
Abstract
Background:
Exosomes are nano-sized extracellular vesicles which are secreted by cells and usually found in body fluids. Previous research has shown that exosomal secretion and autophagy-lysosomal pathway synergistically participates in intracellular abnormal protein elimination. The main pathological manifestations of Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is abnormal accumulation of mutant NOTCH3, and CADASIL vascular smooth muscle cells have been found with autophagy-lysosomal dysfunction. However, whether plasma exosomes change in CADASIL patients is still unclear.
Objective:
We are aimed to investigate the differences of plasma exosomes between CADASIL patients and healthy controls.
Methods:
The subjects included 30 CADASIL patients and 30 healthy controls without NOTCH3 mutation. The severity of white matter lesions (WMLs) of CADASIL patients was quantified by Fazekas score. Transmission electron microscopy and nanoparticle tracking analysis were performed to characterize plasma exosomes. In addition, NOTCH3, Neurofilament light and Aβ42 levels in plasma exosomes were quantified by enzyme-linked immunosorbent assays.
Results:
We found that exosomes from CADASIL patients were lower in quantity. In addition, CADASIL plasma exosomes had significantly lower levels of NOTCH3 and significantly increased levels of NFL than those of matched healthy subjects. Interestingly, plasma exosome NOTCH3 levels of CADASIL patients significantly correlated with severity of WMLs.
Conclusion:
The exosome NOTCH3 may be related to the pathological changes of CADASIL, which provides a basis for the pathogenesis research of CADASIL. In addition, plasma exosome NOTCH3 and NFL levels may act as biomarkers to monitor and predict disease progression and measure therapeutic effectiveness in the future clinical trials.
Keywords
INTRODUCTION
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is the most common hereditary cerebral small vessel disease (CSVD) and is the main contributor for adult stroke and dementia [1, 2]. CADASIL is a progressive and devastating disease, with the main clinical manifestations of young or middle age-onset, migraine with aura, recurrent stroke, mood disturbances, cognitive impairment, or even dementia [2, 3]. Although previous studies have shown that CADASIL is rarely observed in the general population (0.002%–0.005%) [4], the actual prevalence could be much higher due to underdiagnosis and milder cases [5, 6].
CADASIL is caused by NOTCH3 gene mutation, and NOTCH3 is mainly expressed in adult vascular smooth muscle cells (VSMCs), which encodes a transmembrane receptor involved in important cell signaling and cell differentiation [7, 8]. The main pathological changes of CADASIL include degeneration of VSMCs, NOTCH3 protein accumulation and granular osmiophilic material (GOM) deposition near VSMCs in small-medium arteries, which main component is NOTCH3 receptor extracellular domain [9–11]. Currently, the diagnostic gold standard of CADASIL is genetic testing and/or pathological biopsy [12]. However, the molecular mechanism of NOTCH3 mutation causing VSMCs degeneration is unclear.
Exosome has recently attracted widespread attention. Exosomes are bioactive extracellular vesicle (EVs) with a diameter of 30–150 nm [13] and secreted by various cell types, such as reticulocytes, antigen presenting cells, neurons, and VSMCs [14, 15]. In addition, exosomes could be isolated from diverse bodily fluids, including blood, urine, saliva, amniotic fluid, and cerebrospinal fluid (CSF) [16, 17]. Originally, the function of exosomes was thought to remove unwanted proteins from the body. Recently, amounting studies have demonstrated exosomes play a vital role in intercellular communication under physiological and pathological settings [18]. Therefore, exosome components (nucleic acids, lipids, and proteins) may change under some pathological conditions.
Exosomes are endosome-derived nanovesicles. Briefly, the plasma membrane changes shape to allow the ingestion and internalization of materials, resulting in the formation of an intracellular vesicle. Then intracellular vesicles fuse with early endosomes, after the process of endosomal sorting and endosomal transport, and gradually mature and subsequently fuse to form the late endosomes/multivesicular bodies (MVBs) [19]. Then, the limiting membrane of MVBs buds inward to form intraluminal vesicles [20]. Eventually, part of MVBS fuse with lysosomes to degrade its contents while others fusion with plasma membrane of the cell leads to the release of exosomes to the extracellular environment [19].
Autophagy is a lysosome-dependent intracellular degradative pathway, which mediates the clearance of aggregated proteins and dysfunctional organelles [21]. Interestingly, previous research has shown exosomal secretion and autophagy–lysosomal pathways may synergistically participate in intracellular abnormal protein elimination [22]. Furthermore, in vitro and in vivo studies both indicate that compromised cargo turnover within lysosomes and altered trafficking through the endosomal pathway could affect the production, secretion, and content of exosomes [23]. Moreover, Xia et al. has also found that autophagy not only affects the secretion of exosomes, but also affects the α-syn content of exosomes in the pathogenesis of Parkinson’s disease [22]. Those above suggest that exosomes may play a role in maintaining flux through the endosomal-autophagy-lysosomal system.
More importantly, Hanemaaijer et al. have suggested that the mutant NOTCH3 aggregation and accumulation is associated with autophagy-lyso-somal dysfunction in CADASIL VSMCs [24]. Nevertheless, whether the exosomes have changed in CADASIL patients is still unclear. The aim of this study is to examine the differences of plasma exosomes between CADASIL patients and healthy controls.
Neurofilament light (NFL) is a cytoskeletal protein and abundantly present in neurons with large axons. Previous study had found that the level of CSF-NFL is increased of CADASIL patients. The amyloid-β 42 (Aβ42) was generated from the amyloid-β protein precursor via the sequential proteolytic cleavage. Other research found that the level of CSF-Aβ42 is decreased in CADASIL patients. But it is difficult to widely detect the level of NFL and Aβ42 in the CSF because of the invasive nature of lumbar puncture. Fortunately, exosomes can pass the blood-brain barrier and respond precisely to changes in the CSF. In addition, several studies have shown that the level of Aβ42 in plasma exosomes is consistent with the level of Aβ42 in CSF. However, whether the level of NFL and Aβ42 in the plasma exosomes of CADASIL patients have changed is unknown. So, we also want to investigate the content of NFL and Aβ42 in plasma exosomes of CADASIL patients.
Unfortunately, it is still very challenging to study exosomes let alone find the changes of patient’s exosomes due to their comparatively small size. In this study, we use transmission electron microscopy (TEM) and another new technique, nanoparticle tracking analysis (NTA), to characterize the morphology and number of plasma exosomes. The four transmembrane protein superfamily (such as CD63, CD81) is expressed on the surface of all exosomes. That means the level of CD63 indicates the total number of exosomes. The concentrations of pathology-related protein (NOTCH3, NFL, and Aβ42), which were normalized by CD63 [25], were compared between CADASIL patients and healthy controls.
MATERIALS AND METHODS
Participants and plasma collection
All samples were provided by Henan Provincial People’s Hospital. Inclusion criteria: all patients with CADASIL were diagnosed by genetic testing and/or skin biopsy [7, 12]. Normal subjects were healthy controls without NOTCH3 mutation. Exclusion criteria: subjects who refuse to participate in this study were excluded. Plasma samples were collected from patients who met the inclusion criteria and did not meet the exclusion criteria. Plasma sample were collected concurrently from healthy subjects who matched with CADASIL patients in terms of age, region, gender, and education level at the Health Medical Center. Each participant also underwent a detailed clinical evaluation, including magnetic resonance imaging (MRI) examination and cognitive function assessment, such as Montreal Cognitive Assessment (MOCA) and Mini-Mental State Examination (MMSE) scale (Table 1). MRI showed CADASIL-specific white matter lesions (WMLs), such as the external capsule and temporal pole [26]. Then, the severity of WML of CADASIL patients was quantified based on the Fazekas scoring criteria. Blood was collected into EDTA anti-coagulant Vacutainer tubes from all subjects in the morning after a 12 h fast. Then plasma was extracted and frozen at –80°C until testing. Details that might disclose the identity of the subjects under study have been omitted. The procedure was performed after obtaining informed consent.
Demographic information for CADASIL and control populations
Values was expressed as mean±standard deviation (SD). Statistical analysis was performed using Student’s t-test and the χ2 test. MOCA, Montreal cognitive assessment; MMSE, Mini-Mental State Examination.
Plasma exosome isolation
Exosomes were isolated from plasma using the Exosome Isolation Kit (EZB-exo1, EZBioscience) as described in the manufacture’s manual. Briefly, 300μl of plasma was transferred to an Eppendorf tube and centrifuged at 3000×g for 10 min to remove cells and cell debris. The supernatant was then transferred to another Eppendorf tube, mixed with 90μl of exosome precipitation reagent (EPR) and then incubated at 4°C for 2 h. Afterward, the EPR/biofluid mixture was centrifuged at 10000×g for 30 min. After centrifugation, the exosomes appeared as a beige-colored mass at the bottom of the tube. Finally, the supernatant was aspirated, taking great care not to disturb the precipitated exosome pellet.
Transmission electron microscopy
The exosome pellet was resuspended in 50μl phosphate-buffered saline (PBS). 10μl were then removed and diluted 1:10 in PBS buffer. 3μl of the solution was placed onto a copper net grid with carbon film suitable for use in the electron microscope. After 2 min, excess fluid was wicked off and a drop of phosphotungstic acid dye solution was added. 2 min later, excess fluid was wicked off once more and the sample was allowed to air dry. Finally, the completely dry copper mesh was photographed using a Philips-FEI Tecnai TEM (FEI G2).
Nanoparticle tracking analysis
The exosome pellet derived from plasma was resuspended in 300μl PBS. The resultant mixture was diluted 1:100 for testing using the NanoSight LM10 (NanoSight Ltd., Amesbury, UK), which sends a finely focused laser beam through a glass prism to illuminate the sample. Each sample was run 3 times. All analysis settings were kept constant within each experiment. Size distribution profiles obtained from NTA were averaged for each sample across the replicates and then averaged across samples to obtain representative size distribution profiles.
Enzyme-linked immunosorbent assay
150μl lysate and 1.5μl protease inhibitor was added to the exosomes extracted from plasma and the mixture was vortexed for 30 s and resuspended in solution. The solution was chilled at –80°C for 5 min and then left at 25°C for 5 min, and 3 cycles of chilling and thawing were repeated. The solution was then stored at –80°C. Proteins derived from plasma exosomes were quantified using enzyme-linked immunosorbent assay (ELISA) kits (mlbio, MBS,USA) for NOTCH3 (sc-7424, Santa Cruz Bio-technology), NFL (#MBS2541999, MyBioSource), Aβ42 (#MBS592143, MyBioSource), and CD63 (#MBS2544215, MyBioSource), which was measured to normalize the exosome content. The specimen, standard and horseradish peroxidase (HRP)-labeled detection antibodies corresponding to four proteins were sequentially added to microwells pre-coated with human NOTCH3, NFL, Aβ42, and CD63 capture antibody, respectively. The microwells were incubated at 37°C and washed thoroughly. The substrate 3,3’, 5,5’-tetramethylbenzidine (TMB) was used for developing blue for 30 min and then the reaction was blocked with H2SO4 stop solution. The optical densities were recorded at 450 nm. The r2 of the correlation of standard curve for NOTCH3, NFL, Aβ42, and CD63 is 0.9991, 0.9991, 0.9996, and 0.993, respectively.
Statistical analysis
Statistical analysis was performed using SPSS v.23.0 software and results were presented by GraphPad Prism 5. For categorical data, group differences were analyzed using the χ2 test. Two independent sample t-tests were run for the continuous variables. Correlative analysis was performed using Pearson. The data obtained was presented by mean±SD and p < 0.05 was considered statistically significant.
RESULTS
The exosomes are ring-shaped both of CADASIL patients and controls
Ring-shaped plasma exosomes were observed in both CADASIL patients and the healthy controls. Compared to those from the matched control group, the exosomes of CADASIL patients were relatively aggregated (Fig. 1).

Electron micrograph of plasma exosomes. A) Picture of plasma exosomes from normal subjects. B) Picture of plasma exosomes from CADASIL patients. Scale bar = 100 nm.
The number of exosomes of CADASIL patients was significantly lower than healthy controls
Exosomes are believed to be most abundant in the lowest size range (30–150 nm), so the number of exosomes with diameters of 30–150 nm in the control and CADASIL groups was compared. The number of plasma exosomes with diameters ranging from 30–150 nm in CADASIL patients was significantly lower than in the healthy subjects (p =0.0409 < 0.05). In addition, the median size of plasma EVs of CADASIL patients was bigger than controls group, and the difference was statistically significant (p = 0.0488 < 0.05) (Fig. 2). As can be seen from the peak graph, compared to healthy controls, the graph of EVs in CADASIL patients was generally presented as two or multiple peaks, with a lower peak (Fig. 2).

Number and diameter distribution of plasma exosomes by NTA. A, B) The number and median size of plasma-derived exosomes according to NTA. A) Represents the number of exosomes with diameter in the range of 30-150 nm in healthy subjects and CADASIL patients. B) Represents the median of the diameter distribution of plasma exosomes in healthy controls and CADASIL patients. Error bars, representing standard deviation of the sample mean, are a measure of the degree of dispersion of the mean sample distribution and the mean sample error, reflecting the variance between sample means. *p≤0.05 (Student’s t-test). C, D) The size distribution of plasma-derived exosomes observed by NTA. Diameter of the plasma exosomes plotted on the abscissa and concentration plotted on the ordinate. C) Peak map representing plasma exosomes from healthy subjects. D) Peak map representing plasma exosomes from CADASIL patients.
CADASIL plasma exosomes had significantly lower levels of NOTCH3 and significantly increased levels of NFL
The results showed that the levels of NOTCH3 protein were significantly reduced in the CADASIL population compared to the levels in the age-matched healthy controls (p = 0.0002 < 0.05). The levels of NFL protein of plasma exosomes were significantly elevated in CADASIL patients (p = 0.0112 < 0.05). Aβ42 protein levels were slightly lower in CADASIL patients, however, the difference was not statistically significant (p = 0.9012 > 0.05) (Fig. 3).
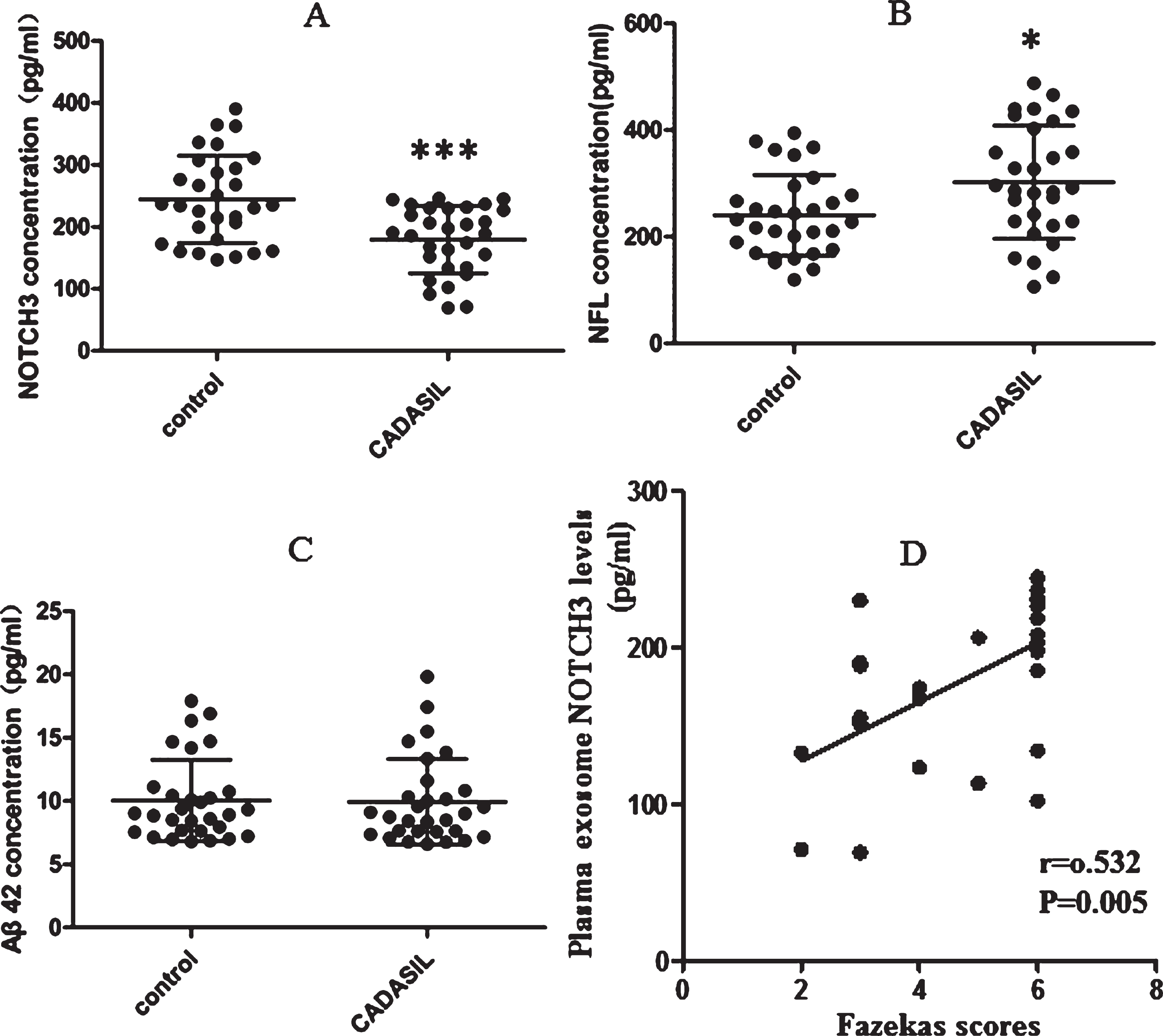
A-C) Comparison of protein concentration from plasma exosome of normal subjects and CADASIL patients. A) NOTCH3 protein; B) NFL protein; C) Aβ42 protein. ***p≤0.001; *p≤0.05 (Student’s t-test). D) Correlation between plasma exosome NOTCH3 levels and Fazekas scores (determined by calculating Pearson’s correlation coefficient).
The NOTCH3 level of CADASIL plasma exosome is significantly correlated with severity of WML
Currently, the clinical indications that reflect the severity and progression of CADASIL, including white matter demyelination, indicated by Fazekas score, and cognitive function, reflected using MOCA and MMSE scale score. Then in order to find out whether there is a correlation between protein concentration and clinical progression of CADASIL, a Pearson correlation analysis was performed. The result showed that plasma exosome NOTCH3 levels were positively correlated with the Fazekas score (r = 0.532, p = 0.0051) (Fig. 3). However, no relation was found in remaining correlation analysis.
DISCUSSION
In this study, TEM and NTA were applied in order to measure the morphology and size distribution of plasma exosomes. Our data showed that exosomes in both CADASIL patients and matched healthy controls are ring-shaped. Previous studies have indicated that exosomes may shrink or change size during preparation for TEM [27], but TEM is still useful for observing the morphology and structure of exosomes.
In addition, compared to plasma exosomes in CADASIL patients, the exosome distribution in healthy subjects is relatively scattered and uniform, and exosome diameter is relatively smaller. What’s more, the number of plasma exosomes in CADASIL patients was significantly lower than in the healthy subjects. which indicate that the formation and/or secretion of exosomes in CADASIL patients may have changed. Exosomes are known as significant mediators of intercellular communication, enabling the transfer biological signals from the donor cells to the recipient cells [28, 29]. So, the intercellular communication of CADASIL patients may be impaired [30], which may be involved in the pathogenesis of the disease. Of course, this is only our preliminary study on the exosomes of CADASIL patients, and further research are needed in the future.
Mounting evidence has shown that exosomes and autophagy collaboratively remove harmful/abnormal proteins to maintain cellular homeostasis [31–33]. Morphologic structures related to autophagy were also present in the pericytes of NOTCH3 mutant transgenic mice [34]. In addition, Hanemaaijer et al. also had discovered that autophagy dysregulation or insufficient autophagosomes-lysosomes fusion take place in human CADASIL VSMCs [24]. However, our data showed that plasma exosomal NOTCH3 is significantly reduced in CADASIL patients compared to matched healthy controls, which seems to be inconsistent with the previous view. The possible explanation is that the mutant NOTCH3 cannot be recognized by the process of endosomal sorting and transportation, considered as a complex process of mutual recognition of proteins, due to structural changes [35]. What’s more, proteomic studies using cultivated VSMCs from a CADASIL patient indicated that mutant Notch3 causes endoplasmic reticulum (ER) stress, leading to impaired cell proliferation [36]. Recently, Neves et al. showed that Notch3-Nox5/ER stress/ROCK signaling may underlie the vasculopathy of CADASIL [37]. Therefore, we hypothesize that autophagy disorder and impaired exosomal formation and secretion may jointly lead to the weakened clearance of mutant NOTCH3 protein in VSMCs, which in turn aggravates ER stress, causing VSMCs degeneration even death.
Unexpectedly, we also found that plasma exosomes of CADASIL had elevated levels of NFL and the difference was statistically significant. Sjögren et al. first reported that CSF-NFL was increased in patients with moderate to severe WMLs after correction for age, gender, and degree of cognitive impairment [38]. As mentioned before, WMLs are a key characteristic in CADASIL patients and always appear precede the clinical symptoms, and gradually worsen with age. Additionally, since exosomes can freely cross the blood-brain barrier. So, the elevated of exosome-NFL may be related to WMLs of CADASIL. Later, Gravesteijn et al. indicated that serum NFL levels correlate with disease severity, disease progression, and 17-year survival in CADASIL patients [39]. Plasma NFL also can predict stroke in CADASIL patients [40]. Additionally, Gattringer et al. also showed that serum NFL is increased in patients who occur the new CSVD-related MRI lesions, even when clinically silent [41]. Although Kuhle et al. discovered that ELISA has relatively low sensitivity to measure NFL levels in serum, it still supports the feasibility of quantifying NFL in body fluids [42]. Fortunately, exosomal membranes protect the contents from degradation (such as acid and alkali) in peripheral blood, which can play a role in enrichment. Therefore, exosome-NFL concentration is a promising biomarker to monitor and predict disease course in CADASIL, as well as potentially assessing therapeutic response in future clinical trials.
Interestingly, the level of NOTCH3 in CADASIL patients is significantly correlated with Fazekas scores, which means that the NOTCH3 concentration of CADASIL plasma exosome is related to the severity of white matter damage. WMLs in CADASIL are underlaid by severe ultrastructural changes of the arteriolar wall [43]. Several studies have shown that the degree of the underlying ultrastructural alterations in the white matter is related to the severity of CADASIL clinical status, and the larger extents of WML in pyramidal tracts were associated with worse outcomes [44, 45]. Therefore, the level of NOTCH3 derived from plasm exosomes in CADASIL patients can reflect the severity of white matter lesions and may act as a biomarker for monitoring and predicting CADASIL disease progression and measuring therapeutic effectiveness, which deserves additional longitudinal studies. However, no obvious correlation was found between exosomal proteins levels and cognitive impairment, maybe because the cognitive scale we chose is not accurate enough. While MOCA and MMSE scale scores assess overall cognitive function, CADASIL patients selectively damage some specific cognitive domains, such as executive function. So, the scoring results of MOCA and MMSE cannot accurately reflect the impairment of specific cognitive domains. A scale that can more accurately assess cognitive impairment and neurological dysfunction should be used for further research.
In conclusion, our study found that plasma exosomal NOTCH3 is significantly reduced in CADASIL patients, which provide a new perspective for pathogenesis research of CADASIL. We believe that in the near future, with further understanding of the molecular mechanisms related to autophagy-exosomal secretion, it will help us clarify the specific pathogenesis of CADASIL. In addition, plasma exosome NOTCH3 and NFL levels may act as biomarkers to monitor and predict disease progression and measure therapeutic effectiveness in the clinical trials. Much more efforts should be done for longitudinal studies on changes in exosomal NOTCH3 and NFL levels and the correlation between protein concentration and clinical severity.