
Abstract
Background:
Odor identification dysfunction occurs early in Alzheimer’s disease (AD) and is considered a preclinical symptom along with subjective cognitive decline (SCD). Nevertheless, whether subjects with SCD are co-symptomatic with odor identification dysfunction remains unclear.
Objective:
To compare the degree of odor identification dysfunction and assess the relation between odor identification and cognitive performance in the AD spectrum (including SCD, mild cognitive impairment (MCI), and AD).
Methods:
Patients (84 SCD, 129 MCI, 52 AD) and 35 controls underwent the Sniffin’ Sticks Screen 16 test and comprehensive neuropsychological examination.
Results:
Odor identification scores were progressively lower moving from normal older adult to SCD, MCI, and AD. Additionally,the proportion of odor identification dysfunction were increasingly higher in the AD spectrum (p for trend <0.001), but no significant difference was found in the proportion of subjective olfactory dysfunction. No significant correlation was found between odor identification and cognition in the normal older adults and SCD subjects, but odor identification correlated with global cognition in the MCI (r = 0.199, p = 0.033) and in the AD (r = 0.300, p = 0.036) patients. Multiple linear regression showed that odor identification dysfunction was most strongly associated with memory among different cognitive subdomains and was most strongly associated with immediate verbal recall among different memory subdomains.
Conclusion:
Odor identification dysfunction is already present with SCD and deepens with disease severity in the AD spectrum, and it may contribute to predicting cognitive decline and identifying SCD subjects who are at risk of developing AD.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is the most common cause of dementia, contributing to a major global health challenge [1]. With no restorative therapy available, identifying individuals at high risk of developing AD and predicting its disease progression is critical for implementing preventive strategies and planning for future care. At present, approved methods of diagnosing AD include cerebrospinal fluid biomarkers (Aβ and tau) and neuroimaging (PET-CT), but their invasiveness and expensiveness limit their wide use [2]. Recently, an increasing number of studies have suggested that odor identification (OI) dysfunction could serve as a noninvasive and inexpensive marker for the early screening of AD, which may improve the efficiency of diagnosis and reduce the cost of screening [3–6].
Postmortem studies [7–11] showed that neurofibrillary tangles occur very early in regions involved in olfactory information processing (entorhinal and transentorhinal areas, anterior olfactory nucleus and olfactory bulb) in AD patients. According to the disease stages described by Braak et al., AD pathology is observed very early in the entorhinal and transentorhinal areas [8, 10]. Consistent with this, several cross-sectional and longitudinal studies have established associations between OI dysfunction and the risk of AD [12–17]. Approximately 85%–90%of patients with AD exhibit OI dysfunction [18, 19]. Woodward et al. [20] considered that OI dysfunction is a useful screening tool for AD-related amnestic disorder. Recent research revealed that intact OI in older adults was related to a very low conversion rate of AD [21]. Moreover, Risacher et al. [22] suggested that OI was associated with tau but not Aβ in subjects with subjective cognitive decline (SCD) and mild cognitive impairment (MCI).
As a high-risk group of AD, approximately 47%of subjects with MCI exhibit OI dysfunction [23]. Moreover, 47%of MCI subjects with OI dysfunction and 11%of MCI subjects with intact OI eventually developed AD in a 2-year follow-up [24]. Furthermore, Growdon et al. [25] suggested that a poor OI in these subjects was associated with markers of neurodegeneration, elevated cortical amyloid, and a thinner entorhinal cortex among community-dwelling older adults with normal cognition. Additionally, longitudinal studies demonstrated that OI dysfunction may predict cognitive decline or progression to AD in clinically normal older adults [26–29]. This evidence suggests that there may be a transitional period between MCI and normal older adults, and OI may contribute to screening this period out.
In 2014, the Subjective Cognitive Decline-Initiative (SCD-I) proposed a common framework for SCD research and considered that SCD may be the earliest stage of cognitive decline in AD [30]. A meta-analysis of longitudinal studies (with at least 4 years of follow-up) found a future conversion to dementia in 14%of SCD individuals and to MCI in 27%of SCD individuals [31]. Moreover, long-term prospective studies suggested that SCD occurs, on average, approximately 10 years before a dementia diagnosis [32, 33].Therefore, exploring markers that could contribute to the screening of individuals at high risk of developing AD with SCD is paramount. Nevertheless, few studies have focused on olfactory function with SCD. A community-based study (n = 81) suggested that subjective memory complainers were significantly worse than non-complainers with respect to olfactory discrimination, identification, and overall olfactory functioning [34]. However, it remains unclear whether SCD is associated with OI dysfunction and whether there is progressive deterioration of OI between normal older adults and those with MCI, which may contribute to the prediction of AD with SCD subjects.
Considering that OI dysfunction can precede cognitive decline by 10 years and may be paralleled with tau-mediated neuronal damage during the progression of AD [4], the present cross-sectional study aimed to compare OI function among different stages in the AD spectrum (including individuals with SCD, MCI, and AD) and to explore the relationships between OI dysfunction and cognitive impairment among different stages in the AD spectrum. We hypothesized that 1) OI dysfunction is already present with SCD; 2) the incidence and severity of OI dysfunction may increase with the different stages of disease in the AD spectrum (SCD < MCI < AD); 3) OI dysfunction may be associated with cognitive impairment (especially memory loss) in the AD spectrum; and 4) the associations between OI dysfunction and cognitive impairment may be increasingly stronger in the AD spectrum. Therefore, the present study provides a deeper understanding of when and how OI dysfunction progresses in the AD spectrum.
METHODS
Subjects
Two hundred and sixty-five subjects were continuously recruited from the Affiliated Brain Hospital of Guangzhou Medical University (Guangzhou Huiai Hospital), and 35 age-matched normal controls (NC) were recruited from the community in Guangzhou. Subjects were assigned to one of three groups: 84 with SCD, 129 with MCI, and 52 with AD. All subjects or their legal guardians provided signed informed consent to participate in the study. This study was approved by the ethics committees of the Affiliated Brain Hospital of Guangzhou Medical University (Guangzhou Huiai Hospital).
The diagnostic criteria of AD were based on the National Institute of Neurological and Communicative Disorders and Stroke-Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) for probable AD [35], and the diagnostic criteria of MCI were based on the Peterson criteria [36]. The SCD criteria included the following two major features [30, 31]. The first was a self-experienced persistent decline in cognitive capacity relative to a previously normal cognitive status, unrelated to an acute event. All respondents were asked the following questions: 1) Do you have complaints about your memory? Participants were asked to answer “yes” or “no”. 2) How long do you think your memory has declined? The participants were asked to respond with the duration of memory decline. 3) Are you worried about your memory problems? The participants were asked to answer “yes” or “no”. If the answer was “yes”, then the following questions were asked presented: 3.1 Are you worried about remembering something difficultly? 3.2 Are you worried about where things are placed? 3.3 Are you worried about forgetting what you said? 3.4 Are you worried about forgetting a meeting or party? The participants were asked to answer with “mildly”, “moderately”, or “severely”. Those who answered “yes” to the first question, who responded to the second question with a duration of memory decline of more than 0.5 years, and who indicated that the decline was unrelated to an acute event, satisfied the first criterion. The second criterion was normal performance on standardized cognitive tests used to classify MCI, adjusted for age, sex, and education. NC individuals were age-matched, cognitively and physically healthy individuals without a complaint of memory decline. The exclusion criterion was as follows: 1) patients with a history of any neurodegenerative disease besides AD; 2) patients with psychosis or other psychiatric conditions such as depression, anxiety, and suicidal behavior. All subjects underwent structured interviews, standardized olfactory tests, and clinical symptom and comprehensive cognitive assessments.
Assessments of odor identification
For OI assessment, the Sniffin’ Sticks Screen 16 test [37, 38] was applied, which involves the presentation of odorants from felt-tip pens. The lid was then removed by the experimenter for almost 3 seconds, and the pen’s tip was placed approximately 2 cm in front of both nostrils. Subjects were asked to smell 16 common odorants from the felt-tip pens and to name the odors using a multiple choices format with four choices, only one of which was correct. The subjects’ scores ranged from 0 to 16. An OI score less than 12 was defined as OI dysfunction [39]. The subjects were asked the questions: Do you have any decline in your ability to identify smells? The answer is “yes” or “no”. It was defined as subjective olfactory dysfunction when the subjects answered “yes” [40].
Assessments of cognitive function
Cognitive function was evaluated by the following neuropsychological tests: Mini-Mental State Examination (MMSE), Memory and Executive Screening (MES), Auditory Verbal Learning Task (AVLT), Trail-Making Test (TMT), Symbol-Digit Modality Test (SDMT), Boston Naming Test (BNT), and Rey-Osterrieth Complex Figure test (ROCF). The severity of dementia was graded by the clinical dementia rating (CDR) score in the AD group. The TMT B was also used in the present study, and the number of correct lines, time, and number of incorrect lines was recorded. The scores for the cognitive domains were calculated by transforming each of the tests to standardized z-scores. Notably, the TMT score was calculated by the reciprocal of the score and then transformed to standardized z-scores, which represent executive function [41]. The average z-scores of the MMSE and MES represented global cognition. The average z-scores of the AVLT N1-3, AVLT N4, AVLT N5, and AVLT N6 represented immediate recall, short-term delayed recall, long-term delayed recall and recognition, respectively. The z-scores of the BNT, ROCF and SMDT represented language, visuospatial skill, and attention, respectively.
Statistics
Statistical Package for Social Sciences version 25.0 (IBM SPSS 25.0, Chicago, IL, USA) was used for the statistical analyses. Two-tailed chi-square tests were used to compare group differences in sex, OI dysfunction, and subjective olfactory dysfunction. One-way ANOVA was used to compare the mean scores of the OI and neuropsychological tests across three or four groups controlling for age, sex, and years of education. Post hoc least significant difference (LSD) tests were used for multiple comparisons in the one-way ANOVA. Partial correlations were calculated to assess the associations between OI and the z-scores of the cognitive functions, controlling for age, sex, and years of education. In the stepwise multiple linear regression analysis, when analyzing the relationships between different cognitive subdomains and OI, the z-scores of the different cognitive subdomains (memory, language, executive function, visuospatial skill, and attention) were defined as the independent variables; when investigation the relationship between different memory subdomains and OI, the z-scores of different submemory domains (AVLT N1-3, AVLT N4, AVLT N5, AVLT N6) were defined as the independent variables. In each step of the stepwise multiple linear regression analysis, the control variables included age, sex and years of education. Variables with p > 0.10 were excluded in the next step, and variables with p < 0.05 were able to enter the model. Because approximately 63.7%of AD patients were unable to complete the cognition subdomain tests (memory, language, attention, executive function, and visuospatial skill), the cognition subdomain scores of the AD group were not included in the statistical analysis.
RESULTS
Demographic data, cognitive function and olfactory function of different groups
The demographic data of the different groups are listed in Table 1. Data are in accordance with normal distribution and expressed as means±SD. Seven patients had very mild disease (CDR = 0.5), 25 patients had mild disease (CDR = 1), 17 patients had moderate disease (CDR = 2), and 3 patients had severe disease (CDR = 3) in the AD group. Significant differences were found in the OI scores and all cognitive scores between the NC, SCD, MCI, and AD group (p < 0.05) (see Table 1). The proportion of subjects displaying OI dysfunction was increasingly higher from NC to SCD, MCI, and AD (p for trend < 0.001) (see Fig. 1A). However, no significant difference was observed in subjective olfactory dysfunction among different groups (p > 0.05) (see Fig. 1B). The OI scores were progressively lower moving from NC to SCD, MCI and finally to AD (see Fig. 2A). The NC and SCD groups performed better than the MCI group in all cognitive domains, and no significant difference was found between the SCD and NC groups (see Fig. 2B). No significant difference was observed in the OI between the males and females in the different groups (p > 0.05).
Demographic data, clinical information, cognitive function, and olfactory function of all subjects
NC, normal controls; SCD, subjective cognitive decline; MCI, mild cognitive impairment; AD, Alzheimer’s disease; OI, odor identification; OI dysfunction (%), percentage of OI dysfunction; MMSE, Mini-Mental State Examination; MES, Memory and Executive Screening; AVLT N1-3, Auditory Verbal Learning Test Immediate recall; AVLT N4, Auditory Verbal Learning Test Short-term delayed recall; AVLT N5, Auditory Verbal Learning Test Long-term delayed recall; AVLT N6, Auditory Verbal Learning Test Recognition; BNT, Boston Naming Test; TMT, Trail-Making Test; ROCF, Rey-Osterrieth Complex; SDMT, Symbol-Digit Modality Test. *Statistically significant at the 0.05 level (2-tailed); **Statistically significant at the 0.01 level (2-tailed). #F refers to the two-tailed chi-square test, χ2 refers to the two-tailed Fisher’s exact test, Z refers to the two-tailed Z-test. aIn post hoc multiple comparisons, A means NC group, B means SCD group, C means MCI group, and D means AD group.

Comparisons of the percentages of objective and subjective OI dysfunction among different groups. A) The percentage of OI dysfunction exhibited a significant increase from NC to SCD, MCI, and finally to AD (p for trend <0.001). B) There was no significant difference observed in subjective olfactory dysfunction among the different groups. NC, normal controls; SCD, subjective cognitive decline; MCI, mild cognitive impairment; AD, Alzheimer’s disease; OI, odor identification; OI impairment (%), percentage of odor identification. *p < 0.05, **p < 0.01, and ***p < 0.001.
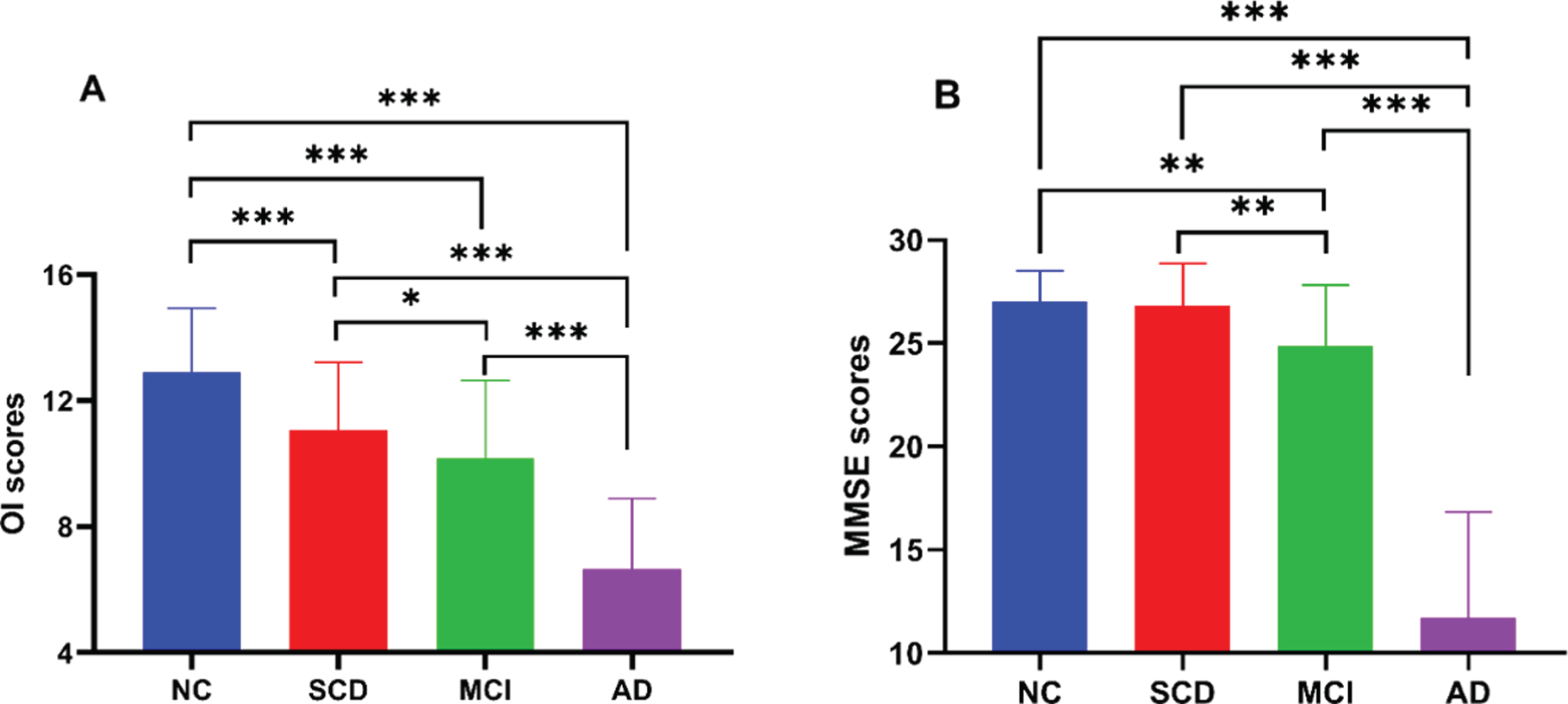
Comparisons of OI scores and MMSE scores among different groups. A) The OI scores decreased from NC to SCD, MCI and finally to AD. B) The MMSE scores decreased from NC or SCD to MCI and finally to AD, but no significant difference was found between NC and SCD. NC, normal controls; SCD: subjective cognitive decline; MCI, mild cognitive impairment; AD, Alzheimer’s disease; OI, odor identification; MMSE, Mini-Mental State Examination. *p < 0.05, **p < 0.01, and ***p < 0.001.
Correlation analyses between OI and cognitive function
Partial correlation analysis showed that the OI scores were positively correlated with global cognition, memory, language, visuospatial skill, and attention among all subjects independent of condition (p < 0.05). In the SCD group, however, there was no significant correlation between any of the different cognitive domains and OI scores. In the MCI and in the AD group, the OI score was positively correlated with global cognition (p < 0.05) (see Table 2).
Partial correlation between OI and cognitive function (control variables included age, sex, years of education)
SCD, subjective cognitive decline; MCI, mild cognitive impairment; AD, Alzheimer’s disease. *Statistically significant at the 0.05 level (2-tailed); **Statistically significant at the 0.01 level (2-tailed). #All subjects except AD patients (n = 248).
Multiple linear regression analysis
In the multiple linear regression analysis, OI was most strongly associated with memory and visuospatial skill across all subjects and was most strongly associated memory in the MCI group (see Table 3). However, after Bonferroni correction, OI was only most strongly associated memory across all subjects. When the z-scores of different memory subdomains were defined as the independent variable, OI was most strongly associated the AVLT N1-3 score across all subjects and in the MCI group (see Table 3). In the NC and SCD groups, there was no correlation between global cognition and OI score (see Fig. 3).
Cognition and memory information from multiple linear regression analysis (control variables included age, sex, years of education)
MCI, mild cognitive impairment; AD, Alzheimer’s disease. *Statistically significant at the 0.05 level (2-tailed); **Statistically significant at the 0.01 level (2-tailed). #All subjects except AD patients (n = 248).
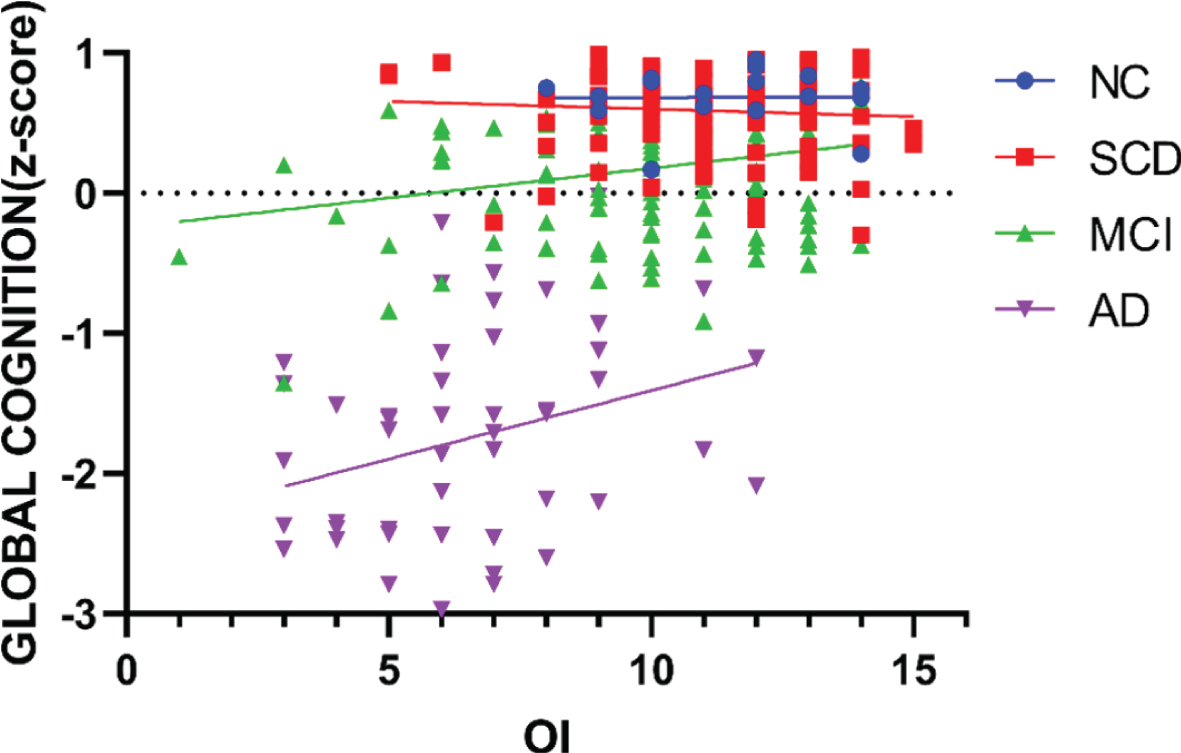
Correlations between the z-scores of global cognition and OI scores in different groups. In the NC and SCD groups, there was no significant correlation between global cognition and OI scores. There was a significant positive correlation between global cognition and OI in the MCI group (r = 0.199; p < 0.05) and in the AD group (r = 0.300; p < 0.05). NC, normal controls; SCD: subjective cognitive decline; MCI, mild cognitive impairment; AD, Alzheimer’s disease; OI, odor identification.
DISCUSSION
The present study compared OI function in the AD spectrum of disease and explored the relationships between OI and cognition. The important findings were as follows. First, OI dysfunction is already present with SCD in the AD spectrum. Second, OI dysfunction was increasingly severe with the different stages of disease in the AD spectrum. Third, poorer OI performance was associated with poorer cognition in the AD spectrum, and their correlation was increasingly stronger with the different stages of disease in the AD spectrum. Fourth, among different cognitive subdomains, OI was most strongly associated with memory; among different memory subdomains, OI was most strongly associated with immediate verbal recall. Fifth, there was no difference in the percentages of subjective olfactory dysfunction among the different groups.
As expected, a strong relationship between OI dysfunction and the AD spectrum was found in the current study. It has been reported that accelerated atrophy of the medial temporal lobe, including the entorhinal cortex, hippocampus, and parahippocampal gyrus, is associated with an increased risk of developing AD [42]. Additionally, the olfactory pathway and memory processing overlap in these brain areas, suggesting that OI and cognition share a common neuroanatomical basis in the AD spectrum. Indeed, abnormalities of the olfactory pathway have been repeatedly shown in subjects with MCI and AD, including reduced volumes of the hippocampus and entorhinal cortex [43] and morphological changes in the olfactory bulb and olfactory tract [44].
Previous studies showed that OI dysfunction predicted a faster cognitive decline and a higher rate of conversion to AD among normal older adults and MCI subjects [42]. Indeed, a low hippocampal volume and entorhinal cortex thickness were associated with poor OI in normal older adults and MCI subjects [25]. For SCD, cross-sectional studies have shown that compared with individuals without SCD, individuals with SCD had small decreases in the volumes of AD-related brain regions (e.g., the medial temporal lobe) [45, 46]. Some studies also identified AD-associated patterns of glucose hypometabolism with SCD [47, 48]. This evidence suggests that SCD may reflect the initial stage of the AD spectrum. However, whether OI is impaired in individuals with SCD and whether it could serve as a predictor for AD conversion remain unclear. These are only a few studies on this topic, which have suggested that SCD patients exhibit significantly lower OI scores than community-dwelling populations [34] and higher OI scores than MCI/AD subjects [49], which is consistent with our present study results with a larger sample size. Therefore, we speculate that in subjects with SCD, OI may also contribute to cognitive decline prediction and identifying SCD subjects who are at risk of developing AD.
In the present study, positive correlations were noted between OI performance and cognitive function in all subjects, which is in line with previous studies [50, 51]. However, there was no such correlation with SCD individuals. Additionally, the correlations between OI dysfunction and cognitive impairment became increasingly stronger with the different stages of disease in the AD spectrum (NC < SCD < MCI < AD). A possible reason is that only 14%of individuals with SCD are expected to convert to dementia [31], which may contribute to the weaker association between OI and cognition with SCD than with MCI and AD. As the disease progresses, greater cognitive impairment occurs during the MCI stage [52] and showing better correlate with OI dysfunction. Furthermore, a stronger correlation (moderate) between OI dysfunction and cognitive impairment was shown in AD patients because their cognitive impairment is as severe as their OI dysfunction [18, 19].
Furthermore, we explored which cognitive doma-ins may be strongly associated with OI in the AD spectrum. OI involves detection and recognition of a previously smelled odor and recall of objects, sources, and/or names associated with the odor, which can be assigned to the episodic memory function [53]. According to our linear regression, the strongest correlation was found between OI and memory function, which is consistent with the result of a previous study [51]. Furthermore, we analyzed which memory domain was most closely related to OI and found that OI dysfunction was best correlated with immediate verbal recall abilities in preclinical AD (NCs and subjects with SCD and MCI). Possible reasons include the fact that immediate memory loss, which was assessed by the AVLT N1-3, is also a typical symptom of the early stage of AD. In addition, the process for testing OI was similar to the AVLT N1-3: in OI assessment, subjects name the odor using multiple choices immediately after having just smelled the odor, and in the AVLT N1-3, subjects are also asked to immediately recall a word they had just heard. The present study showed that OI dysfunction may contribute to predicting cognitive decline and identifying SCD subjects who were at risk of developing AD. Therefore, more attention should be paid to SCD subjects with OI dysfunction, and early intervention should be performed to prevent them from developing AD. Additionally, olfactory training, which is beneficial to olfaction and cognition, may serve as a potential measure for early interventions against developing AD.
Regardless of group status, very few participants reported subjective OI decline in the current study, which corresponds with previous results and implies a weak association between subjective and objective measurements of OI [54, 55]. One possible explanation is that people may have poor self-awareness of OI dysfunction [56]. Another explanation is that subjects who suffer from cognitive impairment may not be able to correctly evaluate their OI abilities, and complaints about cognitive impairment may overwhelm OI dysfunction. The current results suggest that when utilizing OI dysfunction to predict the risk of dementia, objective measurements are needed, and subjective reports are not reliable.
The strong relationship between AD and OI dysfunction may be linked to its nasal-entry infectious hypothesis. The nasal neuroepithelium is the sole region of the CNS in direct communication with the external environment without an interlining blood-brain barrier, therefore representing a susceptible port of entry for exogenous toxins to the brain [57]. The neuropathology of AD, especially tau pathology, also starts from the olfactory bulb, then progresses to the primary olfactory cortex and finally to the secondary olfactory cortex and the whole brain [8]. Currently available evidence strongly supports that the initiating event in AD is related to abnormal processing of the Aβ peptide, and after a lag period, increased tau and cerebral atrophy become the dominant biomarkers of neuronal dysfunction and neurodegeneration [4]. In the AD continuum, OI dysfunction occurs after Aβ deposition, precedes brain structural changes, cognitive decline and clinical symptoms, and may be accompanied by tau-mediated neuronal damage [58]. This evidence strongly suggests that OI may contribute to identifying subjects with SCD at high risk of progression to AD. Our results corroborate this hypothesis, showing that individuals with SCD had poorer OI than healthy older adults and better OI than MCI subjects. Thus, we suspect that the onset of OI dysfunction may begin as early as the SCD stage in the AD spectrum. Thus, we may consider SCD as a new clinical disease stage in the pathogenesis of AD, hallmarked by OI dysfunctions (see Fig. 4)
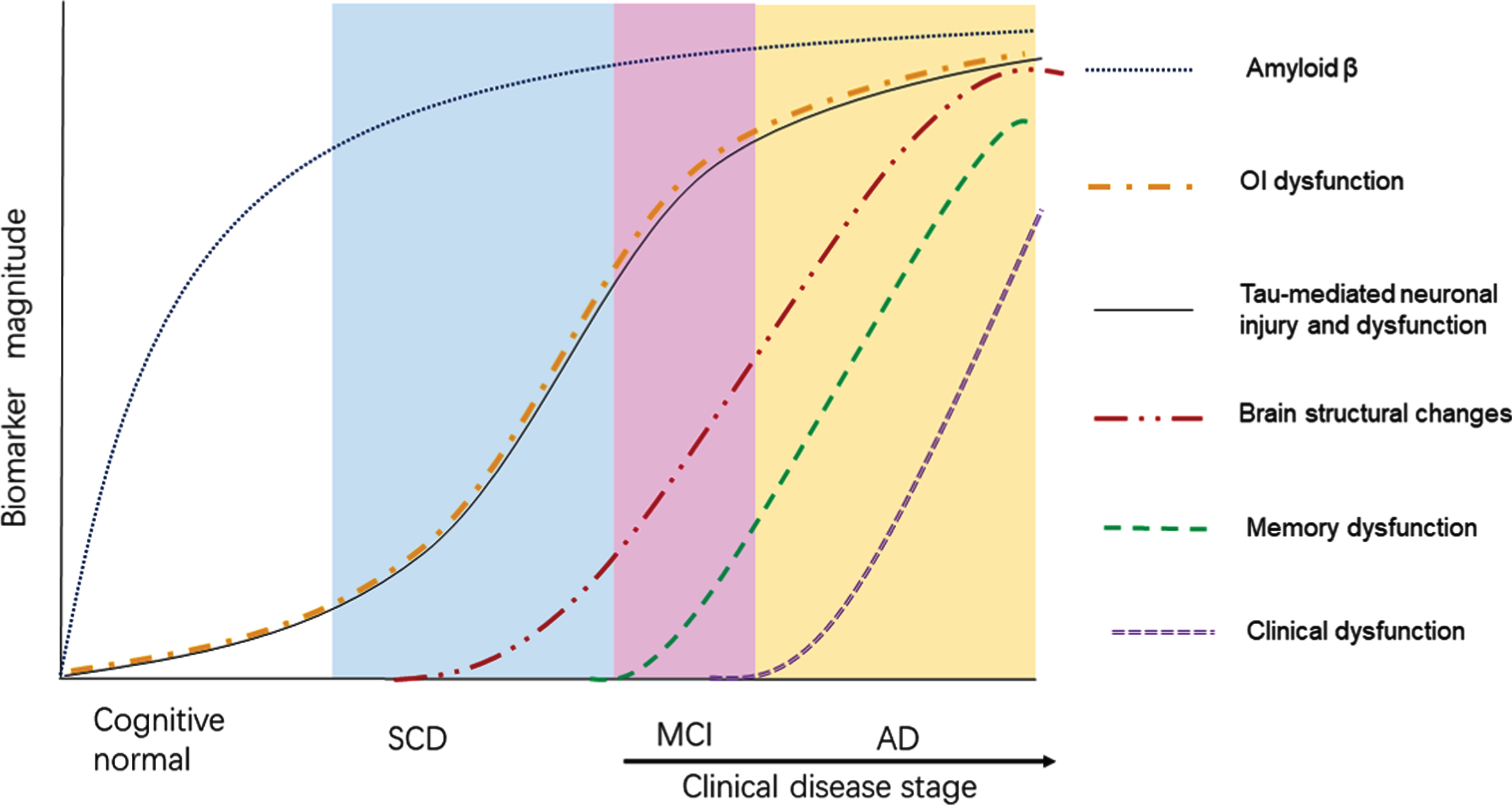
Emergence of OI dysfunction in the AD spectrum. This figure illustrates the emergence of OI dysfunction within the context of the emergence of other indicators of the pathological cascade described by previous studies (modified after references [4, 58]). We added SCD as a new clinical disease stage and suspect that the onset of OI dysfunction may begin as early as the SCD stage in the AD spectrum. SCD, subjective cognitive decline; MCI, mild cognitive impairment; AD, Alzheimer’s disease, OI, odor identification.
There were limitations in the present study. First, due to the cross-sectional design of the study, we cannot draw accurate conclusions about the disease trajectory of the AD spectrum. Longitudinal studies are underway to address this issue. Second, the present study only neuropsychological measures data. Future studies involving the assessment of cerebrospinal fluid biomarkers and PET-CT will further clarify the relationship between OI dysfunction and neurodegenerative markers of AD. Third, the impact of cognitive enhancers in the AD group was not excluded in the present study, which may have influenced the results. Fourth, the current study only included OI, the strongest predictor of AD. Future studies including odor thresholds and discrimination could provide a deeper understanding of the relationship between olfaction and the AD spectrum.
In summary, the current study demonstrated that OI dysfunction is already present with SCD and precedes cognitive impairment in the AD spectrum. OI dysfunction may serve as a simple, noninvasive, and cost-effective biomarker for predicting AD as early as the SCD stage. Further studies are ongoing to determine whether SCD subjects with OI dysfunction will have faster cognitive decline and higher conversion rates to MCI and AD and whether a combination of OI and other AD-related predictors could improve the sensitivity and specificity in predicting AD.
Footnotes
ACKNOWLEDGMENTS
We thank Cong Ouyang, Weiru Zhang, Wanyuan Liang, and Chunying Dai for assistance in collecting the data. We are grateful for the assistance from the Department of Neurology, the Department of Geriatric Psychiatry of the Affiliated Brain Hospital of Guangzhou Medical University (Guangzhou Huiai Hospital).
This study was supported by a grant from the National Natural Science Foundation of China (No. 81701341), the Guangzhou Municipal Psychiatric Diseases Clinical Transformation Laboratory (No: 201805010009), the Key Laboratory for Innovation Platform Plan, the Science and Technology Pro-gram of Guangzhou, China, the Science and Tech-nology Plan Project of Guangdong Province (No. 2019B030316001), and the National Key Research and Development Program of China (No. 2016YFC0906300). The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.