
Abstract
Background:
In addition to cognitive changes, motor impairments have been observed in patients with dementia and are present early in the disease, even at the preclinical stage. Although it is difficult to assess motor function in this population, it is critical for monitoring disease progression and determining the efficacy of therapeutic interventions. However, the best measurement tools for assessing motor function in dementia patients have yet to be determined.
Objective:
We aimed to summarize and critically evaluate the measurement tools used to assess motor function indementia.
Methods:
A systematic review was conducted using the databases CENTRAL, MEDLINE, Embase, and PEDro from their inception to June 2021 to identify all experimental studies conducted in patients with dementia and that included an assessment of motor function. Two reviewers independently screened citations, extracted data, and assessed clinimetric properties.
Results:
We included 200 studies that assess motor function in dementia patients. Motor function was assessed using a total of 84 different measurement tools. Only nine (12%) were used in over ten studies. The Timed-Up-and-Go test, 6MWT, Berg Balance Scale, and the Short Physical Performance Battery are all suggested.
Conclusion:
Currently, a wide variety of measurement instruments are used to assess motor performance in people with dementia, most instruments were not designed for this population and have not been validated for this use. We propose the development of an assessment protocol tailored to the different disease stages. We also recommend that future research continues to develop technological devices that can assist with this task.
Keywords
INTRODUCTION
Dementia is expected to affect 82 million people in 2030 [1]. Rather than being a specific disease, dementia is a syndrome in which there is a significant decline in cognitive function that interferes with the activities of daily living at home and work, and in society [1, 2]. According to the National Institute on Aging (NIA), dementia can be classified into five major groups, namely, Alzheimer’s disease, dementia with Lewy bodies, frontotemporal dementia, vascular dementia, and mixed dementias. While each group has its specific characteristics, they all share a common etiology: the presence of cerebrovascular dysfunction at some point during the disease process [1, 3]. Mild cognitive impairment (MCI) is a term used to describe a cognitive impairment that does not interfere with daily activities [4].
The autonomy to perform daily activities is influenced by the presence of both motor (strength, flexibility, aerobic capacity, and balance) and cognitive (executive function, attention, and memory) problems [5]. Although neuropsychological symptoms are still the most obvious sign of dementia, motor symptoms are common and transversal to dementia syndromes, affecting patients’ daily lives [6]. Slowed movement, decreased body tone, decreased spontaneous activity, impaired gait, and extrapyramidal movement disorders are examples of these [7]. According to a recent meta-analysis, motor problems, specifically upper limb motor function, parkinsonism, and lower limb motor function, precede cognitive impairment and have been proposed as potential clinical biomarkers for dementia [6].
Motor function is defined as the ability to learn or exhibit the effective and efficient assumption, maintenance, modification, and control of voluntary postures and movement patterns. Thus, motor function refers to goal-directed voluntary motor behavior [8]. The evaluation of a patient’s motor function and functionality enables the identification of the patient’s main problems and rehabilitation goals, as well as the design of a personalized treatment plan. These are all crucial aspects of disease management [9]. However, because of the wide range of motor impairments and measurement instruments, there is still no consensus on the best methods for evaluating motor function in the dementia field. The lack of a standard assessment protocol makes it difficult to not only interpret study results, but also to assess the efficacy of therapeutic interventions, and it restricts discussion among healthcare professionals [10]. The goal of this systematic review was to summarize and critically evaluate the measurement tools used to assess motor function in dementia. Based on the findings, recommendations were made.
METHODS
Literature search
We searched CENTRAL, MEDLINE, and PEDro from their inception to June 2021 using “Lewy-body”, “Dementia”, “Alzheimer”, “Frontotemporal-dementia”, “Physiotherapy”, “Physical-therapy”, “Exercise”, and “Motor Function” as key words. Reference lists from the identified articles were cross-checked to identify any further potentially eligible studies.
Study selection
We included all experimental studies that included a motor function assessment and identified the measurement tools used in people with any type of dementia or MCI. Papers in languages other than English, French, Spanish, and Portuguese, were excluded. Observational studies and reviews were also excluded. All retrieved abstracts were independently screened by two authors (AS, ML). The full texts of potentially relevant articles were retrieved for further assessment. Disagreements were resolved by consensus.
Data extraction
Five pre-defined domains were analyzed: general information (title, year and journal of publication, aim of the study, study duration, and type of intervention), methods (type of study design, method of randomization, achievement of allocation concealment, and type of blinding), sample (total number of randomized patients, patients per group, dropout rate, and sample size calculation), outcome measures (pre-defined outcomes, assessment tools, and time point measures) and study results.
The quality of reporting of the included studies was assessed using the Cochrane Risk of Bias (RoB) tool [11]. This tool quantifies the association between certain design features and estimates of treatment effects. The RoB tool is a two-part instrument, the first part refers to the description of what was reported in the trial, detailed enough for a judgement to be made based on this information, the second appraises the risk of bias for each analyzed area and classifies them in three categories: low, high, or unclear risk of bias.
Two authors (AS, ML) independently extracted data. Discrepancies were resolved through discussion or by consultation with a third reviewer (RBM).
Assessment of measurement properties
Based on criteria used in previous reviews, mea-surement instruments were classified as recommended, suggested, or listed [12–15]. These in-cluded: 1) being developed to be used in people with dementia, 2) being used in published studies by people other than the developers, and 3) “successful” clinimetric testing. Measurement instruments were classified as recommended if all three criteria were met; suggested if two of the criteria were met; and listed if only one criterion was met [12–15].
The search for studies evaluating the clinimetric properties of the included measurement tools was based on previous published papers about the topic and the references provided for each measurement tool in the included studies.
To provide a more comprehensive analysis of the instruments’ adequacy, a comment on their feasibility for use in people with dementia and in clinical practice was added, based on published evidence and the authors’ expertise.
Statistical analysis
The primary outcome was to identify the measurement instruments currently used to evaluate motor function in people with dementia. We summarized the publication characteristics using frequencies and percentages.
RESULTS
The electronic search identified 2,941 citations. After screening titles and abstracts 278 articles were deemed potentially eligible. Full-text assessment for eligibility resulted in 200 studies being included. Overall, the main reasons for exclusion were wrong outcome (n = 1,194); wrong study design (n = 781) and ineligible population (n = 499) (Fig. 1).

Flow diagram of the study selection process.
General features
Of the 200 included articles, 175 (87.5%) were published between 2010 and 2020 (Fig. 2). Studies were published in 88 different journals, the journals with the most studies were: The Journal of Alzheimer’s Disease (n = 19, 9.5%, impact factor (IF): 3.909), The Journal of the American Geriatrics Society (n = 10, 5%, IF: 2.675), The International Journal of Geriatric Psychiatry (n = 9, 4.5%, IF: 4.18), and The American Journal of Alzheimer’s Disease and other dementias (n = 8, 4% IF: 1.544). The majority of clinical trials that were registered were funded by public organizations.
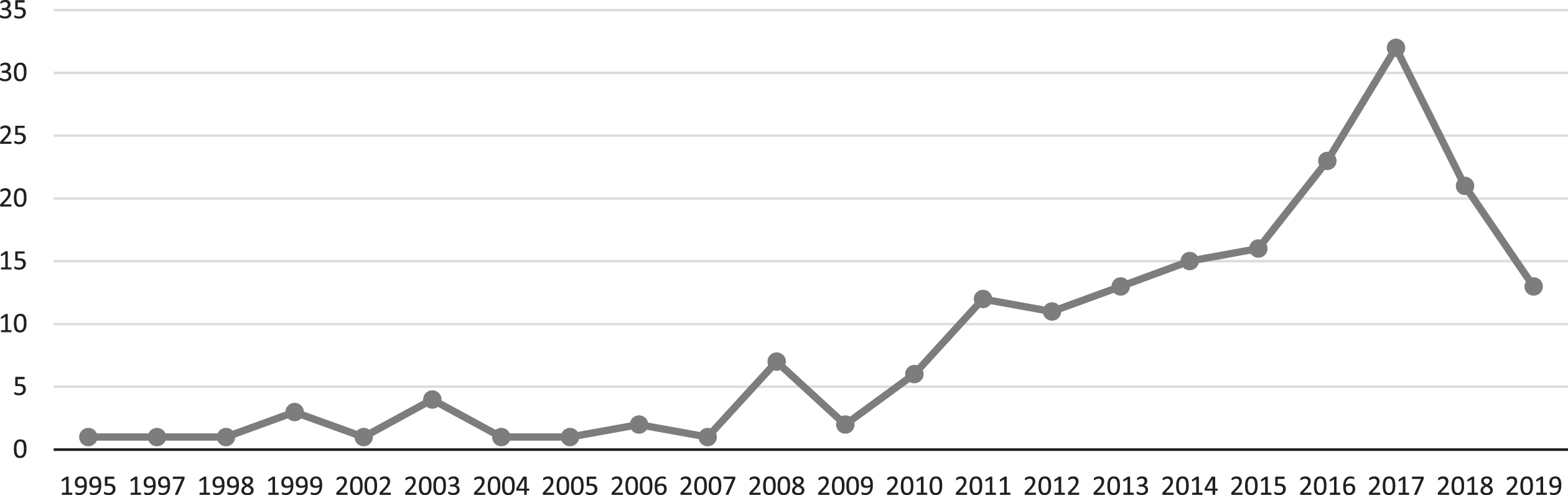
Number of published studies per year.
The most common study designs used were randomized controlled trials (RCT) (n = 115, 58%) and case-control studies (n = 36, 18%). Most of the studies were conducted in a clinical center/hospital (n = 148, 74%).
In 46 (23%) of the included studies, there was a high risk of bias in all domains (Fig. 3). The primary outcome was not specified in 118 (59%) studies. The mean dropout frequency was 19%. Intention-to-treat analysis was used in 63 (31.5%) of the studies.
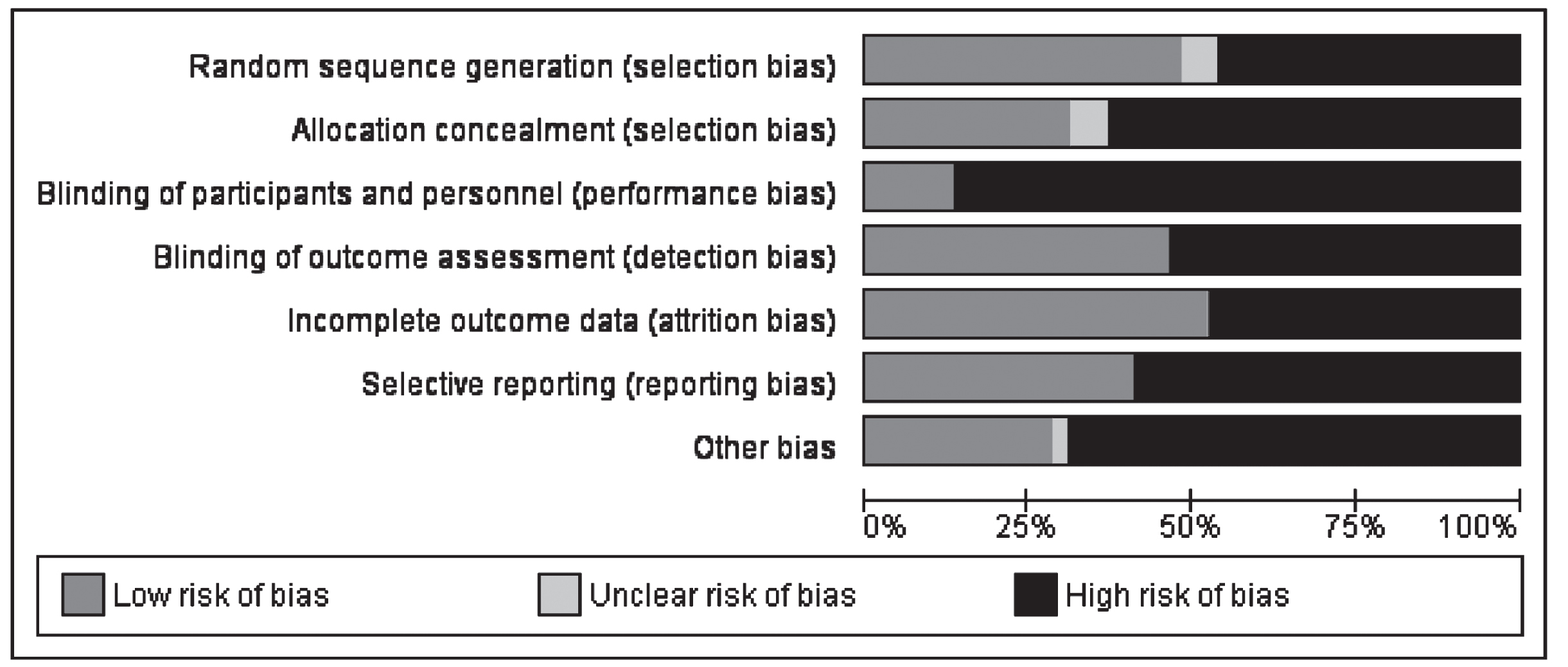
Results of risk of bias assessment.
Most used measurement instruments
The authors found 84 different measurement tools to assess motor function and mobility. Of these, only nine (12%) were used in more than ten studies. These include: The Timed Up and Go (TUG) Test (n = 45, 22.5%), the Sit-to-Stand (STS) test (n = 30, 15%), The Barthel index of Activities of Daily Living (Barthel Index) (n = 23, 11.5%), the Berg Balance Scale (BBS) (n = 22, 11%), the Six-minute Walking Test (6MWT) (n = 20, 10%), the Short Physical Performance Battery (SPPB) (n = 18, 9%), the Functional Reach Test (FRT) (n = 11, 5.5%), and the Falls Efficacy Scale International (FES-I) (n = 11, 5.5%). Kinematic gait analysis was used in 21 (10.5%) of the included studies (Fig. 4).
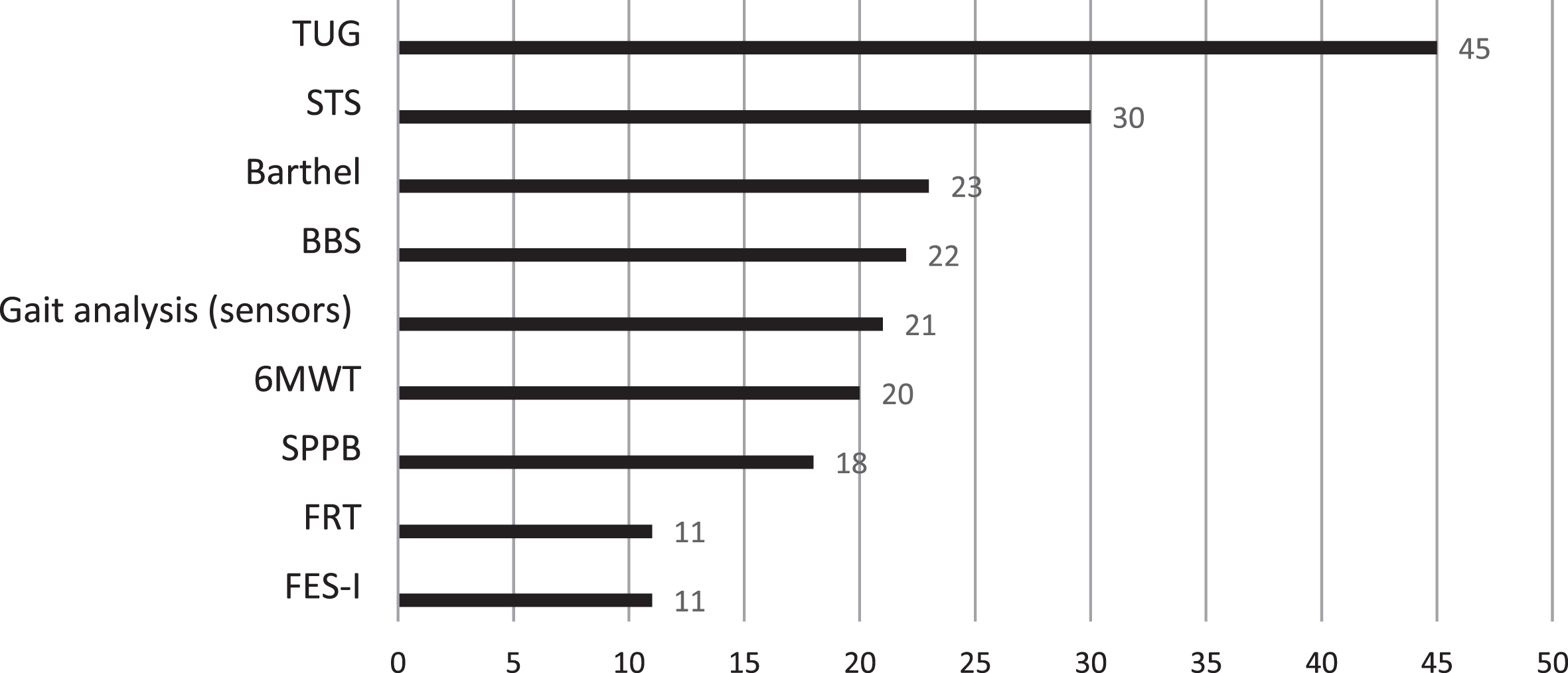
Measurement instruments used in at least five studies.
The STS test (n = 8, 4%) and the TUG test (n = 8, 4%) were the measurement instruments most used as the primary outcome. The most common secondary outcomes were: the TUG test (n = 9, 4.5%), the STS test (n = 7, 3.5%), the 6MWT (n = 5, 2.5%), and the BBS (n = 5, 2.5%). The Functional Independence Measure (FIM) was one of the instruments used as a primary outcome, but it was not among the most cited.
Quality assessment of most used measurement instruments
All measurement tools were administered to a dementia population, with data on their use in clinical studies beyond the group that developed the instrument. Tables 1 and 2 summarize some of the characteristics of the most cited measurement instruments in the included studies. A more detailed description of the clinimetric properties (the previously published results of reliability, validity, and sensitivity to change of each instrument) and feasibility issues is presented below.
Characteristics of the most cited measurement tools
Classification of the most cited measurement tools
Performance-based measures
The Timed Up and Go Test (TUG)
Construct assessed
Test description
The participant must rise from a standard chair, walk three meters at a comfortable and safe pace, turn around, and return to the chair. It is acceptable to use assistive devices. The instructor uses a stopwatch to count the task time [16].
Clinimetric properties
With an excellent test-retest reliability (ICC = 0.99) and a minimal detectable change of 4.09 s, the TUG proved to be a reliable outcome measure for use with people with Alzheimer’s disease [14, 18]. The TUG was able to distinguish between patients with mild to moderate Alzheimer’s disease and those with moderate to severe disease. When repeated measures (SEM - Standard Error of Measurements) were analyzed, participants who were more cognitively impaired had more variability in their performance than those who were less cognitively impaired. In addition, participants who were more cognitively impaired performed worse on the TUG than those who were less cognitively impaired [19]. The TUG was validated as a screening tool to measure the risk of falling in older adults, with a cut-off score of 13.5 s being associated with a high risk of falling [19].
Feasibility
The TUG is a simple and quick-to-use test. Patients must be able to walk (with or without the use of assistive devices) and follow instructions. Because patients take longer when focused on using safety strategies when getting up, turning, and sitting down, the safety training may interfere with TUG results in the early stages of the disease. In more advanced stages, the comprehension and retention of the instructions can interfere with the ability to perform the test [20].
Sit-to-Stand Test (STS)
Construct assessed
Lower extremity strength [15, 21].
Test description
This test has two modalities. Participants begin in both seated in an armless chair with their arms folded across their chest and their backs against the chair. In the Five Times Sit to Stand (5TSTS) the rater instructs the participant to stand and sit five times as quickly as possible without using his or her upper limbs. Participants in the 30-second Sit to Stand challenge are encouraged to complete as many full stands as they can in 30 s [22, 23]. Because both versions of the Sit to Stand test are commonly referred to as the Sit to Stand test, we’ll treat them as one for the purposes of this review.
Clinimetric properties
The clinimetric properties of the two versions of the STS test have not yet been studied in people with Alzheimer’s disease or other forms of dementia. Its clinical properties were investigated for older adults and people with Parkinson’s disease, who may share some motor characteristics, and it was found to be a good test for assessing lower limb strength in these populations[15, 22].
Feasibility
The STS test is an interesting test to use in clinical practice to assess patients’ lower limb strength because it requires minimal instrumentation and is a quick test with simple instructions [24].
Berg Balance Scale (BBS)
Construct assessed
Test description
The test consists of 14 items, each of which is scored from 0 to 4, and is used to assess a participant’s ability to maintain positions or movements that become more difficult as the base of support is reduced. Sitting, standing, standing to a single-leg stance, and positional changes are among the tasks [26].
Clinimetric properties
The BBS proved to be a reliable outcome measure for use with people with Alzheimer’s disease, with excellent test-retest reliability (ICC = 0.995), interrater reliability (ICC =0.83), and internal consistency (Cronbach’s coefficient of 0.95) [27]. The BBS showed a minimal detectable change of 1.92 points [27–29].
Feasibility
The BBS is a relatively safe and straightforward instrument to use. Due to ceiling effects, it may not be very useful in mild to moderately demented patients. The instructions are simple, allowing it to be used in more advanced stages of the disease [14, 30].
The Six-Minute Walk Test (6MWT)
Construct assessed
Physical capacity [14].
Test description
Participants are given six minutes to cover as much ground as possible on a standardized walkway, at their normal pace. Patients are allowed to use assistive devices and to pause if necessary [31].
Clinimetric properties
The 6MWT proved to be a reliable outcome measure for use with people with Alzheimer’s disease, with excellent test-retest reliability (ICC = 0.98, p = 0.001), excellent intra and interrater reliability (ICC = 0.76 and 0.97, respectively), and a minimal detectable change of 33.5 m. The analysis of repeated measures SEM showed a little difference in SEM for the mild to moderate Alzheimer’s disease group compared with the moderate to severe Alzheimer’s disease group [18].
Feasibility
The time and space required for this test to be used in clinical practice are the major drawbacks. It can only be used on patients who can walk (with or without assistive devices). Due to fatigue, when used at the start of the evaluation, it can affect performance in the remaining tests or rehabilitation sessions [32].
Short Physical Performance Battery (SPPB)
Construct assessed
Lower extremity functioning [33].
Test description
A small battery with three daily activities: balance (ability to stand for three seconds with feet together side-by-side, semi-tandem, and tandem), walking ability (two usual-paced 4-meter timed trials), and transfers (time to rise from a chair five times). The SPPB uses a 0-to-12 ordinal scoring system, with higher scores indicating better lower extremity function [33].
Clinimetric properties
The SPPB showed acceptable relative reliability, but the absolute reliability was deemed questionable when tested in demented patients living in aged care facilities [34, 35]. In a posterior study with older patients with dementia, the scale showed an excellent test-retest reliability (ICC = 0.84), a good internal consistency (Cronbach’s coefficient of 0.63), and a SEM of 0.68 points [36]. The authors highlight the importance of the test being applied by trained physiotherapists.
Feasibility
A practical measure that is easy to use and requires little equipment. This is not a difficult test for high-functioning patients [37]. Patients with dementia are more likely to comply with the test if it is divided into separate simple tasks [38].
Functional reach test (FRT)
Construct assessed
Static balance [14].
Test description
A ruler is hung at shoulder height on the wall. In the standing position, the participant must reach forward as far as possible beyond arm’s length while maintaining a stable base of support[39].
Clinimetric properties
The FRT has not yet been validated for use in people with Alzheimer’s disease or other forms of dementia. In Parkinson’s disease, the FRT showed a poor inter-test-retest reliability for patients without a history of falling and an excellent test-retest reliability for patients with a history of falling. It also showed excellent intra and interrater reliability. In older adults, it presented excellent test-retest, intra, and interrater reliability. Its clinical properties were investigated for older adults and people with Parkinson’s disease, who may share some motor characteristics, and it was found to be a good test for assessing lower limb strength in these populations [30].
Feasibility
The FRT is a clinical test that does not take a long time or a lot of materials to complete. Patients with no cognitive impairments frequently require assistance in performing the required movement correctly. Dementia can not only make the movement more difficult to understand, but also keep it going for as long as it is needed [40].
Other type of measures
In this section we included all the measurement instruments that are not based on patients’ capacity to perform a task. These included patient-reported, clinician-reported, and observer-reported measures.
The barthel index of activities of daily living
Construct assessed
Performance in activities of daily living [41].
Test description
This is a 10-item test that assesses the ability to perform activities of daily living. It can take 5 to 20 min depending on how the assessment is performed (patient-reported versus observer-reported). A person’s ability to perform an activity is graded on a scale of 0 (unable) to two (independent) [41].
Clinimetric properties
The Barthel index has not yet been validated for use in people with Alzheimer’s disease or other forms of dementia. In Parkinson’s disease, it showed an excellent internal consistency and interrater reliability [42].
Feasibility
This is a simple to apply scale that provides a global picture of patients’ performance in daily living. The test can be completed by people other than the patient, such as caregivers, and therefore can be used in more advanced disease stages [43].
Falls Efficacy Scale International (FES-I)
Construct assessed
Fear of falling [44].
Test description
This is a 16-item questionnaire that can be used as patient-reported or clinician-reported measurement instrument. The participant is asked to rate their fear of falling during an activity on a four-point Likert scale, with one being unconcerned and four being very concerned [44].
Clinimetric properties
The clinimetric properties of the FES-I have not yet been studied in people with Alzheimer’s disease or other forms of dementia. In Parkinson’s disease and older adults, it showed an excellent internal consistency and test-retest reliability [45].
Feasibility
Although simple to answer, it contains several activities that dementia patients do not engage in daily, making it difficult for them to respond and failing to provide a true picture of their fear of falling [46].
The Functional Independence Measure (FIM)
Construct assessed
Disability [47].
Test description
This is an 18-item questionnaire that evaluates a person’s level of disability and how much assistance they require to perform daily activities. It’s designed to be used as an observer-reported or, if that’s not possible, a clinician-reported measurement tool. Self-care measures include sphincter control, transfers, locomotion, communication, and social cognition [48].
Clinimetric properties
The clinimetric properties of the FIM have not yet been studied in people with Alzheimer’s disease or other forms of dementia. In older adults, it showed an excellent test-retest reliability [47].
Feasibility
It is a comprehensive scale that covers nearly 18 dimensions of daily life. Although it takes some time (30–45 min), focusing on basic ADL and having it rated by a health professional can give a detailed and realistic image of a patient’s disability [49].
Sample characteristics
Studies included a median sample size of 60 (range 4–6104) participants, all with more than 59 years old. The mean disease duration (reported in 9 (4.5%) of the studies) was 8 months.
From the studies that specified the disease stage (156, 78%), 39 (20%) were focused on patients with MCI, 36 (18%) in patients with mild to moderate dementia, and 9 (5%) in patients with moderate to severe dementia.
From the studies focused on Alzheimer’s disease (113 studies, 57%), eight (4%) included patients in the early disease stage, 35 (18%) focused on mild to moderate Alzheimer’s disease, and four (2%) on severe Alzheimer’s disease.
DISCUSSION
In the 200 included studies, a total of 84 different measurement tools were used to assess motor function in people with dementia. From these, only nine (12%) were used in more than ten studies, six clinical tests, and three questionnaires.
What are the most suitable measurement instruments to assess motor function in dementia patients?
As previously stated, motor function is defined as goal-directed voluntary motor behavior. Besides none of the measurement instruments has been designed to be used in dementia patients, none of them was also intended to evaluate the concept as a whole, but rather different aspects of it. As a result, according to the classification used, no instrument received the recommended level (Table 2).
Despite not being designed to measure motor function or used in people with dementia, the TUG test, the 6MWT, the BBS, and the SPPB were classified as suggested because some of their clinimetric properties have been studied. However, they were included in a method proposed by a panel of experts to assess motor function in dementia. According to the panel, motor function should be assessing in a sequential manner, evaluating different aspects of the concept, namely: balance, mobility and gait, lower limb strength, and functional performance [50]. We agree with the panel of experts that the using a selection of measuring instruments we may obtain a more complete view of motor function. This approach, however, has some limitations, including: 1) many of the instruments have not had their clinimetric properties studied in the dementia population, 2) some of the instruments mentioned (e.g., the TUG and the SPPB) are very demanding in terms of cognitive function, and can only be used in the early stages of disease, and 3) the time and effort required for such a comprehensive assessment usually limits its use in clinical routine.
The most used measurement instruments included three clinician-rated questionnaires. Although not validated to be used in dementia patients, the Barthel Index and the FIM may be good options for evaluating motor function when a patient’s ability to understand the instructions and comply with the test arelimited.
Our findings support previous research that re-ported that trials focusing on motor performance in dementia frequently used assessment tools that were not tailored to the target population [50].
Dementia patients and older adults have different motor and cognitive abilities. Dementia patients frequently experience difficulties in concentrating on complex, unknown tasks due to cognitive impairment, and they frequently have trouble understanding instructions, developing appropriate motor actions, and remembering them during execution. As a result, the outcome of motor assessments becomes compromised, i.e., the patient’s poor score is due to the patient’s ability to understand and comply with the test rather than a limitation in motor performance [50]. When planning a clinical assessment or designing studies for this population, these differences should be considered.
Appropriate assessments for cognitive impairments must be tailored to the patients. Assessments should: 1) include simple motor tasks, 2) be short in duration, 3) use appropriate instructions (e.g., no verbal focus, demonstration of the task, clear, short, and 4) repeated instructions [50]. The use of external cues is a controversial topic. External cues are required to ensure feasibility and achieve high relative reliability, according to some authors. Others argue that external cues may have an impact on the results, which may reflect the speed, reliability, and quality of external cues rather than the patients’ actual performance. The disease-specific gait and balance impairments should also be taken into account as the disease progresses. Some authors advocate allowing patients to use walking aids during motor tests to increase patient safety [50],
The use of digital outcomes to assess motor function in dementia
Kinematic gait analysis was used as a measurement instrument in 21 (10.5%) of the included studies. Due to the heterogeneity of the studies, it is not possible to recognize a standardized assessment protocol, or to clarify which are the most suitable technological devices for this purpose. Regarding location, the most common places were close to the individual’s center of gravity, in the feet or wrists.
In recent years, kinematic gait analysis has become a powerful tool for quantitative assessment in individuals with a variety of neurological conditions. It provides more precise and realistic data on the trajectories, velocities, accelerations, and angles of movement of different body parts. Therefore, it appears to be an ideal method for assessing movement in dementia patients. It has also the added values of being non-invasive, allowing for multiple assessments in a short period, providing quantitative and comprehensive kinematic data, and not requiring patients’ active participation [51].
According to a recent systematic review, the main impaired parameter in patients with MCI was slower gait speed, especially under dual task conditions, and that gait variability could predict an incident MCI [52].
Although quantitative gait measurements have been developed as diagnostic tools or instruments to support patient monitoring and assessment of therapeutic interventions, they are still in their infancy due to the lack of representative kinematic features of specific pathologies and a standardized assessment protocol [51].
Trends in clinical trials of physiotherapy and exercise in dementia
According to our findings, the number of papers published has increased over time, but the quality has remained unsatisfactory, with 46 (23%) of the included studies showing a high risk of bias across all domains. Although this has no influence on our findings (this is not an efficacy review), it is important information that should be considered in future studies because it has a direct impact on the overall strength of the published evidence. The primary outcome of many of the included studies was not specified, and the instruments used varied significantly between studies, making it difficult to compare and summarize the published evidence. In a previous study, a panel of experts emphasized the importance of a standardized assessment procedure for ensuring comparability between different trials/clinical examinations [50].
Most of the included studies (n = 184, or 92%), excluded the severe stages of the disease. Motor assessments are more difficult in the moderate/severe stages of the disease because of the inability of patients to understand the test instructions. Future studies should explore how to assess motor function when tests based on performance are not a feasible option. To this end, we believe that a technological device-based assessment would be an asset.
Conclusions
Our findings reveal a wide range of measurement instruments used to assess motor performance in people with dementia, however, the majority were not designed for this population and have not been validated for this purpose. Based on our findings, we propose developing an assessment protocol tailored to the various disease stages. We also suggest exploring the potential advantages of technological devices to assess motor function in this population. Because of their increased accuracy and passive assessments (i.e., not requiring an active test), they can provide a more realistic picture of the patient’s motor limitations.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/22-0151r1).