
Abstract
Background:
To fully characterize the risk for dementia associated with cigarette smoking, studies must consider competing risks that hinder the observation of dementia or modify the chance that dementia occurs (i.e., death). Extant research examining the competing risks fails to account for the occurrence of death following dementia, limiting our understanding of the relation between smoking and dementia.
Objective:
Examine the impact of smoking status, lifetime smoking exposure, and duration of abstinence on incident dementia, death following dementia, and death without dementia.
Methods:
Multi-state models estimated hazard ratios (HR) for 95% confidence interval (CI) of 10,681 cognitively healthy adults for transition from baseline to dementia, baseline to death, and dementia to death based on smoking status, lifetime cigarette exposure, and abstinence duration.
Results:
Compared to never smokers, current smokers had increased risk of dementia (HR = 1.66; 95% CI 1.18– 2.32; p = 0.004), and death from baseline (HR = 2.98; 95% CI 2.24– 3.98; p < 0.001) and incident dementia (HR = 1.88; 95% CI 1.08– 3.27; p = 0.03). Pack years increased risk of death from baseline (HR = 1.01; 95% CI 1.00– 1.01; p < 0.001), but not dementia risk (HR = 1.00; 95% CI 1.00– 1.00; p = 0.78) or death following dementia (HR = 1.01; 95% CI 1.00– 1.01; p = 0.05). Recent quitters (quit < 10 years), compared to never smokers, had increased risk of death after baseline (HR = 2.31; 95% CI 1.55– 3.43; p < 0.001), but not dementia (HR = 1.17; 95% CI 0.73– 1.88; p = 0.52) or death following dementia (HR = 1.01; 95% CI 0.42– 2.41; p = 0.99).
Conclusion:
Current smoking increases the risk for dementia and death, but dementia is better attributed to smoking recency than lifetime exposure. Smoking cessation at any age might reduce these risks for cognitively healthy individuals.
INTRODUCTION
Cigarette smoking is the leading preventable cause of death and disability in the United States (U.S.), accounting for 480,000 deaths and over $300 billion in medical costs annually [1, 2]. Smoking harms nearly every organ in the human body, including the brain [2]. Although the link between smoking and various forms of dementia is not singular, smoking is thought to contribute to dementia risk, either directly or indirectly (e.g., via cardiovascular health [3]). Cigarette smoking prospectively increases the risk of Alzheimer’s disease onset by 70%, accounting for 13.9%of individuals with Alzheimer’s disease and related dementias (ADRD) [4–6]. Currently, 5.8 million adults have ADRD, resulting in annual medical costs of approximately $290 billion [7]. Moreover, the incidence of dementia is expected to triple by 2050 [7]. Smoking and ADRD represent two of the most devastating public health crises that face the U.S. today [1, 7].
Unfortunately, the smoking-dementia relationship is continually questioned [8, 9], possibly due to early studies suggesting that smoking protected against dementia onset [10, 11]. However, a large 2010 meta-analysis demonstrated that tobacco industry affiliation moderated the effects of smoking on dementia; studies affiliated with the tobacco industry showed favorable or null results, while the majority not affiliated with the industry demonstrated consistent negative impact of smoking on dementia [12].
Competing risks (i.e., events of similar clinical importance that prevent or alter the likelihood of the main outcome of interest such as dementia [13]) complicate studies of geriatric populations because increasing age (the strongest risk factor for ADRD [7]) is associated with risk for medical co-morbidities [14] and they may further underestimate the relationship between smoking and dementia. The multitude of negative health effects of cigarette smoking and known impact on mortality [1, 2] may result in a smoker not developing dementia, or being excluded from studies examining risk of dementia, due to earlier mortality and subsequent ineligibility for epidemiological studies [15]. Therefore, case control studies (versus cohort studies) may underestimate the risk of cigarette smoking on dementia due to the competing smoking-related risks of death and disease (i.e., cardiovascular, lung, cancer) [16].
Recent work by Abner and colleagues [17] utilized Fine and Grey’s competing risk model [18] to address competing risks and found that smoking was associated with an increased risk of death, but not dementia. This competing risk model breaks down the composite outcome of death or dementia (Fig. 1A) into subdistributed hazards to more accurately determine the impact of smoking on competing outcomes (Fig. 1B). The Fine and Grey method [18], however, does not allow for transition from dementia to death. A multi-state model (Fig. 1C), that accounts for the informative eventuality of death and allows for transition from baseline to dementia, and also from dementia to death, would provide the most comprehensive estimate of the effect of smoking on dementia [19].
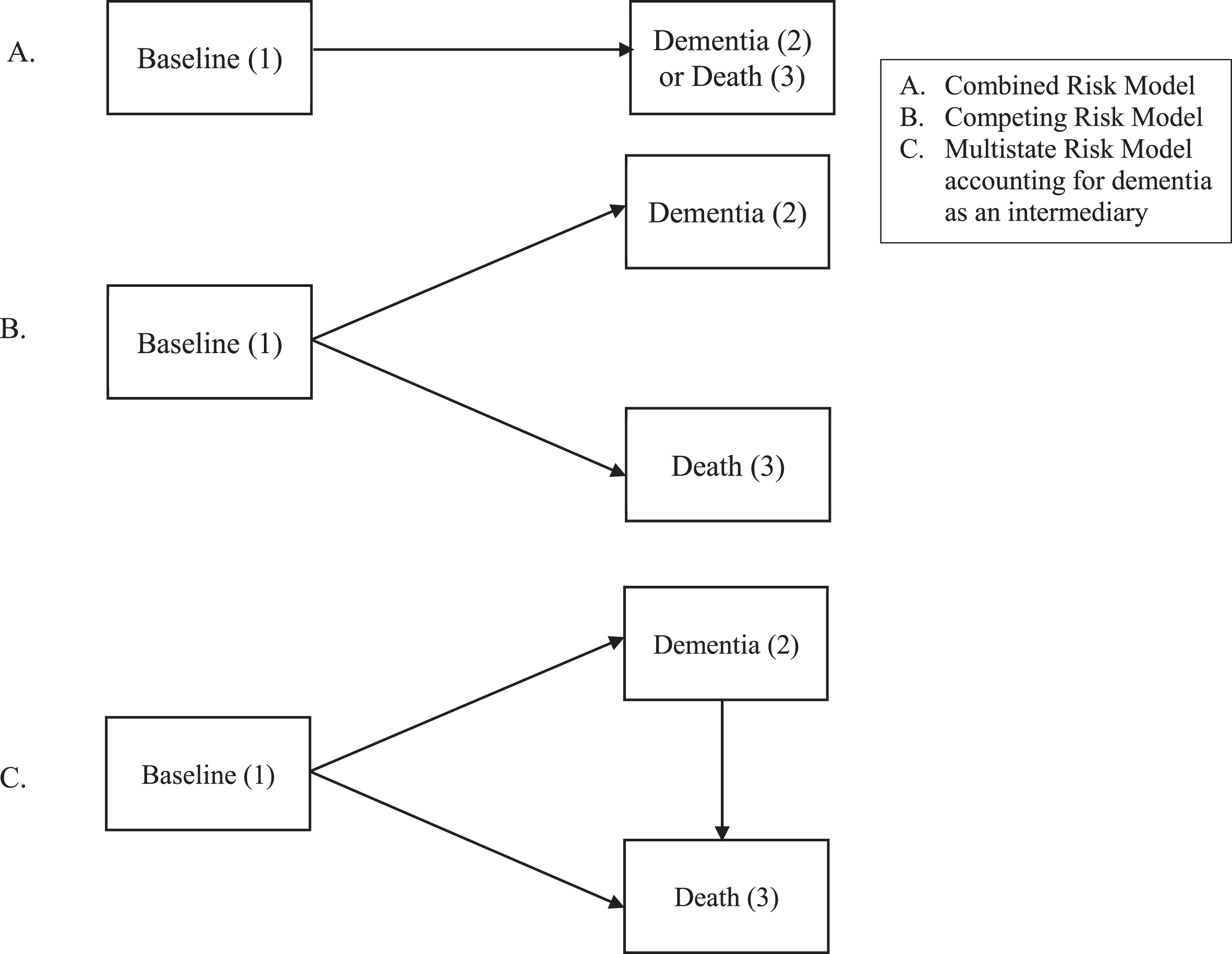
Benefit of multistate models in dementia risk (adapted from [41]).
Inclusion of potential proximal variables for de-mentia, like nursing home placement, would also allow for a more comprehensive assessment of the impact of smoking on dementia. More than two-thirds of nursing home residents have dementia [20], making it one of the primary reasons for nursing home placement [21]. Therefore, nursing home placement may be a proxy for undiagnosed dementia. Although the literature is limited, findings generally support that smoking is linked to increased risk for nursing home placement [22].
Granular analyses of the impact of various smok-ing-related variables (e.g., lifetime smoking, current smoking, duration of abstinence) on dementia risk is necessary, especially in models considering risks for dementia, death, and death following dementia. These variables provide insight into possible biological mechanisms related to the damage caused by smoking (e.g., dose effect) and whether longer abstinence can ameliorate this risk. Although research suggests that former smokers are at decreased risk for dementia onset compared to current smokers [6], it remains unclear how long it takes for smoking-related risk to abate. Research suggests greater lifetime tobacco exposure is related to increased risk of various forms of dementia, but results are mixed [17, 24]. These studies do not include nursing home placement as potential indicator of dementia or account for competing smoking-related risks (i.e., death), perhaps underestimating the impact of smoking on incident dementia. The lone study utilizing competing risk analyses [18] does not examine the transition from dementia to death, and uses a relatively small sample (N = 531) from one, racially homogenous, U.S. location [17].
The current study examined the impact of smoking status, lifetime smoking exposure, and duration of abstinence on the key outcomes of incident dementia diagnosis (including dementia indicated by a composite of nursing home placement and a cognitive rating scale), death, and the transition from dementia to death among a large, racially diverse sample of baseline cognitively healthy adults to provide insight into the impact and potential mechanisms of action of this modifiable risk factor. Using data from the National Alzheimer’s Coordinating Center’s (NACC) Uniform Data Set (UDS) [25], we tested four hypotheses: 1) compared to never smokers, current smokers will be at elevated risk for subsequent dementia onset as well as death directly following baseline and after dementia (Model 1); 2) former smokers (those who quit smoking prior to baseline) will be comparable to never smokers in terms of subsequent dementia onset (Model 1); 3) among all participants, greater lifetime tobacco exposure will be associated with earlier onset of dementia as well as death (Model 2); and 4) the longer participants are abstinent, the more comparable they will be in terms of dementia risk compared to never smokers (Model 3).
METHODS
Study design and participants
The NACC UDS [25] collects data from multiple U.S.-based Alzheimer’s Disease Centers (ADCs). Approximately 725 variables including, but not limited to, sociodemographic, medical history, current medications, family history, neurological examination findings, functional status, neuropsychological test results, clinical diagnoses, imaging, and genetic information were collected (but not required) for each participant. Clinicians determined clinical diagnoses (e.g., normal cognition, dementia) at the initial visit and follow-up visits using clinical data collected at the research visit (Supplementary Material). Data were collected from 33,444 participants between September 2005 to December 2018. Inclusion criteria were completion of baseline and at least one follow-up visit, baseline age ≥45 years old, and baseline cognitively healthy status. To examine the impact of smoking variables on subsequent dementia diagnosis, participants with a baseline diagnosis of dementia or mild cognitive impairment (MCI) were excluded, as well as those predisposed to or diagnosed with strongly heritable forms of dementia (Down syndrome, dominantly inherited Alzheimer’s disease (AD) mutation, hereditary frontotemporal lobar degeneration (FTLD) mutation, or hereditary mutation other than AD or FTLD). Further exclusion criteria by model are described in the analysis section (Fig. 2). Participants included in these analyses (N = 10,578) were, on average, 72 (SD 9.5) years old at baseline.
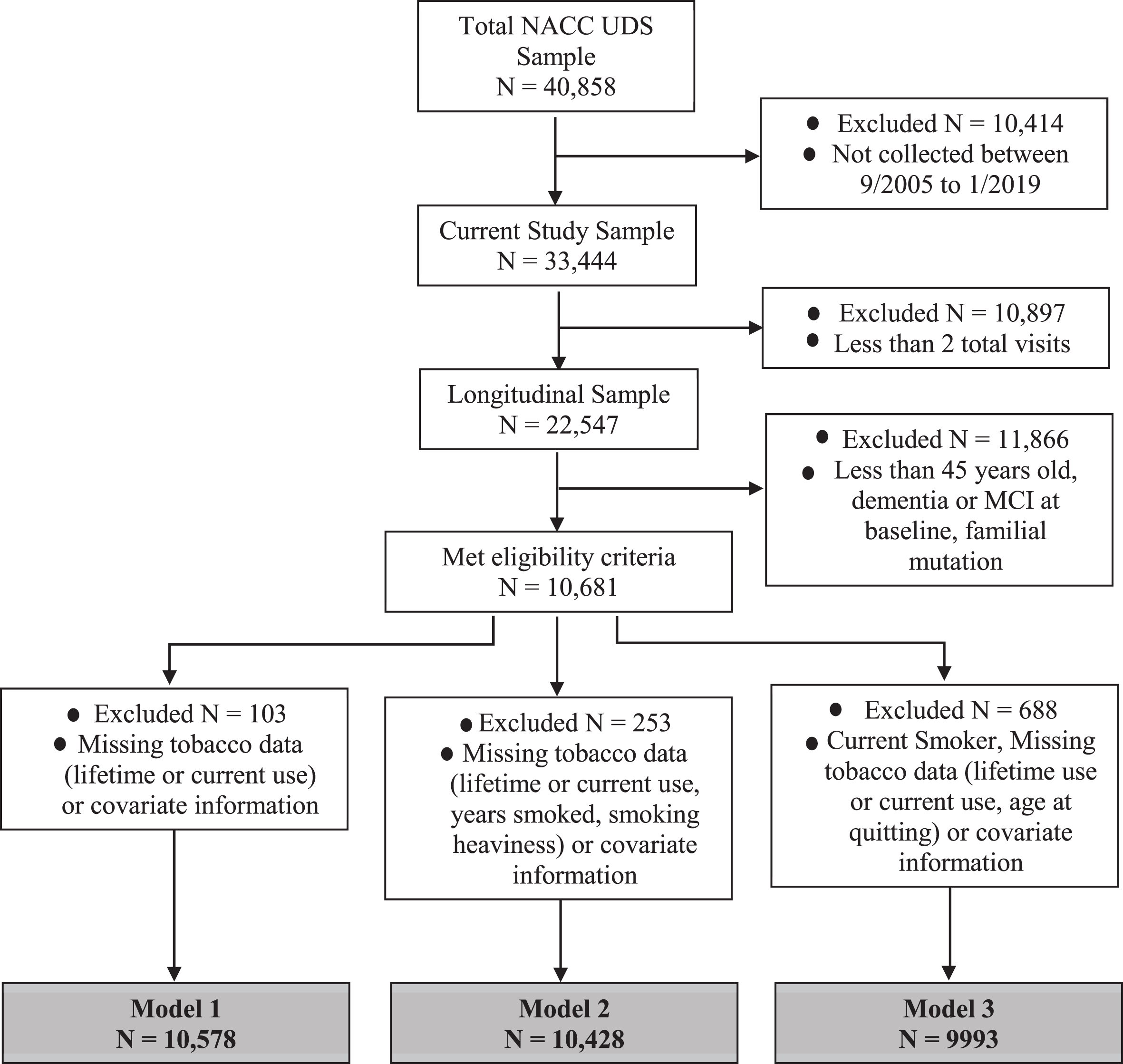
Consortium diagram.
Measures
Tobacco-related information was consistently collected at baseline only; follow-up appointments completed after March 2015 did not assess smoking information. Smoking status was coded as follows. Current smokers reported smoking > 100 cigarettes in their lifetime and smoking within the past 30 days. Former smokers reported smoking > 100 cigarettes in their lifetime but denied smoking in the past 30 days. Never smokers reported smoking ≤100 cigarettes in their lifetime. Lifetime exposure was defined as pack years, calculated by multiplying years smoked by average number of packs smoked per day. Average cigarettes smoked per day were codified in the original dataset. To obtain an exposure amount, the median of ranges of packs per day used (e.g., 1–1.5 pack range became 1.25 packs). Duration of abstinence was calculated by subtracting reported age of quitting from baseline age. To determine the relationship between duration of abstinence and risk of dementia, while permitting interpretation of non-linear behavior over the abstinence time period, abstinence duration was categorized by decades of abstinence (i.e., abstinent for < 10 years, abstinent between 10 to < 20 years, abstinent between 20 to < 30 years, abstinent for ≥30 years).
Participants with normal cognition or cognitively impaired but not MCI at baseline were categorized as cognitively healthy (see the Supplementary Material for grouping rationale). Dementia diagnosis at follow-up was identified one of two ways: 1) via clinical evaluation at follow-up, or 2) if placed in a nursing home and CDR® Dementia Staging Instrument (CDR [26, 27]) global score ≥1. Follow-up contact occurred approximately annually. Nursing home placement (i.e., participant permanently moved to a nursing home) and death were reported by a designated informant at follow-up. Participants who were discontinued or lost to follow-up could not report these statuses. Age-at-event was determined by death date for death events, and follow-up visits date for incident dementia and nursing home placement events.
Additional baseline measures included patient-reported presence of recent/active diabetes or recent/active hypertension and Mini-Mental State Exam score (MMSE) [28]. Demographic variables included race, education, gender, and age at baseline (Table 1). “Unknown” responses of covariates were included as their own category for analyses.
Demographic information for participants by baseline smoking status
*p < 0.05, **p < 0.01, ***p < 0.001 for omnibus tests. MMSE, Mini-Mental State Examination [28].
Analyses
Chi-square tests of independence and Kruskal-Wallis tests were used to examine differences be-tween baseline smoking status (never, former, and current) in demographics, cardiovascular/cerebro-vascular risk, and MMSE at baseline. Multi-state models used Cox proportional hazards to estimate hazard ratios (HR) and 95%confidence intervals (CI) for smoking predictors and were setup to mimic an illness-death model [19] (Fig. 1C), where there are three states a subject can occupy (healthy, dementia, or death), and subjects can transition from healthy to dementia or healthy to death, and those who transitioned to dementia can then transition to death. Each transition used age as the time scale, with a delayed-entry setup to account for varying age of study entry and varying age of dementia diagnosis. In addition to the smoking predictor, each model and transition included baseline reported education, gender, recent/active hypertension, and recent/active diabetes as a priori covariates due to their known impact on dementia risk [7]. “Unknown” responses for main predictor variables were considered to be missing data and were excluded from analyses.
Multi-state time-to-event regression and diagnostics were performed using R 3.6.1, with mstate package for data formatting, and survival [30, 31] package for fitting. IBM SPSS Statistics V25 Premium was used for all other analyses. No major concerns for non-proportionality of covariates were found.
Model 1 examined the differences between never, former, and current smokers on age to dementia onset. Model 2 examined the role of lifetime smoking exposure in pack years (measured as a continuous variable) on age to dementia onset. Model 3 examined duration of abstinence among former and never smokers on age to dementia onset, using never smokers as the reference category.
Due to the three transitions in each model, and the smoking predictor being included as a covariate in each transition direction within a model, each model has multiple p-values associated with the smoking outcome (i.e., primary covariate). Benjamini-Hoch-berg correction to these p-values were performed, controlling false discovery rate (FDR) at 5%for the smoking-related covariates within each model [32, 33].
Sensitivity analyses
Pack-years was added as a covariate in Model 3 to determine if level of smoking exposure affected results. Due to collinearity between pack years and duration of abstinence (i.e., “never smokers” pack year value is always 0), the effect of pack years could only be estimated for the baseline to dementia transition. To ensure findings related to conversion from dementia to death were not solely due to the known impact of smoking on cardiovascular risk factors (e.g., stroke) [2], we descriptively examined duration of time in each state prior to transition and presence of stroke by smoking status.
RESULTS
Current smokers were younger, more likely to be African American, less educated, and had lower baseline MMSE scores than never and former smokers. Never smokers had lower rates of diabetes and hypertension and were more likely to be male than current smokers or former smokers (Table 1).
Smoking status
Current smokers were at increased risk for dementia, and conversion to death from both baseline and incident dementia, compared to never smokers (Model 1 in Table 2; Fig. 3). Former smokers were at decreased risk for dementia onset compared to never smokers but did not statistically differ from never smokers in terms of risk for death from either baseline or dementia diagnosis. Findings remained substantively unchanged after correcting for FDR.
Cox-regression proportional hazard models for Models 1, 2, and 3 for baseline cognitively healthy individuals
*p < 0.05, **p < 0.01, ***p < 0.001. Note. Covariates for adjusted models included gender, education, diabetes status, and hypertension status. Presented p-values are prior to adjusting for false discovery rates. †Findings from Model 3 remained substantively unchanged after adding smoking exposure (pack years) to the model as a sensitivity analysis. ‡Findings were no longer significant after adjusting for false discovery rates.
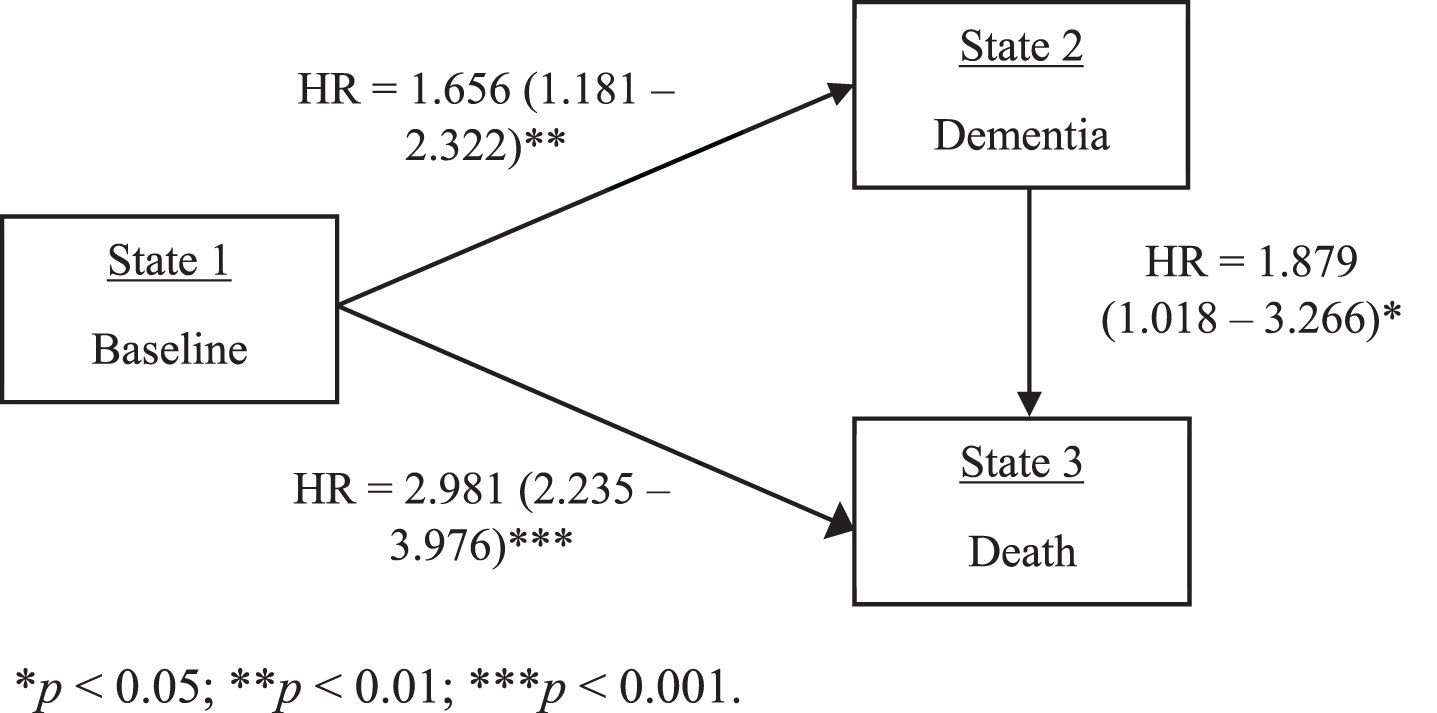
Multi-state hazard ratios, confidence intervals, and p-values for current smokers compared to never smokers.
Lifetime exposure
Results revealed no significant association of smoking exposure (in pack years) on incident dementia diagnosis. Greater lifetime cigarette exposure was related to increased risk of death from baseline, but not from dementia diagnosis (Model 2 in Table 2). Results remained substantively unchanged after correcting for FDR.
Abstinence duration
Former smokers with up to 30 years of abstinence did not show statistically significant differences in risk of dementia compared to never smokers (Model 3 in Table 2), although a linear trend for reduced risk over time was observed. Interestingly, former smokers with more than 30 years of abstinence were less likely to convert to dementia compared to never smokers. When converting from baseline to death, participants abstinent for < 10 years and between 20 to < 30 years were at increased risk of conversion, all other results were not statistically different from never smokers. The relation between smokers quit for 20 to < 30 years was no longer significant when controlling for FDR; all other results remained substantively unchanged. Former smokers did not significantly differ from never smokers in terms of risk of transition from incident dementia to death, regardless of abstinence duration.
Sensitivity analyses
Sensitivity analyses for abstinence duration, which controlled for pack years in addition to previously listed covariates, showed similar results to those corrected for FDR (Model 3 in Table 2). Sensitivity analyses examining the potential impact of stroke on findings looked at prevalence of stroke in current versus never smokers after baseline, and duration in each state prior to transition (i.e., time before transitioning to dementia following baseline assessment, death following baseline assessment, or death following dementia diagnosis). Participants who switched states spent approximately 4–5 years in cognitive status established at baseline (i.e., in a cognitively healthy status) prior to dementia diagnosis, 5-6 years in cognitive status established at baseline prior to death, and 2-3 years following dementia diagnosis before dying. Current smokers reported fewer strokes following baseline than never smokers (50.0%versus 56.3%).
DISCUSSION
This analysis is the first to comprehensively examine the role of cigarette smoking, a modifiable risk factor for ADRD, on the risk of death, dementia, or death following dementia. Moreover, this is the first study to include nursing home placement (if cognitive status was impaired as estimated by an elevated CDR [26] score), a likely proxy for ADRD diagnosis [21, 22]. Current smokers were 1.7 times more likely to convert to dementia, almost three times more likely to convert to death from baseline, and almost twice as likely to convert to death following a dementia diagnosis compared to never-smokers, supporting our first hypothesis.
These results are contrary to recently publicized work examining the competing risks of dementia and death in smoking [17] and suggest that examination of outcomes following dementia onset coupled with a more comprehensive assessment of dementia (i.e., dementia and/or nursing home placement with cognitive impairment) results in more robust impact of smoking status on ADRD-related outcomes. Notably, the NACC UDS includes data used in the aforementioned manuscript [17] as well as data collected from other ADCs. These results are consistent with existing literature demonstrating that cigarette smoking negatively impacts ADRD onset [6] as well as mortality [1, 2]. Sensitivity analyses also suggest that conversion to dementia was not solely due to cardiovascular events (i.e., stroke) for current or former smokers and remained irrespective of pack years smoked. Together, findings paint a picture that smoking not only results in death but can also lead to suffering through lost cognitive functioning and independence.
Former smokers were significantly less likely to convert from baseline to dementia than never smokers. This unexpected finding was inconsistent with our hypothesis. Findings from Model 3 coupled with the majority (56%) of former smoker reporting abstinence for ≥30 years highlight a potential cohort effect of those who quit long ago. A broader shift toward healthy lifestyle changes among former smokers may have contributed to decreased risk of dementia. Notably, this change in smoking behavior did not result in decreased risk of death (from baseline or following dementia) compared to never smokers.
Contrary to our hypothesis and research demonstrating a dose-response relationship between smoking and ADRD onset [23, 34–37], there was no association between lifetime smoking exposure and incident dementia onset. However, greater smoking exposure was associated with increased risk for death from baseline suggesting that the impact of lifetime smoking exposure is more related to death than other ADRD-associated outcomes (i.e., dementia onset or conversion from dementia to death) [17]. This is consistent with research highlighting the dose-response of cigarette smoking exposure on mortality [2, 38], and reinforces the critical impact of current smoking, rather than the cumulative impact of smoking, on ADRD onset.
We also explored whether there were any recency effects. Our hypothesis that, compared to never smokers, longer abstinence from smoking would be associated with lowered risk of ADRD was only partially supported by the data. Recent (< 10 years) and intermediate (10 to < 20 years) quitters showed no significant differences in risk for dementia compared to never smokers. However, we must be cautious in assuming that a lack of statistically significant difference infers equality; a larger sample size of recently quit smokers (< 10 years) may find a difference in terms of dementia risk. Given the trend of hazard ratio decreasing by time of abstinence (i.e., the longer someone has quit the lower their risk for incident dementia) coupled with the decreased standard errors for longer duration of abstinence, we can surmise that greater duration of abstinence is related to decreased risk of ADRD. Abstinence from smoking ≥30 years had significantly lower hazard-rates of developing dementia than never smokers, suggesting that early cessation is associated with improved health. This effect may be related to a larger sample size of those quit for 30 or more years, an overall change in health behaviors (e.g., greater health awareness), or a cohort effect; the underlying causes of this effect cannot be assessed in the current data.
In comparison, it took 10 years for former smokers to appear not statistically different to never smokers in terms of death risk. These findings suggest that smoking has a more robust relationship with death than with dementia onset, and consequently, the risk for dementia may be abated quicker (as the data from this study would support). Alternatively, smoking can cause a variety of negative health outcomes which may result in death, but smoking may impact fewer biological processes that influence cognitive functioning. A larger sample of recent quitters is needed to determine with more precision the duration of abstinence required for the risk of dementia to abate.
Certain study limitations exist. First, smoking data were self-reported during baseline interviews only due to only a portion of the sample having updated smoking status at follow-up. Baseline smoking status may have changed throughout the 14 years of data collection, which could have had considerable undetected impact on clinical outcomes. Future work would benefit from biochemical verification of smoking status at follow-up interviews. Reasons for smoking cessation were not collected and may have provided information on cessation motivation as it relates to cognition or other health conditions (e.g., individuals may have quit smoking because their cognition was declining or after suffering a significant health event like a stroke or heart attack). This study is subject to healthy survivor bias [39] in that all participants must have been healthy enough to survive to the age of entry in this study (45 years minimum; 72 years on average); smokers may not have not survived to this age due to health issues potentially biasing groups. Future research would benefit from larger samples of recent quitters to compare to never smokers, as well as longer duration of follow-up, preferably starting at a younger age and followed prospectively. This cohort was highly educated, and many individuals specifically wanted to be in the NACC UDS to advance science specific to dementia, limiting generalizability. Further, recruitment for inclusion in the NACC UDS is geared toward AD dementia, although recruitment methods differ by specific ADC and all ADCs recruit other forms of dementia (e.g., Lewy body dementia, frontotemporal dementia). While AD dementia is the leading type of dementia, accounting for 60 to 80%of current dementia diagnoses [7], future studies focused on all forms of dementia are warranted to ensure findings are replicated. Although this sample had significant racial diversity, increasing the generalizability of findings, there were significant differences in smoking status by race. Due to recent evidence suggesting an impact of race-based selection bias on subsequent conversion to dementia [40], which could influence results due to the known association between smoking and race [2], we did not use race as a covariate.
CONCLUSIONS
Among cognitively healthy individuals, current cigarette smoking at baseline was associated with an increased the risk of incident dementia, death, and death following dementia. Pack-years were not significantly associated with dementia risk but were significantly associated with increased risk of death following dementia. Lack of significant differences between never and former smokers (with < 30 years of abstinence) coupled with the trend of decreased risk by duration of abstinence suggests that risk of incident dementia is better attributed to recency, rather than overall exposure, of cigarette use. However, former smokers were only comparable to never smokers after 10 years of abstinence for the competing risk of death. These findings highlight the benefit of smoking cessation at any age for cognitively healthy individuals.
Footnotes
ACKNOWLEDGMENTS
Data were obtained from the National Alzheimer’s Coordinating Center Uniform Data Set. The NACC database is funded by NIA/NIH Grant U01 AG016976. NACC data are contributed by the NIA-funded ADCs: P30 AG019610 (PI Eric Reiman, MD), P30 AG013846 (PI Neil Kowall, MD), P30 AG062428-01 (PI James Leverenz, MD) P50 AG008702 (PI Scott Small, MD), P50 AG025688 (PI Allan Levey, MD, PhD), P50 AG047266 (PI Todd Golde, MD, PhD), P30 AG010133 (PI Andrew Saykin, PsyD), P50 AG005146 (PI Marilyn Albert, PhD), P30 AG062421-01 (PI Bradley Hyman, MD, PhD), P30 AG062422-01 (PI Ronald Petersen, MD, PhD), P50 AG005138 (PI Mary Sano, PhD), P30 AG008051 (PI Thomas Wisniewski, MD), P30 AG013854 (PI Robert Vassar, PhD), P30 AG008017 (PI Jeffrey Kaye, MD), P30 AG010161 (PI David Bennett, MD), P50 AG047366 (PI Victor Henderson, MD, MS), P30 AG010129 (PI Charles DeCarli, MD), P50 AG016573 (PI Frank LaFerla, PhD), P30 AG062429-01(PI James Brewer, MD, PhD), P50 AG023501 (PI Bruce Miller, MD), P30 AG035982 (PI Russell Swerdlow, MD), P30 AG028383 (PI Linda Van Eldik, PhD), P30 AG053760 (PI Henry Paulson, MD, PhD), P30 AG010124 (PI John Trojanowski, MD, PhD), P50 AG005133 (PI Oscar Lopez, MD), P50 AG005142 (PI Helena Chui, MD), P30 AG012300 (PI Roger Rosenberg, MD), P30 AG049638 (PI Suzanne Craft, PhD), P50 AG005136 (PI Thomas Grabowski, MD), P30 AG062715-01 (PI Sanjay Asthana, MD, FRCP), P50 AG005681 (PI John Morris, MD), P50 AG047270 (PI Stephen Strittmatter, MD, PhD). This work was supported by the Veterans Affairs Advanced Fellowship in Women’s Health (Johnson) and R01 AG054059 (Gleason, PI). The funding source had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. Content does not represent views of the US Department of Veterans Affairs or the US Government.