
Abstract
Background:
Education plays a potential important effect on the prevalence and incidence of dementia. However, most of the evidence based on convenience sampling.
Objective:
To explore effects of education on cognition in individuals with subjective cognitive decline (SCD) and cognitive impairment (CI) from a population-based study.
Methods:
We examined the effect of education on cognition among individuals with SCD (n = 451) and CI (n = 280) from a population-based study. A series of neuropsychological tests of memory, executive, language, and general cognitive function were used to assess the participants.
Results:
Multiple regression analyses revealed that education has a positive effect on cognition in both SCD and CI group in the population-based research. Further stratification study showed that the beneficial effect of education remains in the SCD group regardless of the education level, especially in the SCD participants with a low education level. However, that effect of education exists in the CI group with a low education level and disappears in the high education level.
Conclusion:
These results from a population-based sample suggest that high educational attainment may delay cognitive decline in the individuals with SCD regardless of high or low educational level, and high education only predicts cognition in those in the low educational level in CI group.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is the leading cause of dementia and is characterized by the progressive deterioration of cognitive functions like learning and memory, attention, language, and executive function [1]. Biologically, AD is now defined by the presence of its underlying neuropathologic change: amyloid-β (Aβ) and pathologic tau accumulation [2]. No disease-modifying treatment for AD is currently available [3]. Although the etiology of AD is elusive, there is agreement that it arises from interactions between lifestyle, genetic, and environmental factors [4, 5]. At present, several potentially modifiable risk factors for AD and dementia have been identified, including less education [6–8]. Study has suggested that the highest estimated population-attributable risk of AD was for low educational attainment (19.1%, 95% CI 12.3–25.6) worldwide [9]. In addition, epidemiological study indicated that the prevalence and incidence of dementia are stable or declining in some Western countries over the past decades and improvements in education may partly explain the observed trends [10]. Therefore, a core strategy to effectively prevent AD relies on management of those modifiable risk factors.
Subjective cognitive decline (SCD) refers to a sub-jective experience of cognitive decline, in the absence of impairment on objective neuropsychological tests [11]. There is accumulating evidence that older individuals with SCD are more likely to develop mild cognitive impairment (MCI) and AD [12–14]. Biomarker studies have found an association between SCD and AD pathology [15, 16]. Therefore, individuals with SCD could serve as a target population for prevention in AD [17]. Our recent work indicates that high education may have a potential to delay cognitive decline in individuals with SCD in convenience sampling [18]. However, evidence suggested that SCD from convenience and population sampling were different in clinical and neuropsychological features, frequency of APOE ɛ4 allele, biomarkers, and the incidence of MCI [19–21]. Therefore, examining the effect of education on cognition in individuals with SCD from a population-based sample may contribute to a better understanding of education for AD prevention in SCD.
Here, we used data from a population-based study to examine the effect of education on cognition in ol-der adults with SCD. Moreover, we explored whether education exerts differential effect on cognition in individuals with SCD and cognitive impairment (CI).
METHODS
Ethics statement
This study was approved by the medical ethics committee of Xuanwu Hospital of Capital Medical University, Beijing, China. Written informed consent was obtained from each participant.
Sources of subjects
Data for this present study were obtained from a population-based epidemiologic study conducted from September to November 2016 in ShunYi District in Beijing, China. Details of the study design have previously been published [22]. Briefly, the main purpose of the study was to investigate the prevalence of SCD in China. There were 426 village committees and 85 subdistrict area committees in the ShunYi District at the end of 2015. A multistage stratified cluster random sampling design was used to select the subjects. In total, 16 communities were selected and 2,689 subjects participated in the study. Each subject was required to complete a medical history, neurological examination, and a comprehensive neuropsychological test battery. Inclusion criteria were 1) permanent residents (living in the target community for at least half a year); 2) Han ethnicity; 3)≥60 years old. Exclusion criteria were 1) other neurological diseases like cerebrovascular disease, brain trauma, Parkinson’s disease; 2) current major psychiatric diagnoses such as severe depression and anxiety; 3) metabolic diseases such as anemia, thyroid dysfunction; 4) other conditions such as a history of CO poisoning, cancer and general anesthesia; 5) serious systemic diseases; 6) severe visual or hearing impairment.
After finishing those examinations, participants were divided into the following categories: normal controls (NC), SCD, MCI, or AD dementia. The clinical diagnostic criteria for AD dementia are according to the diagnostic guidelines established by National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) [23]. The diagnostic criteria for MCI are defined by an actuarial neuropsychological method proposed by Jak and Bondi [24]. Participants who meet all of the following conditions were considered SCD: 1) presence of self-perceived continuous cognitive decline compared to a previous normal status; 2) failure to meet the above criteria for MCI and AD dementia and there did not exist other diseases or conditions that would lead to cognitive decline. NC was assigned when they achieved a normal cognitive performance according to the results of standard neuropsychological assessments and did not have self-reported persistent decline in cognition. Here, we included n = 451 SCD and n = 281 CI participants (273 MCI+8 AD dementia) for the present study. A study flowchart is presented in Fig. 1.
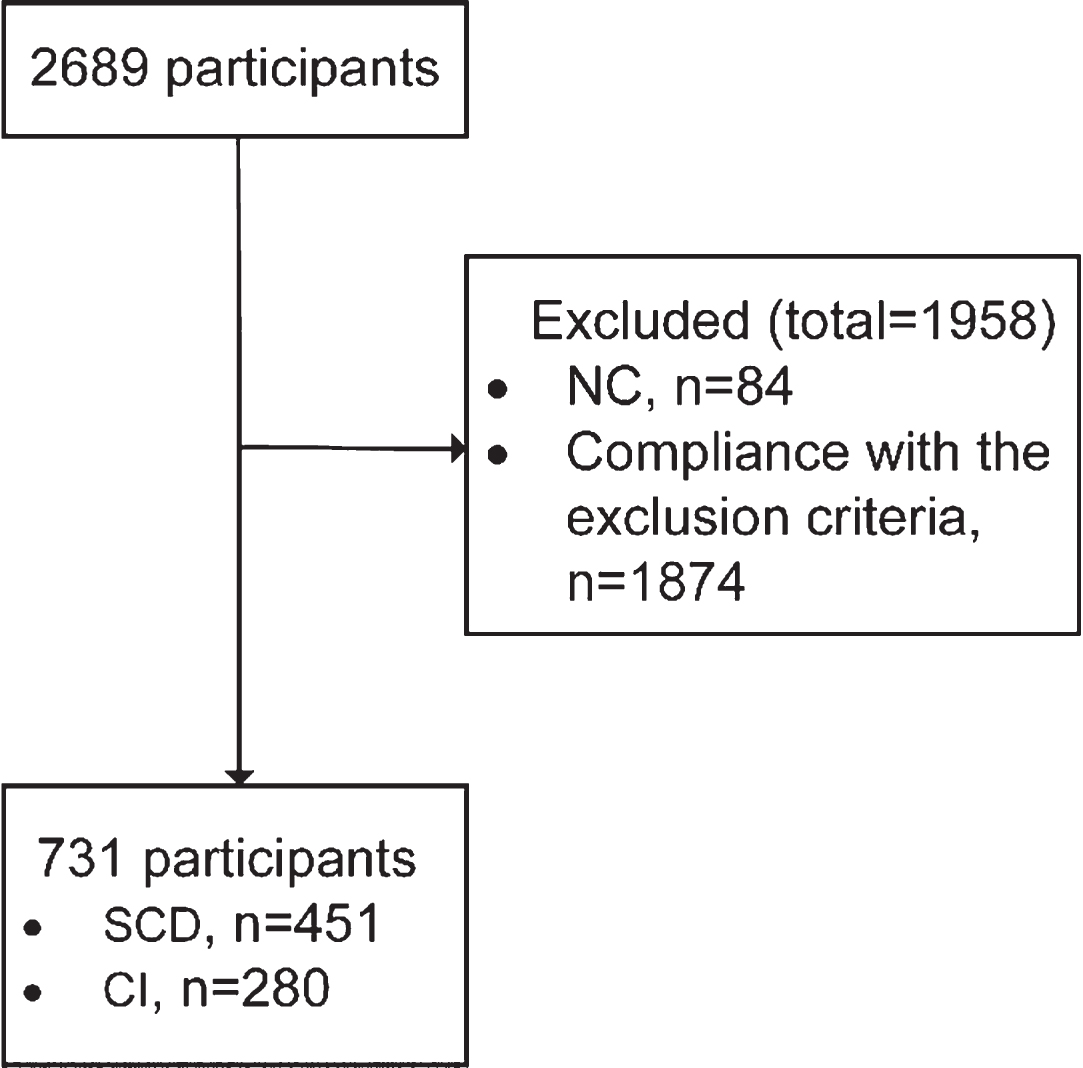
The flow charts of this study. NC, normal controls; SCD, subjective cognitive decline; CI, cognitive impairment.
Clinical assessments and neuropsychological tests
At each committee unit, trained staff collected data in local neighborhood committees or village committees. Paper-printed case report form (CRF) was used to record demographic features (name, birthdate, sex, education, occupation, ethnic origin, residential address and contact information etc.), medical history (particularly including the history of hypertension, diabetes, dyslipidemia, etc.), results of neuropsychological tests and clinical diagnosis for each participant.
A standardized neuropsychological test battery was used to assess performance in three cognitive domains: memory (Auditory Verbal Learning Test-Huashan version long-delayed free recall [AVLT-H-N5] and recognition [AVLT-H-N7]) [25], executive function (Clock-Drawing Test [CDT-30]) [26], language (Animal Fluency Test [AFT]) [27]. Montreal Cognitive Assessment-Basic (MoCA-B) [28] scores were used as an index of global cognitive condition. The Hamilton Depression Rating Scale (HAMD) [29] and the Hamilton Anxiety Scale (HAMA) [30] were used to assess neuropsychiatric symptoms. In addition, to obtain a total test score of cognitive performance, all raw cognitive function scores were first converted into a z-scores calculated by subtracting the score from the mean test score and dividing it by the standard deviation of initial test scores, and then the total test score was expressed as a global composite z-scores created by averaging all cognitive function test z-scores.
Statistical analyses
First, the Kolmogorov–Smirnov (KS) test and histogram were performed to assess for normality of distribution of continuous variables. Normally distributed continuous data were expressed as the mean±standard deviation (SD) and non-normally distributed variables were expressed as median (inter-quartile range). Categorical variables were expressed as number (n) and percentage (%). Second, simple correlation analysis was conducted to examine associations between education and raw score of cognitive function tests including AVLT-H-N5, AVLT-H-N7, AFT, CDT-30, and MoCA-B. Third, the effect of education on cognition in the total sample were determined using multiple linear regression model with the raw scores of neuropsychological tests as the dependent variable and education as independent variable while controlling for the effects of age, sex, and the presence of hypertension, diabetes, and dyslipidemia. Then, we examined whether the effect of education on cognition differed according to disease stage, by performing previous multiple linear regression analysis in the SCD group (n = 451) and the CI group (n = 280). Next, we used the median of education to divide SCD and CI group into two groups, “low” or “high” (SCD group: 0–8 = low, 9–18 = high; CI group: 0–6 = low, 7–12 = high), respectively. We explored the effects of education on cognition among subjects with low versus high education, by performing above multiple linear regression analysis in both SCD and CI group. In addition, we presented the effect of education on the total test score of cognitive performance in the total sample and two subgroups. We used Welch t test, using partial regression coefficients (β) and corresponding standard error, to assess the differences in effects among two subgroups. Furthermore, we examined whether the effect of education on the total test score of cognitive performance differed according to low or high education in both SCD and CI group. Multiple linear regression analysis controlling for age, sex, and the presence of hypertension, diabetes, and dyslipidemia was conducted to examine the differences in effects among low or high education group in both SCD and CI subjects, using the low education group as the reference group. Regression diagnostics were performed to ensure the assumptions for linear regression were met. Residuals were normally distributed. Durbin-Watson test statistics indicated independence of observations and heteroscedasticity was in conformance with test assumptions (results not shown). The “Performance Analytics”, “tableone”, “forestplot”, and “effects” packages in R 3.6.3 software (https://www.r-project.org) were used to perform all the analyses. The significant level was set at p < 0.05 (2-sided).
RESULTS
Demographic characteristics
Demographic and clinical characteristics of the total sample and according to disease stage are presented in Table 1. A higher percentage of these subjects (59%, n = 431) were females. The median age of the entire sample was 66 years and median education was 8 years. There were no differences according to disease stage in sex, HAMD, HAMA, and the prevalence of hypertension, diabetes mellitus, and dyslipidemia. The CI group had a lower level of education and was older than the SCD group. As expected, participants with CI have lower cognitive scores in all neuropsychological tests compared to SCD participants.
Demographic and clinical characteristics of the study participants
SCD, subjective cognitive decline; CI, cognitive impairment; HAMD, Hamilton Depression Rating Scale; HAMA, Hamilton Anxiety Scale; AVLT-H-N5, Auditory Verbal Learning Test-Huashan version long-delayed free recall; AVLT-H-N7, Auditory Verbal Learning Test-Huashan version long-delayed recognition; AFT, Verbal Fluency Test (animal); CDT-30, Clock-Drawing Test; MoCA-B, Montreal Cognitive Assessment-Basic. aThe p value was calculated using Chi-square. bThe p value was calculated using Mann-Whitney U. cThe p value was calculated using independent samples t tests.
Effects of education on neuropsychological test scores in the total sample and according to disease stage
Simple linear correlation analysis reveals a modest association between education and all neuropsychological test scores in the total sample (AVLT-H-N5: r = 0.29, AVLT-H-N7: r = 0.23, AFT: r = 0.36, CDT-30: r = 0.34, MoCA-B: r = 0.5, all p < 0.001), in the SCD group (AVLT-H-N5: r = 0.19, AVLT-H-N7: r = 0.11, AFT: r = 0.28, CDT-30: r = 0.33, MoCA-B: r = 0.44, all p < 0.001), and in the CI group (AVLT-H-N5: r = 0.31, AVLT-H-N7: r = 0.26, AFT: r = 0.4, CDT-30: r = 0.29, MoCA-B: r = 0.56, all p < 0.001).
The results of the multiple linear regression models are shown in Figs. 2, 3. Multiple regression analyses with adjustment for age, sex, and the presence of hypertension, diabetes, and dyslipidemia reveals a positive effect of education on all neuropsychological test scores in the total sample (all p < 0.001; Fig. 2) and subgroups with the exception of the effect on AVLT-H-N7 in the SCD group (p = 0.086; Fig. 3). Furthermore, Fig. 4 indicates that as years of educational attainment increased, the total test score increased in the total sample (β=0.096 [95% CI, 0.082–0.111], p < 0.001; Fig. 4a), SCD and CI group (β=0.061 [95% CI, 0.048–0.076], p < 0.001 versus β=0.09 [95% CI, 0.07, 0.11], p < 0.001; Fig. 4b), while the benefit of educational attainment was significantly higher in the CI group compared to the SCD group (p = 0.024).

Effect sizes of education on neuropsychological tests in the total sample. β, partial regression coefficients; CI, confidence interval; AVLT-H-N5, Auditory Verbal Learning Test-Huashan version long-delayed free recall; AVLT-H-N7, Auditory Verbal Learning Test-Huashan version long-delayed recognition; AFT, Verbal Fluency Test (animal); CDT-30, Clock-Drawing Test; MoCA-B, Montreal Cognitive Assessment-Basic.
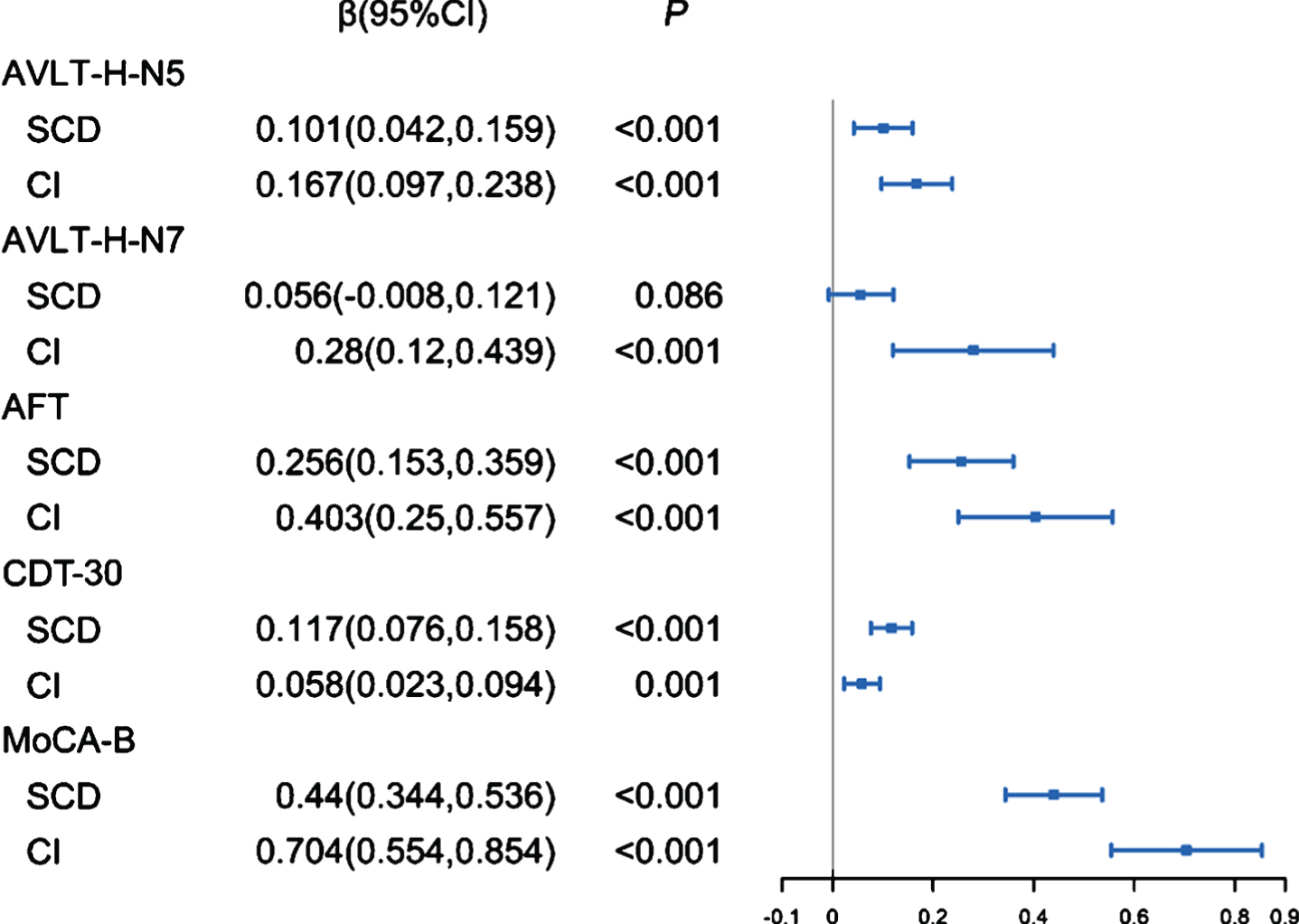
Effect sizes of education on neuropsychological tests in the SCD and CI group. β, partial regression coefficients; CI, confidence interval; AVLT-H-N5, Auditory Verbal Learning Test-Huashan version long-delayed free recall; AVLT-H-N7, Auditory Verbal Learning Test-Huashan version long-delayed recognition; AFT, Verbal Fluency Test (animal); CDT-30, Clock-Drawing Test; MoCA-B, Montreal Cognitive Assessment-Basic.
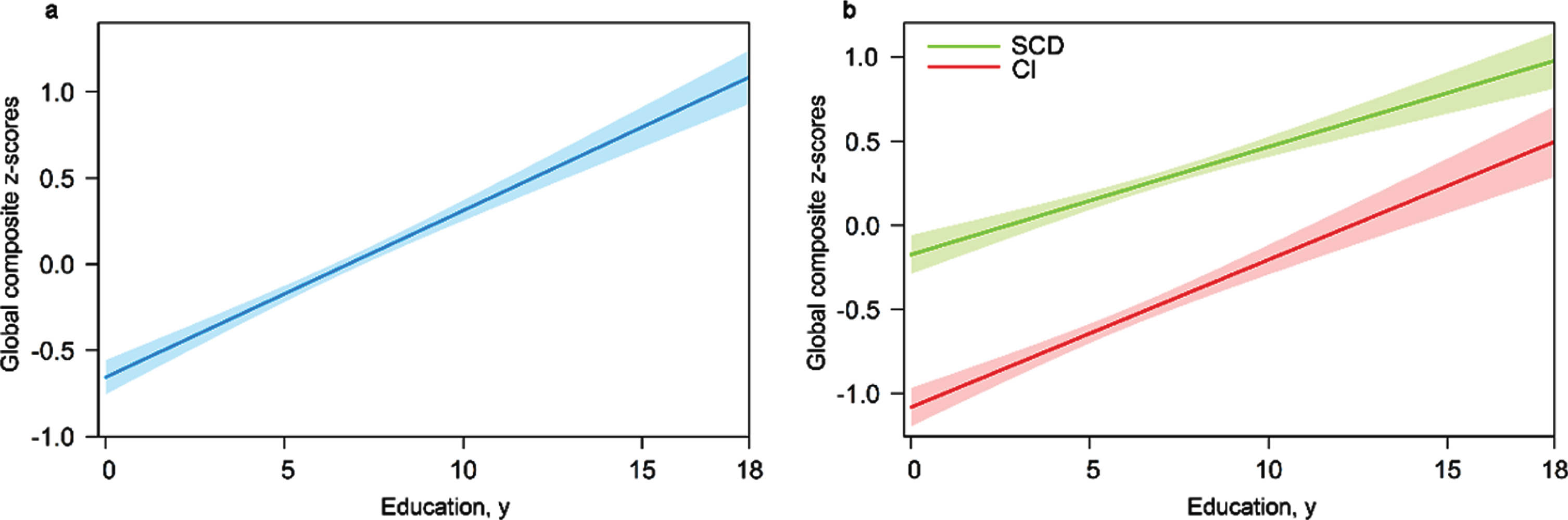
Predicted global composite z-scores. a) For the total sample. b) For the subgroups. SCD, subjective cognitive decline; CI, cognitive impairment.
Effects of education on neuropsychological test scores in the SCD and CI group according to low and high education level
In the SCD group, multiple regression analyses show a positive effect of education on AVLT-H-N5, CDT-30, and MoCA-B in the low education level and AFT, CDT-30, and MoCA-B in the high education level (Fig. 5). Among the CI group, education has a beneficial effect on AFT, CDT-30, and MoCA-B in the low education level, while education has no significant effect on any of the cognitive tests in the high education level (Fig. 6). Furthermore, as years of educational attainment increased, the total test score increased in the SCD group regardless of the education level (β=0.072 [95% CI, 0.045–0.099] among low level, p < 0.001 versus β=0.041 [95% CI, 0.007–0.075] among high level, p = 0.018; Fig. 7a) and the benefit of educational attainment was higher in the low education level compared to the high educational level (β=0.289 [95% CI, 0.203–0.376], p < 0.001). However, the protective effect of education exists in the CI group with the low education level and disappears in the high education level (β=0.098 [95% CI, 0.062–0.134] among low level, p < 0.001 versus β=–0.0003 [95% CI, –0.113–0.112] among high level, p = 0.996; Fig. 7b).
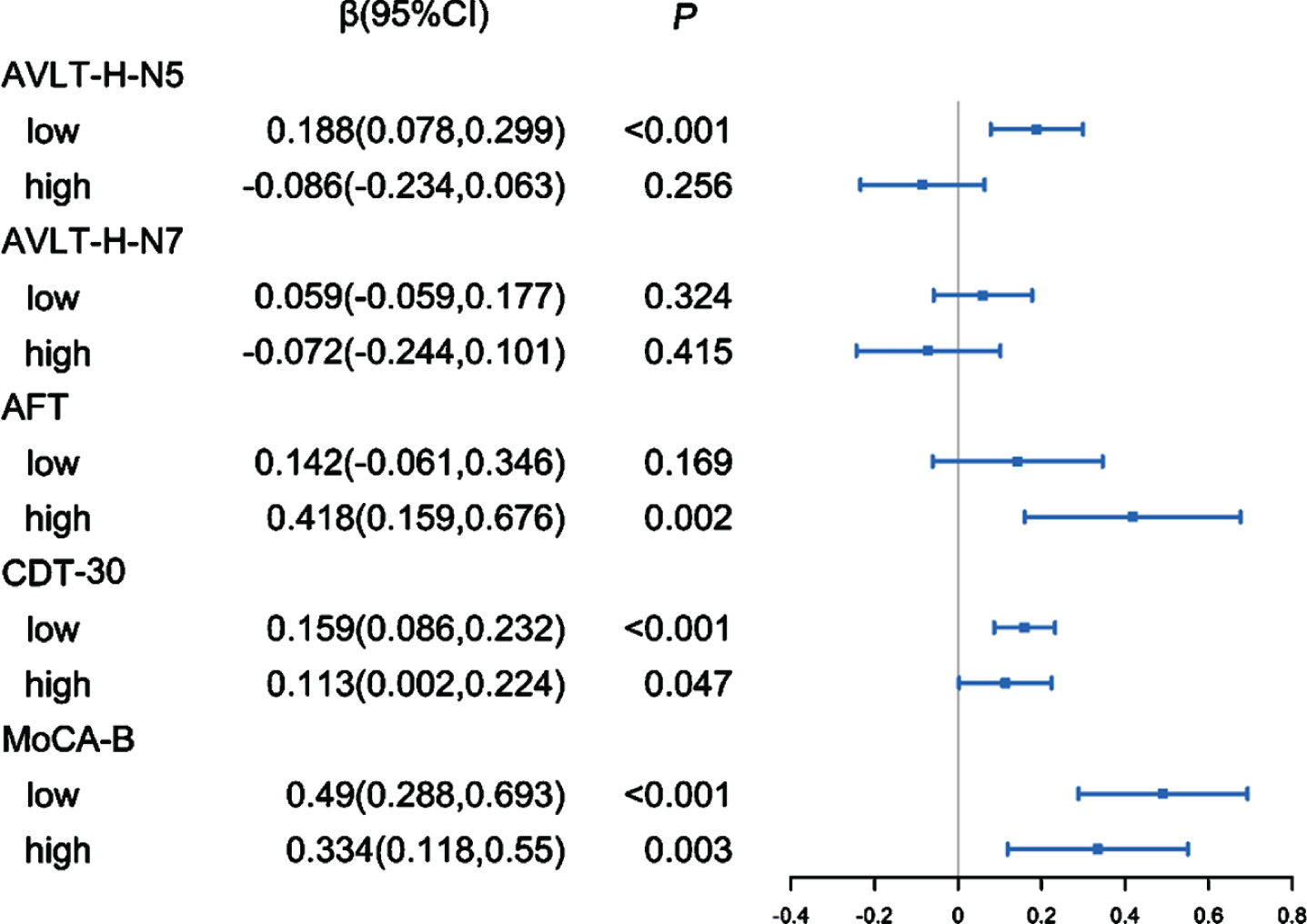
Effect sizes of education on neuropsychological tests in the SCD group according to low and high education level. β, partial regression coefficients; CI, confidence interval; AVLT-H-N5, Auditory Verbal Learning Test-Huashan version long-delayed free recall; AVLT-H-N7, Auditory Verbal Learning Test-Huashan version long-delayed recognition; AFT, Verbal Fluency Test (animal); CDT-30, Clock-Drawing Test; MoCA-B, Montreal Cognitive Assessment-Basic.
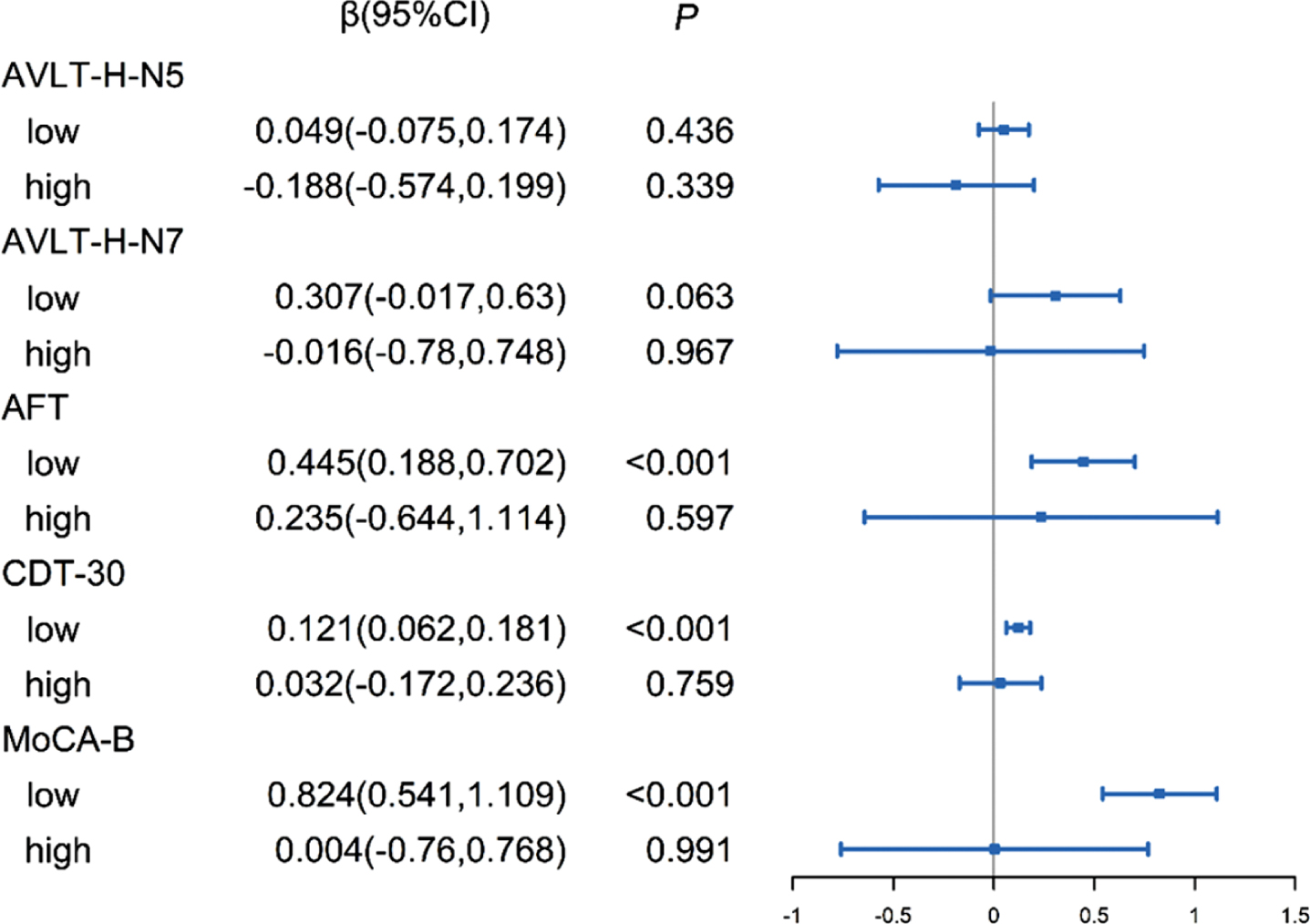
Effect sizes of education on neuropsychological tests in the CI group according to low and high education level. β, partial regression coefficients; CI, confidence interval; AVLT-H-N5, Auditory Verbal Learning Test-Huashan version long-delayed free recall; AVLT-H-N7, Auditory Verbal Learning Test-Huashan version long-delayed recognition; AFT, Verbal Fluency Test (animal); CDT-30, Clock-Drawing Test; MoCA-B, Montreal Cognitive Assessment-Basic.
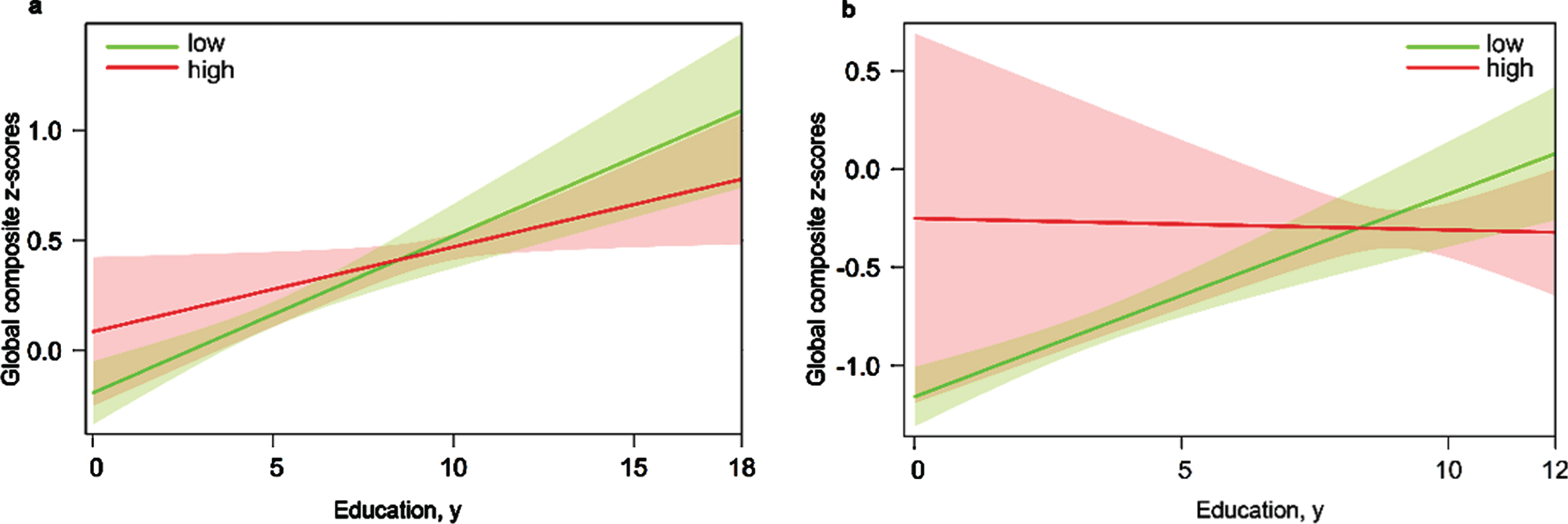
Predicted global composite z-scores in the SCD and CI group according to low and high education level. a) For the SCD group. b) For the CI group. SCD group: 0–8 years = low, 9–18 years = high; CI group: 0–6 years = low, 7–12 years = high.
DISCUSSION
In the present study, we examined the effect of education on cognitive performance in SCD subjects in a population-based survey, and we also investigated whether there was a difference in the effect between the SCD and CI group. The main findings of our study are 1) education has a positive effect on cognition among both SCD and CI group in the population-based research; 2) the beneficial effect of education remains in the SCD group regardless of the education level, especially in the SCD participants with low education level; and 3) the effect of education exists in the CI group with low education level and disappears in the high education level.
A recent study by convenience sampling from our group suggested that high education has a positive effect on multiple cognitive measures in both APOE ɛ4 carriers and non-carriers with SCD [18]. The SCD population in the current study was relatively older, lower educated compared with the former SCD group from a cohort using convenience sampling. These differences in sample characteristics between population and convenience sampling are in line with most literature [21, 31]. Accordingly, we extend on our previous findings by demonstrating that high education has a beneficial effect on cognition in the SCD population from a population-based study. Furthermore, the present study showed that education exerts a different effect on cognition in the SCD and CI group with varying education levels. These findings may be explained by the theory of cognitive reserve (CR). The concept of CR refers to the ability of functional brain processes that allow some people to maintain function in response to brain changes or damage, which was proposed to account for a mismatch between the degree of neuropathologic burden and the level of cognitive function [32, 33]. CR is a theoretical construct and was not directly measured, instead surrogate indices such as education, intelligence quotient, occupational complexity, and leisure and physical activity were measured [34]. According to the theory of CR, individuals with high CR can tolerate more AD pathology and decline in cognitive function will be delayed at the early stage of AD, while the rate of decline in cognition is more rapid in individuals with high CR than those with low CR at the advanced stage of AD [35]. A previous cross-sectional study found that CR has a positive effect across multiple cognitive domains in AD biomarker–positive participants in the predementia stages [36]. A longitudinal follow-up study confirmed that higher CR slows the clinical progression in predementia stages of AD and accelerates disease progression after the onset of dementia in Aβ-positive individuals [37]. Therefore, our findings that education has a positive effect on cognition in both SCD and CI group are in line with the theory of CR. On the other hand, according to the theory of CR, when patients with AD matched for a given level of clinical severity, the patients with high CR suffer from more severe pathological brain changes than that in those with low CR [35], and that was also confirmed in neuroimaging studies [38, 39]. Thus, one possibility for our findings that the effect of education on cognition varies from education levels in both SCD and CI group is that highly educated participants may reflect a greater degree of pathology. In other words, SCD and CI participants with high educational level may have a more severe AD pathology than those with low education level, respectively. Findings from a prospective population-based cohort study showed that the association between SCD and risk of AD is stronger in the high education group, which also supports our hypothesis [40]. However, this needs to be further validated by biomarker-based studies.
The major strength of the present study is the participants from the general population, which increases the study’s representativeness. However, this study has its own shortcomings. First, the present study was a cross-sectional design, and therefore, long-term follow-up data are required to confirm whether education has a differential effect on cognition in the SCD and CI group. Second, we are unable to obtain AD pathological biomarkers and APOE ɛ4 allele due to a population-based design. It is important that incorporating these high-dimensional data reveals the mechanism of the effect of education on cognition.
In summary, this study based on population sampling indicated that high education has a potential role to delay or slow down cognitive decline in individuals with SCD regardless of the education level and CI with low education level. Therefore, it is urgent to solve the problem of unfair education and promote the popularization of education worldwide, which may be a potentially promising approaches to prevente AD currently.
Footnotes
ACKNOWLEDGMENTS
This article was supported by the National Natural Science Foundation of China (Grant 61633018). The authors thank Dr. Yili Chen, Dr. Jiaojiao Liu, Dr. Jing Cao, Dr. Xiaodong Zhi, Dr. Ting Wang, Dr. Yang Yu, Dr. Bin Mu, Dr. Hongyan Li, Dr. Lixiao Hao, Dr. Liu Yang, Dr. Yu Sun, Dr. Xuanyu Li, Dr. Xiaoqi Wang, and Dr. Wenying Du for their contributions to the data collection.