
Abstract
Background:
Physical exercise is suggested to be effective for preventing cognitive decline in older adults, but the relative efficacy of different types of exercise have yet to be clarified.
Objective:
This single-blinded randomized controlled trial was designed to investigate the differential effects of aerobic exercise training (AT), resistance exercise training (RT), and combined exercise training (CT) on cognition in older adults with subjective memory complaints (SMC).
Methods:
Community-dwelling older adults with SMC (n = 415; mean age = 72.3 years old) were randomly assigned to one of the four groups: AT, RT, CT, or control group. The study consisted of two phases: a 26-week intervention and a 26-week follow-up. The participants were evaluated at baseline, 26 weeks (postintervention), and 52 weeks (follow-up). The primary outcome of this study was memory function, which was assessed using the Logical Memory II subtest of the Wechsler Memory Scale-Revised (WMS-R) score. The secondary outcomes included global cognitive function, verbal fluency, working memory, processing speed, and executive functions.
Results:
Intention-to-treat analysis by a mixed-effect model repeated measure showed that the AT group had significantly improved performance on the WMS-R Logical Memory II test (2.74 [1.82–3.66] points) than the control group (1.36 [0.44–2.28] points) at the postintervention assessment (p = 0.037). The effect was more pronounced in those without amnesia than those with amnesia. No significant improvement was observed in the RT and CT groups.
Conclusion:
This study suggests that AT intervention can improve delayed memory in community-dwelling older adults, particularly in individuals without objective memory decline.
Keywords
INTRODUCTION
There has been considerable and steadily growing interest in slowing cognitive decline and delaying dementia onset through behavioral interventions [1, 2]. Physical activity and exercise have been suggested to be effective in preventing cognitive decline and may decrease dementia risk in older adults [3–7], improve neural plasticity [8], and promote quality of life [9]. Ngandu et al. showed that a multi-domain intervention including physical exercise could improve or maintain cognitive function among at-risk older adults in the community [10]. However, systematic reviews and meta-analyses of randomized controlled trials (RCTs) of physical exercise interventions have failed to provide clear evidence of benefits from exercise on cognitive function [11–13]; thus, further large scale and high-quality trials are needed to clarify the effects of physical exercise on cognitive function [12].
Although the previous RCTs which assessed the effects of multimodal exercise, including aerobic, resistance, balance, and stretching activities, have reported on cognitive improvement [14, 15], it is not clear what types of exercise is most effective, and whether combining multiple exercise types could provide larger benefits on cognition. The World Health Organization recommends aerobic physical activity, muscle strengthening activity, or multicomponent physical activity for health outcomes, such as mortality, cardiovascular disease, type-2 diabetes, cancer incidence, adiposity, mental health, and cognitive outcomes in older adult populations [16]. The American College of Sports Medicine recommends a combination of aerobic exercise training (AT) and resistance exercise training (RT) for older adults, as it is more effective than either form of training alone on physical functioning and overall health [17]; however, it does not refer to the effects of exercise on cognitive function. Among the RCTs which were targeted to improve cognitive function, AT or RT have been the main exercise interventions and each has been associated with cognitive improvement [18–21]. Few studies have compared the impacts of different exercise modalities as well as their combined effect. Although one RCT has compared the efficacy of AT versus RT on cognitive function [22], the sample size was small and the efficacy of a combination of AT and RT was not evaluated. An animal study suggested that AT and RT improved cognitive functions through divergent molecular mechanisms and distinct signaling pathways [23]. Thus, the effects of different exercise modalities on human cognitive function need to be better evaluated [24].
In addition, identifying targets for preventing cognitive decline is a crucial issue, while it is expected to be more effective to start interventions in preclinical or prodromal Alzheimer’s disease (AD) [25]. According to the Cochrane reviews, one review showed that aerobic exercise improves cognitive performance among cognitively healthy individuals [26], whereas another review has revealed no clear evidence of benefit from exercise on cognitive function among older people with dementia [13]. The effectiveness of physical exercise on cognitive function may be different at each clinical stage of dementia. A conceptual framework of subjective cognitive decline (SCD) has been proposed to define the population for targeted dementia prevention trials [27]. SCD, a self-perceived decline of cognitive function without objective deficits on neuropsychological tests, is the preclinical stages of AD, with a high risk of AD and amnestic mild cognitive impairment (MCI) due to AD [28]. The benefits from exercise on cognitive function may be different between those with and without objective cognitive decline in memory [27] and is expected to be more effective in those without amnesia (i.e., SCD) than those with amnesia (i.e., MCI) [29]. SMC (subjective memory complaints; also termed subjective cognitive complaints) is defined as everyday-memory and related cognitive concerns, which may be expressed by people who may or may not have deficits on objective testing [30]. This has been proposed as the first subtle sign of cognitive impairment before the appearance of AD or MCI and even before actual objective cognitive decline [27, 31]. Indeed, latest RCT of on-line multidomain lifestyle intervention targeted older adults with SMC [32].
The main purpose of this study was to evaluate similarities and differences among the effects of AT, RT, and combined exercise training (CT) on cognitive function in community-dwelling older adults with SMC. We hypothesized that CT would be more effective on cognitive performance than AT or RT because CT was reportedly more effective on physical functioning or global health than a single exercise modality [17]. Our secondary objective was to examine the differences of the effects of AT, RT, and CT on cognitive function according to the amnesia status. We hypothesized that the effect would be more pronounced in the non-amnesia group than in the amnesia group.
METHODS
Study design
A single-blinded RCT named “TOyota Prevention Intervention for Cognitive decline and Sarcopenia” (TOPICS) was designed to evaluate the effects of AT, RT, and CT on cognitive function, physical function, and physical activity in community-dwelling older adults with SMC. Assessors were blinded to group membership, whereas participants were not. It was not possible to blind the participants to group membership, owing to the easily discernible nature of the exercise modalities required of each group. Participants were randomly assigned, using allocation concealment, to one of the four groups: the AT, RT, CT, or control group with an allocation ratio of 1:1:1:1. The study consisted of two phases: a 26-week intervention and a 26-week follow-up. The participants were evaluated at baseline before randomization, 26 weeks (postintervention), and 52 weeks (follow-up). The ethics committee of the Graduate School of Medicine, Nagoya University approved the study protocol (approval no. 2014-0155-2), and the study was registered with the University Hospital Medical Information Network (UMIN) clinical trials registry (registration no. UMIN000014437, URL: https://upload.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000016788). All participants provided written informed consent before their inclusion in the study. The recruitment of participants began in October 2014.
Sample size
The calculation of sample size was derived from a meta-analysis of studies on the effects of physical training on cognition in healthy older adults [3]. Because the average effect size in this meta-analysis was defined as Cohen’s d = 0.33, an effect size of f = 0.15 (small-to-medium) was assumed to be clinically relevant for the interaction of group*time in the repeated-measurements analysis of variance with four groups and three time-points of measurement. The power analysis of G*Power [33] found that a sample size of 328 was sufficient to demonstrate this effect (type I error rate of 0.05 [two-tailed] and 80%power). Allowing for 20%attrition owing to withdrawal and illness, commonly found in other intervention studies with healthy older adults [34], the recruitment of 103 participants per group for a total of 412 older adults was aimed.
Participants
The workflow detailing participant recruitment and criteria is shown in Fig. 1. Toyota, where this research was conducted, is a city located in north-central Aichi Prefecture, central Japan. The aging rate in Toyota city was 20.7%in 2015. As the first step, older adults at high risk for future decline in instrumental activities of daily living (IADL), were screened using the “Kihon Checklist” questionnaire, which was sent by the Toyota City municipal government to citizens aged≥65 years in selected areas, based on comprehensive resident registration records. The questionnaire comprises of 25 self-reported items [35], including the following three items concerning subjective cognitive problems: “Q18. Do your family or friends point out your memory loss?” (e.g., “You ask the same question over and over again.)”; “Q19. Do you make a call by looking up phone numbers?”; and “Q20. Do you find yourself not knowing today’s date?” Individuals who answer yes to Q18 or Q20, or who answer no to Q19 are regarded to be at high-risk of cognitive decline [36]. A previous study showed that at least one or more negative responses in these three questions could effectively screen for older adults with potential decline in IADL and at risk of cognitive decline [37]. Thus, respondents of “Kihon Checklist” having at least one or more negative responses in those three questions were defined to have SMC in this study.
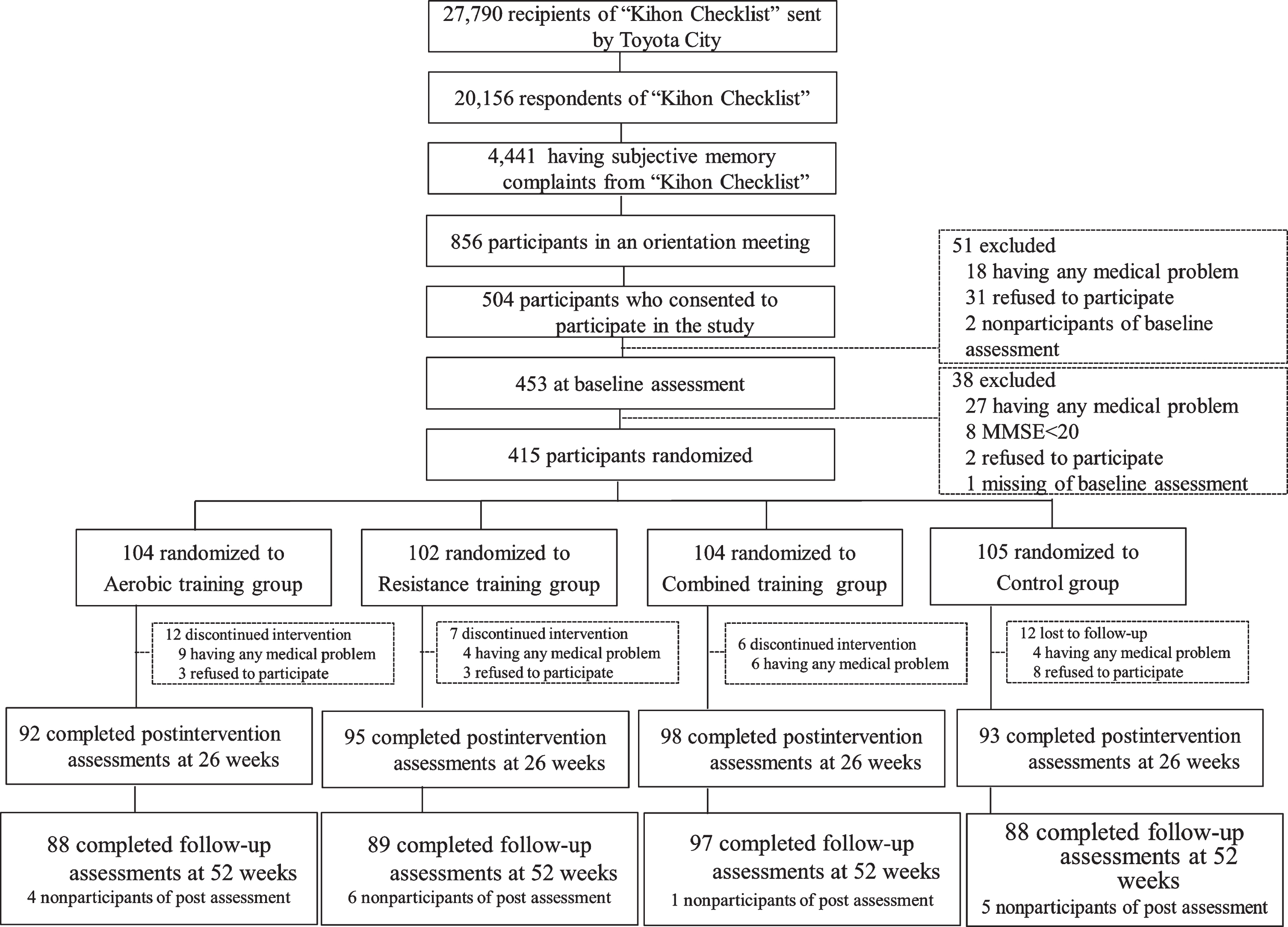
Workflow detailing participant recruitment and criteria.
The Toyota City municipal government screened participants who provided at least one or more negative responses to questions 18–20, and generated a list of names and addresses that were provided to Nagoya University. Invitations to the study orientation meeting to residents who were younger than 85 years old were sent using the provided list. Participants who attended the meeting but met the following criteria were excluded: 1) required support or care from the Japanese public long-term care insurance system; 2) had significant cognitive function impairment (i.e., Mini-Mental State Examination (MMSE) [38] score≤19); 3) met clinical criteria for dementia according to the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition [39]; 4) had a severe visual impairment; 5) met clinical criteria for a psychiatric disorders (i.e., psychosis, major depression); 6) any disability with the basic or IADL; 7) had a neurodegenerative disease (i.e., Parkinson’s disease); 8) medical contraindications to exercise; or 9) history of serious cardiovascular, musculoskeletal, respiratory, or cerebrovascular disease or other severe health issue. Criteria 6 to 9 above were based on self-reports and 2 to 5 on assessment by medical professionals. At baseline, we collected demographic information (i.e., age, sex, education) and information about currently prescribed medications. Additionally, blood samples were obtained, and the apolipoprotein E (APOE) phenotypes were determined using a turbidimetric immunoassay with a commercial kit (Apo E auto N series [Daiichi]; Sekisui Medical Co. Ltd, Tokyo, Japan).
Randomization
After completion of the baseline assessment, participants were randomly assigned to one of the four groups using a minimization algorithm [40]. The randomization factors were the age (≥75 versus < 75 years old), sex, years of education (≥10 versus < 10 years of education), presence or absence of amnesia, and MMSE scores (≥24 versus 20–23). We ensured equal distribution of these relevant factors in each group. Amnesia status was defined according to the Alzheimer’s Disease Neuroimaging Initiative criteria [41]. The allocation list was provided by an independent statistician not involved in the intervention or assessment of the participants or data collection.
Intervention
Participants in the AT, RT, and CT groups exercised under the supervision of well-trained fitness instructors for 60 min/day, two days/week, for a total of 52 sessions over the first 26 weeks. The training intensity of the exercises in this study was regulated using ratings of perceived exertion (RPE). The target RPE was a rating of “Easy” (i.e., a rating of “11”) for weeks 1–2, “Somewhat hard” (i.e., a rating of “13”) for weeks 3–12, and “Hard” (i.e., a rating of “15”) for the remainder of the program. The classes consisted of three parts: 10 min warm-up, 40 min of core training activities, and 10 min cool down. Attendance was recorded at each session, and this value was used to calculate adherence. The intervention was conducted at local gyms which are public facilities in Toyota City. Participants were required to visit the gym by themselves (no transportation was provided by those who conducted the study).
Aerobic exercise training protocols
This program comprised 40 min of core content including 10–15 min of step-in-place exercises, 10–15 min of a walking program, and intervals for rest and monitoring heart rate. In reference to RPE, we regulated the intensity using the targeted heart rate. To achieve the target heart rate, exercise intensity was increased after each monitoring interval until the target heart rate reserve (HRR) was achieved. HRR was calculated using the Karvonen method [42]. The target heart rate zone was 40%HRR for weeks 1–2, 50%HRR for weeks 3–8, 60%HRR for weeks 9–12, and 70%HRR for the remainder of the program, regardless of the participants’ demographic characteristics, medication, physical functions at the baseline, and prior levels of exercise experience. Resting heart rates at the baseline were measured with an automated blood pressure sphygmomanometer, and heart rates before, during, and after workouts were measured using wearable devices. Aside from the structured program in class, outdoor walking was recommended to the AT group. The participants in the AT group were asked to keep a notebook where they recorded the amount of time spent walking, their heart rate before and after exercise, and their daily total steps according to a pedometer.
Resistance exercise training protocols
This program involved elastic resistance training and bodyweight exercises. Two types of elastic tubes, each with a different stiffness, were given to each participant. Participants were asked to advance their effort in a manner consistent with the progression identified above by changing the grip width or rubber stiffness of the elastic tubes to achieve a greater resistance. Elastic resistance training consisted of bicep curls, chest presses, side raises, seated rowing, leg presses, hip abduction, and side bends. Body weight exercises consisted of shrugs, knee ups, trunk curls, squats, kneeling kickbacks, toe raises, and calf raises. Two sets of each exercise were performed with 10 repetitions each. Aside from the structured program in class, home-based exercise was recommended to the RT group. The participants in the RT group were asked to keep a notebook where they recorded the amount of time spent on home-based exercise, the number of times they completed the training sessions, and the RPE.
Combined exercise training protocols
This program combined the AT and RT programs. The progression of exercise intensity was the same as that in the AT and RT program, while the amount of time spent on each type of training was halved. For aerobic training, step-in-place exercises or the walking program alternated between each class. For resistance training, each exercise was performed for one set. RT programs were performed before AT programs at each session. Aside from the structured program in class, both outdoor walking and home-based exercises were recommended to those in the CT group.
Control
Participants in this group were asked to attend educational classes 2 times during the 26-week intervention period. The classes provided information about health promotion regarding aging, healthy diet, and prevention of cerebrovascular disease. These classes did not provide specific instructions regarding exercise, physical activity, or cognitive health.
Measurements
Primary outcome
A neuropsychological test battery was performed by well-trained clinical psychologists, speech therapists, and occupational therapists to examine the cognitive function of the participants. The primary outcome was memory function changes, because memory impairment confirmed by neuropsychological testing is the most common syndromic presentation of AD [43]. The Logical Memory II subtest of the Wechsler Memory Scale-Revised (WMS-R) score [44] was chosen as the primary outcome because of its known sensitivity to predicting the risk of converting to dementia [45].
Secondary outcomes
The secondary outcomes include the following measures of cognitive function: the MMSE for global cognition; the Logical Memory I and Visual Reproduction I subtest of the WMS-R for immediate memory; the Visual Reproduction II subtest of the WMS-R for delayed memory; the Digit Span Forward and Visual Memory Span Forward subtest of the WMS-R for memory span; the Digit Span Backward and Visual Memory Span Backward subtest of the WMS-R for working memory; the Category Fluency (animal naming) Test and Letter Fluency Test for verbal fluency; the Digit Symbol subtest of the Wechsler Adult Intelligence Scale-III (WAIS-III) [46], the Stroop Test [47] Color and Trail Making Test [48] part A for processing speed; and the Stroop Test Colored Word and Trail Making Test part B for executive function.
Exploratory outcomes
Physical function. As exploratory outcomes, muscle strength, gait speed, exercise capacity, balance ability, and basic mobility skill were measured. Muscle strength was assessed using grip strength for the upper extremities and timed chair stands [49] for the lower extremities. A portable grip strength dynamometer (GRIP-D; Takei Ltd., Niigata, Japan) was used to measure dominant hand grip strength. Gait speed was assessed in different conditions, normal walking, in which participants were asked to walk at their preferred speed; and maximal walking, in which participants were asked to walk at their maximal speed. Exercise capacity was assessed using the 6 min walking test [50]. Participants were instructed to walk as far as possible in a 6 min period along a 10-meter course. Balance ability was assessed by the one-legged standing test, and basic mobility skill was assessed by the timed Up & Go test [51].
Physical activity. Participants were asked to wear a uniaxial accelerometer (Kenz Lifecorder; Suzuken Co., Ltd., Nagoya, Aichi, Japan) to obtain daily physical activity data. Participants were required to attach the device to their waist while they are awake for 14 consecutive days and were blinded to their counts. The monitors counted steps (steps/day) and recorded the amount of time spent at specific activity intensities (the device records a signal of 0, 0.5, 1–9 every 4 seconds while worn). Based on the Kumahara’s criteria [52], the intensities were defined as follows: 1 to 3 as light (< 3 metabolic equivalents [METS]), 4 to 6 as moderate (3–6 METS), and 7 to 9 as vigorous (> 6 METS) intensity of physical activity.
Statistical analyses
Baseline characteristics were compared among the four groups (three treatment groups and one control group) using chi-square statistics for categorical variables and one-way analysis of variance (ANOVA) with Bonferroni-adjusted pairwise comparison for continuous variables. The primary analysis of effect on the cognitive functions, physical functions, and physical activity were based on intention-to-treat (ITT) analysis by a Mixed-effect Model Repeated Measure (MMRM), with group allocation and time as fixed effect, and the subject as a random effect, using the data collected at three time points (baseline, postintervention, and follow-up).
For stratified analysis, according to the amnesia status, the ITT cohort was divided into two groups: amnesia and non-amnesia. Baseline characteristics of cognitive functions were compared between the two groups (amnesia and non-amnesia) using chi-square statistics for categorical variables and Student’s t-test for continuous variables. Outcomes within the two groups (amnesia and non-amnesia) were compared among the four groups (three treatment groups and one control group) using chi-square statistics for categorical variables and ANOVA with Bonferroni-adjusted pairwise comparison for continuous variables, respectively. Differences in those outcome measures in amnesia stratified patients were compared using MMRM.
All analyses were performed using SAS Version 9.4 for Windows (SAS Institute, Inc., Cary, NC) and IBM SPSS statistics for Windows version 24.0 (IBM Corp. Armonk, NY). We used a type I error rate of p < 0.05 (two-tailed) to indicate statistical significance for the efficacy of the outcomes.
RESULTS
A total of 415 participants who did not meet our exclusion criteria were randomly assigned to one of the four groups: n = 104 in the AT group, n = 102 in the RT group, n = 104 in the CT group, and n = 105 in the control group. Overall, 378 (91%) participants completed assessments at the postintervention stage and 362 (87%) at the follow-up. Figure 1 shows the detailed workflow. Average adherence to the exercise training programs was 82.5, 85.9, and 83.5%for the AT, RT, and CT groups, respectively.
Baseline demographics and characteristics of the participants are shown in Table 1. The mean age and education as well as proportion of women, presence of amnesia, and presence of the APOE ɛ4 allele of the four groups were not significantly different. The baseline means for the neuropsychological and physical function tests, and the daily physical activity data of the four groups also did not differ significantly.
Baseline characteristics of the participant groups
AT, Aerobic exercise Training; RT, Resistance exercise Training; CT, Combined exercise Training; SD, Standard Deviation; MMSE, Mini-Mental State Examination; WMS-R, Wechsler Memory Scale-Revised; WAIS-III, Wechsler Adult Intelligence Scale-III.
Tables 2 3 show the change in outcomes from baseline in the ITT cohorts. A significant beneficial effect of the intervention for cognitive functions, physical functions, and physical activity with reference to the control group was observed for several parameters. For the cognitive functions at the postintervention, compared to the control group, only the AT group had significantly improved performance in the WMS-R Logical Memory II test (p = 0.037). At follow-up, no significant beneficial effects of the intervention on cognitive functions were observed. For the physical functions at the postintervention, compared to the control group, the AT and CT groups had significantly improved performance in the timed chair stands (p = 0.006 and 0.001, respectively), normal walking (p = 0.001 and 0.014, respectively), maximal walking (p = 0.001 and 0.009, respectively), 6 min walking test (p < 0.0001 and p = 0.002, respectively), and timed Up & Go test (p < 0.0001 and p = 0.001, respectively). The AT group also had significantly improved step numbers (p = 0.004) and moderate intensity activity time (p = 0.003) compared to the control group. The RT group had significantly improved performance in the grip strength (p = 0.011), timed chair stands (p = 0.001), maximal walking (p = 0.002), and timed Up & Go test (p = 0.0004), though no significant differences in physical activity were observed. At the follow-up, compared with the control group, the AT group had significantly improved performance in the timed chair stands (p = 0.004), 6 min walking test (p = 0.016), and timed Up & Go test (p = 0.005), and the RT group had significantly improved performance on the timed chair stands (p < 0.0001), maximal walking (p = 0.0001), and timed Up & Go test (p = 0.011), while the CT group had significantly improved performance in the timed chair stands (p = 0.0002), and timed Up & Go test (p = 0.030). The RT group also significantly improved on the light intensity activity time (p = 0.022) compared with the control group.
Changes at the postintervention from baseline in the intention-to-treat cohorts
AT, Aerobic exercise Training; RT, Resistance exercise Training; CT, Combined exercise Training; CI, Confidence Interval; MMSE, Mini-Mental State Examination; WMS-R, Wechsler Memory Scale-Revised; WAIS-III, Wechsler Adult Intelligence Scale-III. Note: * in bold, p < 0.05; significant beneficial effect of the intervention by reference to the control group were analyzed by mixed-effect model repeated measure.
Changes at the follow-up from baseline in the intention-to-treat cohorts
AT, Aerobic exercise Training; RT, Resistance exercise Training; CT, Combined exercise Training; CI, Confidence Interval; MMSE, Mini-Mental State Examination; WMS-R, Wechsler Memory Scale-Revised; WAIS-III, Wechsler Adult Intelligence Scale-III. Note: * in bold, p < 0.05; significant beneficial effect of the intervention by reference to the control group were analyzed by mixed-effect model repeated measure.
Secondly, subgroup analysis stratified by the amnesia status was performed. Baseline demographics and characteristics of cognitive functions of the participants groups stratified by the amnesia status are shown in Table 4. Compared with the non-amnesia group, the amnesia group’s mean age and education were significantly high (p = 0.040 and 0.029, respectively), whereas the proportion of women was significantly lower (p < 0.0001). The presence of the APOE ɛ4 allele was not significantly different across groups. The performance of the MMSE (p = 0.001), WMS-R Logical Memory I (p < 0.0001) & II (p < 0.0001), WMS-R Visual Reproduction I (p < 0.0001) & II (p < 0.0001), WMS-R Digit Span Backward (p = 0.007), Category Fluency Test (p < 0.0001), Letter Fluency Test (p = 0.005), WAIS-III Digit Symbol (p = 0.002), Stroop Test Color (p = 0.012) & Colored Word (p = 0.002), and Trail Making Test part A (p = 0.007) & B (p < 0.0001) were also significantly lower. In both groups, the mean age and education as well as the proportion of women and presence of APOE ɛ4 allele across the four groups were not significantly different. A significant difference was observed for only the WMS-R Digit Span Forward test in the amnesia group in terms of baseline cognitive function (p = 0.037).
Baseline characteristics of cognitive functions of the participant groups by the amnesia status
AT, Aerobic exercise Training; RT, Resistance exercise Training; CT, Combined exercise Training; SD, Standard Deviation; MMSE, Mini-Mental State Examination; WMS-R, Wechsler Memory Scale-Revised; WAIS-III, Wechsler Adult Intelligence Scale-III. Note: In bold, significant differences among the 4 groups. *p < 0.05; significant differences between amnesia group and non-amnesia group.
Tables 5 6 show the changes in cognitive functions from baseline in the ITT cohorts according to the amnesia status. In the amnesia group, no significant beneficial effect of the intervention was observed at both the postintervention and the follow-up assessments. In the non-amnesia group, the AT group had significantly improved performance in the WMS-R Logical Memory I & II (p = 0.048 and 0.002, respectively), and the CT group significantly improved performance on the WMS-R Logical Memory I test (p = 0.034) compared to the control at postintervention. However, no significant differences were observed across all groups at follow up.
Cognitive functions changes at the postintervention from baseline by the amnesia status
AT, Aerobic exercise Training; RT, Resistance exercise Training; CT, Combined exercise Training; CI, Confidence Interval; MMSE, Mini-Mental State Examination; WMS-R, Wechsler Memory Scale-Revised; WAIS-III, Wechsler Adult Intelligence Scale-III. Note: * in bold, p < 0.05; significant beneficial effect of the intervention by reference to the control group were analyzed by mixed-effect model repeated measure.
Cognitive functions changes at the follow-up from baseline by the amnesia status
AT, Aerobic exercise Training; RT, Resistance exercise Training; CT, Combined exercise Training; CI, Confidence Interval; MMSE, Mini-Mental State Examination; WMS-R, Wechsler Memory Scale-Revised; WAIS-III, Wechsler Adult Intelligence Scale-III. Note: * in bold, p < 0.05; significant beneficial effect of the intervention by reference to the control group were analyzed by mixed-effect model repeated measure.
DISCUSSION
The TOPICS trial was designed as a proof-of-concept RCT to evaluate the effects of various exercise modalities including AT, RT, and CT on cognitive function, using a relatively large sample recruited from at-risk community-dwelling older adults in Japan. The dropout rate was low, and adherence to interventions was relatively high. We hypothesized that CT would be more effective on cognitive performance than AT or RT because CT was reportedly more effective on physical functioning or global health than a single exercise modality [17]. Further, we also hypothesized that the effect of training would be more pronounced in the non-amnesia group than in the amnesia group.
However, the AT, and not RT or CT, showed short-term beneficial effects on the primary outcome. Participants in the AT group showed a significant improvement in delayed memory function (i.e., in WMS-R Logical Memory II) compared to those in the control group at postintervention assessment. Further, all three treatment groups showed improvement in muscle strength, gait speed, and basic mobility skill at postintervention assessment. However, improvements in physical activity (average daily step number and moderate intensity activity time) were observed only in the AT group. These results suggest that any improvement in physical activity but not in physical functions might be beneficial for memory improvement. A previous cross-sectional study showed that moderate to vigorous physical activity, rather than light physical activity, was associated with better performance in memory and executive function [53], which partially agrees with our results. We expected the CT group to perform better than the other groups, because the CT was reportedly more effective on physical functioning or global health than a single exercise modality [17]. In the current study the total amount of time spent on exercise was equal for the three treatment groups, which gave the CT group less time for each training session than for the single modality exercise groups of the AT and RT interventions. This could have led to the reduced effect of CT in the current study. Some systematic reviews and meta-analyses of RCTs on aerobic exercise interventions have reported that either there is no evidence supporting that exercise improves cognitive function [54, 55] or that there are limited benefits to specific cognitive domains [26]. Jonasson et al. showed that aerobic exercise had the potential to improve cognition in a broad sense, and that the change was positively associated with the change in thickness of dorsolateral prefrontal cortex [56]. Further, ten Brinke et al. showed aerobic training significantly increased hippocampal volume [57]. Erickson et al. also showed that aerobic exercise training increased the hippocampal volume and that a change in size of the hippocampus was associated with increased serum levels of brain-derived neurotrophic factor and improved memory [18]. These results support our results anatomically and physiologically.
Our results did not show any improvements in secondary outcome variables. The WMS-R Visual Reproduction II in delayed memory scales did not have beneficial intervention effects. It is not clear why only verbal learning and memory of stories (i.e., WMS-R Logical Memory II), and not visual learning and memory of designs (i.e., WMS-R Visual Reproduction II) had beneficial effects. Umfleet et al. showed that both the WMS-R Logical Memory II and WMS-R Visual Reproduction II performances were significantly correlated with hippocampal volumes, while only WMS-R Visual Reproduction II was also correlated with volumes of temporal lobe, amygdala, and lateral ventricle [58]. These two scales in delayed memory were correlated differently with regional brain volumes, which might be relevant to our results. Although some systematic reviews and meta-analyses of RCTs on exercise interventions showed improvement in executive function [59, 60], our results did not show significant improvement. The baseline data with regard to executive functions in this study showed well-preserved performance that indicated very small cognitive decline. Ceiling effects might have influenced the result.
The results of the present study are inconsistent with a previous RCT, including older adults with MCI, which directly compared the efficacy of AT versus RT on cognitive function [61]. The study showed that both intervention groups had no improvement in delayed memory performance, though the AT group remembered significantly more items in the loss after the interference condition of the Rey Auditory Verbal Learning Test. These discrepancies in results may have been due to differences in the clinical stages of cognition. We expected that the effect of intervention was more pronounced in the non-amnesia group than in the amnesia group. Indeed, the results of the subgroup analysis according to amnesia status showed that only the non-amnesia group had beneficial effects of AT on memory function. These results suggested that the AT may be beneficial for older adults with SMC despite unimpaired performance on cognitive tests, as in SCD [27]; however, the AT may not be beneficial for older adults with objective memory decline as in MCI.
No significant improvements in primary and secondly outcomes were detectable for any group at follow-up. Specifically, the performance in the WMS-R Logical Memory II test at follow-up was better than at baseline and postintervention in the three treatment groups and even in the control group. Practice or placebo effects might have influenced this result. As in a previous study [10], practice effects of repeated cognitive testing might occur in both the intervention and control groups. It is hard to conclude that there was no effect by exercises based only on these results.
One of the strengths of this trial was that our data collection comprised a wide range of physical functions, body compositions, and physical activity, which could act as mediators for the association between exercise and cognitive functions. Aging is accompanied not only by cognitive decline, but also by changes in physical function and body composition. Some studies have demonstrated a correlation of sarcopenia [62] with cognitive decline [63] and brain atrophy [64]. Burns et al. suggested that some aspects of the pathophysiology of sarcopenia and Alzheimer’s disease may be shared, such as systemic anabolic and inflammatory abnormalities [64]. We aim to clarify the impact of physical exercise modalities on cognitive functions through future analyses.
The present study has several limitations. First, the possibility of practice or placebo effects on cognitive function cannot be excluded. In addition, there was also a possibility that the improvement observed in the exercise group resulted from social contact across the training groups. It may be impossible to completely exclude this factor in the study design. Second, no examinations were conducted during the follow-up period. Although the participants were instructed to perform daily activities as usual during the follow-up period, the interventions might have affected their usual lifestyle. The influence of interventions on behavioral changes needs to be addressed in future studies. Third, there is also a possibility that the type of transportation used by the participants might have affected the results. Toyota city, as the home town of Toyota Motor Corporation does not have a sufficient railway system, which suggests that private cars could be a dispensable transportation [65]. Although information about the type of transportation used by the participants were not collected, the influence of type of transportation to the gym or distance from home to the gym needs to be analyzed.
In conclusion, the current study suggests that the AT intervention can improve delayed memory function in older adults, particularly in individuals without objective memory decline. The findings of the current study could be applied to the development of evidence-based guidelines for educating and training the public, health professionals, and policy makers for the dementia risk reduction as encouraged by the recent consensus paper by the International Research Network on Dementia Prevention [66].
Footnotes
ACKNOWLEDGMENTS
This work was supported by JST COI Grant Number JPMJCE1317 and the Toyota Motor Corporation. The Toyota Motor Corporation was the funding source and was not involved in any of the stages of the study conduct and analysis. We would like to thank the participants of the TOPICS study and acknowledge the Toyota City Office for assistance with participant recruitment, assessment, and intervention.