
Abstract
In a woman with Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL) followed for 15 years, we observed magnetic resonance imaging white matter hyperintensities that vanished in the anterior temporal poles while the brain volume decreased unexpectedly. These imaging changes were transient and detected when the patient was being treated by valproic acid for stabilizing mood disturbances. This intriguing case supports that mechanisms underlying white matter hyperintensities can vary from one brain area to another and that important modifications of water influx into the brain tissue might be involved in some imaging features of CADASIL.
INTRODUCTION
White matter hyperintensities (WMH) on T2-wei-ghted or FLAIR magnetic resonance imaging (MRI) are the most striking imaging marker of Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL) [1]. They are detected early during the course of the disease, even decades before clinical manifestations. More specifically, WMH in the anterior temporal lobes are a recognized imaging hallmark of CADASIL [2]. The same areas are usually free of lesions in the most common forms of cerebral small vessel disease. Obviously, the larger burden of WMH in CADASIL cannot explain this discrepancy [3]. In contrast with hyperintensities located in other brain areas, WMH in the anterior temporal lobes have higher water contents [4] and appear associated with larger brain volumes in CADASIL [5, 6]. Recent data also suggest that their presence in the temporal poles is associated with milder forms of the disease [6]. We report a singular CADASIL case with a long-term follow-up in whom WMH, particularly in the anterior temporal lobes, vanished while the brain volume decreased rapidly. These lesions reappeared later as the brain volume increased again. This observation further supports that the substrate of some WMH in this genetic model of small vessel disease cannot be ascribed to only consequences of chronic hypoperfusion.
MATERIALS AND METHODS
This woman was enrolled in 2003 in an ongoing cohort study of genetically confirmed CADASIL patients from the French national referral center of rare cerebrovascular disease (http://www.cervco.fr). All patients were prospectively evaluated with systematic clinical, biological, and MRI investigations obtained every 18–24 months [7]. A specific MRI protocol with imaging sequences allowing fine volumetric measures of the whole brain and of WMH was used [7]. To ease the comparison of WMH across different acquisitions despite different head positions in the MRI scanner, the FLIRT algorithm of the FSL suite was used to register all FLAIR and 3DT1 high resolution scans in the space of acquisition of the first MRI scanner [8]. SIENAX, a validated tool, was used to estimate the brain volume at different visits from 3DT1 high resolution acquisitions [9]. A written informed consent was obtained and the study was authorized by an independent ethics review board.
RESULTS
This woman was enrolled at age 50 years and was evaluated 8 times both clinically and according to the specific MRI cohort-study protocol until September 2017. Her main medical history at time of inclusion was only that of several major depressive episodes for which she received sequentially only serotonin reuptake inhibitors (escitalopram, fluoxetine, and paroxetine). In July 2011, she attempted suicide a few weeks after she stopped her antidepressant medication. Soon after, she developed a manic episode. A diagnosis of bipolar disorder was made and a treatment with valpromide 900 mg was initiated and subsequently increased to 1,200 mg/day. In late 2013, a latent pulmonary tuberculosis was diagnosed and a treatment combining isoniazid, rifampicin, and pyrazinamide was initiated. In February 2014, she presented a manic relapse, attributed to the interaction between valpromide and anti-tuberculous medications. Valpromide was then stopped and replaced by lithium. The patient did not report any stroke event and her blood pressure was stable during the entire follow-up period (always inferior to 120/75).
Her brain FLAIR acquisitions, registered in the space of the first MRI, are presented on Fig. 1. As previously reported after the age of 50 years in CADASIL [10, 11], her brain volume decreased progressively during the 2003-2010 period, with a yearly rate of 0.7%. Between 2010 and 2012, her brain volume decreased more abruptly by 6.7% (yearly rate of 3.3%). This was followed by a lower yearly rate of 1% until 2014. Between 2014 and 2015, her brain volume unexpectedly increased by 4.5% (2.2% a year), and restarted decreasing by 0.3% each year thereafter (Fig. 2).
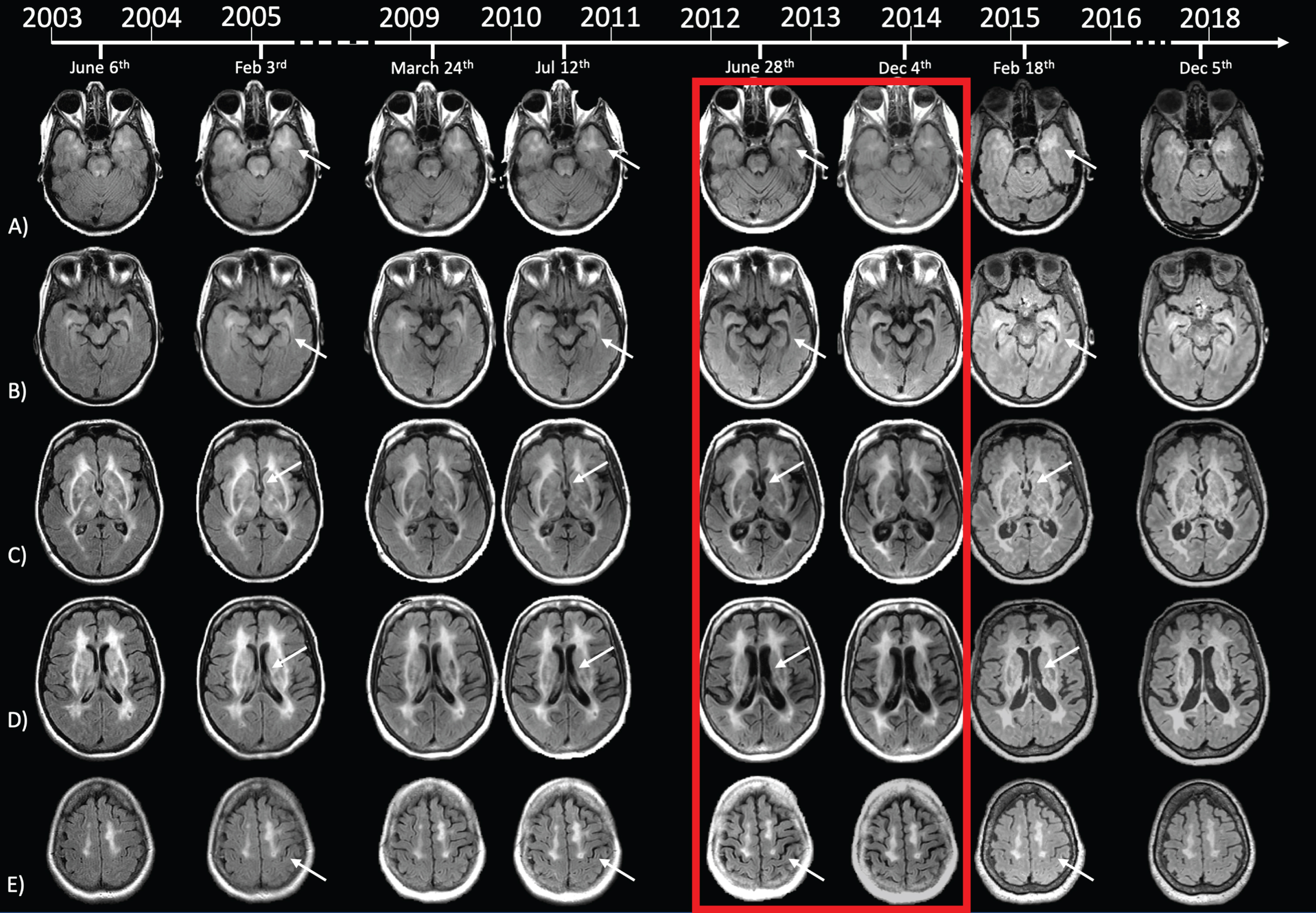
Evolution of brain MRI during 15 years of follow-up. FLAIR scans obtained at each evaluation, registered in the space of the inclusion MRI to ease comparisons. The red box corresponds to the two MRI scans that were performed while the patient was taking valpromide, where white matter hyperintensities in anterior temporal poles vanished. Note the concomitant drastic reduction of brain volume, obvious in temporal horns. This also affected, to a lesser extent, the bulk of lateral ventricles and the cortical structure, with opening of cortical sulci on the vertex. In total contrast, MRI scans in 2015 and 2017 showed reappearance of white matter hyperintensities in anterior temporal poles with concomitant re-increase of brain volume.
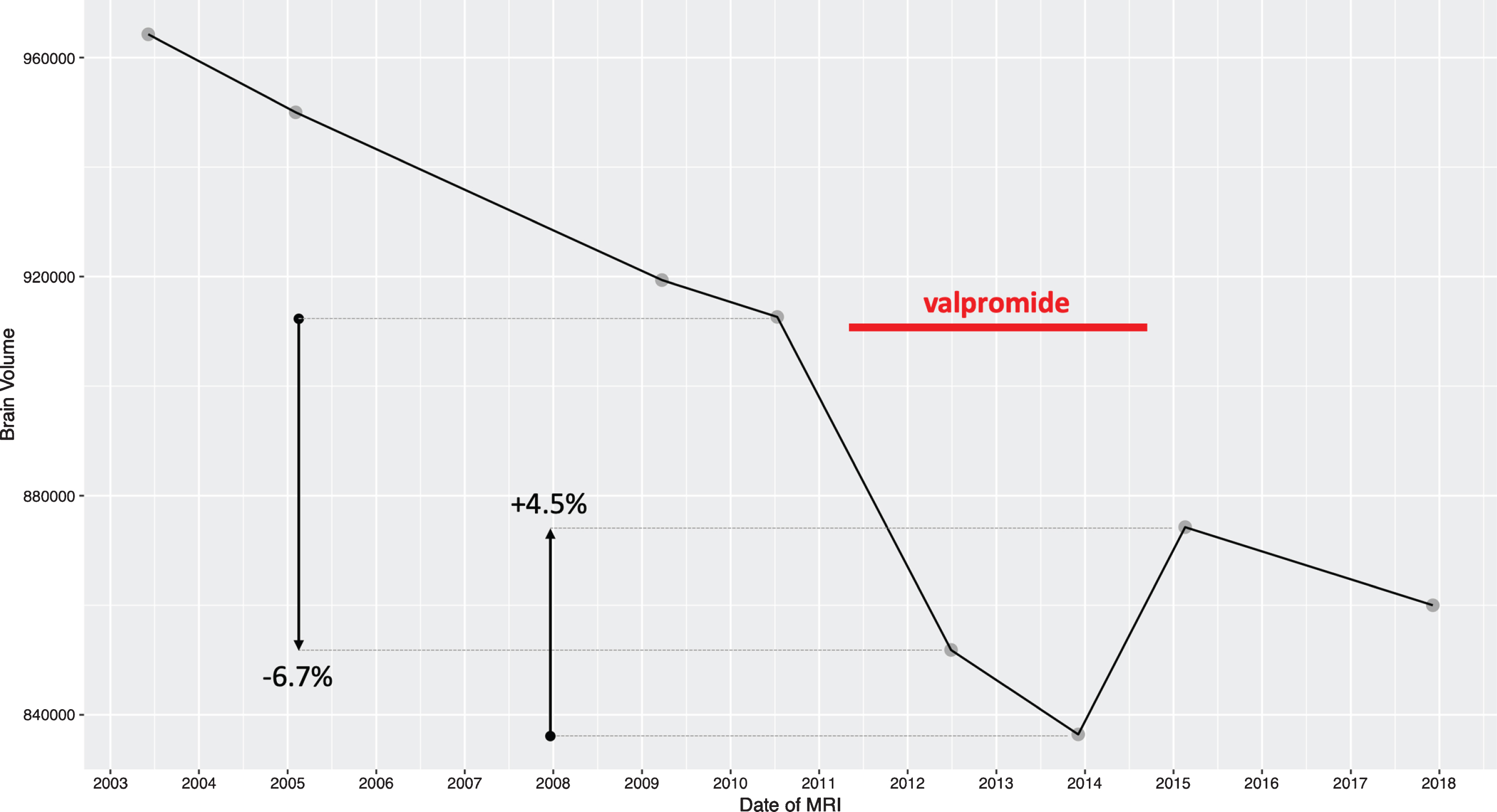
Evolution of brain volume during 15 years of follow-up. Brain volume measures obtained from 3DT1 scans at each evaluation. In contrast to a brain volume decrease of 0.7% /year or less before 2010 and after 2015, valpromide intake was associated with a drastic reduction of brain volume of 6.7% in 2 years. After valpromide was changed for lithium, brain volume increased by 4.5%.
DISCUSSION
In this CADASIL case, a massive reduction of WMHs was detected on FLAIR images twice out of 8 repeated MRI examinations obtained over a 15-year follow-up. These changes were prominent in the white matter of temporal lobes, particularly in periventricular and polar areas. They were observed parallel to an obvious enlargement of lateral ventricles. Volumetric measures confirmed a major and global shrinking of the whole cerebral volume during the same time-frame. This latter phenomenon was unexpected, largely exceeded the continuous atrophy process previously depicted and reversed totally on the two latest examinations. These imaging changes were detected in the absence of significant blood pressure changes and exactly when the patient was treated by valproic acid. Only large variations of the water content in the cerebral tissue could explain these major structural changes. White matter lesions in the temporal lobes are mainly related to the accumulation of dilated perivascular spaces with major structural alterations of astrocytes in CADASIL [12]. A retraction of the astrocytes end-feet containing multiple aquaporin 4 water channels and encircling cerebral microvessels was recently reported postmortem in the white matter of CADASIL patients, predominantly within anterior temporal lobes [13]. On the other hand, experimental studies already showed that several antiepileptic drugs including valproic acid can inhibit aquaporin 4 functioning and reduce in vitro hypoosmotic volume changes of oocytes [14]. The present observation supports that water influx in the cerebral tissue may be significantly altered in CADASIL, could participate to the pathophysiology of MRI lesions and are possibly modulated by a pharmacological agent. Further investigations are obviously needed to test this hypothesis.
Footnotes
ACKNOWLEDGMENTS
This work was supported by grants from Assis-tance Publique-Hôpitaux de Paris (Contrat de Rer-cherche Clinique (CRC) 16170) and the Agence National de la recherche (ANR) (Ministry of Health and Research (Commissariat General à l’Invest-issement), Recherche Hospitalo-Universitaire (RHU - TRT_cSVD).