
Abstract
Background:
Cognitive decline in older adults is a serious public health problem today. Association between vitamin D supplementation and cognition remains controversial.
Objective:
To determine whether a 12-month vitamin D supplementation improves cognitive function in elderly subjects with mild cognitive impairment (MCI), and whether it is mediated through the mechanism in which telomere length (TL) regulate oxidative stress.
Methods:
This was a double-blind, randomized, placebo-controlled trial in Tianjin, China. Participants were all native Chinese speakers aged 65 years and older with MCI. 183 subjects were randomized to an intervention group (vitamin D 800 IU/day, n = 93) or a placebo group (the matching starch granules, n = 90), and followed up for 12 months. Tests of cognitive function and mechanism-related biomarkers were evaluated at baseline, 6 months, and 12 months.
Results:
Repeated-measures ANOVA showed substantial improvements in the full scale intelligence quotient (FSIQ), information, digit span, vocabulary, block design, and picture arrangement scores in the vitamin D group over the placebo group (p < 0.001). Leukocyte TL was significantly higher, while serum 8-OXO-dG, OGG1mRNA, and P16INK4amRNA revealed greater decreases in the vitamin D group over the placebo group (p < 0.001). According to mixed-model repeated-measures ANOVA analysis, vitamin D group showed a significant enhancement in the FSIQ score for 12 months compared with the control (estimate value = 5.132, p < 0.001).
Conclusion:
Vitamin D supplementation for 12 months appears to improve cognitive function through reducing oxidative stress regulated by increased TL in order adults with MCI. Vitamin D may be a promising public health strategy to prevent cognitive decline.
INTRODUCTION
Nowadays, Alzheimer’s disease (AD) is one of the most common causes of dementia which puts a heavy burden on the health care system [1]. For the early clinical diagnosis of AD, the concept of “mild cognitive impairment” (MCI) has been proposed as the transitional stage between normal aging and AD [2]. Exploring factors and biomarkers that are related with MCI have received much attention. Currently, epidemiological evidence has demonstrated that dietary might play an important part in cognitive function, especially vitamin supplementation [3, 4].
Vitamin D has been considered as a neuroprotective hormone [5, 6]. Before exerting biological effects, vitamin D must undergo hydroxylation to convert into 25-hydroxy-vitamin D (25(OH)D3) and 1,25-dihydroxy-vitamin D (1,25(OH)2D3) in the body. The lower 25(OH)D3 strongly associated with cognitive decline and neurodegenerative disease [7, 8]. Additionally, a study for vitamin D supplementation showed positive effects on specific cognitive domains, such as visual and working memory [9]. While some conflicting results were indicated that vitamin D supplementation did not influence cognitive performance [10, 11]. Besides, the mechanism still remains unclear.
Telomeres are DNA-protein structures located at the ends of linear eukaryotic chromosomes that protect chromosomal ends from DNA damage [12]. Studies have discovered telomere length (TL) might be a critical factor in predicting the rate of MCI or AD progression [13, 14]. Thus, a potential beneficial method for improving cognitive function is to maintain or enhance TL to protect neurons. The further biochemical reaction is oxidative stress (OS). OS is the state that refers to the imbalance between oxidation and antioxidant activity [15]. Attrition of tel-omere activates DNA damage response (DDR) which might increase OS damages [16]. In this state, OS induces cellular senescence and causes cognitive decline [17]. Therefore, in the battle against cognitive impairment, TL-OS system is a feasible mechanism.
The aims of this study were to evaluate the effects of 12-month vitamin D supplementation on cognitive function in older Chinese adults with MCI, and explore whether vitamin D supplementation possesses the mechanism of TL-OS system to improve cognitive performance.
METHODS
Study design and participate screening
This was a single-center, double-blind, randomized, placebo-controlled trial. A sample of 3,506 participants was selected from August 2017 to September 2017 by multistage cluster random sampling. Participants were all community dwellers in Nankai District, Tianjin and were enrolled according to the following criteria: 1) age 65 years or older; 2) no terminal illness or mental disorders (such as major depression, schizophrenia, two-way affective disorder, etc.); 3) not using any nutritional supplements known to interfere with nutritional status, vitamin D metabolism or cognitive function within 3 months prior to recruitment; 4) no medical condition prohibiting the use of vitamin D; 5) not living in a nursing home or about to be admitted to a nursing home. Of 3,506 possible participants, 2,676 were willing to participate, but only 2,210 eligible subjects received clinical, physical, and neuropsychological examinations. The flow diagram for screening, randomization, and follow-up is shown in Fig. 1.
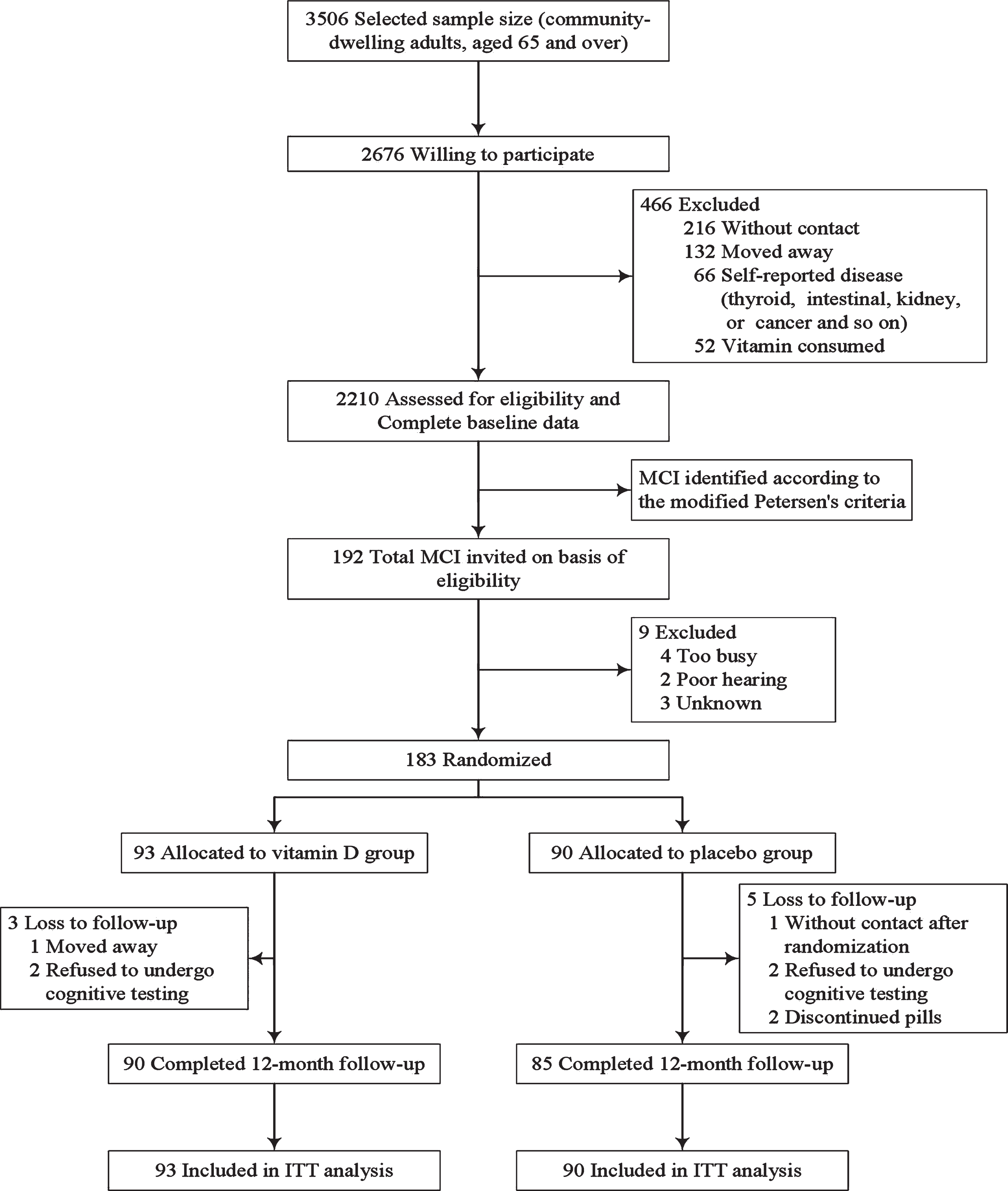
Enrollment and flow of participants. ITT, intent to reat; MCI, mild cognitive impairment.
This study was in accordance with the principle of the Declaration of Helsinki and was approved by the ethics committee at Tianjin Medical University, China (study number: TMUhMEC2018007). Each participant was provided written informed consent.
Definition of MCI
The MCI diagnostic criteria for this study was established according to the modified Petersen’s criteria [18], as follows: 1) Subjective and objective examinations have memory complaint; 2) Memory loss with at least 3 months duration; 3) 17 points in the illiterate group, 20 points in the primary school group, and 24 points in the middle school or above group on Mini-Mental State Examination (MMSE) subtask, the score lower than the demarcation is judged as cognitive impairment [19]; 4) Reduced living and social functions, as measured by Activity of Daily Living (ADL) scale (i.e., scores≤18) [20]; 5) Absence of dementia (Diagnostic and Statistical Manual of Mental Disorders-IV) [21]; 6) Eliminate cognitive decline due to special causes.
Intervention procedures
A total of 183 subjects with MCI was determined on the basis of the above criteria. After screening, subjects were randomly assigned to a vitamin D sup-plementation group or a placebo group. The randomization sequence was computer generated by the study sponsor. Then intervention began in October 2017 and completed in October 2018. Participants in the intervention group received two tablets consisting of 800 IU Vitamin D3 daily oral for the entire 12-month period. The ‘Aiweidi’ vitamin D3 capsule (400 IU/tablet; state medical permit No.: 2013012) was manufactured by Shanghai Sinopharm Health Industry Co. Ltd, China. And the placebo group was administered to the identical capsules daily oral which contained starch granules without vitamin and were manufactured by the same producer. Subjects were instructed to supplement with tablets at the same time every day and were monitored by telephone assessment monthly. Adherence was evalu-ated through a self-reported number of days on which capsules were taken and a count of the number of tablets returned from all participants. All subjects, researchers, doctors, and nurses of this trial were blinded to the treatment allocation until the completion of the statistical analyses.
Follow-up
Both groups were assessed at baseline, 6-month, and 12-month follow-up. All participants accomplished a health status questionnaire (include basic demographic characteristics, lifestyle, and medical history), MMSE scale, and ADL scale. In addition, blood biochemical parameters tests and cognitive assessments were measured for each subject at each time point.
Evaluation of cognitive function
Standard neuropsychological tests were administered at the baseline, 6-month, and 12-month follow-up by trained psychologists. The primary outcome was cognitive function assessed by the Chinese version of the Wechsler Adult Intelligence Scale-Revised (WAIS-RC) and the full scale intelligence quotient (FSIQ) [18]. The WAIS-RC contains 11 subtests: information, digit span, vocabulary, arithmetic, comprehension, similarity, picture completion, block design, object assembly, digit symbol, and picture arrangement. Additionally, FSIQ was computed by age-appropriate norms from the Chinese standardization [19]. MMSE was also evaluated as a measure of general cognitive function.
Evaluation of blood biomarkers
Fasting venous blood samples were collected from each subject, and the whole blood and serum- separating tubes were stored in liquid nitrogen. Genomic DNA extraction in 10 ml of whole blood applied a simple salting out procedure [22] and a column membrane method. Isolation of RNA used TRIzol LS reagent (Invitrogen, USA). Serum 25(OH) D3 and 1,25(OH)2D3 which are the main storage forms of vitamin D in the body were detected by liquid chromatography tandem mass spectrometer (API4000, AB SCIEX, USA), using high-perfor-mance liquid chromatography–mass spectrometry method. Real-time quantitative polymerase chain reaction (RT-qPCR) was adopted to determine TL in leukocyte genomic DNA with fluorescence quantitative PCR instrument (Lightcycler 480II, Roche) [23]. Moreover, since 8-oxo-2′-deoxyguanosine (8-OXO-dG) and 8-oxoguanine DNA glycosylase (OGG1) are the primary products of OS, the level of 8-OXO-dG in lymphocyte genomic DNA was measured with an ELISA test kit (Cayman chemicals, 589320). Meanwhile, gene expression for OGG1mRNA and P16INK4amRNA was determined by Rotor-Gene Q 6plex real-time PCR instrument (Qiagen, Germany), also using RT-qPCR [24].
Statistical analysis
The intent-to-treat (ITT) principle was used in all analyses in this study. Statistical differences between the intervention group and the placebo group at baseline were demonstrated using chi-square test or Fisher’s exact test for categorical variables and independent t-test or Wilcoxon’s signed-rank test for continuous variables. Post hoc comparisons used the Bonferroni test for multiple comparisons. The main analyses in this trial were repeated-measures analysis of variance (ANOVA) and mixed-model repeated-measures ANOVA. Repeated-measures ANOVA was conducted to assess the effects of vitamin D intervention and placebo treatment on cognitive function and blood biomarkers during 12 months. The values of variables at each time point were presented by calculating the mean unadjusted concentrations or scores plus standard deviations. And p value included time-treatment interaction that was adjusted for respective baseline value. Mixed-model repeated-measures ANOVA was applied to examine the hypothesis about differential changes obs-erved between vitamin D group and placebo group over time. The model was developed primarily for cognitive variable FSIQ. The critical test of the effectiveness was the evidence of showing that vitamin D supplements improved cognitive function compared to the placebo over time. The level of significance was set to a two-sided p value of 0.05 or less in all analyses, and the SAS statistical package (version 9.2, SAS Institute) was applied.
RESULTS
Characteristics of participants
A total of 183 participants was randomized to the vitamin D group (93) or the placebo group (90). Dropout rates were comparable between the two groups: 3 (3.23%) dropout in vitamin D and 5 (5.56%) dropout in placebo (p = 0.439). At baseline, characteristics of demography, lifestyle, and medical history were similarly distributed between groups except three variables. Moreover, there were no statistical differences in MMSE, level of 25(OH)D3 and 1,25(OH)2D3 between groups. Baseline characteristics of the study population are dis-played in Table 1.
Baseline characteristics of the study population
MMSE, Mini-Mental State Examination; 1,25(OH)2D3, 1,25-dihydroxy-vitamin D; 25(OH)D3, 25-hydroxy-vitamin D. *Data are presented as mean±SD unless otherwise specified. †p < 0.05 significant difference between groups. ‡Results are expressed as scale scores.
Cognitive status
With regard to cognitive status, repeated-measures ANOVA indicated significant interaction effects for FSIQ, information, digit span, vocabulary, block design, and picture arrangement over 12 months, as shown in Table 2. In addition, other cognitive domain tests of WAIS-RC were not significant. The FSIQ score was substantially higher in the vitamin D group than in the placebo group (p < 0.001); the vitamin D group increased by 1.81%, while the control group reduced by 3.28%. Both information and digit span scores demonstrated marked increments in the vitamin D group (+30.50%, +65.46%) compared with the placebo group (–6.19%, –0.67%) during 12 months periods (p < 0.001). Moreover, vocabulary, block design, and picture arrangement scores indicated improvements in the intervention group (+10.01%, +15.42%, +16.87%), while had the decline trend in the placebo group (–5.85%, –5.00%, –10.68%); differences in the change of vocabulary, block design, and picture arrangement scores were significant between the two groups (p < 0.001). The specific cognitive domain changes are presented in Table 2.
Cognitive domain scores at baseline, 6 months, and 12 months in the vitamin D and placebo group
FSIQ, full scale intelligence quotient. *Presented as mean±SD. †p values for each group (intervention versus placebo) were derived from repeated-measures analysis of covariance adjusted for the respective baseline value. ηp2 describes the percentage of variance in the dependent variable interpreted by an independent variable. In all tests, higher scores indicate better cognitive function.
Blood biomarkers
Concerning the main biomarkers of vitamin D status, as shown in Table 3, repeated-measures AN OVA demonstrated that 25(OH)D3 level in vitamin D group was significantly higher than in the pl-acebo group during the 12-month period (p < 0.001); the vitamin D group increased by 22.60%, while the placebo group reduced by 1.52%. Serum 1,25(OH)2D3 showed substantial rises in both groups (p < 0.001) and was greater in intervention group (+12.24%) than in placebo (+1.82%). About biomarkers for the mechanism-related, leukocyte TL in the vitamin D group was marginally higher than in placebo (p < 0.001), with increased by 12.68% in the vitamin D group, and decreased by 0.68% in the placebo group. Besides, concentrations of serum 8-OXO-dG, OGG1mRNA, and P16INK4amRNA revealed substantial percentage decreases in both groups (p < 0.001), and all of them showed a greater reduction in the intervention group with –14.84%, –65.53%, –44.48%, respectively, compared to the placebo group (–1.84%, –2.70%, –1.51%).
The level of blood biomarkers at baseline, 6 months and 12 months between the two groups
OGG1, 8-oxoguanine DNA glycosylase; TL, telomere length; 1,25(OH)2D3, 1,25-dihydroxy-vitamin D; 25(OH)D3, 25-hydroxy-vitamin D; 8-OXO-dG, 8-oxo-2′-deoxyguanosine. *Presented as mean±SD. †p values for each group (intervention vs placebo) were derived from repeated-measures analysis of covariance adjusted for the respective baseline value. ηp2 describes the percentage of variance in the dependent variable interpreted by an independent variable. ‡TL is expressed as T/S ratio-copy number of the telomere DNA (T) to the single copy gene (S).
Variable estimates from the final model for FSIQ are given in Table 4. The model took into account baseline related biomarkers and used mixed-model repeated-measures ANOVA. Compared with the placebo group, vitamin D group showed statistically a significant increase in the FSIQ score from baseline to 12 months (estimate value = 5.132, p < 0.001). Apart from the effect of vitamin D supplementation, baseline biochemical indicators were not found to be associated with cognitive function for FSIQ score at 12-month period.
Mixed-model analysis for describing the association between FSIQ and blood biomarkers at baseline
CI, confidence interval; FSIQ, full scale intelligence quotient; OGG1, 8-oxoguanine DNA glycosylase; SEMs, standard error of mean; TL, telomere length; VD, vitamin D; 1,25(OH)2D3, 1,25-dihydroxy-vitamin D; 25(OH)D3, 25-hydroxy-vitamin D; 8-OXO-dG, 8-oxo-2′-deoxyguanosine. *Represents interaction effect. † Reference category.
DISCUSSION
In this randomized controlled trial, daily oral vitamin D supplementation (800 IU/day) for 12 months significantly improved cognitive function in tests of global cognitive function (represented by FSIQ), information, digit span, vocabulary, block design, and picture arrangement subtests of WAIS-RC in Chinese older adults with MCI. Furthermore, vitamin D supplementation increased TL substan-tially while declined in serum 8-OXO-dG concentration, OGG1mRNA, and P16INK4amRNA gene expression compared to the placebo group. These discoveries support the hypothesis that the neuroprotective effect of vitamin D may be associated with reducing OS modulated by increased TL.
Our findings are consistent with several studies that have discovered the role of vitamin D supplementation in preventing cognitive degradation [9, 25–27]. But our results are incongruent with one existing evidence that indicated no effect for vitamin D on improving cognitive performance during a four-month intervention [11]. In this trial, supplements had higher FSIQ which may correlate with more efficient information transfer in the brain. Besides, the main characteristics of MCI are memory loss and impaired executive function. In this study, vitamin D supplementation beneficially affected information, digit span, and vocabulary subtests that are valid indicators of long-term or immediate memory, and vitamin D also had advantageous effects on block design and picture arrangement subtests which are corresponding to executive function [7, 28]. Thus, we can infer that memory and executive function domains enhance in order adults with MCI due to vitamin D supplements. This finding conforms to most of the previous trials in which vitamin D supplementation rescued nonverbal memory performance in the older adult with MCI [29, 30]. On the other hand, whole hippocampal volume and structural brain connectivity that play a distinct role in memory processing or executive function have been certified a correlation with serum 25(OH)D3 level in older adults with MCI [29]. Therefore, vitamin D supplements may lead a growth of hippocampal volume and strengthen hippocampal-thalamus-prefrontal connectivity to improve memory and brain function [31]. According to the above, it implied that vitamin D supplementation may have potential advantages on cognitive performance.
The underlying biological mechanism between vitamin D and cognitive performance is unclear currently. Some studies have been indicated that vitamin D might affect cognition through TL [32]. In various population-based studies, vitamin D supplementation may reduce the degradation of TL or slow down the premature shortening of telomeres [33]. In our current study, vitamin D supplementation during 12 months effectively increased the level of TL. Hence, vitamin D might play a role in maintaining telomere integrity. Apart from this, many population-based research have observed a correlation between the level of TL and cognitive performance in MCI or AD [13, 34]. TL may affect the nervous system through the following mechanism: it has been suggested that attrition of telomere may cause DDR, then the DDR induces severe OS damages further [16]. Thus, the expression of 8-OXO-dG and OGG1 may increase which can represent indicators for major oxidative DNA lesion or base excision [35]. Afterwards, a biomarker of cellular senescence, P16INK4a is activated and expressed highly in response to the increased OS [36]. Owing to emerging the cellular senescence, neurons and neuroglial cells in the brain may occur apoptosis and necrosis, further impacting on cognitive decline [37]. In this research, vitamin D supplementation increased TL in leukocyte and lower the concentrations of serum 8-OXO-dG, OGG1, and P16INK4a. So we speculated that vitamin D intervention might resist cognitive decline through enhancing TL and further weakening the OS response. The treatment can be a promising public health strategy to prevent cognitive impairment. In summary, vitamin D supplementation among subjects with MCI may improve cognitive function in related cognitive domains through the TL-OS system.
The study has some advantages. First, we used successful randomization and masking, then dropout rates over 12 months were low. Second, eligible subjects with MCI were determined using standardized diagnostic criteria through strict expert judgment. Moreover, a standard measure of cognitive function was applied which has robust internal consistency and validity. However, some methodological limitations of our study should be stressed. First, the optimal dose of vitamin D supplementation is uncertain. Second, in this trial, several characteristic variables (body mass index, history of hypertension, and alcohol habit) at baseline had statistical differences between the two groups. Finally, the biochemical markers in peripheral blood were used as surrogate indicators for the brain due to its easy to collect, but may not accurately reveal the changes in the brain.
In conclusion, this randomized placebo-controlled trial found that daily oral vitamin D supplementation (800 IU/day) for 12 months may significantly improve cognitive function through reducing oxidative stress regulated by increased telomere length in Chinese older adults with MCI. The results provide a possible direction for preventing cognitive decline in order adults. Larger scale and longer duration trials for vitamin D are needed in the future.