but there are no findings on test-retest reliability and interrater reliability of the SDS. The NOSGER and SF-DEM showed high values for the test-retest and interrater reliability. These instruments thus measure SF independently of the rater.
Besides the above discussed instruments, we have found a number of other instruments that include items to assess SF as part of a more comprehensive construct. The majority of these instruments add-ress a range of neuropsychiatric symptoms (e.g., aggression, agitation, wandering, yelling, repetitive behavior, etc.). Because single items of these instruments may only cover aspects of SF as opposed to measures such as the SF-DEM, which provide a comprehensive understanding of multiple facets of SF, these instruments may give rather limited information about SF in individuals with dementia. Therefore, instruments like the NOSGER scale “social behavior” and the SF-DEM seem more suitable, specifically as these instruments have been psychometrically tested.
Strengths and limitations
Our systematic review is, to the best of our kno-wledge, the first to provide an overview about instruments to assess SF in individuals with dementia. Our literature search was broadly diversified by using three databases. This ensured that as many relevant articles as possible were found. Only articles from peer-reviewed journals were considered. This procedure should make sure that the basic scientific quality of the studies that were included was given.
Nevertheless, there are also limitations in our study. First, it is possible that we missed relevant articles that were not covered by our search terms. Therefore, we additionally searched the references of potentially eligible articles. A second limitation concerns the restriction of the language of the selected articles: we were only able to consider articles in English or German language. Consequently, we may have missed instruments or versions of instruments published in different languages.
Further research and recommendations
Overall, the number of instruments to assess SF or aspects of SF in individuals with dementia was small. Moreover, the SF-DEM and the SDS are currently only available in English language. However, valid and reliable instruments to assess SF in individuals with dementia should also be available in different languages, for assessment in culturally different populations. Therefore, it is necessary to make progress toward adapting original instruments with promising psychometric properties for different languages. Moreover, specific inspection of the applicability of promising instruments could be tested in regard to different stages of disease progression, including more severe dementia, but also pre-stages and prodromal stages. This would be especially interesting to describe change in SF in relation to disease progression. Different types of dementia should be targeted as well. Currently, there is no instrument for SF specifically for individuals with AD. This is despite the fact that this is the most common of all dementias. It would be worthwhile to consider whether such a specific instrument would be useful. It could include aspects of personality and social changes, such as rigidity, self-centeredness, and limitations of social control, but also limitations in emotional recognition. There is evidence that such changes can occur in the preclinical and prodromal stages of AD [31, 32].
CONCLUSION
There are a few instruments to comprehensively assess SF in individuals with dementia, of which two instruments have been found to be psychometrically sound in regard to the considered populations (the NOSGER and the SF-DEM). Further reliability and validation studies would be useful in regard to instrument applicability in individuals at different stages of dementia including pre- and prodromal stages as well as different types of dementia. Studies that inspect the reliability of SDS would be valuable. Adaptations of standardized original instruments into other languages and cultural settings would be highly useful. Such adaptations should include examining the content of the questions in the questionnaire with regard to cultural differences, as social conventions and habits can differ in different societies [33, 34]. Having reliable standardized instruments to measure SF in individuals with different types of dementia is a prerequisite to driving our understanding and knowledge about the role of SF in any type of de-mentia. Research on the social aspects, especially SF in different types of dementia, is still incipient (except for bvFTD and LBD). Further questionnaires to assess specific aspects of SF depending on the type of dementia are necessary to gain a comprehensive understanding of this largely unexplored topic.