
Abstract
Background:
Severe socio-emotional impairments characterize the behavioral variant of frontotemporal dementia (bvFTD). However, literature reports social cognition disorders in other dementias.
Objective:
In this study, we investigated the accuracy of social cognition performances in the early and differential diagnosis of bvFTD.
Methods:
We included 131 subjects: 32 bvFTD, 26 Alzheimer’s disease (AD), 16 primary progressive aphasia (PPA), 17 corticobasal syndrome (CBS), and 40 healthy control (HC). Each subject completed the Ekman 60 faces (Ek-60F) test assessing basic emotion recognition and the Story-based Empathy Task (SET) assessing attribution of intentions/emotions. A combined social measure (i.e., Emotion Recognition and Attribution (ERA) index) was calculated. One-way ANOVA has been used to compare performances among groups, while receiver operating characteristic (ROC) curve tested measures ability to distinguish subjects with and without bvFTD.
Results:
Ek-60F and ERA index scores were significantly lower in bvFTD versus HC, AD, and PPA groups. ROC analyses significantly distinguished bvFTD from HC (AUC 0.82–0.92), with the Ek-60F test showing the highest performance, followed by the ERA index. These two social measures showed the best accuracy in detecting bvFTD from AD (AUC 0.78–0.74) and PPA (AUC 0.80–0.76). Investigated measures failed in detecting bvFTD from CBS.
Conclusion:
Accuracy analyses support the advantage of using social cognition tests for bvFTD diagnosis. Short social battery may reduce uncertainties and improve disease identification in clinical settings. We recommend a revision of current clinical criteria considering neuropsychological deficits in emotion recognition and processing tasks as key cognitive markers of this neurodegenerative syndrome.
Keywords
INTRODUCTION
Changes in social behavior and emotion regulation characterize patients affected by the behavioral variant of frontotemporal dementia (bvFTD) since the early disease stages [1, 2]. These early pervasive social and emotional modulation disorders, followed in a later stage by marked executive dysfunctions, are linked to the progressive functional and structural neurodegeneration of frontotemporal-limbic regions [2, 3].
Despite extensive literature on bvFTD reporting significant social cognitive dysfunctions in emotion recognition [4, 5], theory of mind (ToM) [6, 7], empathy [8, 9], and decision-making [10], the use of social tasks in the neuropsychological assessment of bvFTD is at present not required by any diagnostic guideline. In fact, at the time of the definition of the currently used bvFTD diagnostic criteria [11], no standardized test for the assessment of social cognition skills was available and only qualitative reporting of “loss of sympathy/empathy” and “socially inappropriate behavior” was taken into consideration. From 2011, many progresses have been made, and multiple studies evaluated the accuracy of different social tasks in distinguishing bvFTD from healthy controls or other neuropsychiatric disorders (for a systematic review, see [12]).
In this sense, increasing available evidence sugge-sts a wider and more selective impairment in affective rather than cognitive facets of social processing [12–14]. For instance, one of the previous studies evaluating the sensitivity and specificity of a well-known test for emotion recognition (i.e., Ekman-60 Face test) found a sensitivity of 94% and a specificity of 100% in distinguishing bvFTD from healthy controls [14]. Thus, changes in the ability to create an explicit representation of other’s feelings in a social contextual world (i.e., emotion recognition, [15]), as well as in the ability to represent and predict affective states in the self and others to guide adaptive homeostatic behavioral responses (i.e., empathy, [16]), are the core of social brain changes occurring in bvFTD patients [17–19]. Comparably, affective facet of ToM, which is considered as the ability to attribute independent mental states to others, overlapping with the construct of cognitive empathy [20], is selectively impaired in bvFTD compared to Alzheimer’s disease (AD) patients [13].
A crucial challenge in the clinical diagnosis of bvFTD is represented by the differential diagnosis with other neurodegenerative diseases presenting a signi-ficant overlap with bvFTD in both clinical-neurop-sychological [21, 22] and imaging findings [23, 24]. Among these, a crucial issue is the distinction bet-ween bvFTD and AD patients. Indeed, accumulating literature [25, 26] shows that neither executive dysfunctions nor amnestic deficits are sufficient to clearly distinguish these two disease categories, as bvFTD can present overlapping features with AD, possibly due to variability of its functional correlates [23].
On the other hand, recent evidence suggests that AD patients might present changes in emotion processing and ToM [7, 28]. Comparably, social cognition dysfunctions have been reported in the other frontotemporal lobar degeneration syndromes (i.e., semantic or non-fluent variant of primary progressive aphasias (PPA) or atypical parkinsonism belonging to the spectrum of corticobasal syndrome (CBS)) [29–32]. However, no studies evaluated the diagnostic accuracy of these tests in distinguishing bvFTD from PPA or CBS.
The aim of this study is thus to evaluate the diagnostic accuracy of tasks for the assessment of emotion recognition and processing in distinguishing bvFTD from healthy controls (HC) and other cognitive neurodegenerative disorders (i.e., AD, PPA, and CBS). Besides, we also evaluated the accuracy of a social index, obtained combining the performance at two tasks of basic emotion recognition and attribution, i.e., the Emotion Recognition and Attribution (ERA) index [33].
METHODS
Participants
An overall sample of 131 subjects was enrolled for the present study. The sample included 32 mild-to-moderate patients fulfilling Rascovsky criteria for probable bvFTD [11], 26 patients fulfilling Albert and McKhann criteria for prodromal (n = 13; [34]) and mild (n = 13; [35]) AD, 16 PPA patients according to Gorno-Tempini criteria [36], and 17 patients fulfilling Armstrong criteria for CBS [37]. Patients were consecutively enrolled at the Department of Clinical Neurosciences, San Raffaele Hospital (Milan, Italy) and at the Department of Experimental and Clinical Medicine, Polytechnic University of Marche –Osp-edali Riuniti (Ancona, Italy) in the years between 2012 and 2017. PPA group included 7 semantic var-iant (svPPA) and 9 non fluent variant (nfvPPA) pat-ients who were consecutively referred to our memory clinic center during the year range of this study. No patient with logopenic variant (lvPPA) was included in the PPA group.
All patients underwent a standard neurological and neuropsychological assessment of basic cognitive functions (memory, language, visuo-spatial abilities, executive functions, and attention). Neuroimaging data (i.e., MRI and/or FDG-PET) were collected to provide support for the diagnosis. Expert clinicians blind to the performance at social tasks performed the clinical diagnosis. A 2-year mean follow-up confirmed the initial classification.
The HC sample included 40 subjects recruited at local community centers. Exclusion criteria for HC were: 1) positive history of neuropsychiatric disorders; 2) positive neurological exam; 3) Clinical Dementia Rating scale (CDR) > 0; 4) a Mini-Mental Examination raw score < 28; 5) medication interfering with neurobehavioral functioning.
All patients or informants/caregivers, and each HC, gave informed consent to the experimental procedure that had been approved by the local ethical committee. Demographic and clinical features of participants are shown in Table 1.
Demographic and clinical features of the sample
bvFTD, behavioral variant of frontotemporal dementia; AD, Alzheimer’s disease; PPA, primary progressive aphasia; CBS, corticobasal syndrome; HC, healthy controls; MMSE, Mini-Mental State Examination; CDR-sob, Clinical Dementia Rating scale sum of boxes; GS, global score; SET, Story-based Empathy Task; EA: emotion attribution; IA: intention attribution; CI: causal inference; EK-60F: Ekman 60 Faces test; ERA, Emotion Recognition and Attribution; *p < 0.05; **p < 0.01;***p < 0.005.
Social cognition assessment
Participants were administered with a brief social cognition battery including two standardized tasks for the Italian population that investigate different facets of social cognition: recognition of basic emotions from face expression (Ekman-60 Faces test (Ek-60F); [38]) and inference of affective and cognitive mental states of others (Story-based Empathy task (SET); [39]).
The Ek-60F evaluates the recognition of six basic emotions from faces, with a maximum score of 60 (10 stimuli for each emotion). It consists of pictures from the Ekman and Friesen series [40], which depict the faces of 10 actors (6 females, 4 males), each displaying six basic emotions (i.e., happiness, sadness, anger, fear, surprise, and disgust). The task administration lasts about 10 minutes. Subjects are required to answer choosing the label that best describes the facial expression shown by the actor.
The SET is a cartoon task including two mentalizing conditions, namely intention attribution (IA) and emotion attribution (EA), plus a control condition entailing the comprehension of causality based on knowledge about the physical properties of objects or human bodies (i.e., causal inference, CI). Each condition includes six trials requiring selection of the correct ending of a comic strip. An upper (story) and a lower row of three vignettes (possible endings) compose each comic strip. The possible endings are presented only later. A score of 1 is assigned only in case of selection of the correct ending, and the global score is computed based on the number of correct answers given by the subjects for each cartoon. A global score (GS) of 18 indicates the best possible task performance. Overall, the task administration lasts about 15 minutes.
Moreover, according to previous literature [33], we computed the cumulative ERA Index by combi-ning EK-60F and SET-EA performances (i.e., SET-EA*10 + Ek-60F), in order to obtain a global direct measure of patient performance on emotion recognition and processing skills.
Statistical analysis
Comparison between groups in demographic features and social cognition tasks was performed thr-ough one-way ANOVA (Bonferroni post-hoc test). Sex, age, and education in years were added as covariates when required. Adjusted Ek-60F and SET scores [38, 39], which take into account the effect of demographic variables on performances, were considered for statistical analyses.
Receiving operating curve (ROC) analyses were performed to evaluate the ability of the Ek-60F global score (GS), SET-GS and sub-scores (EA, IA, and CI), as well as of the ERA Index, in differentiating bvFTD from HC, AD, PPA, and CBS. For those social measures showing a significant discriminative effect, the cut points were derived from the Youden index (Sensitivity + Specificity - 1).
RESULTS
All patient groups showed reduced performance at the MMSE compared to HC (F(4,123) = 13.3, p < 0.001). No significant differences were found in education, disease duration, and severity. See Table 1 for demographic and clinical details of the sample.
Compared to HC, bvFTD patients showed lower performances in all the investigated measures, except for the control condition of SET task (SET-CI). This latter task was particularly impaired in the CBS group that showed a decreased SET-CI performance compared to all the other groups (F (4, 126) = 4.8, p = 0.001). Notably, bvFTD performance on basic emotion recognition was significantly lower (F(4, 126) = 19.7, p < 0.001) not only in comparison to HC (p < 0.001), but also to AD (p < 0.001) and PPA (p < 0.001) groups. Comparably, ERA index score was significantly lower in bvFTD (F(4,126) = 18.0, p < 0.001) compared to HC (p < 0.001), AD (p = 0.003), and PPA (p = 0.005). No differences were found in bvFTD versus CBS groups, nor in the ERA index or in single tasks. See Table 1 for further details.
The ROC curve analyses significantly distinguishing bvFTD from HC show an AUC ranging from 0.82 to 0.92, with the Ek-60F test showing the highest performance (AUC = 0.92, p < 0.001, SE 0.034 CI 95% (0.845–0.99), accuracy 89%), followed by the ERA index (AUC = 0.90, p < 0.001, SE 0.04 CI 95% (0.83–0.97)). As expected, SET-IA showed the lowest performance (AUC = 0.82, p < 0.001, SE 0.05 CI 95% (0.71–0.92)) and consistently with the ANOVA analysis, SET-CI failed in significantly separating bvFTD from HC. In the Ek-60F test, a cut point equal to 43.1 showed 84% of sensitivity and 93% of specificity (accuracy: 89%), while a score of 95.8 at the ERA index had the 94% of sensitivity and the 73% of specificity in distinguishing bvFTD from HC (accuracy: 82%). See Table 2 and Fig. 1 for details.
Coordinates for ROC curve in bvFTD versus HC, bvFTD versus all patient groups and bvFTD versus all AD patients
bvFTD, behavioral variant of frontotemporal dementia; HC, healthy controls; AD, Alzheimer’s disease; SET, Story-based Empathy Task; EA, emotion attribution; IA, intention attribution; CI, causal inference; GS, global score; EK-60F, Ekman 60-Faces test; ERA, Emotion Recognition and Attribution.
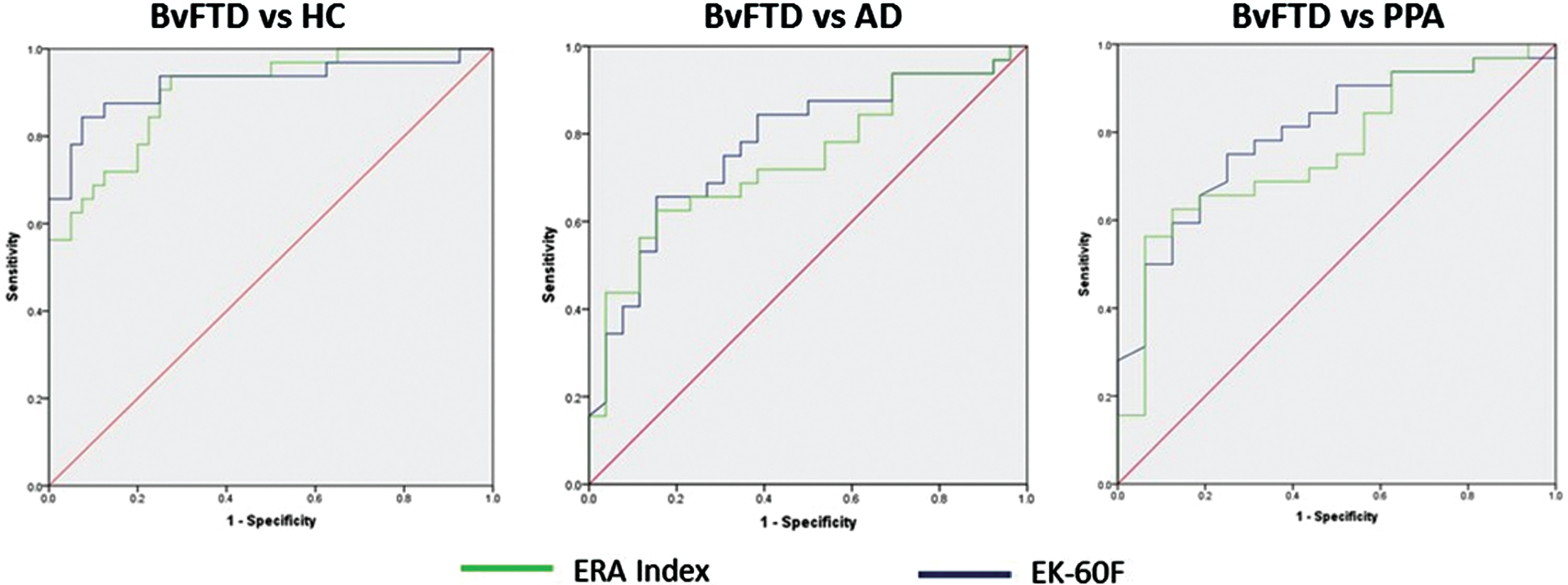
Receiving operating characteristic curve for the Ekman 60-Faces test (EK-60F) and the Emotion Recognition and Attribution (ERA) index in the behavioral variant of frontotemporal dementia (bvFTD) versus healthy controls (HC), bvFTD versus all Alzheimer’s disease (AD) patients, and bvFTD versus primary progressive aphasia (PPA).
ROC analysis comparing bvFTD group with all other patient groups taken together found a significant discriminatory effect of SET-EA performance (AUC = 0.65, p = 0.02, SE 0.06 CI 95% (0.53–0.78)), EK-60F test (AUC = 0.75, p < 0.001, SE 0.05 CI 95% (0.64–0.86)), and ERA index (AUC = 0.72, p = 0.001, SE 0.06 CI 95% (0.60–0.83)). See Table 2 for details.
ROC analysis in bvFTD versus AD (both prodromal and mild patients) showed significant AUC in a range from 0.67 to 0.78. As seen in comparison with HC, the Ek-60F test and the ERA index showed the highest performance in the differential diagnosis with AD, with an AUC of 0.78 and 0.74, respectively. SET-GS, as well as SET-IA and SET-CI, failed in distinguishing the two groups. Cut-off scores computed through the Youden index identified a cut point score equal or below 36.5 for the Ek-60F test (sensitivity: 0.66, specificity: 0.85, accuracy: 74%) and a score of 65 for the ERA index (sensitivity: 0.63, specificity: 0.85, accuracy: 72%). Specific analyses performed separately on bvFTD versus prodromal AD and bvFTD versus mild AD showed that while emotion recognition performance at Ek-60F was useful in discriminating bvFTD from both prodromal and mild AD groups, intention and emotion attribution performances at SET were helpful in separating bvFTD only from prodromal AD. See Tables 2and 3 and Fig. 1 for details.
Coordinates for ROC curve in bvFTD versus prodromal AD and bvFTD versus mild AD
bvFTD, behavioral variant of frontotemporal dementia; AD, Alzheimer’s disease; SET, Story-based Empathy Task; EA, emotion attribution; IA, intention attribution; CI, causal inference; GS, global score; EK-60F, Ekman 60-Faces test; ERA, Emotion Recognition and Attribution.
Finally, the results from ROC analyses evaluating the diagnostic accuracy of the investigated measures in separating bvFTD from PPA and CBS are shown in Table 4 and Fig. 1. While emotion recognition and processing measures (i.e., Ek-60F, SET-EA, and ERA index) successfully distinguished bvFTD from PPA, with an accuracy ranging between 65–77%, they failed in distinguishing bvFTD from CBS.
Coordinates for ROC curve in bvFTD versus PPA and bvFTD versus CBS
bvFTD, behavioral variant of frontotemporal dementia; PPA, primary progressive aphasia; CBS, corticobasal degeneration; SET, Story-based Empathy Task; EA, emotion attribution; IA, intention attribution; CI, causal inference; GS, global score; EK-60F, Ekman 60-Faces test; ERA, Emotion Recognition and Attribution; *equal or lower scores than cut-off are indicative of CBS.
Finally, we performed differential ROC analyses on single emotion recognition of Ek-60F test in order to evaluate possible discriminatory role of single em-otions in bvFTD versus other cognitive syndromes. Overall, no single emotion exceeded the global score in accuracy levels. See Tables 1and 5 for details.
Coordinates for ROC curve in bvFTD versus HC, bvFTD versus all AD patients and bvFTD versus PPA in single emotion recognition at the Ekman 60-Faces test
bvFTD, behavioral variant of frontotemporal dementia; HC, healthy controls; AD, Alzheimer’s disease; PPA, primary progressive aphasia.
DISCUSSION
The development of validated tests assessing social cognition abilities in clinical settings for the early and differential diagnosis of bvFTD represents a clinical research priority. The identification of accurate cognitive markers supportive for a better clinical ass-essment and work-up may add crucial information for those clinicians who deal with dementia. Neuropsychological tools routinely used in clinical settings usually lack the sufficient strength to offer the confidence to clinicians for a highly demanding diagnosis. In this study, we thus assessed the diagnostic accuracy of a short social cognition battery including two easy to administer tasks in separating bvFTD from HC, AD, and the other main clinical phenotypes belonging to the frontotemporal lobar degeneration spectrum (i.e., PPA and CBS). The aim is to offer a more comprehensive view on new clinical tools for the evaluation of affective social components in dementia. Overall, we showed a good performance of social tasks focused on emotion recognition and processing in the diagnosis of bvFTD. Some limitation in the use of such tasks for the differential diagnosis of bvFTD syndrome from the other frontotemporal subtypes however emerged.
Accumulating evidence reveals a close overlap bet-ween brain neurodegeneration pattern in bvFTD and empathy networks, both involving the fronto-limbic regions [18]. Consistently, tasks tapping affective processing such as the Ek-60F test, SET-EA, and the derived combined ERA index measure showed the highest discriminatory ability in distinguishing bvFTD from HC. In agreement with literature [12], these tests showed in fact a good performance in separating bvFTD from normal subjects (AUC 0.84–0.92). These measures entailing the affective facets of social cognition also showed good performances in the differential diagnosis with AD and PPA (Fig. 1), while cognitive ToM (SET-IA) and executive control (SET-CI) conditions failed in clearly separating bvFTD from AD, as no significant difference was found in patients’ performance at these subtasks.
Although the presence of a “pure” social cognition deficit in AD is still a matter of debate, our results as well as previous research findings [12] pointed out that cognitive ToM tasks might not be sufficiently accurate in distinguishing bvFTD from AD. Cognitive ToM skill recruits a complex brain network including both frontal and parietal regions, respectively required for different components of ToM (i.e., behavioral adaptation and social attribution [41, 42]), that can be differentially affected in AD and bvFTD, according to the distribution of the neurodegenerative patterns in these two cognitive syndromes. Thus, although a differential involvement of social brain regions [43, 44], both patient groups can be impaired in cognitive ToM tasks that do not clearly isolate anterior and posterior sub-components of ToM networks.
Furthermore, several studies now report a signifi-cant relationship between ToM and executive functions, meaning that many other neurological disorders apart from bvFTD can be impaired at these tasks [45]. However, the association between executive functions and affective processing is limited, suggesting that tasks based on the integrity of limbic regions and assessing emotion recognition and processing [23, 46] might represent the right tool for the clinical diagnosis of bvFTD.
Deficits in social skills, and particularly at the Story-based Empathy Task, have been previously linked to structural and functional changes in right limbic and fronto-insular networks in bvFTD patients [33, 48]. However, socio affective deficits can characterize also the clinical profile of PPA and CBS patients, in relation to significant degeneration in common brain regions implied in social cognitive abilities [29–32, 49]. In our sample, emotion recognition and attribution deficits accurately distinguished bvFTD from PPA. Although literature provides consistent deficits in emotion recognition, empathy, and ToM also in the semantic and non-fluent variants of PPA, this deficit seems primary and independent of language disturbances only in the semantic PPA variant [29]. The small sample size of the here considered PPA group including both non-fluent and semantic variant patients represent a limitation for these findings and further studies exploring accuracy of social measures in non-fluent and semantic PPA variant groups separately compared to bvFTD are certainly needed to better explain our result. Such evidence may also provide information about the advantage of the use of a non-verbal social tasks (i.e., Ek-60F and SET tasks) in the neuropsychological batteries of PPA patients for the differential diagnosis between the two different language variants.
Conversely to PPA, social cognition tasks did not distinguish bvFTD from CBS. Behavioral analyses on CBS revealed deficits in both basic face processing and high-level emotion processing tasks, with persistence of emotion processing disturbances even after controlling for face processing deficits [30]. Our results are in line with this literature evidence. In particular, the low performance at the SET-CI control condition in CBS compared to other patient groups suggests that CBS cognitive performance at social tasks is certainly influenced by the visual complexity of the stimuli. On the other hand, impaired high-level emotion processing in CBS has been related to a damage of posterior cortical regions, as well as of the basal ganglia [30]. The damage of this latter brain structures may be responsible for changes in automatic and controlled emotion processing, which is specifically regulated by a complex network involving subcortical structures and limbic regions [50]. CBS neuropsychological profile at social cognition tasks thus resembles the pattern of performance typically seen in patients with bvFTD [18, 51], making highly demanding a differential diagnosis based on performances at these cognitive tasks. Future studies should consider examining the relationship between visuospatial functioning and social cognition performances by including comparison between verbal and non-verbal tasks assessing the same social cognition facet.
The heterogeneity of underlying pathological substrates modulating the neurophenotype presentation within PPA or CBS syndromes (for example, see [52–54]) can result in different social cognition deficit profiles even within the same syndromic group. Unfortunately, relationships between selective neuropathological triggers and social cognitive phenotypes in the different syndromes belonging to the frontotemporal spectrum are poorly explored. Future studies investigating this issue are certainly needed.
Finally, present findings show lower diagnostic accuracy for the SET-EA condition and the combined ERA index compared to the Ek-60F test. This result suggests a greater diagnostic usefulness of testing basic emotion recognition compared to higher-level social cognition skills (i.e., ToM/cognitive empathy). SET is a more complex task designed to test cognitive empathy compared to cognitive ToM, controlling for basic causal inference ability. It engages other cognitive functions (e.g., working memory, ability to infer causal relationships, visual perception, and processing), required for task performance. This level of complexity is shared with cognitive/affective ToM and cognitive empathy tasks [55], which are overall more difficult than tasks of recognition of basic emotions from visual expression (i.e., Ek-60F). This results in a decrease of specificity when testing more severe demented patients as proved by the lack of accuracy in discriminating bvFTD from mild AD patients, while good accuracy emerged in bvFTD versus prodromal AD patients. Future comparative studies are thus recommended to evaluate the clinical validity of different tasks in assessing single facet of social cognition in demented patients according to disease severity. In addition, studies exploring accuracy of affective empathy tasks in the diagnosis of bvFTD versus other dementias should be also promoted in order to test whether they may be an adequate choice in clinical settings. The definition of tests clinical validity, as well as other important aspects such as administration time and the choice of verbal and/or non-verbal stimuli, is particularly relevant in view of the definition of a bvFTD-sensitive neuropsychological assessment to be introduced in the clinical setting.
Having these relevant elements in mind, the introduction of socio-emotional processing tasks to the standard neuropsychological assessment of bvFTD patients may provide an extra value for the early and differential diagnosis of this syndrome. Both our data and previous findings strongly suggest the use of high-order social information processing tasks on clinical setting. Overall, the use of a single test or a short battery, with low demand on high-cognitive non-social skills and ideally developed for a specific clinical need (i.e., bvFTD diagnosis), may reduce the inconsistencies and improve the identification of this clinical phenotype. Besides, considering the hig-her specificity compared to sensitivity defined in the present work, these tests can be of particular utility in the second level cognitive assessment of patients suspected for bvFTD for a better differential diagnosis.
Future research priorities, however, should be focused on the comparison between different tasks tapping the same facet of social cognition (i.e., verbal/visual) and in the evaluation of the advantages of combined batteries aimed at assessing multiple social (i.e., emotion recognition and empathy) and non-social (e.g., language or visuo-spatial abilities) over single tasks to identify a cognitive marker for the bvFTD syndrome.