
Abstract
Background:
Identifying modifiable risk factors, such as obesity, to lower the prevalence of Alzheimer’s disease (AD) has gained much interest. However, whether the association is causal remains to be evaluated.
Objective:
The present study was designed: 1) to make a quantitative assessment of the association between obesity and AD; 2) to validate whether there was a causal association between them; and 3) to provide genetic clues for the association through a network-based analysis.
Methods:
Two-sample Mendelian randomization (2SMR) analysis, meta-analysis, and protein-protein interaction (PPI) network analysis, were employed.
Results:
Firstly, the meta-analysis based on 9 studies comprising 6,986,436 subjects indicated that midlife obesity had 33%higher AD odds than controls (OR = 1.33, 95%CI = [1.03, 1.62]), while late-life obesity were inversely associated with AD risk (OR = 0.57, 95%CI = [0.47, 0.68]). Secondly, 2SMR analysis indicated that there was no causal association between them. Thirdly, CARTPT was identified to be shared by the anti-obesity drug targets and AD susceptibility genes. Further PPI network analysis found that CARTPT interacted with CD33, a strong genetic locus linked to AD. Finally, 2SMR analysis showed that CNR1 could be a protective factor for AD.
Conclusion:
Multiple bioinformatic analyses indicated that midlife obesity might increase the risk of AD, while current evidence indicated that there was no causal association between them. Further, CARTPT might be an important factor linking the two disease conditions. It could help to better understand the mechanisms underlying the associations between obesity and AD.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is widely recognized as the most common cause of age-related neurodegenerative disease. According to the report of Alzheimer’s Disease International (ADI) in 2019, it was estimated that over 50 million people around the world were affected by dementia, and this figure was expected to rise steadily in the following decades due to the ageing of the population [1, 2]. Despite extensive efforts have been devoted to developing anti-AD drugs, the therapeutic effects of drugs currently available for AD are still limited and cannot effectively prevent the development of AD [1, 2]. Therefore, the identification of modifiable risk factors to help reduce the risk of developing AD has become a promising approach for the prevention, intervention, and drug discovery of AD.
As a common chronic metabolic disease worldwide, obesity has also become a major public health problem due to the increase in global incidence [3–5]. Two large population and long-term studies provided convincing evidence that since 1980, the prevalence of obesity has increased continuously across different countries and age groups, and in males and females [6, 7]. According to statistics, more than 700 million people, including children and adults, suffered from obesity in 2015 [7]. Besides, another challenge posed by obesity is the harm in a variety of obesity-related diseases. In the past decades, obesity has been widely reported to be associated with the development of multiple chronic diseases, including AD. Previous studies have demonstrated that subjects with obesity had a higher risk of developing AD and dementia, especially in midlife [8–11]. However, not all studies consistently showed that obesity could affect the risk for AD, and especially whether there is a causal association between obesity and AD remains to be further evaluated. In addition, AD drug development has encountered great difficulties owing to the numerous failures. The recent web-based pharmacological research has provided a new way to deepen the understanding of the mechanisms of drug action and identify potential drug targets [12]. Investigating the interactions between anti-obesity drug targets and AD genes may provide useful clues for AD drug discovery.
Therefore, the present study was designed with the following aims: 1) conducting a quantitative assessment of the association of obesity predicting the incidence of AD; 2) evaluating whether there was a causal association between obesity and AD; 3) performing a network-based analysis of the interactions between anti-obesity drug targets and AD susceptibility genes; and 4) also exploring the causal effects of anti-obesity targets on the risk of AD.
MATERIALS AND METHODS
Meta-analysis
Based on published literature and MeSH, we identified keywords of “obesity” and “Alzheimer’s disease” and searched the PubMed database until June 2019. All searches were restricted to original clinical studies, and the types like case reports, re-views, animal studies, were firstly ruled out. Furthermore, the reference list was also reviewed for covering possible additional studies. During the data collection, two independent investigators (QSZ and LM) retrieved potentially eligible literature and reached a consensus finally. The inclusion of studies in this paper met the following three criteria: 1) studies reporting AD incidence as an outcome; 2) interested in obesity at baseline and/or at the end of follow-up; and 3) estimation of the impact of relative risk (RR), hazard ratio (HR), or odds ratio (OR) with 95%confidence intervals (CIs). A detailed data extraction, comprising first author, publication year, number of participants, adjustments, age at baseline, RR, HR or OR estimates, 95%CIs and corresponding p-value, was conducted among the included studies. The calculation of the extracted data was performed by the Stata statistical software version 12.0 using random-effects model. In the meta-analysis, Q-test and I2 score were used to evaluate heterogeneity, while publication bias of the included studies was evaluated by funnel plot and Egger’s test.
Data sources for obesity
The data of obesity is obtained from the MR-Base platform through the MR-Base GWAS catalog, and the genetic data is derived from the Genetic Investigation of ANthropometric Traits (GIANT) meta-GWAS statistics, which included six obesity-related traits. Among them, obesity class 1 (BMI ≥30 kg/m2) was selected as the exposure, comprising 32,858 obesity cases and 65,839 controls [13]. The significant single nucleotide polymorphism (SNPs) were included in our study with a threshold of p-value<5.0 × 10–8.
Data sources for AD
The SNPs of AD were obtained from the meta-GWAS statistics of International Genomics of Alz-heimer’s Project (IGAP), comprising 17,008 AD cases and 37,154 controls [14]. The significant SNPs were included in the study with a threshold of p-value<1.0×10–5. In addition, the identified significant SNPs were mapped into related genes according to the location of SNPs on the human chromosome.
Identification of anti-obesity drug targets
To obtain target genes of anti-obesity drugs, we searched the DrugBank database (http://www.drugbank.ca) with the searching term “obesity” and “anti-obesity” for drugs until June 2019 [15]. Because of the lack of semantic information, the results of keyword retrieval were comprehensive, but not accurate enough. Therefore, it was necessary to further filter the retrieval results to exclude invalid information. The descriptions or pharmacological indications of drugs that met the criteria, including the reduction in appetite or other anti-obesity effects, were collected as available anti-obesity drugs. Finally, the relevant information of available anti-obesity drugs including the drug name, accession number, target gene and UniProt name was extracted in the study.
Protein-protein interaction (PPI) network
The overlapped genes were identified by comparing the anti-obesity drug target genes with AD susceptibility genes. To investigate the PPI information between overlapped genes and AD susceptibility genes, we constructed network-based analyses by STRING databases (Version 11.0) [16]. The generated network was visualized by Cytoscape software (Version 3.7.1) [17]. Besides, we mapped the combined score to the edge size (high values to big sizes), the node degree to the node size and color (high values to big sizes and dark color).
Two-sample Mendelian randomization methods
In the present study, the software R (version 3.5.3) and R packages (TwoSample MR package 0.4.22) provided by MR-Base were used to automate two-sample Mendelian randomization (2SMR) analysis [18]. On the one hand, we chose SNPs of obesity as instrumental variables to infer the causal association between obesity and AD. On the other hand, based on GTEx eQTL catalog, we also identified SNPs to proxy the protein targets of anti-obesity drugs [19], and the effect sizes of these SNPs were used to estimate the association between anti-obesity target genes (exposure) and AD (outcome). In the 2SMR analysis, strong correlation (p < 5×10–8) and independent inheritance (r2 < 0.001), without any link disequilibrium (LD), were selected to summarize the data for further analysis. Inverse variance weighting (IVW) was employed for 2SMR statistical analysis, and all statistical tests were considered to be statistically significant at p-value <0.05.
RESULTS
Meta-analyses of AD risk with obesity
We identified 1632 potential related studies thr-ough a computerized literature search. The flow diagram of the selection of eligible studies is shown in Fig. 1. A total of 9 studies including 18 sets of data met inclusion criteria, comprising a total population of 6,986,436 [20–28]. The 16 sets of data were divided into two subgroups according to the age of midlife (<65 years old) or late-life (≥65 years old), and two sets of data were excluded due to not meeting these criteria. Table 1 provides the main characters including the first author, year of publication, age, country, number of subjects, adjustments, risk factor, the OR and 95%CI, extracted from each study. The overall result of the meta-analysis showed no statistical significance, which is shown in Fig. 2. In these studies, statistical heterogeneity was found (p = 0.000, I2 = 97.3%), and the funnel plot showed symmetric distribution, indicating no evidence of publication bias (Fig. 3). Further subgroup analysis indicated that the midlife obesity subjects had 33%higher AD odds than controls (OR = 1.33, 95%CI = [1.03, 1.62]), while late-life obesity individuals were inversely associated with odds of AD (OR = 0.57, 95%CI = [0.47, 0.68]).

Selection flow of studies for inclusion in the meta-analysis.
Main characteristics of studies included in the meta-analysis of obesity predicting the risk of AD
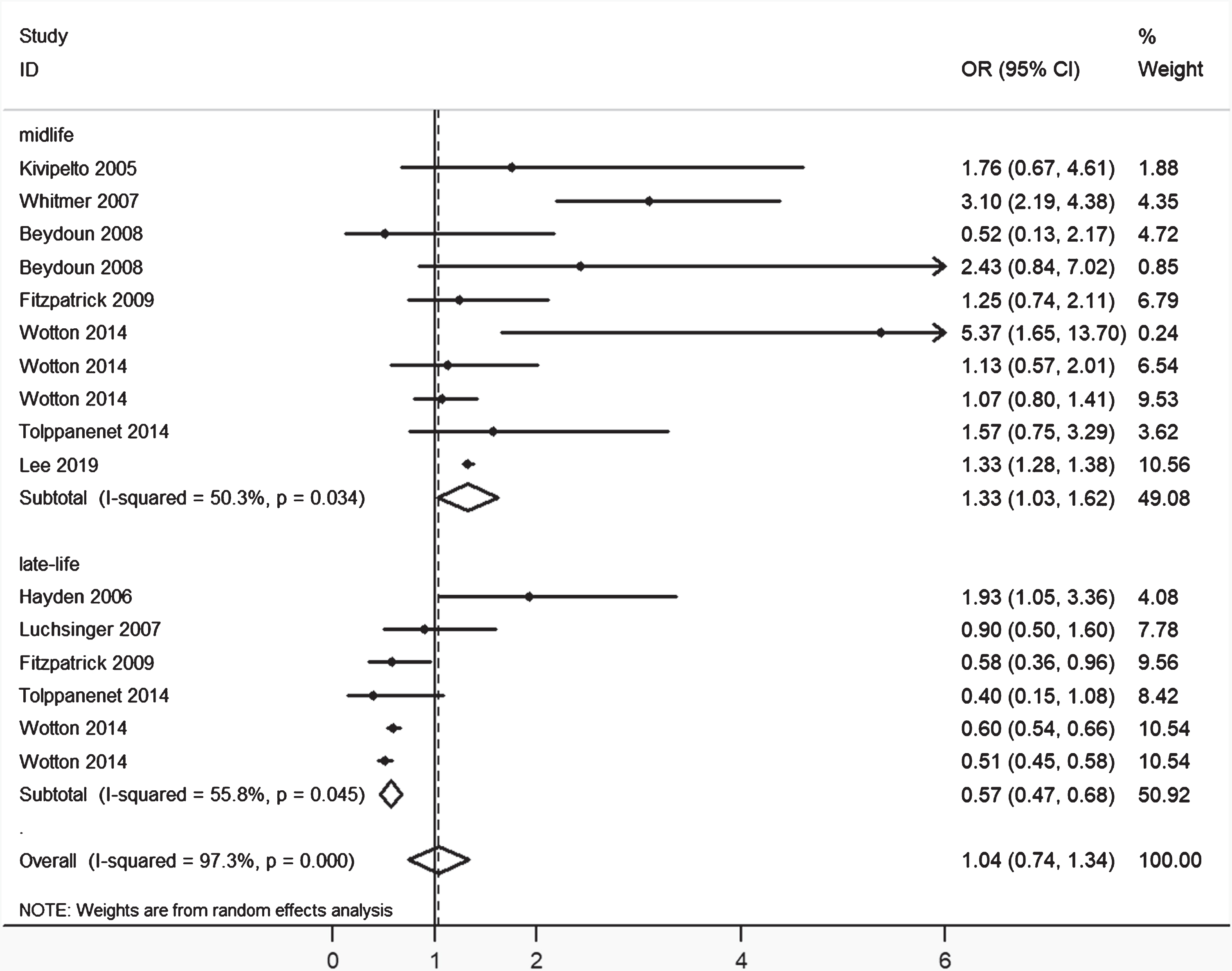
The pooled estimate of OR and 95%CI of obesity and AD. OR is represented by squares, whose sizes are proportional to the sample size of the relative study. The whiskers represent the 95%CI. The diamond represents the pooled estimate based on the random-effects model, with the center representing the point estimate and the width representing the associated 95%CI.
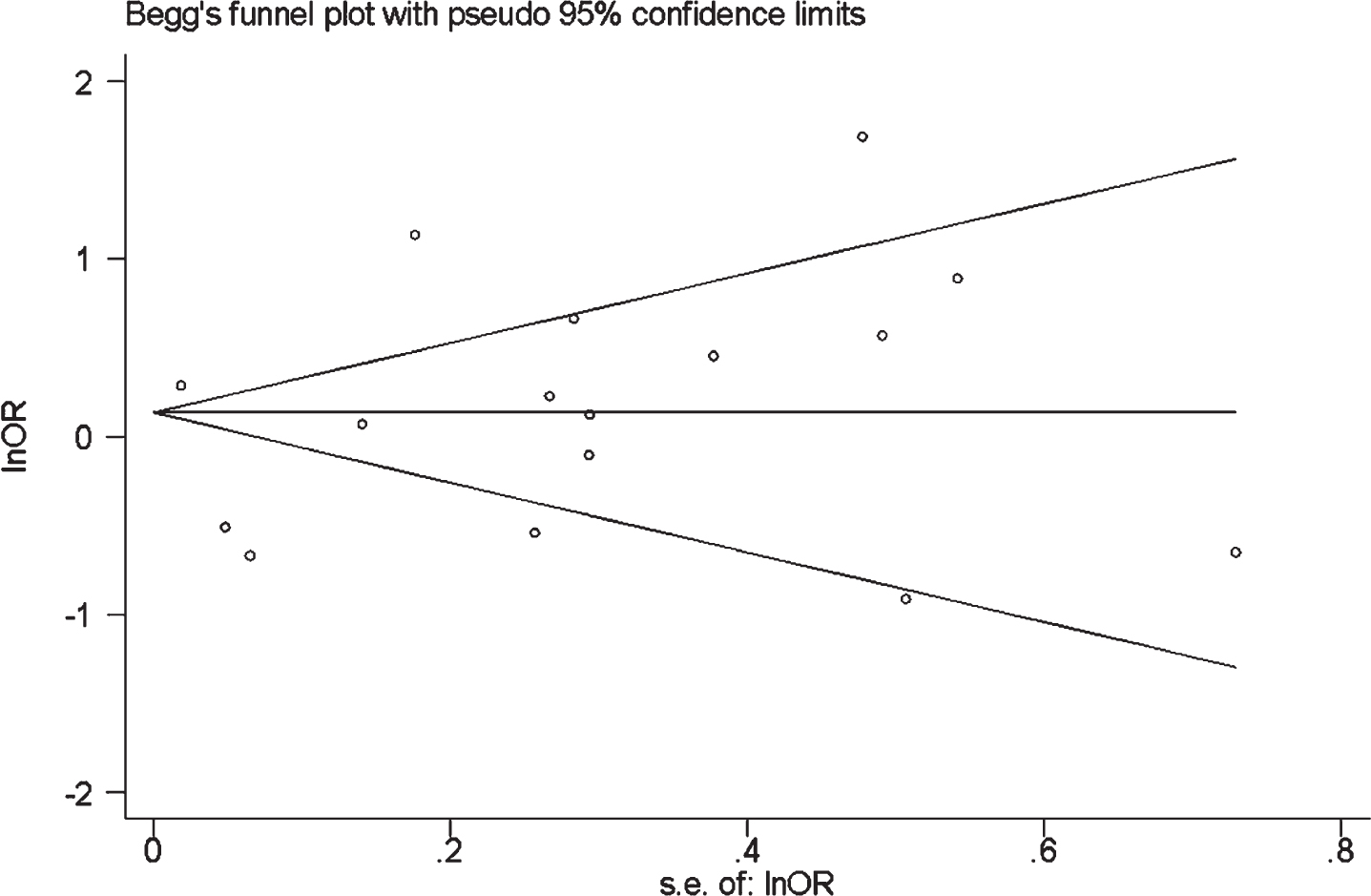
Begg’s test was used to test the publication bias. The funnel plot showed symmetric distribution in the figure of overall meta-analysis (eight sets of data were above the line and the other eight sets of data were below the line), suggesting that there did not appear to be a publication bias.
Causal associations between obesity and AD
In the 2SMR analysis, we used SNPs significantly related to obesity (p < 5×10–8) as instrumental variables. A total of 14 independent SNPs were linked to obesity by independent and LD analyses, and it was found that the OR of obesity and AD risk was 0.97 (95%CI = [0.89, 1.06], p = 0.49) in the random-effects IVW model (Table 2). As the p-value of the 2SMR result was larger than 0.05, it was inferred that there was no significant causal association between obesity and AD.
2SMR estimates of the causality between obesity and AD
Comparison analysis and PPI network
A total of 36 anti-obesity drugs were obtained from the DrugBank database, covering 31 target genes (there were 15 drugs without identified targets). The details of these drugs including drug name, accession number, target genes and UniProt name are displayed in Table 3.
Main characteristics of the anti-obesity drugs
When setting p-value < 1.0×10–5 as cutoff criteria, we collected 2,746 SNPs associated with AD. By mapping the significant SNPs to genes on the basis of the NCBI database, 152 AD susceptibility genes were identified and included in this study. Through overlapping the anti-obesity drug target genes and AD susceptibility genes, CART prepropeptide (CARTPT) was identified to be shared. As a neuropeptide, CARTPT is involved in the regulation of appetite and satiety. The PPI network that followed was constructed from the STRING databases, including 152 AD susceptibility genes and overlapped gene CARTPT. The final network was visualized by Cytoscape software as shown in Fig. 4. According to this network, it was found that the overlapped gene CARTPT interacted with CD33, a strong genetic locus linked to AD.
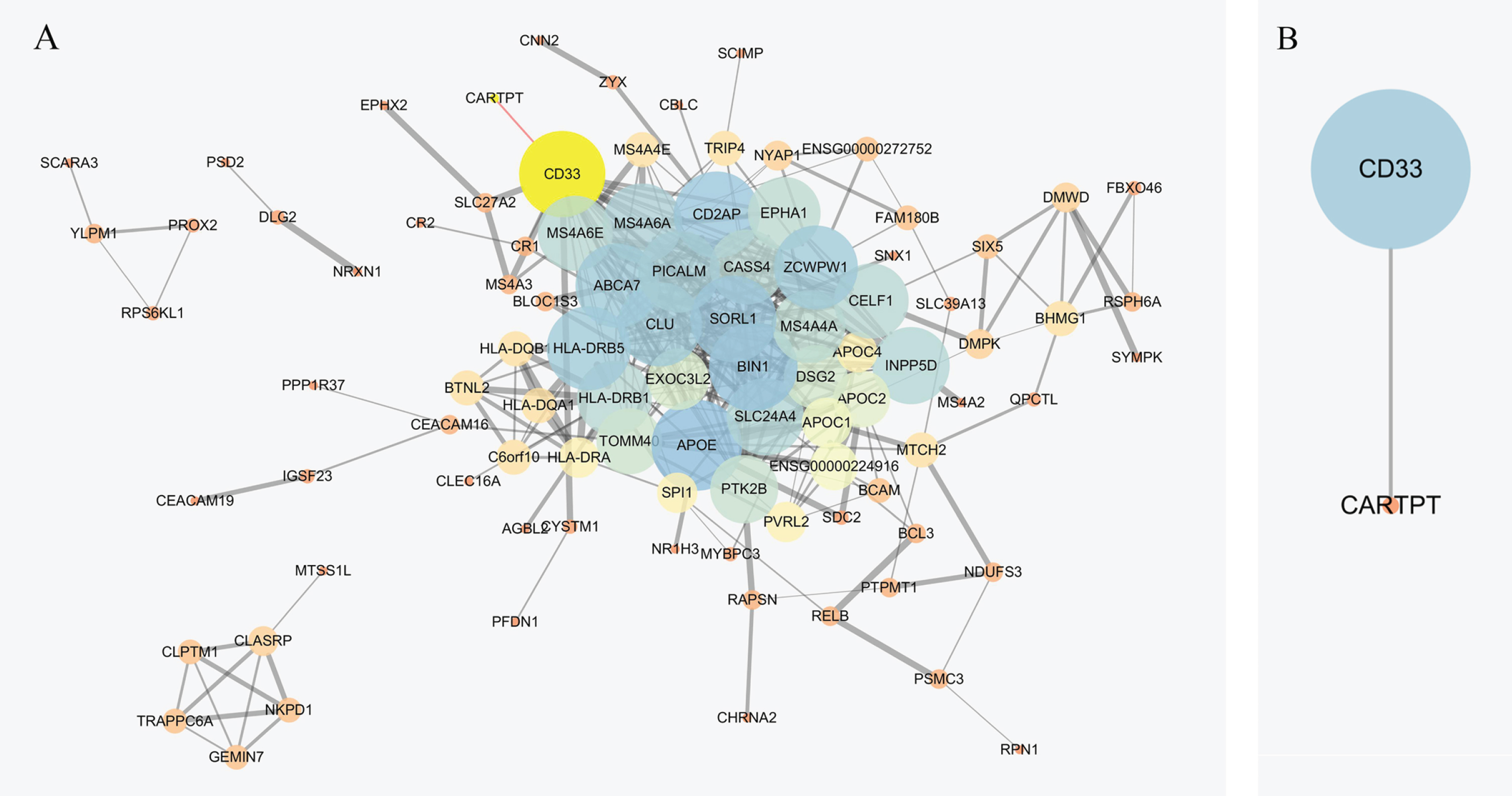
PPI analysis of overlapped gene and AD susceptibility genes. A) A network-based analysis based on overlapped gene and AD susceptibility genes. B) A sub-network analysis based on CARTPT and first neighbor of AD susceptibility genes.
Causal associations between the anti-obesity drug target genes and AD
By using SNPs associated with each anti-obesity drug target gene as instrumental variables, we condu-cted a 2SMR analysis for the causal associations between each anti-obesity drug target and AD risk (Table 4). A total of 2 independent SNPs (p < 5×10–8, r2 < 0.001) have an association with cannabinoid receptor 1 (CNR1) gene by independent and LD analyses. Genetically predicted the CNR1 gene could be a protective factor in AD (IVW, OR = 0.95, 95%CI = [0.92, 0.99], p = 0.01). Further investigation of the PPI network demonstrated that the CNR1 gene interacted with CARTPT (Fig. 5), the common gene among the anti-obesity drug targets and AD susceptibility genes, identified above. In combination with the interaction between CARTPT and CD33, it was inferred that CARTPT may be an important linker between anti-obesity drug targets and AD.
MR estimates of the causality between anti-obesity targets and AD
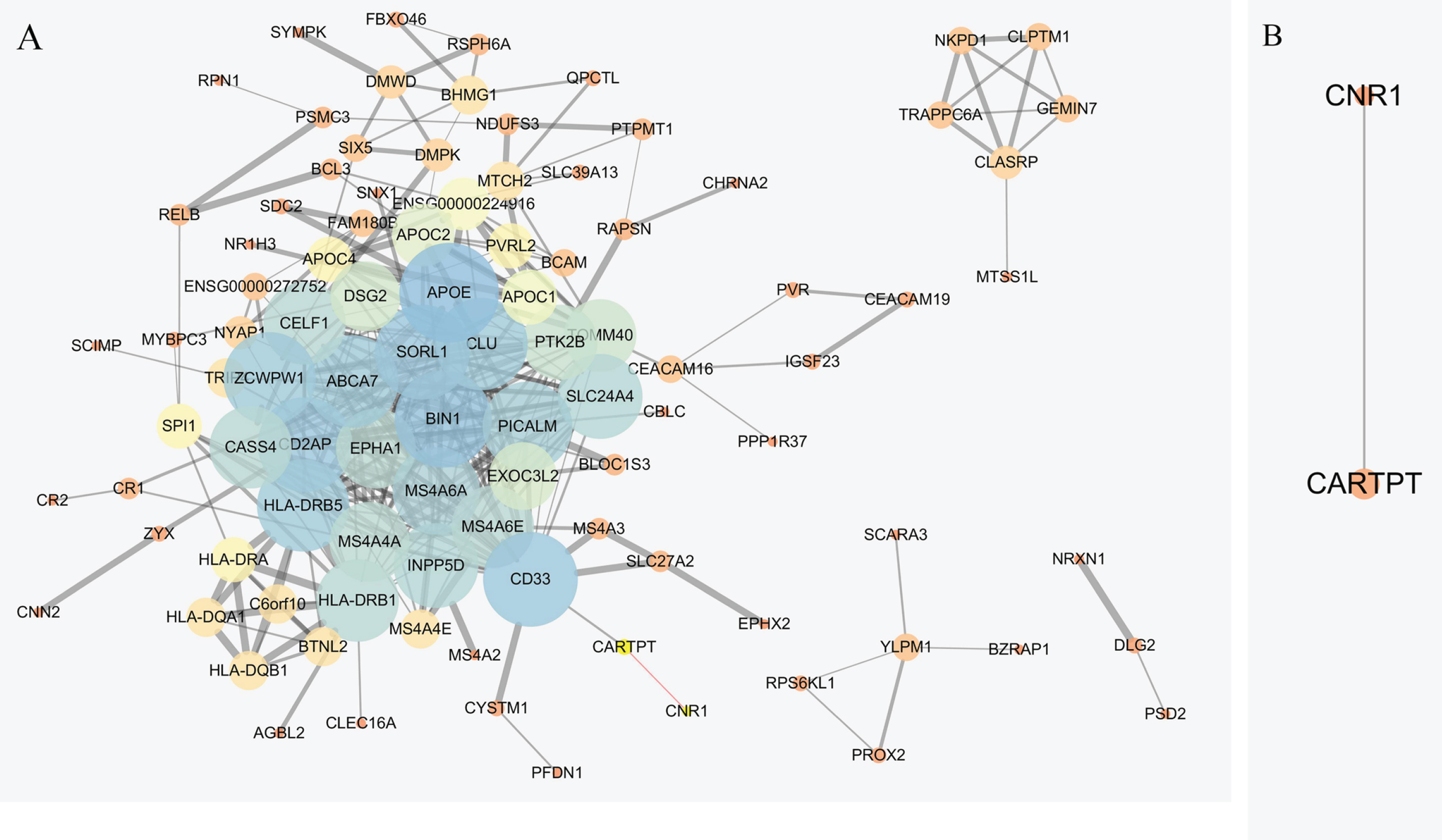
PPI analysis of CNR1 and AD susceptibility genes. A) A network-based analysis based on CNR1 and AD susceptibility genes. B) A sub-network analysis based on CNR1 and first neighbor of AD susceptibility genes.
DISCUSSION
The present results were significant in at least two major respects: the first part focused on epidemiological associations, and the second focused on the PPI and 2SMR analysis of anti-obesity drug targets and AD susceptibility genes. Firstly, we performed a quantitative analysis and confirmed a significantly increased incidence for AD by 33%in midlife obesity subjects, implying that midlife obesity may be a risk factor for AD. Several studies have revealed that obesity was associated with the structure and function changes of the brain, and the higher the BMI, the lower the brain capacity, supporting those obese people has a higher risk than non-obese subjects [29–31]. It has also been demonstrated that obesity is associated with inflammation, oxidative stress, and mitochondrial dysfunction, all of which are involved in the development of neurogenesis [32–34]. Besides, leptin deficiency, as a risk factor of obesity, also played a role in memory and may lead to memory impairment [35, 36]. Further investigation demonstrated that circulating leptin was associated with a reduced incidence of dementia and AD [37].
Secondly, the present analysis identified CARTPT to be overlapped between anti-obesity drug targets and AD susceptibility genes. CARTPT is a neuropeptide involved in regulating appetite and satiety. The mutations in CARTPT have been reported to be related to reduced metabolic rate, obesity, and diabetes [38]. Further, amphetamine, the drug that targets CARTPT, has also shown promise in improving AD and dementia in the elderly [39]. Besides, the investigation of the PPI network that the overlapped gene CARTPT interacts with CD33. It has been found that CD33 impairs microglia-mediated Aβ clearance, leading to the formation of amyloid plaques in the brain [40]. In particular, the increase of CD33 level was positively correlated with the amyloid plaque and disease severity [40].
Another important finding from 2SMR analysis was that CNR1, a promising anti-obesity drug target, could be a potential protective factor in AD. As shown in Table 3, we have collected multiple anti-obesity drugs targeting CNR1, including rimonabant (approved, investigational), V24343 (investigation-al), CP-945598 (investigational), AVE-1625 (investigational), and SLV319 (investigational). The protein encoded by CNR1 is a member of the guanine-nuc-leotide-binding protein (G-protein) coupled receptor family and involved in the cannabinoid-induced CNS effects. The pathways involved in CNR1 included the Rap1 signaling pathway, neuroactive ligand-receptor interaction, thermogenesis, and retrograde endocannabinoid signaling. Previous research also indicated that CNR1 was significantly downregulated in the presence of AD [41]. Further, recent studies have also found that AD could be treated by modulating the endocannabinoid system [42]. Most recently, it has been revealed that abnormal expression of CNR1 may impair long-term potentiation and induce AD [43].
Limitations
Several limitations deserve to be mentioned. First, the information in the current studies was insufficient to enable assessment of the association of obesity with AD risk in subgroups, such as different sexes. Second, in the meta-analysis, the obesity levels in the included studies varied, which may have an impact on the strength of the association between obesity and AD. Third, in 2SMR analysis, the relatively small number of SNPs can only interpret the limited causal association. Fourth, the currently available data cannot permit us to perform the age subgroup MR analysis for the causal association between obesity and AD.
CONCLUSIONS
To summarize, the present study confirmed an increased risk for AD in midlife obese subjects and provided insights into the mechanisms underpinning the associations between the two diseases through PPI and 2SMR analysis. These findings might be valuable for the development of AD drug targets and encourage future experimental validations.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the Shandong Provincial Natural Science Foundation (Grant No. ZR2019MH020), University Youth Innovation Team of Shandong Province (Grant No. 2019KJK017), Shandong Provincial Key Research and Development Program (Grant No. 2018GSF121001) and Talent Program of Zibo.