
Abstract
Background:
Dementia policy states that the early diagnosis of dementia can keep people living well for longer; however, there is little robust evidence to support this. Mild cognitive impairment (MCI) is considered a prodrome to dementia and can aid with the earlier diagnosis of dementia.
Objective:
The objective of this study was to use a previous diagnosis of MCI, before dementia, as a proxy for early diagnosis to investigate the relationship between an early diagnosis and mortality.
Methods:
A retrospective cohort study of electronic health care records from South London and Maudsley NHS. Patients aged 50+, diagnosed with dementia between January 2008 and November 2018, were divided into two groups: those with a previous diagnosis of MCI (early diagnosis) and those without. Cox regression models used to compare the risk of mortality between groups.
Results:
Of 18,557 participants, 5.6%(n = 1,030) had an early diagnosis; they had fewer cognitive, psychiatric, and functional problems at dementia diagnosis. The early diagnosis group had a reduced hazard of mortality (HR = 0.86, CI = 0.77–0.97). However, the magnitude of this effect depended on the scale used to adjust for cognitive difficulties.
Conclusion:
A previous diagnosis of MCI is a helpful proxy for early diagnosis. There is some evidence that an early diagnosis is associated with a reduced risk of mortality; however, it is not clear how Mini-Mental State Exam scores affect this relationship. While these findings are promising, we cannot be conclusive on the relationship between an early diagnosis and mortality.
INTRODUCTION
There is no cure for dementia; therefore current policy and guidelines for the treatment of dementia focus on delaying progression, improving quality of life, and increasing survival for people living with dementia [1]. The number of people living and dying with dementia is increasing, and it is now the leading cause of death in the UK [2]. The median survival time for people living with dementia is 10.5 years from the onset of symptoms and 5.7 years from the time of diagnosis [3]. However, survival estimates can vary greatly depending on the severity of the disease at the time of diagnosis with those diagnosed with mild dementia experiencing longer survival times and fewer life years lost than those diagnosed with moderate or severe dementia [4].
The early diagnosis of dementia is the cornerstone of the dementia policy in the UK, asserting that an early diagnosis can keep people living well for longer [5–7]. A diagnosis of mild cognitive impairment (MCI) presents the opportunity to identify dementia in the earlier stages of the disease. Current evidence suggests that dementia starts up to 10 years before the onset of symptoms; this asymptomatic phase is followed by an early symptomatic phase, during which people experience mild problems with their memory—and may be diagnosed with MCI—which then progresses to the full disease [8, 9]. Due to the complexity of diagnosing dementia, there is an increased risk of misdiagnosis in the early stages of the disease [10]. Furthermore, the diagnosis of MCI is a grey area, and it is not clear how MCI progresses into dementia as not everyone with MCI will go on to develop dementia [11–13]. However, a diagnosis of MCI is considered to be a useful clinical tool for identifying people at risk of developing dementia and could help with the early diagnosis of dementia [8].
While dementia policy in the UK has suggested that diagnosing dementia early can keep people living longer [5–7], there is very little robust evidence to support this. In 2011, Alzheimer’s Disease International assessed the strength of the evidence for the proposed benefits of diagnosing dementia early. They found only three population-based studies which examined the relationship between early diagnosis and mortality, or cognitive decline and these studies reported small effects [14]. When the researchers reviewed statements summarizing the benefits of early diagnosis, they found them largely to be unreferenced and not evidenced-based. Furthermore, much of the research into the benefits of diagnosing dementia early is based on modelling and not patient data [15]. More research using real-world data is needed to understand how an early diagnosis can keep people with dementia living well for longer.
One of the challenges of investigating the effects of early diagnosis is how to identify people living with dementia who have received an early diagnosis. While not all people who are diagnosed with MCI will go on to develop dementia, a diagnosis of MCI before dementia could be a helpful proxy for early help-seeking and early diagnosis. Using a previous diagnosis of MCI presents the opportunity to explore the effects of early diagnosis on long-term outcomes, such as mortality, in existing cohort studies and populations ascertained from routinely collected data. Therefore, the aim of this study was to investigate the association between a previous diagnosis of MCI and mortality.
Objectives
To address the overall aim of this study, we used a retrospective cohort design to compare participants who had been diagnosed with MCI before dementia and those who had never received a diagnosis of MCI.
The specific objectives of this study were to:
Explore whether a previous diagnosis of MCI—before dementia—can be used as an indicator for early diagnosis or early help-seeking;
Investigate differences between participants with a previous diagnosis of MCI and those without;
To investigate the association between a previous diagnosis of MCI and mortality, while taking differences between groups into account.
MATERIALS AND METHODS
Data sources
The data used in this study were extracted from electronic health care records from the South London and Maudsley NHS Trust (SLaM) Biomedical Research Centre Clinical Record Interactive Search (CRIS). SLaM provides specialist dementia care to people living in the catchment areas of Lambeth, Lewisham, Southwark, and Croydon. Data are stored both in structured fields and in free text, the extraction of which has been described previously [16, 17]. The CRIS database has full approval for secondary analysis (Oxford Research Ethics Committee C, reference: 08/H0606/ 71 + 5). This study utilized an existing linkage between CRIS and the Office for National Statistics (ONS) for mortality data.
Sample identification
Data from all SLaM patients who were diagnosed with dementia according to International Classification of Disease (ICD-10) diagnostic criteria [18] between 2 January 2008 and 4 November 2018 and were over the age of 50 at the time of diagnosis were extracted using CRIS. Date of first dementia diagnosis served as the index date. Dementia diagnosis was determined using structured ICD-10 codes in structured fields in the clinical record, supplemented by a bespoke natural language processing (NLP) algorithm using General Architecture for Text Engineering (GATE) software [19, 20].
Measures
Mild cognitive impairment
A diagnosis of MCI according to ICD-10 code F06.7 before the index date was ascertained from structured fields supplemented by free-text using GATE-derived software. This was included as a dichotomous variable (yes/no).
Mortality
Mortality data, including date and cause of death up until 14 November 2018, were collected from the data linkage with the ONS. All causes of death were included in this study. Participants were followed-up from the date of diagnosis until death or the census date.
Covariates
Demographic data were extracted from routinely completed fields including age at the time of dementia diagnosis, gender, marital status, and ethnicity. Marital status was coded as current partner or no current partner. Ethnicity was coded as European, Black, Asian, or Other. Mini-Mental State Exam (MMSE) scores were extracted from CRIS using NLP. Where patients had multiple MMSE scores, we used the score closest to the date of dementia diagnosis. Data were extracted from the Health of the Nation Outcome Scales (HoNOS), a routine measure of wellbeing in UK mental health and dementia services [21]. The HoNOS subscales are rated on a five-item ordinal scale (from 0 for no problem to 4 for severe or very severe problems), whereby we dichotomized following the clinicians’ approach of first considering whether there is a problem requiring intervention (score 2–4) or not (score 0-1). Dichotomized variables based on HoNOS scores have been shown to have predictive validity for mortality in cohorts of patients with dementia assembled from this cohort [22, 23]. We examined HoNOS subscales for clinician-rated cognitive problems, physical illness and disability, and activities of daily living (ADL), and used the remainder to adjust for the presence of psychiatric symptoms experienced by participants and grouped those by number of symptoms (no symptoms, one symptom, two symptoms, and three or more symptoms). Two measures of cognitive problems (MMSE and HoNOS) were included in this study as we anticipated multicollinearity between MMSE scores and a previous diagnosis of MCI. Index of Multiple Deprivation was derived from the patient’s address at the time of diagnosis [24]. The prescription of acetylcholinesterase inhibitors (AChEIs) up to six months after diagnosis were extracted using GATE hosted applications and were dichotomized (yes/no).
Statistical analysis
Data were analyzed using Stata 15 [25]. This was an exploratory study, the exposure under investigation in this study was the prior diagnosis of MCI, referred to as an early diagnosis, and the outcome was all-cause mortality. We used chi-squared tests and t-tests to examine the differences between the two groups, in categorical or dichotomous variables and continuous variable respectively. The significance threshold was set at 0.05 for all analyses.
Kaplan-Meier curves with log-rank tests were used to compare survival between the two groups. Cox regression models were used to investigate the association between early diagnosis and all-cause mortality, age at diagnosis, gender, ethnicity, levels of physical illness, clinician-rated cognitive impairment, prescription of ACHEIs, and MMSE scores at diagnosis were included in the models to control for confounding. A sensitivity analysis was conducted to compare the dichotomized and ordinal versions of the HoNOS measure of cognition. We checked the proportional hazards assumption was met by using a test of Schoenfeld residuals. Where this assumption was not met, a time interaction for the problematic variables was included in the model.
Missing data
MMSE scores were missing for 30%of participants and 13%of participants were missing one or more items on the HoNOS. All other variables had 1%or less missing data. Missing data were imputed using multiple imputation by chained equations [26], assuming missing at random, to maximize statistical power. Ten datasets, including all covariates and outcomes, were imputed using the mi package in STATA before using Cox regression models on the imputed datasets.
RESULTS
Participants
We identified 18,555 patients diagnosed with dementia. The characteristics of the sample are presented in Table 1. The mean age of participants was 80.8 (SD = 8.7) years, and the majority of patients (60.6%) were female, without a current partner (66.6%) and had high levels of physical illness and disability (56%). The majority of participants (35.9%) had no psychiatric symptoms. The average MMSE score was 18.6 (SD = 6.3) and AChEIs were prescribed to one third (31.9%) of participants in this study.
Characteristics of participants and factors associated with the early diagnosis of mild cognitive impairment
HoNOS, Health of the Nations Outcome Scales. †Higher score indicates more socially deprived. *Significant p≤0.001. **Significant p < 0.05.
Factors associated with an early diagnosis
Of the 18,555 patients included in this study, 1,030 (5.6%) had a previous diagnosis of MCI recorded. The mean time between the diagnosis of MCI and dementia was 1.2 years (SD = 1.5). In Table 1, the differences between patients who received an early diagnosis of MCI and those who did not are also presented. T-tests showed that participants with an early diagnosis had better cognition, rated by the MMSE, and higher levels of social deprivation. Chi-squared tests showed participants with an early diagnosis differed in terms of ethnicity, with a greater proportion of white participants receiving an early diagnosis compared to other ethnic groups. Participants with an early diagnosis reported fewer problems with cognition, had fewer psychiatric symptoms and less impaired ADL as rated by the HoNOS. Additionally, a greater proportion of participants with an early diagnosis were prescribed AChEIs following diagnosis.
Early diagnosis and mortality
Between baseline diagnosis of dementia and the census date, there were 10,344 deaths (55.7%) with a median survival time of 4.02 years (IQR = 1.8–7.2). Kaplan-Meier curves show increased survival in people with an early diagnosis of MCI (Fig. 1) (log-rank test: p < 0.01).
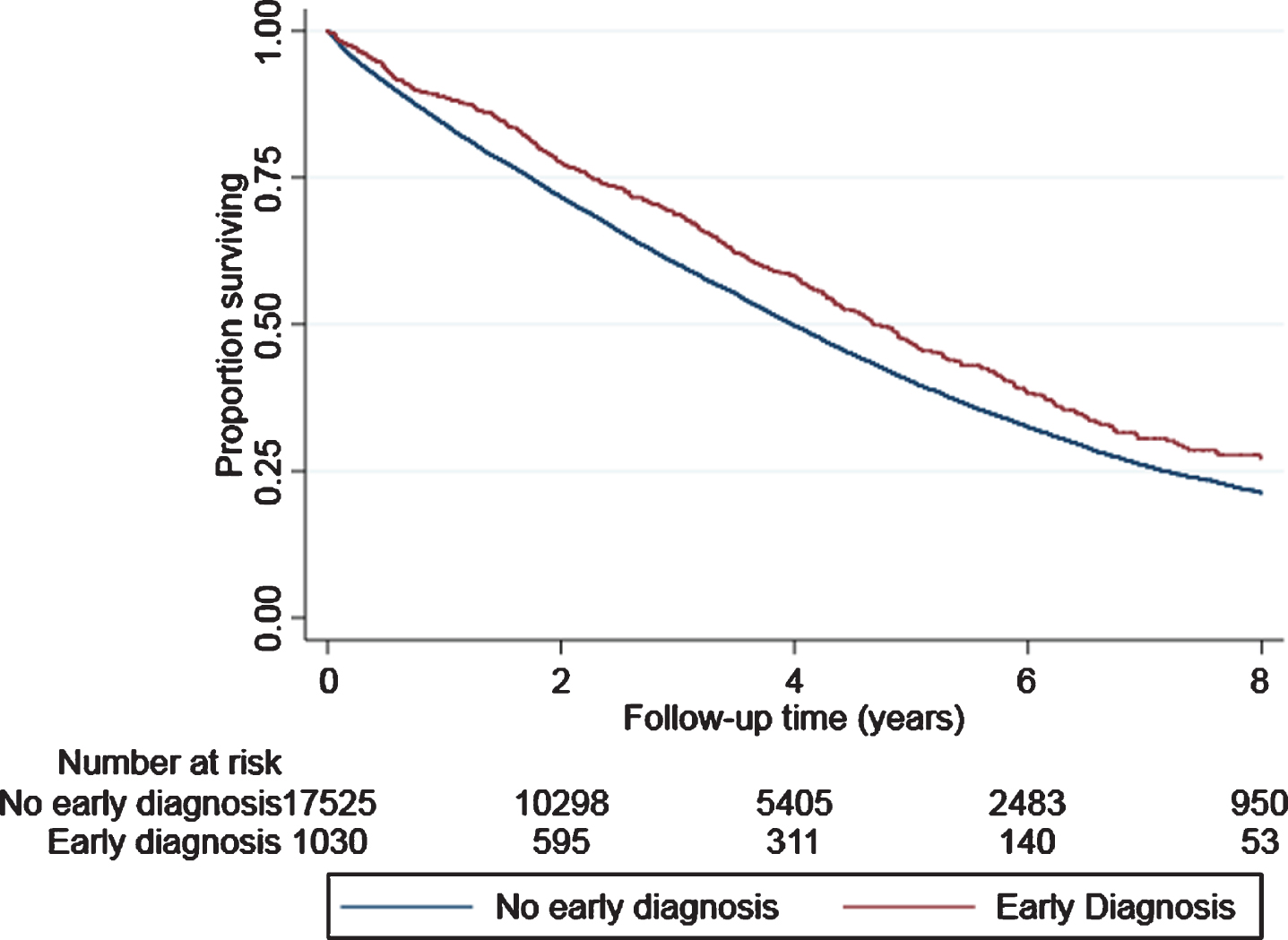
Kaplan-Meier curves comparing survival between a previous of mild cognitive impairment (Early diagnosis) and no previous diagnosis of mild cognitive impairment. Log-rank test: χ2 = 17.2, p < 0.01.
We used Cox regression models to further assess the relationship between an early diagnosis and mortality, and we added variables which were found to violate the proportional hazards assumption as time-varying covariates (Table 2). We ran 11 Cox regression models of increasing complexity, adjusting for a range of confounding factors, which showed the hazard of mortality was significantly lower in the early diagnosis groups in all but one of the models. The hazard ratios ranged between 0.77 and 0.92. A previous diagnosis of MCI remained a significant predictor of a lower mortality risk in models adjusting for demographics and physical illness, psychiatric symptoms, ADL problems, and prescription of AChEIs both individually and simultaneously (Model 9 HR = 0.86, CI = 0.77 –0.97). Associations remained significant when using HoNOS ratings to adjust for cognitive impairment (Model 10 HR = 0.87, CI = 0.78 –0.97). Supplementary Table 1 presents models using the full ordinal measure of HoNOS cognition. The hazard ratio for the fully adjusted model shows the same direction of effect as those presented in Table 2 (HR = 0.90, CI = 0.80–1.01, p = 0.07); however, it does not reach the threshold for significance where p = 0.05. When using the MMSE to account for cognition in a similar model, associations between a previous MCI diagnosis and mortality were attenuated and no longer significant (Model 11 HR = 0.92, CI = 0.83 –1.04).
Hazard ratios for the association between a previous diagnosis of mild cognitive impairment and mortality
ADL, Activities of Daily Living; AChEIs, acetylcholinesterase inhibitors; HoNOS, Health of the Nation Outcome Scales; MMSE, Mini-Mental State Exam. †Variables found to violate the proportional hazards assumption were added as time-dependent covariates. *p≤0.05.
DISCUSSION
In this study of electronic health records from 18,555 participants in routine secondary care, we found that a previous diagnosis of MCI can be used as an indicator to measure the effects of an early diagnosis or early help-seeking. We found 5.6%of all participants with dementia had previously received a diagnosis of MCI. People with a previous diagnosis of MCI had lower MMSE scores and fewer severe psychiatric symptoms at the time of dementia diagnosis, indicating that they were diagnosed in the earlier stages of the disease. We have found evidence to suggest there is an association between an early diagnosis of MCI and a lower risk of mortality; however, it is not clear how MMSE scores at diagnosis affect this relationship.
While only 5.6%of participants in our sample had a previous diagnosis of MCI, we have demonstrated that a diagnosis of MCI before dementia is a useful tool for measuring early diagnosis/early help-seeking for memory loss. Participants with a previous diagnosis of MCI had fewer psychiatric symptoms, less impaired cognition (both clinician and MMSE rated) and less impaired ADL at dementia diagnosis. Higher levels of cognitive decline and behavioral and psychological symptoms of dementia are associated with the later stages of the disease [27, 28]. In our sample, participants who received an early diagnosis were more likely to come from European backgrounds, compared with other ethnic groups. Surprisingly, people with an early diagnosis had higher levels of social deprivation. However, while statistically significant, a difference of 1 point between the groups may not be a clinically significant difference. Our findings indicate there may be systemic differences between those who received a diagnosis of MCI and therefore an earlier diagnosis of dementia. This is consistent with reports that people with MCI are largely a self-selecting group; most receive a diagnosis after requesting a memory assessment [29].
Participants in the sample had a median survival time of 4.0 years, and this is slightly less than other studies assessing mortality in dementia which reported average survival times of 5.7 years after diagnosis [3, 31]. Over half of the participants (55.74%) died during the study period. The risk of mortality was between 9–23%lower in participants with a previous diagnosis of MCI compared to those without when adjusting for a range of covariates. There was no statistically significant difference between groups when MMSE scores at dementia diagnoses were included in the Cox regression models (Model 11 HR = 0.92; CI = 0.83–1.04). However, models controlling for HoNOS rated cognitive impairment showed an early diagnosis was associated with a lower risk of mortality (Model 10 HR = 0.87, CI = 0.78–0.97). It is possible that the introduction of MMSE scores nullified the effects due to collinearity between MMSE scores and MCI diagnosis as, typically, a diagnosis of MCI in clinical practice is highly dependent on MMSE scores [32]. However, models containing the HoNOS measure of cognitive impairment may be lacking statistical power as this is a dichotomous variable, increasing the risk of a false-positive finding [33]. A sensitivity analysis found that models using the full HoNOS measure of cognition were attenuated but did not reach statistical significance. It would be interesting to investigate how cognitive impairment as rated by other measures affected the relationship between an early diagnosis and mortality. It was not possible to include other measures of cognition in this study, as the variables available for analysis were limited to what is routinely collected.
A greater proportion of people with a previous diagnosis of MCI were prescribed AChEIs within 6 months of their diagnosis of dementia (38.54%, compared with 31.45%). One of the proposed benefits of early diagnosis is access to earlier treatment [5–7, 14]. The findings of this study indicate that people with a previous diagnosis of MCI are more likely to be diagnosed with dementia in the earlier stages of the disease and are more likely to receive treatment with AChEIs at diagnosis. Although antidementia medications have been linked with a reduced risk for mortality and severe cardiovascular events in several observational studies [23, 35], it remains unclear whether this reflects a bias by indication or a direct effect of these medications. As antidementia medications are not appropriate for all people diagnosed with dementia [36], more research is needed to investigate the relationship between and early diagnosis of dementia and mortality related to pharmacological and non-pharmacological treatments.
Despite national initiatives to increase the diagnosis rate of dementia in the UK, only 60%of those with dementia have received a formal diagnosis [29]. The decision to seek help for suspected memory loss is complex. A lack of understanding of the causes and symptoms of dementia, the perception that nothing can be done to treat dementia and fear of stigmatization can deter people from seeking a diagnosis [37]. There is some evidence that expectations of support following a diagnosis differ between those seeking an early diagnosis for emerging memory problems and those seeking a diagnosis for the later stages of cognitive decline. Those seeking help for early-stage memory loss were more likely to proactively ask about treatment, most commonly medications [8, 38]. Therefore, any benefits of an early diagnosis may be due to proactive help-seeking behaviors rather than post-diagnostic support.
Additionally, people from black and minority backgrounds are less likely to seek timely help for memory problems. This is supported by our finding that white participants were more likely to have an early diagnosis. While we have found some evidence of the potential benefits of an early diagnosis, this remains limited to specific groups of people. Going forwards, it is imperative more research is conducted to understand the real-life benefits of an early diagnosis. This information could help people make a more informed choice about when to seek a diagnosis and the possible consequences. However, it is equally important to address systemic differences in diagnosis rates between different social and ethnic groups.
Strengths and limitations
In this study, we have developed a method to identify people with dementia that have early help-seeking behaviors. This method is easily replicable and can be applied to other hospital databases. The linkage of electronic health care records to a national mortality database allowed us to follow participants from diagnosis to death and excludes the risk of bias from inaccurate mortality records. Generally, studies which explore the progression of dementia or MCI have limited follow-up periods [14]. This study had a large sample size of 18,555 people living with dementia, drawn from a diverse population of patients in routine clinical care, increasing the generalizability of these findings.
There are limitations to this study, which should be considered. While we have shown that a previous diagnosis of MCI can be a helpful proxy for measuring early diagnosis and early help-seeking, it is not a perfect indicator. How the diagnosis of MCI is used differs between clinicians [39], and participants may have had a memory assessment before their diagnosis of dementia but were not diagnosed with MCI. Additionally, this study has used a large sample size; however, only a small group of participants had a previous diagnosis of MCI which affects the statistical power of our analysis. We have limited the effect of this by imputing missing data, to maximize the power of the data that was available to us. Additionally, this study used a cohort design, therefore there may be residual confounding which has not been controlled for.
Conclusions and future directions
In this study, we successfully used the prior diagnosis of MCI in people living with dementia as a proxy for early diagnosis/early help-seeking. Previously, there had been no studies which examined the reported benefits of early diagnosis or early help-seeking for people living with dementia, their caregivers or society, and many of the previously presumed benefits were dependent on the availability of disease-modifying treatments [15]. While we found that only a small percentage of participants received an early diagnosis, they presented a symptom profile associated with the earlier stages of dementia at diagnosis, were more likely to be prescribed ACHEIs and had a lower risk of mortality when adjusting for a dichotomized measure of clinician-rated cognitive impairment. However, this effect was attenuated but no longer significant when using a more sensitive measure of cognition. These findings are promising; however, they are not conclusive on the benefits of an early diagnosis. More research is needed to better understand the association between an early diagnosis and mortality and other long term outcomes.
Footnotes
ACKNOWLEDGMENTS
We thank Hitesh Shetty from King’s College London and Megan Pritchard from South London and Maudsley NHS Foundation Trust for their assistance with data extraction.
EC is supported by a studentship from ESRC LISS-DTP.
CRIS is supported by the NIHR Biomedical Research Centre for Mental Health BRC Nucleus at the South London and Maudsley NHS Foundation Trust and Institute of Psychiatry, Psychology and Neuroscience, King’s College London jointly funded by the Guy’s and St Thomas’ Trustees and the South London and Maudsley Trustees.