
Abstract
Background:
The Frontal Behavioral Inventory (FBI) is a questionnaire designed to quantify behavioral changes in frontotemporal dementia (FTD). Literature showed heterogeneous FBI profiles in FTD versus Alzheimer’s disease (AD) with variable occurrence of positive and negative symptoms.
Objective:
In this study, we constructed a short FBI version (i.e., mini-FBI) with the aim to provide clinicians with a brief tool for the identification of early behavioral changes in behavioral variant of FTD (bvFTD), also facilitating the differential diagnosis with AD.
Methods:
40 bvFTD and 33 AD patients were enrolled. FBI items were selected based on internal consistency and exploratory factor analysis. Convergent validity of mini-FBI was also assessed. A behavioral index (i.e., B-index) representing the balance between positive and negative mini-FBI symptoms was computed in order to analyze its distribution in bvFTD through a cluster analysis and to compare performance among patient groups.
Results:
The final version of the mini-FBI included 12 items, showing a significant convergent validity with the Neuropsychiatric Inventory scores (rp = 0.61, p < 0.001). Cluster analysis split patients in four clusters. bvFTD were included in three different clusters characterized by prevalent positive symptoms, both positive and negative symptoms, or prevalent negative behavioral alterations, similar to a subset of AD patients. A fourth cluster included only AD patients showing no positive symptoms.
Conclusion:
The mini-FBI is a valuable easily administrable questionnaire able to early identify symptoms effectively contributing to the bvFTD behavioral syndrome, aiding clinician in diagnosis and management.
Keywords
INTRODUCTION
Frontotemporal dementia (FTD) is a rare neurodegenerative condition accounting for about 10% of early-onset dementias [1, 2]. The behavioral variant of FTD (bvFTD), which represents the half of all FTD cases [3], is characterized by a variable combination of positive and negative behavioral symptoms, and socio-affective, executive and other cognitive disorders [4].
Many scales and questionnaires have been developed with the aim to evaluate behavioral disturbances in FTD syndromes and add information for a better diagnosis [5–10]. In this context, the Frontal Behavioral Inventory (FBI) is a valuable tool to quantify personality and behavioral changes in FTD syndromes [10–12] that has been adapted and validated in different languages being extensively used in many research and clinical settings [11–17]. This is a 24-item scale developed by A. Kertesz [10] that includes two subscales assessing negative and positive behavioral changes. Items have been chosen considering core behavioral symptoms needed for the diagnosis of bvFTD [18]. The scale determines the presence/absence of behavioral changes on a 4-point Likert scale for each item as gauged by the caregiver interview.
Despite the fact that bvFTD syndrome has a very distinctive clinical pattern, its cognitive and behavioral features may overlap with those of Alzheimer’s disease (AD) leading to misdiagnosis or delay in diagnosis. A timely differential diagnosis between bvFTD and AD has significant implications for both clinical management and quality of life of patients and caregivers. This is a crucial challenge especially in clinical settings where costly biological markers of pathology (biofluids or MRI/PET imaging assessment) are not alwaysavailable.
Accumulating literature shows that neither executive dysfunctions [19, 20] nor amnestic deficits [21–23] alone are sufficient to clearly distinguish these two disease categories, as bvFTD can present overlapping features with AD, possibly due to topographical variability in brain vulnerability [24, 25]. Assessment of social cognition skills may add relevant information reducing uncertainties and improving disease identification [19, 27]. Nonetheless, the use of standardized social cognition measures in clinical settings is still limited [28]. Integration among different cognitive and behavioral markers has also been suggested as possible solution to improve diagnostic accuracy in bvFTD [19, 29].
Literature evidence proved heterogeneous FBI profiles in the characterization of bvFTD versus AD or other diseases causing frontal lobe behavioral symptomatology, with variable occurrence of positive and negative symptoms [11]. FBI has been proved well performing in both discriminating bvFTD from other dementia and tracking disease progression [12–17]. A self-administered caregiver modified version has been also developed in order to save time and avoid the intervention of a trained investigator [30].
The main aim of this study is to propose a short version of the FBI, i.e., the mini-FBI, to provide a time-saving instrument for the clinical settings. The secondary aim is to identify communalities and differences of mini-FBI profiles in bvFTD and AD and to propose mini-FBI cut-off scores for the clinical implementation.
METHODS
Participants
An overall sample of 73 patients was included in the present study. The patient sample encompassed 40 patients fulfilling Rascovsky criteria for probable bvFTD in mild disease phase [31] and 33 patients fulfilling McKhann criteria for mild AD [32] who were consecutively enrolled at the memory clinic of the Department of Rehabilitation and Functional Recovery, San Raffaele Hospital (Milan, Italy) in the years between 2012 and 2018. See Table 1 for demographic and clinical features.
Demographic and clinical features of the sample
bvFTD, behavioral variant of frontotemporal dementia; AD, Alzheimer’s disease; MMSE, Mini-Mental State Examination; CDR, clinical dementia rating scale. Data are expressed as mean±standard deviation or median [interquartile range] according to data distribution. Significant differences are highlighted in bold.
All patients underwent a standard neurological and neuropsychological assessment of basic cognitive functions (memory, language, visuo-spatial abilities, executive functions, and attention). Neuroimaging data (i.e., MRI and/or FDG-PET) were collected to provide support for the diagnosis. Clinical diagnosis was performed by expert clinicians, blind to the performance at behavioral assessment. A 2-year mean follow-up confirmed the initial classification.
All patients and caregivers gave informed consent to the experimental procedure that had been approved by the local ethical committee and in accordance with the ethical principles of the Declaration of Helsinki.
Behavioral assessment
Participants were administered with a brief behavioral battery including the FBI [11, 12] and the Neuropsychiatric Inventory (NPI) [6]. Behavioral assessment was performed by a neuropsychologist as part of the routine diagnostic algorithm blind to the clinical classification, which was formulated at the end of the clinical-neuropsychological and instrumental evaluation and after the follow-up time by expert clinicians.
The FBI is a 24-item behavioral inventory specifically designed to be administered by a trained examiner to caregivers, who are asked to report behavioral or personality changes from the patient’s premorbid state, and it is aimed to capture symptoms of frontal lobe dementia [10]. FBI items consist of a “negative” group of deficit behaviors (apathy, aspontaneity, indifference, inflexibility, concreteness, personal neglect, disorganization, inattention, loss of insight, logopenia, verbal apraxia, alien hand) and a “positive” group of disinhibition behaviors (perseveration, irritability, excessive jocularity, poor judgement, inappropriateness, impulsivity, restlessness, aggression, hyperorality, hypersexuality, utilization behavior, incontinence). Each item is valuated on a 4-point Likert scale of severity as judged by the caregiver interview. A global score (range 0–72) is computed, as well as two subscale scores for negative (FBI-A) or positive (FBI-B) behaviors. Each subscale score ranges from 0 to 36.
The NPI questionnaire [6] assesses 12 behavioral disturbances occurring in dementia patients: delusions, hallucinations, agitation/aggression, depression/dysphoria, anxiety, euphoria, apathy, disinhibition, irritability/lability, aberrant motor activity, sleep, and eating behaviors. Even in case of NPI, information about changes is obtained from a caregiver, familiar with the patient’s behavior. Both frequency and severity are determined for each of 12 behaviors in case of positive answer to the screening question. While frequency is valuated on a 5-point Likert scale (never, rarely, sometimes, frequently, almost always), severity is evaluated on a 3-point Likert scale (mild, moderate, severe). Finally, a frequency per severity score is computed for each item and all item scores are merge into a global NPI score (range 0–144).
Statistical analysis
First, we assessed FBI internal consistency within the bvFTD sample through Cronbach’s alpha to identify non-contributory items. The scores of the resulting subscales were factor analyzed using the Maximum Likelihood factor analysis. Items were removed if showing a factor loading lower than 0.4.
Based on these results, a shorter version of the FBI was computed (i.e., mini-FBI), and convergent validity was assessed through Pearson’s correlation between NPI overall score and mini-FBI score.
Significant differences in demographic and clinical variables between AD and bvFTD groups were computed based on parametric (t-student) or non-parametric tests (Mann-Whitney U test) according to data distribution, evaluated through Shapiro-Wilk statistics.
To characterize behavioral symptoms in bvFTD and AD, we also computed a summary measure of positive and negative symptoms (“mini-FBI”), as well as a behavioral index (“B-index”) representing the balance between positive and negative symptoms of mini-FBI (i.e., [(negative symptoms – positive symptoms)/(negative symptoms + positive symptoms)]. We then used the positive and negative symptoms, as well as the B-index, to perform a hierarchical cluster analysis on whole patient sample using the Ward’s minimum variance method with a squared Euclidean distance measure.
Parametric or non-parametric ANOVA statistics were then used to compare emerging patient clusters in demographic and clinical features. Tuckey and Dwass-Steel-Critchlow-Flinger post-hoc analyses were used to perform pairwise comparisons in positive and negative symptoms among disease groups.
Finally, ROC curve analyses were computed to derive accuracy of mini-FBI measures in significantly distinguishing bvFTD from AD groups. Cut-off score were derived using the Youden index. Statistical analyses were performed through Jamovi v1.6.23.
RESULTS
The analysis of internal consistency for FBI in the bvFTD group showed a Cronbach alpha of 0.784. Based on the item reliability statistics, 4 items were dropped out (i.e., verbal apraxia, irritability, jocularity, and restlessness). The exploratory factor analyses highlighted two factors, including respectively six negative or positive behavior subscales each. Items classified in Factor 1 (eigeinvalue = 3.85) were apathy, lack of initiative, distractibility, personal neglect, indifference, and loss of insight. Factor 2 (eigenvalue = 1.66) included hypersexuality, inflexibility, inappropriateness, perseveration, inattention, and incontinence mini-FBI score positively correlated with NPI score (rp = 0.61, p < 0.001).
Consistently with clinical diagnosis, bvFTD patients were younger compared to AD (t(71) = –2.89, p = 0.005) and showed higher level of global cognitive functioning as evaluated by the Mini-Mental State Examination (MMSE) (t(71) = 3.15, p = 0.002).
The hierarchical cluster analysis classifying patients based on the presence of positive and negative symptoms, as well as their balance, showed four clusters, characterized by a different distribution of AD and bvFTD patients (χ2(3) = 20.9, p < 0.001). The first cluster mainly included AD patients (Cluster #1, ↑AD-) presenting with mild negative symptoms with no positive behavioral disturbances. The second cluster (Cluster #2, ↑bvFTD+) mainly included bvFTD patients with prevalent positive symptoms, as suggested by the low level of B-index. The third cluster (Cluster #3,
Comparison of demographic and clinical variables in the four groups resulting from hierarchical cluster analysis
bvFTD, behavioral variant of frontotemporal dementia; AD, Alzheimer’s disease; Cluster #1, ↑AD-, predominant AD patients presenting mild negative symptoms with no positive behavioral disturbances; Cluster #2, ↑bvFTD+, predominant bvFTD patients with prevalent positive symptoms; Cluster #3,
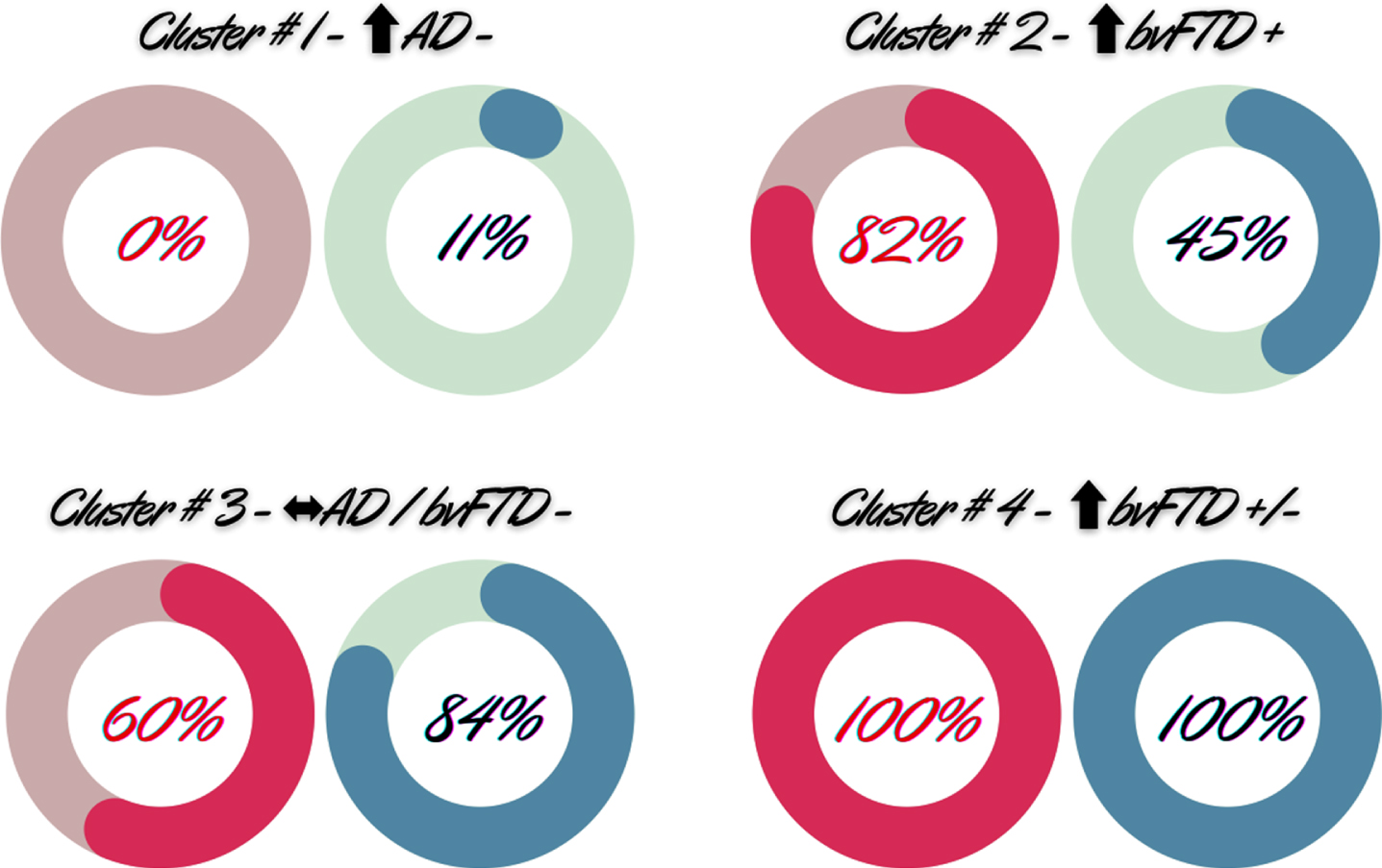
A) Amount of positive (red) and negative (light blue) symptoms in the 4 patient subgroups derived from the cluster analysis. The percentage represents the rate of patients with positive and negative symptoms above the cut-off scores resulting from the ROC curve analysis. Cluster #1, ↑AD-, predominant AD patients presenting mild negative symptoms with no positive behavioral disturbances; Cluster #2, ↑bvFTD+, predominant bvFTD patients with prevalent positive symptoms; Cluster #3,
Finally, ROC analysis comparing mini-FBI performances in distinguishing bvFTD and AD groups highlighted a sensitivity of 73% and a specificity of 76% (cut-off score≥13, AUC = 0.81, SE = 0.049, p < 0.001, accuracy: 74%). Focusing on the contribution of positive and negative symptoms in the differential diagnosis, we found a higher accuracy of positive symptoms in distinguishing bvFTD from AD (cut-off score≥2, AUC = 0.83, SE = 0.048, p < 0.001, sensitivity: 83%, specificity: 76%, accuracy: 79%) compared to negative symptoms (cut-off score≥9, AUC = 0.77, SE = 0.054, p < 0.001, sensitivity: 83%, specificity: 57%, accuracy: 71%) (Fig. 2). Considering the 4 subgroups, 100% of ↑bvFTD+/- and two-thirds (i.e., 67%) of the
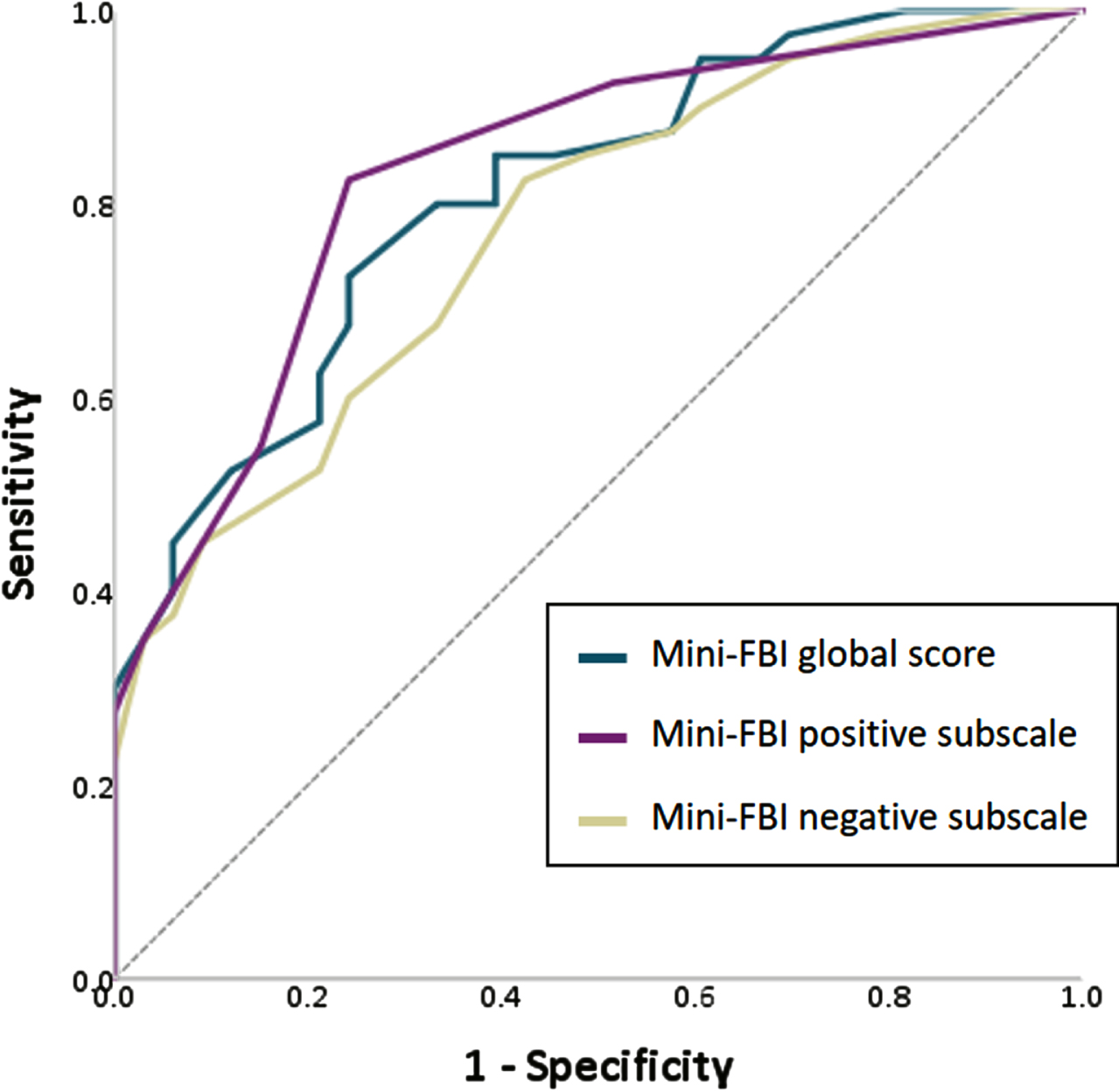
Receiving operating characteristic (ROC) curve for positive (violet), negative (beige) mini-FBI symptoms, as well as global score (green) in bvFTD versus AD patients. Reference line is reported in light grey.
DISCUSSION
The huge amount of new information on the etiopathology (including genetic drivers and dysfunctional molecular pathways) and the endophenotype characterization of the frontotemporal dementia disorders has drastically changed the requirements we place on a cognitive or behavioral clinical measure. The development of accurate clinical measures for a better early and differential diagnosis of behavioral changes in bvFTD represents a clinical research priority for the appropriate use of expansive diagnostic biomarkers and the evaluation of the efficacy of new-generation disease-modify treatment options [33].
The FBI scale has been specifically developed with the aim to identify behavioral changes following frontal lobe dementia, and its relevance is underlined by its use as outcome in clinical trials [34–36]. It has been proved to be more effective than standard neuropsychological testing in detecting FTD, particularly the behavioral variant [16, 37]. However, since the original version of the questionnaire can be rather time-consuming, previous authors proposed possible alternatives [30, 38].
In the current study, we built a shorter version of the FBI (i.e., mini-FBI) and computed new cut-off scores for its clinical implementation. In addition, we analyzed commonalities and differences in mini-FBI in bvFTD compared to AD in order to detect possible differential profiles that could help clinicians in the diagnostic framework. Our findings proved easy administrability and good accuracy of the mini-FBI contributing not only to early differentiate bvFTD from other neurodegenerative disease, among which AD represents one of the most challenging [39, 40], but also to quick identify positive and negative symptoms better contributing to the early diagnosis.
No item centered on language disturbances was included in the mini-FBI. This result can be explained considering the specific focus of this study (i.e., the early differential diagnosis of bvFTD from AD). Language items were included in the original FBI questionnaire with the aim to better pointing towards the identification of a language variant of FTD. Nonetheless, during the last two decades validated and more accurate cognitive tools (see for example the Screening for Aphasia in NeuroDegeneration (SAND) [41] and the Mini-Linguistic State Examination (MLSE) [42, 43] batteries) have been developed to provide more complete and accurate information for the early diagnosis of primary progressive aphasia (PPA). The relevance of language items in FBI questionnaire is thus decreased. Language profile in bvFTD is less severe than that of PPA and usually worsens over time [44]. Severity of speech and language deficits in bvFTD might be associated with global cognitive impairment and predominantly fronto-temporal or temporal predominant atrophy as well as genetic triggers [45]. Language items currently included in the FBI questionnaire (i.e., verbal apraxia and logopenia) may thus be insufficient and inappropriate to capture subtle linguistic alterations typical of early bvFTD.
The cut-off we derived from the mini-FBI scale is in line with what previous found using the whole FBI scale [15], and it is intended to be referred only to bvFTD subjects. Notably, the here-proposed cut-off score is considerably lower if compared to the cut-off score of Alberici et al. (i.e. cut-off = 28.6 [12]) which is the reference for the Italian version of FBI. Crucial differences between the enrolled samples may be responsible of this result. The sample from Alberici et al. [12] included all FTD variants (i.e., bvFTD, PPA, and atypical parkinsonism) and subjects in more advance disease stage (i.e., MMSE = 14.2±10.5) with respect to our sample of mild bvFTD patients (i.e., MMSE = 23.75±3.36). Further replication studies on independent samples of bvFTD patients should be promoted to clarify controversial results as well as longitudinal studies on bvFTD patients at different disease stages may explain the contribution of single items.
Separate investigation of positive and negative FBI sub-scores confirmed previous findings [10] according to which the positive symptomatology might represent a better index in distinguishing bvFTD from AD compared to negative symptoms. This is certainly supported by literature evidence reporting a higher proportion of positive symptoms (e.g., euphoria, disinhibition) in FTD compared to AD patients (see Liu et al. [46] for example). Nonetheless, clustering patient sample on positive and negative symptomatology and considering the unbalance between these two facets highlighted the presence of three subgroups of bvFTD patients with different behavioral profiles. We found indeed one bvFTD subgroup with severe clinical profile characterized by prevalent positive symptoms (i.e., Cluster #2, ↑bvFTD+), one subgroup with combined negative and positive behavioral alterations (i.e., Cluster #4, ↑bvFTD+/-) and a third subgroup with prevalent negative symptomatology (i.e., Cluster #3,
In conclusion, our results support the idea of a multi-facet presentation of bvFTD syndrome. The more we learn about the complexity of this clinical syndrome, the more necessary it is to develop refined measures and to combine different cognitive instruments for an individualized diagnosis. The use of short questionnaire as the mini-FBI, capable of easily exploring behavioral alterations in their full complexity without being time-consuming (i.e., the administration of the mini-FBI lasts about 5 min), should be recommended as gateway for the selection of second-level neuropsychological measures. These latter can be in fact more sensitive to detect the various degree of alterations of positive and/or negative symptoms that may characterize the different phenotypical presentations of bvFTD in early phases. In this sense, the caregiver-administered version of Interpersonal Reactivity Index (IRI) [55] or the revised Self-Monitoring Scale (rSMS) [9] could be valid option to evaluate social behavior and social control functioning in bvFTD with prevalent positive symptoms (e.g., irresponsibility, inappropriateness, impulsivity, and hyperorality). Comparably, the assessment of subjective rating discrepancy score between the self-evaluated scoring of cognitive complaint (e.g., self-administered IRI scores) and the information gathered by the caregiver (i.e., caregiver-administered IRI scores) may help in better quantify loss of insight in cognitivepatients [56].
Overall, although we acknowledge some limitations in this study, such as a single center sampling, a relatively small sample size, and the lack of neuropathological confirmation of the dementia diagnosis, the mini-FBI could be promoted as a useful tool to evaluate negative and positive symptom profiles in suspected bvFTD cases. Future studies, also including neuropsychological and imaging data, will allow to better characterize different cognitive-behavioral phenotypes distinguishing bvFTD from AD patients.
The mini-FBI use should be recommended to aid clinicians in the early phases of the complex diagnostic path of FTD and in the assessment of behavioral profile changes in response to disease-modifying treatments. Cost-effectiveness of its regular use in the first-level neuropsychological testing battery of suspected bvFTD patients, however, needs to be assessed in future longitudinal observation studies investigating also its combination with different second-level behavioral measures.
Footnotes
ACKNOWLEDGMENTS
We acknowledge the Italian Association for Frontotemporal Dementia (AIMFT) that always encouraged and supported our work. We thank patients and caregivers for their help to foster our research.
Mondino Foundation IRCCS was funded by Italian Ministry Ricerca Corrente 2022–2024.