
Abstract
Background:
Age-related hearing loss (HL) has been associated with dementia, though the neurocognitive profile of individuals with HL is poorly understood.
Objective:
To characterize the neurocognitive profile of HL.
Methods:
N = 8,529 participants from the National Alzheimer’s Coordinating Center ≥60 years and free of cognitive impairment who were characterized as Untreated-, Treated-, or No HL. Outcomes included executive function (Trail Making Test [TMT] Part B), episodic memory (Immediate/Delayed Recall), language fluency (Vegetables, Boston Naming Test), and conversion to dementia. Regression models were fit to examine associations between HL and neurocognitive performance at baseline. Cox proportional hazards models examined the links between HL, neurocognitive scores, and development of dementia over follow-up.
Results:
At baseline, those with Untreated HL (versus No HL) had worse neurocognitive performance per standardized difference on executive function (TMT Part B [mean difference = 0.05 (95% CI 0.00, 0.10)]) and language fluency (Vegetables [mean difference = –0.07 (95% CI –0.14, –0.01)], Boston Naming Test [mean difference = –0.07 (95% CI –0.13, –0.01)]). No differences in these neurocognitive performance scores were demonstrated between Treated HL and No HL groups other than MMSE [mean difference = –0.06 (95% CI –0.12, 0.00)]. Through follow-up, executive dysfunction differed by hearing group (χ2(2) = 46.08, p < 0.0001) and was present among 39.12% in No HL, 44.85% in Untreated HL, and 49.40% in Treated HL. Worse performance across all cognitive domains predicted incident dementia.
Conclusion:
The observed association between Untreated HL and lower cognitive ability that improved when hearing aids were worn may reflect an inability to hear the test instructions. Future studies using cognitive assessments validated for use in HL are needed to evaluate the neuropsychological profile of HL and identify individuals at risk for dementia.
INTRODUCTION
In recent years, the adverse health outcomes associated with age-related hearing loss (ARHL), which is nearly ubiquitous among older adults [1], increasingly have been appreciated. ARHL contributes to the growing epidemic of social isolation and loneliness in older adults [2] and has been linked to incident frailty and increased fall risk [3]. Neuropsychiatric complications of ARHL prominently include cognitive decline and dementia [4, 5]. For example, an analysis of 639 participants in the Baltimore Longitudinal Study of Aging found that those who converted to dementia over 12-year follow-up had significantly greater hearing loss (HL) compared to those who did not. The hazard ratio for incident dementia increased with more severe HL, rising to 4.9 in participants with severe HL compared to those with normal hearing [6].
While compelling, the growing literature linking ARHL to progressive cognitive decline is limited by use of categorical clinical diagnoses (e.g., dementia) and global cognitive outcome measures (e.g., Mini-Mental State Examination [MMSE] [7]) appropriate for large epidemiologic surveys as opposed to a com-prehensive neurocognitive assessment. Global cognitive screening tools do not break down cognition by domain, and therefore may capture only limited variability in a normally aging population, with ceiling effects that potentially could lead to an underestima-tion of the true relationship between ARHL and cognitive performance. Very few studies report on the neuropsychological performance of older adults with ARHL by individual cognitive domain. For example, an analysis of 894 participants in the Staying Keen in Later Life study demonstrated statistically signifi-cant, but minimal, decreases in measures across all cognitive domains, such as episodic memory, proces-sing speed, attention, and executive function among individuals with HL [8]. In the National Health and Nutritional Examination Survey, worsening HL was associated with lower scores on the Digit Symbol Substitution Test [9], a finding consistent with prior literature showing slowed processing speed and executive dysfunction as risk factors for cognitive decline [10] as well as late-life depression [11]. ARHL also is associated with increased risk for late-life depression [12], which may be an intermediate step linking ARHL to dementia.
Further limiting the few studies reporting on cognitive performance by domain is their cross-sectional design, as it is unknown whether the patterns identified conferred increased risk for eventual conversion to dementia. Characterizing cognitive performance deficits that place hearing-impaired older adults at specific risk for further cognitive decline could provide insights as to the pathophysiologic mechanisms linking ARHL to dementia. Hypothesized mechanisms include decreased cognitive reserve caused by allocation of resources to process degraded auditory inputs, adverse neuroplastic changes to brain structures important for cognition resulting from auditory deafferentation, and “common-cause” mechanisms such as microvascular disease impacting both hearing and cognition [13]. Understanding the specific cognitive profile associated with ARHL that mediates risk for incident dementia could help adjudicate between these hypothesized mechanisms and identify novel therapeutic targets. For example, findings of slowed processing speed and decreased working memory performance may favor decreased cognitive reserve as an explanation [14], whereas diminished cognitive control and manifest executive dysfunction may point toward prefrontal cortex atrophy secondary to ARHL [15, 16].
In this study, we utilized the National Alzheimer’s Coordinating Center’s (NACC) longitudinal database of older adults to investigate the neuropsychological profile associated with ARHL. The NACC database is particularly well-suited to a study of this type, as it incorporates comprehensive neuropsychological assessments, rigorous classification of cognitive sta-tus, and longitudinal follow-up. In a recent publication, we evaluated the effects of HL on incident dementia, dividing individuals with HL into those who wore hearing aids (Treated HL) and those who did not (Untreated HL) [17]. We found that participants with Treated HL were at higher risk for con-version to dementia compared to those with No HL (HR = 1.29), whereas individuals with Untreated HL were not at higher risk for incident dementia compared to those with No HL. Here, we expand upon this earlier publication by examining cognitive perfo-rmance by individual domain in a cohort of participants with HL ≥60 years old who were free of mild cognitive impairment (MCI) or dementia at baseline. We hypothesized that 1) HL would be associated with worse performance on processing speed, executive function, episodic memory, and language fluency tasks and that 2) worse performance on these tasks would confer increased risk for developing dementia.
MATERIALS AND METHODS
Study population
NACC has collected the Uniform Data Set (UDS) on participants from >.30 United States Alzheimer’s Disease Research Centers from 2005 to the present. Participants with normal cognition and with clinical diagnoses of MCI and dementia of various etiologies were enrolled and followed approximately annually until death or study drop-out. Our cohort included NACC participants ≥60 years who were free of dem-entia or MCI at baseline, presented for at least two follow-up visits or one follow-up visit followed by death within a year, and had baseline hearing and depression assessments. Baseline was defined as ei-ther the initial UDS visit for participants ≥60 years or the first follow-up visit after the participant reached 60 years.
Assessments
HL and hearing aid (HA) use were assessed at baseline by a clinical interview and physical examination. The clinician responded to items querying (1) “Without a HA(s), is the subject’s hearing functionally normal?” (0 = Normal Hearing, 1 = Impaired Hearing), (2) “Does the subject wear a HA(s)?” (0 = No Aid, 1 = HA), and (3) “If the subject usually wears a HA(s), is the subject’s hearing functionally normal with a HA(s)?” (0 = Normal Hearing with Aid, 1 = Impaired Hearing with Aid). Utilizing clinicians’ responses to these items, we classified participants into categories of ‘No HL, ‘Untreated HL’, and ‘Tre-ated HL’ at baseline. The No HL category comprised participants with normal hearing who did not use a HA (i.e., 0 on Question 1, 0 on Question 2). Participants classified as Untreated HL had HL and either no HA or else continued hearing impairment despite HA use (1 on Question 1, 0 on Question 2 or 1 on Question 2 combined with 1 on Question 3). Finally, the Treated HL category included participants who wore HAs with consequent perceived functionally normal hearing (i.e., 1 on Question 2, 0 on Question 3).
Cognitive status was evaluated at baseline and at each follow-up visit through a history and physical, behavioral assessments (Clinical Dementia Rating [18], Neuropsychiatric Inventory Questionnaire [19]), functional assessments (Functional Assessme-nt Questionnaire [20]), and a comprehensive neurop-sychological battery [21]. The neuropsychological battery included six domains: global cognition (MMSE [7]), attention (Digit Span Forward [22], Digit Span Backward [22]), processing speed (Digit Symbol [23], Trail Making Test (TMT) Part A [24]), executive function (TMT Part B [24]), episodic memory (Immediate Recall [22] and Delayed Recall [22],) and language fluency (Animal list generation [25], Vegetable list generation [25], and the Boston Naming Test [26]). Higher scores correlate to better cog-nitive performance on all cognitive assessments except for TMT Part A and TMT Part B, where lower scores indicate better performance.
Participants were classified as having normal cognition, MCI, or dementia using guidelines set forth by the Alzheimer’s Disease Centers Clinical Task Force [27]. Blood samples were collected to determine APOE ɛ4 status, and participants were classified as having lowest risk (no ɛ4 alleles), intermediate risk (one ɛ4 allele), and highest risk (two ɛ4 alleles). As depressive symptoms also are associated with cognitive decline and dementia, we extracted the 15-item Geriatric Depression Scale (GDS) [28] collected at the initial UDS and at each follow-up visit. The 15-item GDS uses a yes/no answer format and scores range from 0 to 15. A cut-off of 5 or greater on this short-form 15-item GDS has shown to be highly sensitive to the identification of major depression [29].
Statistical analysis
Descriptive summaries of HL categories by demographics, baseline depression, and average length of follow-up were calculated and tested for differences using multinomial regression. To examine the association between HL and neurocognitive performance at baseline, regression models were fit for each neurocognitive performance score with cognition as the outcome and hearing category as the predictor variable. All analyses were estimated after controlling for age, sex, race, education, and APOE status and standardized scores of neurocognitive performance were used. TMT Part B scores were calculated after controlling for TMT Part A scores to assess executive function as opposed to processing speed. Executive dysfunction was a categorical measurement defined by TMT Part B scores 1 SD above the NACC mean (e.g., >128.5 s to complete the test), controlling for TMT Part A scores. An additional analysis on executive dysfunction during follow-up was conducted in a logistic regression controlling for age, sex, race, education, APOE status, baseline executive dysfunction, and TMT Part A score.
To examine the association between HL, neuro-cognitive scores, and development of dementia, we used Cox proportional hazards models with time from baseline until time of the dementia diagnosis as the primary outcome. Following the classic cause-specific hazard method for dealing with competing risk [30], we treated death (without a previous dementia diagnosis) as a censoring event. Specifically, cen-soring time for those not developing dementia was taken to be time until death or time until the last observed visit with no dementia diagnosis. An ass-umption of this method is that death is a non-info-rmative type of censoring for the event of interest (dementia). To mitigate possible assumption violation, and to take consideration that death may be in fact due to dementia, participants were deemed to have dementia if either the dementia diagnosis occ-urred in two consecutive visits or if the dementia diagnosis was followed by a death within one year. Those who had normal cognition followed by death or mild cognitive impairment followed by death were not considered to have dementia as it is likely that death was due to a different unrelated cause. We fit two models. The first model (Model 1) included baseline standardized neurocognitive performance on dementia controlling age, sex, race, education, APOE status, and HL group. The second model (Model 2) investigated interaction effects between baseline HL and baseline neurocognitive performance to identify if any HL group had a stronger or weaker association between neurocognitive performance and dementia.
RESULTS
Sample characteristics
As shown in Fig. 1, an analysis of the UDS visits conducted between September 2005 and December 2017 yielded N = 36,799 participants. Among this group, N = 19,385 were excluded for having dementia or MCI at baseline, and N = 2,923 were excluded for being < 60 years old at baseline. N = 5,432 participants were excluded for having only one follow-up visit unless death occurred within one year and N = 530 participants were excluded for having missing hearing or depression data, resulting in a final analytic sample of N = 8,529 participants.
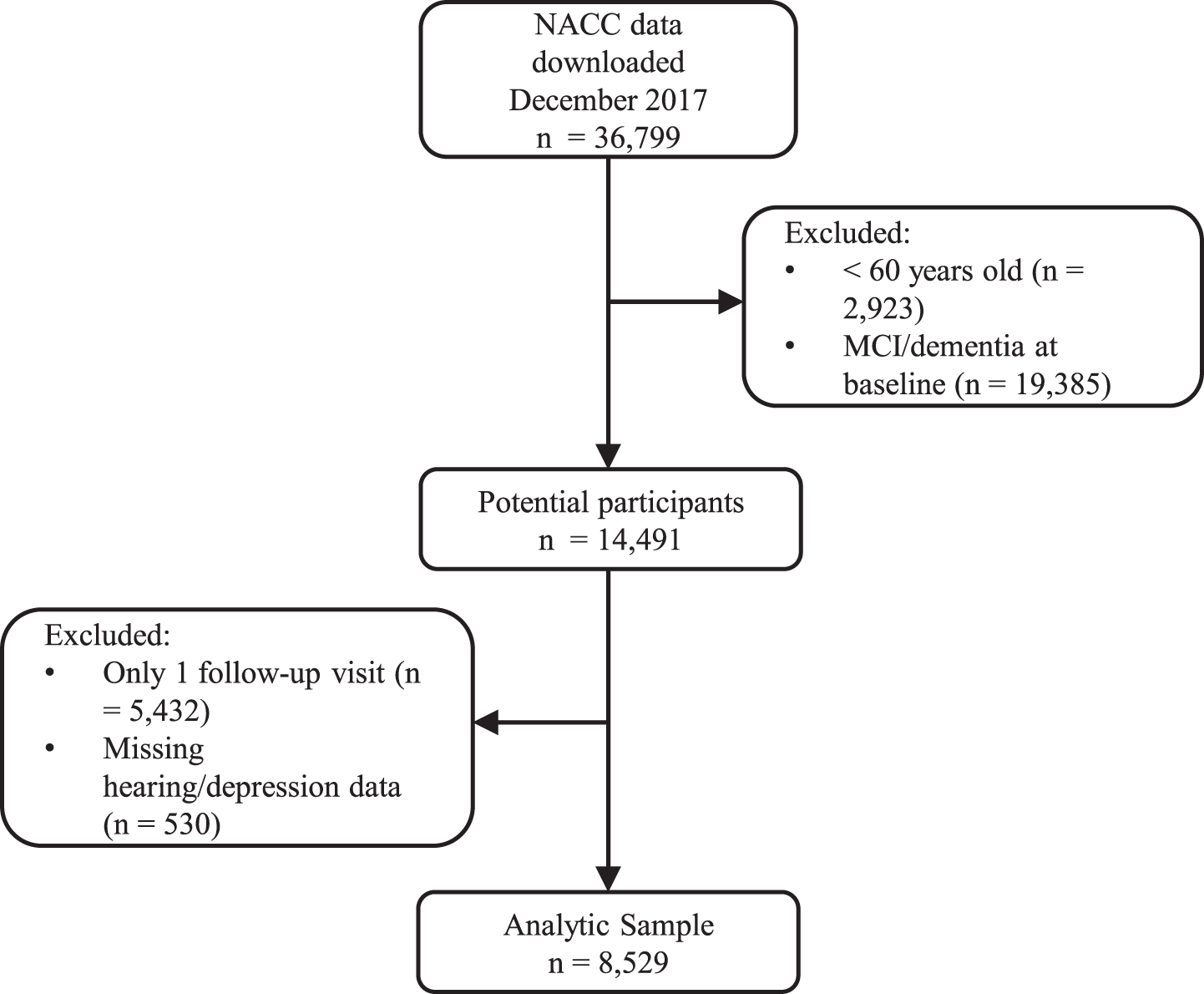
Flow diagram of included participants.
Of the 8,529 participants (Table 1), 949 (11.1%) were categorized as having Untreated HL and 1,102 (12.9%) were categorized as having Treated HL. Both hearing groups, particularly the Treated HL group, were older (χ2(6) = 443.17, p < 0.0001) and more likely to be male (χ2(2) = 84.00, p < 0.0001). Participants with Treated HL were less likely to be Hispanic and Non-Hispanic African American than Non-Hispanic White (χ2(8) = 80.75, p < 0.0001), and had a higher likelihood of having more years of schooling (χ2(2) = 9.57, p = 0.0084). The Untreated HL group was less likely to have an intermediate or high risk APOE genotype (χ2(6) = 14.99, p = 0.0203). There were no significant differences in mean depression scores (χ2(2) = 0.95, p = 0.6217) between hearing groups. The average length of follow-up in the sample was 67 months (5.58 years) with a range of 9–144 months, with an average of 5 repeated assessments and a mean interval of 14 months between follow-up visits.
Baseline demographics of the analytic sample (N = 8,529) and characteristics of the hearing categories
aYears of schooling measured as a continuous variable (Range 0–29). Depression = 15-item Geriatric Depression Scale (GDS) ≥.5.
Baseline hearing loss and neurocognitive performance
As shown in Table 2, several neurocognitive variables were significantly associated with HL group (Treated, Untreated, or No HL) at baseline. Those with Untreated HL (versus No HL) had worse performance on global cognition (i.e., lower scores on MMSE [mean difference = –0.09 (95% CI –0.15, –0.03)]), executive function (i.e., higher scores on TMT Part B [mean difference = 0.05 (95% CI 0.00, 0.10)]) and language fluency (i.e., lower scores on Vegetables [mean difference = –0.07 (95% CI –0.14, –0.01)] and Boston Naming Test [mean difference = –0.07 (95% CI –0.13, –0.01)]). For example, among those with Untreated HL, TMT Part B standardized scores were 0.05 higher (i.e., worse performance), and Boston Naming Test standardized scores were 0.07 lower (i.e., worse performance) than to those with No HL. Treated HL (versus No HL) did not have worse performance on these neurocognitive variables, except for MMSE scores [mean difference = –0.06 (95% CI –0.12, 0.00)]. There were no differences in odds of executive dysfunction between Untreated HL and No HL groups [OR = 1.01 (95% CI 0.81, 1.26)], and Treated HL and No HL groups [OR = 0.90 (95% CI 0.73, 1.12)]. Interestingly, those with Treated HL had better performance (i.e., higher scores) on Immediate- [mean difference = 0.07 (95% CI 0.01, 0.13)] and Delayed Recall [mean difference = 0.10 (95% CI 0.04, 0.17)] than those with No HL.
Distribution of baseline neurocognitive performance by hearing category and regression models of hearing category on neurocognitive performance.a
aN = 133 participants were missing baseline cognitive assessments (total N = 8,396); Analyses are controlling for age, sex, race, education and APOE; HL, hearing loss; Bold, statistically significant differences in mean scores; On all cognitive assessments except for TMT Part A and TMT Part B, higher scores represent better cognitive performance; Standardized scores of neurocognitive performance were applied in the regression analyses, and only one binary outcome, executive dysfunction, was analyses in the logistic regression. bMMSE, Mini Mental State Examination (total score). cWechsler Memory Scale-Revised (correct trials, total number of trials correct prior to two consecutive errors at the same digit length, length = maximum number of correct digit sequences recalled.). dWechsler Adult Intelligence Scale-Revised (number of items correctly completed in 90 s). eSeconds to complete. Trail Making Test Part B scores were calculated after controlling for Trail Making Test Part A scores to measure executive function rather than processing speed. fTrail Making Test Part B scores>128.5 s (1 SD above the NACC mean), controlling for Trail Making Test Part A scores. gLogical Memory IA Immediate Memory (total number of story units recalled). hLogical Memory IIA Delayed Memory (total number of story units recalled). iAnimal and Vegetable list generation (total number of animals/vegetables named in 60 s). jTotal score.
Risk for incident dementia based on neurocognitive performance
Lower performance within all cognitive domains (global cognition, attention, processing speed, executive function, immediate memory, delayed memory, and language fluency) at baseline increased risk for diagnosis of dementia over follow-up after controlling for hearing category (Model 1, see Table 3). In terms of the hazard of incident dementia associated with neurocognitive variables, worse processing speed (Digit Symbol [HR = 0.55]), executive function (TMT Part B [HR = 1.42]), Immediate- (HR = 0.58) and Delayed Recall (HR = 0.52) performance was associated with the greatest hazard, lower MMSE scores (HR = 0.65) and performance on language fluency (Animals [HR = 0.60], Vegetables [HR = 0.56]) was intermediate, and attention performance (Digit Span Forward [HR = 0.89]) imparted the lowest mag-nitude risk. Risk for dementia based on neurocognitive performance score (Model 2) was not modified by HL status at baseline. For example, no HL group had a stronger or weaker association between neurocognitive performance and dementia.
Relationships between neurocognitive performance and conversion to dementia, controlling for hearing category (Model 1).a
aN = 133 participants were missing baseline cognitive assessments (total N = 8,396); Analyses are controlling for age, sex, race, education and APOE; HL, hearing loss; On all cognitive assessments except for TMT Part A and TMT Part B, higher scores represent better cognitive performance; Standardized scores of neurocognitive performance were applied. bMMSE = Mini Mental State Examination (total score). cWechsler Memory Scale-Revised (correct trials = total number of trials correct prior to two consecutive errors at the same digit length, length = maximum number of correct digit sequences recalled.). dWechsler Adult Intelligence Scale-Revised (number of items correctly completed in 90 s) e Seconds to complete. Trail Making Test Part B scores were calculated after controlling for Trail Making Test Part A scores to measure executive function rather than processing speed. fLogical Memory IA –Immediate Recall (total number of story units recalled). gLogical Memory IIA –Delayed Recall (total number of story units recalled). hAnimal and Vegetable list generation (total number of animals/vegetables named in 60 s). iTotal score.
Finally, we were also interested in assessing the effects of HL on executive dysfunction over time. Over follow-up, Treated HL (versus No HL) were more likely to have executive dysfunction (OR = 1.19 [95% CI 1.02, 1.41]). Untreated HL (versus No HL) were not more likely to have executive dysfunction over follow-up (OR = 1.05 [95% CI 0.88, 1.26]). Through the study follow-up, executive dysfunction differed by hearing group (χ2(2) = 46.08, p < 0.0001) and was present among 39.12% in No HL, 44.85% in Untreated HL, and 49.40% in Treated HL.
DISCUSSION
This analysis of 8,529 older adults contributing to the NACC database found important relationships between HL, neurocognitive performance, and incident dementia. At baseline, we found that HL (Untre-ated) was associated with decreased cognitive ability on measures of executive function and language fluency compared to those without HL. HA treatment appeared to help minimize decline in neurocognitive performance at baseline, as participants with Treated HL did not demonstrate lower performance on neurocognitive measures compared to those without HL. Furthermore, over 45% of participants with Untreated HL and almost 50% of participants with Treated HL demonstrated executive dysfunction over follow-up. Lower performance across all cognitive domains (global cognition, attention, processing sp-eed, executive function, episodic memory, and language fluency) predicted increased risk for dementia over an average follow-up period of 5.6 years.
These analyses of cognitive performance and hearing status were consistent with a view of HL as being associated with lower executive function and language fluency. Our results may provide insights into the pathophysiologic mechanisms linking ARHL to dementia, as it has been proposed that HL may hasten cognitive decline by depleting cognitive reserve [13], which has been associated with impairment in working memory [14] and increased risk for dementia [31]. Conversely, it has been hypothesized that ARHL can lead to adverse neuroplastic changes and deafferentation-induced atrophy in frontal regions, which can tax the cognitive control network and cause executive dysfunction [13]. In terms of mechanistic models, our finding that HL was associated with lower performance in executive function and language, as opposed to episodic memory, might argue in favor of neuroplastic changes in the prefrontal cortex rather than decreased cognitive reserve as a model linking ARHL to dementia.
However, our previous finding in this dataset that Treated HL, not Untreated HL, predicted incident dementia over longitudinal follow-up introduces complexity to this interpretation. One possibility is that using HAs may be deleterious or cause individuals to feel stigmatized and enfeebled, which may alter one’s mood or behavior and thereby increase risk for dementia. However, this seems unlikely as existing studies have found significant associations between HA use and improvement in quality of life measures [32]. Another possibility is that HA use is a proxy indicator for more severe and longer duration HL, which are themselves associated with increased risk for dementia. In favor of this latter interpretation is that HA treatment in the NACC UDS was determined by a clinical interview (i.e., whether the participant was wearing a HA to their clinical evaluation) as opposed to objective measures of HA adherence. In general, HA utilization rates are low [33] and compliance is often inaccurately reported. Therefore, we suspect that many participants in the Treated HL group (i.e., who reported to clinicians that HAs normalized their hearing) were not in fact receiving adequate hearing treatment at home, which may help explain why hearing treatment did not mitigate their dementia risk.
In that case, the baseline association between Un-treated HL and lower cognitive performance may instead reflect the fact that cognitive assessments were not specially modified for individuals with HL. We suspect that executive function and language fluency assessments are likely to be most affected by difficulty hearing the test instructions, which is con-sistent with our observed association between Un-treated HL and decreased executive function/langu-age fluency that resolved when HAs were worn during baseline cognitive evaluation. The NACC neuropsychological battery was administered with verbal instructions, as opposed to instructions that are written or visually presented, which we hypothesize may present misleading results when interpreting cognitive performance among participants with uncorrected HL. Whereas we set out to characterize the cognitive profile associated with ARHL, it seems most likely that instead we evaluated the methodologic problem of not adapting the cognitive battery for older adults with HL.
Interestingly, there was not clear specificity bet-ween individual cognitive domain performance and risk for dementia. It was not surprising that worse performance on Immediate and Delayed Recall had the strongest association with incident dementia, as numerous studies have shown early episodic memory impairments in Alzheimer’s disease [34, 35]. Strong effects were also observed on tests of executive function, processing speed, and language fluency, which is consistent with prior literature demonstrating that deficits within these cognitive domains can predict progression to dementia [36]. The weakest association was observed between attention tasks and incident dementia, which is consistent with analyses demonstrating impaired attention primarily in later stages of Alzheimer’s disease [37]. However, the Digit Span test evaluates both working memory and attention, and in previous reports has demonstrated deficits in individuals with both MCI and dementia [38].
Recently, there has been significant interest in ex-ploring associations between ARHL and cognitive decline. For example, the 2017 and 2020 Lancet Commission on dementia identified HL as the single largest modifiable risk factor for dementia [39, 40], estimating that dementia prevalence would be reduced by 8% if HL was eliminated [40]. In addition, recent studies have demonstrated cognitive improvements with HA use [40], highlighting the importance of identifying and treating HL to mitigate risk for dementia. As ARHL is extremely common and often undiagnosed in older adults [41], our finding that Untreated HL can affect neuropsychological test performance is highly relevant to future studies. It is important to ask about HL, refer research participants for audiometric testing, and use cognitive testing batteries that are designed for use in individuals with HL. Although most cognitive batteries employ only verbal explanations of instructions and/or presentation of stimuli, specific cognitive tests such as the Repeatable Battery for the Assessment of Neuropsychological Status for Hearing Impaired Populations (RBANS-H) assess five cognitive domains (Attention, Immediate Memory, Delayed Memory, Language, and Visuospatial/Constructional) [42] and are appropriate for use in individuals with HL as all components of the evaluation are simultaneously presented orally and in written format [43]. Furthermore, given our hypothesis that length and severity of HL is more important than current cognitive performance in predicting incident dementia, studies that do not use cognitive batteries such as the RBANS-H may consider evaluating risk for dementia based on the long-term hearing trajectory rather than the current neuropsychological performance. Lastly, as the current studies evaluating ARHL and cognitive decline do not use cognitive tests designed for use in individuals with HL, new studies using cognitive batteries adapted for HL are needed in order elucidate the cognitive profile of older adults with ARHL who develop dementia.
These findings must be interpreted considering several limitations, which prominently include the use of clinician evaluations of both HL and HA use rather than measurement of pure-tone hearing thresholds in each ear and objective measures of HA compliance. The NACC protocols for clinician examinations are not completely standardized and allow some variability between ADRC sites, and we did not account for clustering of participants within each ADRC by HL category or cognitive performance, or for change in HL diagnosis over time. While some ARDC clinicians may diagnose HL by reviewing an audiometric evaluation if available, others rely on the participants’ report of HL. However, mitigating the effects of this limitation on our analyses, self-reported HL has demonstrated high sensitivity and specificity for HL, comparable to pure tone audiometry in some reports [44]. Additionally, the two HL groups, particularly those with Treated HL, were older and may have influenced our demonstrated findings between HL and incident dementia, though we did control for age in our analyses. Offsetting these limitations are numerous strengths of the study, most notably the large sample size, longitudinal follow-up of a carefully constructed cohort, high-quality cognitive assessments, and rigorous classification of cognitive status.
ARHL and dementia are common health conditions that are responsible for tremendous public health costs, including extensive disability, morbidity, and mortality. Several recent studies have linked ARHL to cognitive decline, but do not consider how hearing impairment may influence the results of cognitive testing. Future studies using cognitive batteries designed for use in hearing impaired populations are needed to further evaluate the cognitive profile of ARHL, which may identify good targets for early interventions (e.g., effective hearing remediation) to alter the trajectory of a phenotype at high risk for dementia.
Footnotes
ACKNOWLEDGMENTS
The manuscript was supported by the NIMH Gr-ants R25 MH086466 and T32 MH020004–22. The National Alzheimer’s Coordinating Center’s data-base is funded by NIA/NIH Grant U01 AG016976. NACC data are contributed by the NIA-funded ADCs: P30 AG019610 (PI Eric Reiman, MD), P30 AG013846 (PI Neil Kowall, MD), P30 AG062428-01 (PI James Leverenz, MD) P50 AG008702 (PI Scott Small, MD), P50 AG025688 (PI Allan Levey, MD, PhD), P50 AG047266 (PI Todd Golde, MD, PhD), P30 AG010133 (PI Andrew Saykin, PsyD), P50 AG005146 (PI Marilyn Albert, PhD), P30 AG062421-01 (PI Bradley Hyman, MD, PhD), P30 AG062422-01 (PI Ronald Petersen, MD, PhD), P50 AG005138 (PI Mary Sano, PhD), P30 AG008051 (PI Thomas Wisniewski, MD), P30 AG013854 (PI Robert Vassar, PhD), P30 AG008017 (PI Jeffrey Kaye, MD), P30 AG010161 (PI David Bennett, MD), P50 AG047366 (PI Victor Henderson, MD, MS), P30 AG010129 (PI Charles DeCarli, MD), P50 AG016573 (PI Frank LaFerla, PhD), P30 AG062429-01(PI James Brewer, MD, PhD), P50 AG023501 (PI Bruce Miller, MD), P30 AG035982 (PI Russell Swerdlow, MD), P30 AG028383 (PI Linda Van Eldik, PhD), P30 AG053760 (PI Henry Paulson, MD, PhD), P30 AG010124 (PI John Trojanowski, MD, PhD), P50 AG005133 (PI Oscar Lopez, MD), P50 AG005142 (PI Helena Chui, MD), P30 AG012300 (PI Roger Rosenberg, MD), P30 AG049638 (PI Suz-anne Craft, PhD), P50 AG005136 (PI Thomas Gra-bowski, MD), P30 AG062715-01 (PI Sanjay Asthana, MD, FRCP), P50 AG005681 (PI John Morris, MD), P50 AG047270 (PI Stephen Strittmatter, MD, PhD).