
Abstract
Degenerative dementia, of which Alzheimer’s disease is the most common form, is characterized by the gradual deterioration of cognitive function. The events that trigger and promote degenerative dementia are not clear, and treatment options are limited. Experimental and epidemiological studies have revealed chronic noise exposure (CNE) as a potential risk factor for cognitive impairment and degenerative dementia. Experimental studies have indicated that long-term exposure to noise might accelerate cognitive dysfunction, amyloid-β deposition, and tau hyperphosphorylation in different brain regions such as the hippocampus and cortex. Epidemiological studies are increasingly examining the possible association between external noise exposure and dementia. In this review, we sought to construct a comprehensive summary of the relationship between CNE, cognitive dysfunction, and degenerative dementia. We also present the limitations of existing evidence as a guide regarding important prospects for future research.
INTRODUCTION
Dementia is a general term for conditions involving cognitive dysfunction, with symptoms that include impaired learning and memory, behavior and personality changes, and altered thinking and language. Dementia can be divided into non-degenerative and degenerative dementia. Alzheimer’s disease (AD), which makes up 60%to 80%of all dementia cases, is the most common form of degenerative dementia [1]. The pathological signs of AD are neuritic plaques and neurofibrillary tangles in brain tissues, which are respectively related to the accumulation of amyloid-β (Aβ) and cytoskeletal changes caused by the hyperphosphorylation of tau in neurons [2, 3].
In 2016, more than 43 million people had been diagnosed with dementia globally, making it the fifth leading cause of death [4]. While Turkey and Brazil had the highest prevalence of dementia, Mainland China had the greatest number of cases, with more than 10 million people diagnosed with various types of dementias [4]. In terms of AD specifically, a recent US report showed that more than 5.8 million people over the age of 65 had AD, and this number was predicted to grow to 13.8 million by the middle of the century [5]. Indeed, as the population grows and ages, the global number of people with dementia may continue to grow in the next few decades.
The events that trigger and promote degenerative dementia are still unknown. Degenerative dementia is currently thought of as a heterogeneous disease influenced by a combination of multiple factors such as diet, lifestyle, physical activity, sleep, genetics, and cardiovascular disease [3, 6–10].
Recent studies have indicated that noise might accelerate the risk of degenerative dementia, especially AD in late life. Based on findings from previous research, Cui et al. [11, 12] put forward a hypothesis regarding the role of chronic noise exposure (CNE) in the risk of degenerative dementia and launched a series of associated experiments. Further, Jafari et al. [13] summarized evidence on the relationship between noise, cognition, and neuropathology collected during animal studies. In addition, several reviews and comments have briefly mentioned the possible relationship between noise and dementia [14–17].
For most people living in urban settings, noise is a ubiquitous part of the environments in which we live and work. One report found that approximately 22 million workers in the US were exposed to hazardous occupational noise, based on self-reported exposure [18]. Further, more than 1.1 million workers were exposed to noise at levels above the daily occupational exposure limit (85 dB) in Australia [19]. Apart from hearing loss, noise can contribute to a series of health problems such as metabolic syndromes [20–22], cardiovascular disease [23, 24], sleep problems [25, 26], anxiety [27], and depression [28]. In this review, we intended to generate a comprehensive summary of the relationship between CNE, cognitive dysfunction, and degenerative dementia. We also sought to identify the limitations of existing evidence in terms of testing this association, and to propose prospects for future research.
METHODS
We performed a search of PubMed, EMbase, and Web of Science from inception to 31 October 2020 to identify relevant studies on CNE and cognition or degenerative dementia. We combined both medical subject headings (MeSH) and free text terms to identify relevant articles. Our search strategy in the PubMed database was as follows: ((noise) OR (sound)) AND ((spatial learning) OR (spatial memory) OR (learning and memory) OR (cognition) OR (cognitive) OR (hippocampus) OR (dementia) OR (Alzheimer’s disease) OR (AD)) in all fields. This strategy was adjusted for use with other databases. References from relevant articles, including review articles, were also examined for additional information.
The inclusion criteria of this study were as follows: 1) Type of study: original studies on CNE and cognitive impairment, degenerative dementia; 2) Object: humans or animals; 3) Exposure factors: CNE. Literature with the following characteristics was excluded: 1) Editorials, reviews, letters, proceedings, meeting reports, and books; 2) Literature in which acute or short term noise exposure (less than 1 day) was used to induce hearing loss in objects [29–32]; 3) Studies purely concerned with hearing loss or age related hearing loss (ARHL) rather than noise-based stressors.
EXPERIMENTAL STUDIES
The noise types on which the experimental studies were focused mainly included traffic noise (aircraft noise, urban traffic noise, and railway noise) and white noise (WN). Various types of noise stressors have been recently found to induce cognitive dysfunction and neuropathology in different brain regions such as the hippocampus, prefrontal cortex (PFC), and auditory cortex.
CNE and early cognitive impairment
Traffic noise (75 dBA, 8 h/d, 30 d) was reportedly associated with hypothalamic-pituitary-adrenal (HPA) axis hyperactivity, anxiety-like behavior, impaired learning and memory, and balance and motor coordination dysfunction [33]. Further, long-term high-speed railway noise (HSRN, 70 dBA) and combined traffic noise (CTN, 70 dBA), which included HSRN and highway noise, were reported to impair learning and memory function in the temporal lobe [34, 35]. In contrast, short-term CTN only produced stimulating effects and increased glutamate levels in the hippocampus [36].
Uran et al. [37] discussed the effect of both acute and sub-acute noise and found that sub-acute noise (SANE, WN, 95 to 97 dB, 15 d) appeared to lead to behavioral changes and could serve as an index of oxidative stress abnormalities. Further, oxidative stress values tended to normalize in the sub-acute group compared with the acute group. In another study by the author, the same research group observed mild noise-based disruptions in hippocampal regions (total cells increased in CA3 and dentate gyrus, and pyknotic cells increased only in CA3) [38], indicating that hippocampal cells underwent necrosis or apoptosis.
In addition, studies indicated that CNE (WN, 100 dB, 4 h/d, 30 d) might not only impair early spatial learning and memory but could also harm Nissl bodies and reduce expression of N-methyl-D-aspartic acid receptor 2B (NR2B) [11, 39]. However, another study conducted by the author showed that acute noise exposure caused an increase in NR2B expression [30], indicating that subjects may have adapted to chronic long-term stimulation after a transient rise in NR2B expression. Similar noise exposure paradigms were also found to lead to impaired spatial memory [40] and a decreased dendritic count in the hippocampus [41].
Cognitive dysfunction was also observed in experimental studies that focused on gestational noise stress and prenatal noise stress. Gestational noise stress was revealed to have adverse effects on the HPA axis and spatial learning and memory after giving birth [42], and also to accelerate postpartum cognitive decline and increases in Aβ deposition, which are potential risk factors for AD-like neuropathological changes [43]. Furthermore, prenatal noise stress also negatively impacted cognitive function, learning and memory performance, and synaptic activity in the offspring [44–47]. Early neuropathological changes were also observed, with females showing higher susceptibility [48, 49].
CNE and late neuropathological changes
Neuropathological changes, especially the deposition of tau protein, are generally considered to be more closely related to AD-related cognitive decline than other markers [50] and usually occur in the middle and late stages of AD [51]. Even low intensity noise (WN, 80 dB, 1, 3, or 6 w) was found to induce tau hyperphosphorylation in the hypothalamus and auditory cortex, along with peroxidative damage (decrease in the superoxide dismutase/malondialdehyde ratio) and alterations in auditory coding, with the most obvious changes occurring in the hippocampus [52, 53]. Studies using other noise exposure paradigms also observed similar changes, such as Aβ deposition, tau hyperphosphorylation, and neurogenesis reduction or apoptosis in the hippocampus, with corresponding increases in cognitive dysfunction [54–59].
Other findings
Delayed and cumulative effects
The surveyed studies indicated that CNE had cumulative effects on the triggering and development of AD. For instance, CNE-induced Aβ deposition, increases in non-NFT hyperphosphorylated tau, and delayed formation of misfolded NFT tau in the hippocampus and PFC persisted for 7–14 days after exposure [56]. In addition, Aβ accumulation was accompanied by up-regulated expression of amyloid-β protein precursor (AβPP) and its cleavage enzymes, β- and γ-secretases [55]. Park et al. extended the follow-up period from 6 months to 12 months, and observed progressively worsening cognitive performance, tau hyperphosphorylation, and lipofuscin (markers of aging) in the hippocampus [57, 60].
Recovery trend
Although CNE caused various adverse changes in the hippocampus and auditory cortex, such as excitotoxicity, inflammation, psychological stress, and oxidative injury, these markers showed a time-dependent recovery pattern when noise stress was terminated [37, 61]. It could be inferred that the subjects may have adapted to the external stimulation. However, the normalization trends of the biomarkers usually along with continuous cognitive dysfunction and progressively worsening situation in the hippocampus, indicating that noise stress either acts as a trigger or induces hearing loss to cause further pathological changes.
Interaction effect
CNE may disturb the expression of characteristic genes as well as interact with genetic factors in AD-like neuropathology. Combined exposure of noise and Apolipoprotein E ɛ4 (APOE ɛ4) might activate mTOR signaling, which could lead to Aβ deposition and the acceleration of AD-like changes [62]. Senescence Accelerated Mouse-Prone 8 (SAMP8) mice, which are an excellent model of early learning and memory problems [63], were used to study the synergistic effects with CNE. The researchers reported that CNE could accelerate the cognitive decline and AD-like neuropathology of SAMP8 mice, and that these changes could be related to dysfunction in the microbiome-gut-brain axis and Wnt signaling pathway [64, 65]. In addition, CNE could induce up-regulation of Arc, Egr1, Egr2, Fos, Nauk1, and Per2 in SAMP8 mice, indicating that gene-environment interactions might be one of the underlying mechanisms that trigger or exacerbate AD [66]. Another study focused on genetic susceptibility to AD and hearing loss also confirmed this association in another way [67].
Discussion regarding underlying mechanisms
Various researchers have examined the possible mechanisms of the relationship between noise exposure and AD and put forward hypotheses. Here, we summarize the possible pathways by which noise exposure might lead to cognitive dysfunction and dementia (Fig. 1).
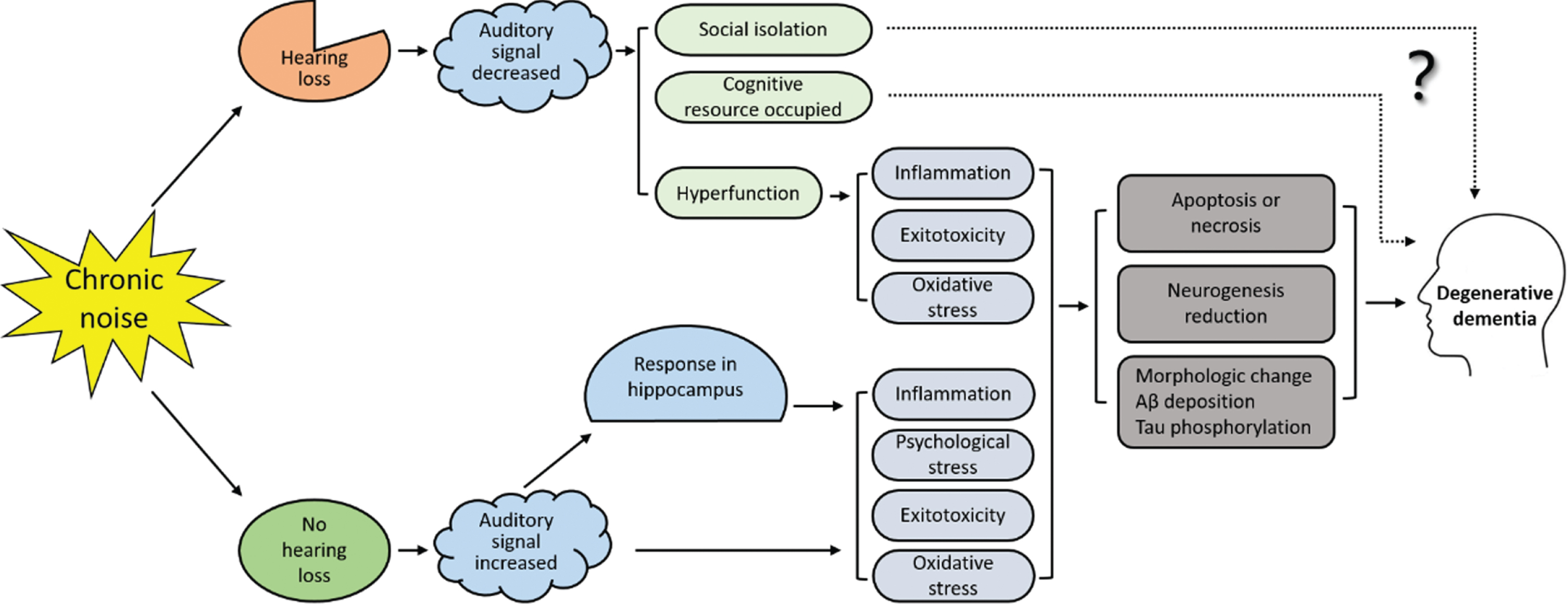
The paths by which noise exposure may lead to cognitive dysfunction and dementia. Chronic noise exposure may cause hearing loss. In the ‘hearing loss pathway’, noise-induced hearing loss leads to social isolation, occupied cognitive resources, and hyperfunction of the auditory cortex and hippocampus. However, the underlying mechanisms by which social isolation and cognitive resource shortages lead to dementia are unclear. In the ‘no hearing loss pathway’, excessive stimulation leads to neuroinflammation, excitotoxicity, psychological stress, and oxidative stress injury in the auditory cortex and hippocampus. These changes further lead to a reduction in neurogenesis, necrosis or apoptosis, Aβ deposition, and tau hyperphosphorylation. Eventually these changes may result in degenerative dementia.
First, several authors suggested that CNE might activate the HPA axis [33, 46] and the corticotropin-releasing factor (CRF) system [68, 69], and then upregulate secretion of CRF, glucocorticoids, and corticosterone, which are the psychological responses to external stress. In this model, CNE-induced psychological stress might accelerate changes in redox state, and thus contribute to the hyperphosphorylation of tau and corresponding AD-like changes in the hippocampus.
Second, the Glu-NMDAR signal pathway was found to be involved in tau hyperphosphorylation and early noise-induced spatial memory impairment [70]. Noise exposure could cause significant changes in NMDAR expression especially in NR2B and lead to upregulation of glutamate [11, 39]. Elevated glutamate is known to have the potential to cause excitotoxicity, and excessive glutamate signaling could lead to changes in the redox potential of neurons [71], which might further induce tau hyperphosphorylation and neural apoptosis in the hippocampus.
Third, the elevated expression of proinflammatory cytokines and microglial activation, which are features of neuroinflammatory responses, were observed in the auditory cortex and hippocampus after noise exposure [72, 73]. Indeed, many studies have suggested that hearing loss could induce neuroinflammatory responses in different brain regions [74, 75]. Persistent neuroinflammation has been associated with many psychological and neurological disorders [76, 77]. Although current studies cannot answer whether is the effect of noise itself, noise-induced hearing loss (NIHL), or even both, inflammation in the auditory cortex and hippocampus does exist.
It is worth noting that none of the above-cited studies produced sufficient evidence to determine whether it is the effect of noise itself or NIHL that mediates the relationship between CNE and cognitive impairment. From the perspective of mechanism research, the current research failed to distinguish the effect of noise and hearing loss perfectly.
In those studies which focused on hearing loss, nearly all of the studies used external noise to induce hearing loss in rodents. There were a few exceptions, such as bilateral cochlear ablation [78] and hereditary hearing loss [79]. However, the above two studies also observed consistent changes such as cognitive impairment, impaired synaptic plasticity, and excitotoxicity in the hippocampus [78, 79], indicating that hearing loss was independent risk factor for dementia. Indeed, many epidemiological studies have confirmed that hearing loss, especially ARHL, is significantly related to cognitive impairment and dementia [80–84]. Several hypotheses were proposed to explain the correlation between hearing loss and dementia. These include hearing loss-induced sensory deprivation and social isolation leading to accelerated cognitive impairment [85, 86], depleted cognitive resources (resources were used to deal with auditory signals rather than non-auditory signals) [87], and increased nerve fragility such as elevated susceptibility to Aβ-induced damage [78]. The above explanations indicate that forms of hearing loss such as ARHL, tympanum damage, and cochlea damage rather than NIHL might also accelerate cognitive dysfunction.
Yet, another theory holds that central auditory dysfunction rather than conductive hearing loss (relatively undamaged pure tone thresholds) is the culprit leading to cognitive deterioration [88–90]. Noise-induced peripheral hearing damage is well known to be positively correlated with noise intensity and/or dose. Indeed, many studies using lower-intensity noise exposure paradigms [33–36, 53] observed cognitive changes similar to those seen with high-intensity noise, indicating that noise could cause damage in the auditory cortex or hippocampus via non-hearing damage pathway. Researchers have summarized how auditory signals reach the auditory cortex and hippocampus [91], and further pointed out that the hippocampus is more susceptible to noise stress than the auditory cortex [53, 92].
In summary, several hypotheses have been proposed regarding the mechanisms of noise exposure, cognitive dysfunction, and dementia, although the evidence is insufficient to draw a conclusion. First, whether it is the noise pressure or peripheral hearing loss induced by noise that leads to neuronal damages is not clear. Current evidence suggests that the two may coexist. Second, the way in which abnormalities such as neuroinflammation, psychological stress, changes in redox state, and excitotoxicity after noise exposure cause neuropathological changes in the hippocampus (as triggers or persistent exacerbation) has yet to be determined. That some early changes seem to be able to recover in chronic exposure models while cognitive dysfunction and neuropathological changes are often continuous and non-recoverable indicates that further mechanism research is warranted.
EPIDEMIOLOGICAL STUDIES
CNE and early cognitive impairment
Laboratory experiments with humans showed that noise exposure significantly impacted short-term learning and memory as well as work performance. For instance, one study found that when the noise level reached 68 dBA, the number of work errors increased along with the reaction time (RT) [93]. Noise conditions such as those found in an open office or industrial workplace had adverse effects on work performance and learning and memory [94–96]. In addition, combined noise events including nocturnal airplane, road, and rail traffic noises had a similar effect, especially in terms of RT, which showed a small but significant increase [97]. Another study found that nocturnal aircraft noise (45 to 80 dBA) led to an increase in Psychomotor Vigilance Task time (0.3 ms/dB) [98]. However, Sandrock et al. [99] found no association between noise and learning and memory, although individuals with high noise sensitivity reported more annoyed and exhibited poorer performance compared with those with low sensitivity.
Cross-sectional studies confirmed the above observations and further revealed that CNE might cause early cognitive and neuronal dysfunction. The researchers reported that CNE had a negative effect on attention [100] and event-related potentials [101] in adults. Noise-induced cognitive impairment has also been verified in groups of women [102], elderly individuals [103], and industrial workers [104]. Further, noise has been found to have negative effects on school-age children in terms of annoyance, study performance, and cognitive function [105, 106]. Clark et al. [107] reviewed the related literature and proposed that aircraft noise appears to have a tangible effect on learning and long-term memory, but a minimal effect on attention and executive function. In addition, Tzivian et al. [108, 109] pointed out that traffic noise may not only lead to poor performance in terms of global cognitive score, but may also have an interactive effects with air pollutants.
Certain occupational groups may experience specific noise-related changes in cognitive function. One study of individuals in the Norwegian Navy showed that RT was significantly higher in those subjected to high noise exposure. Compared with control group (<72.6 dBA), the RT of individuals in two exposure groups (77.1–85.2 dBA and >85.2 dBA) was increased by 23.8 ms and 24.6 ms, respectively [110]. Zeydabadi et al. found that occupational noise exposure (≥85 dBA) not only led to hearing loss, but also adversely affected RT, attention, and memory [111]. Another study found that pilots exhibited working memory deficits, as well as decreased grey matter volumes, regional homogeneity, and amplitudes of low-frequency fluctuation signals in the left hippocampus, indicating the presence of early noise-induced neuronal dysfunction [112].
CNE and degenerative dementia
Most epidemiological studies that were assessed focused on the relationship between urban traffic noise and different types of dementia. For instance, they often sought to estimate the risk ratio (RR) or hazard ratio (HR) of individuals with AD and other forms of dementia using different strategies to evaluate noise levels at specific residential addresses.
A cross-sectional study in Germany showed that traffic noise exposure was associated with mild cognitive impairment (MCI) in adults, and that RR corresponded with LDEN and LNIGHT (measured in incremental 10 dB increases in noise) values of 1.40 (1.03, 1.91) and 1.80 (1.07, 3.04), respectively [113]. A study by Weuve et al. produced a similar result, with incremental increases of 10 dBA corresponding to 36%and 29%increases in the odds of developing MCI and AD, respectively [114]. However, another study reported no relationship between noise, cognitive function, and AD [115]. This discrepancy may be due to differences in the ways that noise levels or doses were estimated, such as noise prediction models versus official reports.
A longitudinal Spanish study reported no association between emergency admissions in AD patients and traffic noise (RR and HR were not mentioned) [116]. Another article on dementia-related emergency hospital admissions indicated that traffic noise might exacerbate dementia symptoms, corresponding to a RR (1 dB increase each) of 1.15 (1.11, 1.20), but did not mention the type of dementia [117]. In those two studies, disease-related medical events were used to represent the dependent variable rather than a measure of symptoms. A longitudinal study in elderly individuals found no association between traffic noise exposure and dementia, but no distinction was made between AD and vascular dementia (VaD) [118]. Another retrospective cohort study conducted by Carey yielded no association between traffic noise and AD but did not rule out the possible impact of air pollutants [119]. Finally, in contrast to the above findings, one study found that excessive occupational noise exposure could reduce the risk of AD (RR 0.12 (0.02, 0.96)), but the researchers did not mention the actual noise exposure level or dose [120].
Several studies have used the distance from a residence to a road or road proximity rather than noise level to explore the relationship between noise, AD, and other forms of dementia. A cohort study concluded that living a shorter distance from a road was associated with a higher risk of dementia [121]. Another study analyzed both traffic noise and road proximity and reached a similar conclusion [122]. However, these data are insufficient to establish a comprehensive link between noise exposure and dementia.
Discussion regarding epidemiological investigations
From the perspective of etiology, epidemiological evidence is very important. However, as stated by several researchers, the current studies failed to provide the required evidence to link noise exposure to AD or cognitive decline [14, 16].
Among the examined epidemiological studies, there are several important limitations in terms of demonstrating an association between noise and dementia: 1) Few studies focused on the relationship between noise and degenerative dementia. Studies were either concerned with air pollution, with noise as a secondary factor, or used the distance to a road or road proximity to measure exposure without reporting the specific noise level or dose. 2) Study populations and noise characteristics were not typical. The examined studies mainly focused on community populations and residential noise, and groups with higher noise doses and more typical exposure characteristics in the workplace were seldom the study population. 3) Imprecise dose assessment. Many studies used a traffic noise exposure prediction model to evaluate noise, in which data were based on traffic flow and speed, geographic information, building size, street distribution, and distance. While such models are convenient, they may be accompanied by biases regarding population migration, traffic changes, and additional occupational exposure. Changes in the above variables are inevitable and can be difficult to evaluate over a period of 20–30 years. 4) Ambiguous outcome variables. Whether disease-related medical events (such as hospital admission records, outpatient records, and emergency records) can be used to represent disease remains to be determined. In studies that used dementia as an outcome variable, no distinction was made between degenerative dementia and non-degenerative forms of dementia such as vascular dementia, although these usually have different pathogeneses. 5) NIHL and its underlying effects on dementia were not covered in any of the epidemiological studies examined.
Experimental studies on noise and cognitive function, degenerative dementia
AD, Alzheimer’s disease; ANE, acute noise exposure; Aβ, amyloid-β; CRF, corticotropin-releasing factor; CTN, combined traffic noise; GDs, gestational days; GNS, gestational noise stress; HPA axis, hypothalamic-pituitary-adrenal axis; HSRN, high-speed railway noise; ISI interstimulus interval; NFT, neurofibrillary tangles; NIHL, noise-induced hearing loss; PFC, prefrontal cortex; PNS, prenatal noise stress; SANE, sub-acute noise exposure; WN, white noise.
Epidemiologic studies on noise and cognitive function, degenerative dementia
AD, Alzheimer’s disease; ALFF, amplitudes of low-frequency fluctuation; CO, closed offices; CR, control rooms; GCS, global cognitive score; GMVs, grey matter volumes; HR, hazard ratio; IW, industrial workplaces; LAeq, equivalent noise level; LDEN, Weighted 24-h Mean Noise; Leqd, Equivalent Diurnal Noise Level; Leqn, Equivalent Nocturnal Noise Level; LNIGHT, Night Time Noise; LPALF, large pressure amplitude and low frequency; MCI, mild cognitive impairment; MRI, magnetic resonance imaging; MS, multiple sclerosis; NAD, non-Alzheimer’s dementia; OPO, open-plan offices; PD, Parkinson’s disease; PVT, Psychomotor Vigilance Task; QC, quiet conditions; ReHo, regional homogeneity; RR, risk ratio; RT, reaction time; SPL, Sound Pressure Level; VaD, vascular dementia.
PROSPECTS FOR FURTHER RESEARCH
In-depth investigations of underlying mechanisms
The effects of noise and NIHL could not be well distinguished in most of the current studies examined, and so the design of future studies should be conducted with this in mind. For example, hearing loss could be more directly induced in animal models rather than using noise stress in studies which purely focused on hearing loss and cognitive dysfunction. In contrast, low-intensity and long-term noise exposure paradigms are more suitable for studies concerned with non-hearing damage mechanisms. Research examining the role of CNE in the triggering or persistent exacerbation of dementia is also needed.
Accumulation of noise and gradual development of dementia
Degenerative dementia is a type of disease that develops chronically. Symptoms of cognitive impairment usually appear in middle-aged or elderly individuals and may develop over a span of 20–30 years or even longer. Whether it is environmental noise or occupational noise, it may last for very long periods, even including an entire professional career. Therefore, long-term continuous studies should be carried out to explore the etiological link and underlying mechanisms of CNE-induced impairments.
The importance of workplace and related noise exposure
Compared with traffic noise and residential noise, noise in the workplace is often louder and more consistent, leading to more serious health implications. Thus, research in this field is urgent and also of great significance for protecting workers. On the other hand, noise levels or doses in the workplace can be easier to measure and evaluate compared with traffic or residential noise, and the confounding factors may be easier to distinguish and control, which is advantageous for tracing etiology. In addition, prevention and intervention measures are often more feasible and cost-effective among occupational groups.
Minimize bias and distinguish the effect of noise and NIHL
Although experimental studies have provided sufficient evidence to indicate an association between noise exposure and AD-like neuropathology, they have failed to explain the role of noise stress and hearing loss (NIHL and ARHL). Exploring this issue from an epidemiological perspective may have numerous advantages, such as the representativeness of conducting longitudinal studies with specific populations and the accuracy of assessing noise exposure and pure tone thresholds.
Interaction effect
Degenerative dementia is a heterogeneous disease with multiple genetic factors. While experimental studies have suggested that noise and genetic factors might have interactive effects in dementia and AD-like neuropathology, this has not been verified by epidemiological studies. Examining the interaction effects of noise and specific genes associated with dementia may have important implications regarding the pathogenic mechanisms of AD and cognitive decline.