
Abstract
Background:
Cardiovascular risk factors increase the risk of developing dementia, including Alzheimer’s disease and vascular dementia.
Objective:
Studying individuals with autosomal dominant mutations leading to the early onset of dementia, this study examines the effect of the global cardiovascular risk profile on early cognitive and neuroimaging features of Alzheimer’s disease and vascular dementia.
Methods:
We studied 85 non-demented and stroke-free individuals, including 20 subjects with Presenilin1 (PSEN1) E280A mutation leading to the early onset of autosomal dominant Alzheimer’s disease (ADAD), 20 subjects with NOTCH3 mutations leading to cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) and to the early onset of vascular dementia, and 45 non-affected family members (non-carriers). All subjects underwent clinical and neuropsychological evaluations and an MRI. The global cardiovascular risk profile was estimated using the office-based Framingham Cardiovascular Risk Profile (FCRP) score.
Results:
In individuals with CADASIL, a higher FCRP score was associated with a reduced hippocampal volume (B = –0.06, p < 0.05) and an increased severity of cerebral microbleeds (B = 0.13, p < 0.001), lacunes (B = 0.30, p < 0.001), and perivascular space enlargement in the basal ganglia (B = 0.50, p < 0.05). There was no significant association between the FCRP score and neuroimaging measures in ADAD or non-carrier subjects. While the FCRP score was related to performance in executive function in non-carrier subjects (B = 0.06, p < 0.05), it was not significantly associated with cognitive performance in individuals with CADASIL or ADAD.
Conclusion:
Our results suggest that individuals with CADASIL and other forms of vascular cognitive impairment might particularly benefit from early interventions aimed at controlling cardiovascular risks.
Keywords
INTRODUCTION
Modifiable cardiovascular risk factors, such as hypertension, smoking, diabetes, and hypercholesterolemia, tend to cluster and exert a deleterious additive effect on brain integrity, as reflected by an increased presence of neuroimaging markers of cerebrovascular disease and decrease in global or regional brain volume [1–4]. Cardiovascular risk factors also increase the risk of developing dementia [5–7] and have been linked to lower cognitive performance in individuals with normal cognition, emphasizing the relevance of vascular contributions to cognitive impairment and dementia [8–11].
Alzheimer’s disease (AD) and vascular dementia (VaD) are the two most prevalent causes of dementia in the aging population [12]. Past research suggests that cardiovascular risk factors influence the incidence and clinical trajectory of both AD and VaD [5, 14]. However, because cerebrovascular changes and age-related neurodegenerative pathologies (e.g., AD) frequently co-exist in aging individuals [15], it has been challenging to characterize the disease-specific impact of cardiovascular risk factors on the clinical presentation of VaD and AD. The examination of individuals with autosomal dominant mutations leading to the early onset of dementia might allow a more precise examination of the early and disease-specific effects of cardiovascular risks, in the absence of confounding factors associated with older age.
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), a condition linked to mutations on the NOTCH3 gene, leads to the early onset of cerebral small vessel disease and VaD [16, 17]. On neuroimaging investigation, individuals with CADASIL present hallmark features of cerebral small vessel disease, including the presence of widespread white matter hyperintensity (WMH), cerebral microbleeds (CMB), lacunes of presumed vascular origin (lacunes), and enlarged perivascular spaces (EPVS) (for reviews, see [18–20]). Global and regional brain atrophy has also been reported in this population [21]. Cognitive deficits in executive function and processing speed are a central symptom of the disease and eventually progress into a VaD syndrome [22–24].
Individuals with the PSEN1 E280A mutation develop, with utmost certainty, autosomal dominant Alzheimer’s disease (ADAD) at an early age, with cognitive symptoms usually emerging in the mid-forties [25, 26]. Individuals with ADAD present early volumetric changes in the posterior parietal lobe and medial temporal lobe regions [27]. While the presence of white matter hyperintensity has recently been described as a potentially significant manifestation of the disease [28], the neuropathological hallmarks of ADAD consist in the abnormal aggregation of amyloid and tau proteins in the brain [29, 30]. Reduced performance in verbal episodic memory is one of the earliest and predominant cognitive symptoms in ADAD [27, 31]. Deficits in semantics and attention have also been reported, but at more advanced stages of the disease [27].
The objective of this study was to examine associations between a widely used office-based global cardiovascular risk score, the Framingham general cardiovascular disease risk profile (FCRP), structural neuroimaging features, and cognitive functioning in presymptomatic individuals with CADASIL and ADAD. This study will shed light into the disease-specific influence of the global cardiovascular risk burden on early clinical features of ADAD and VaD, as well as provide relevant information on modifiable factors potentially influencing the phenotypic heterogeneity of these disorders.
METHODS
Participants
This cross-sectional study examined participants aged over 30 years (no upper limit) from a cohort of individuals presenting a family history of ADAD or CADASIL. Participants were recruited between December 2015 and June 2019 from the patient registry of the Neuroscience Group of the University of Antioquia (Colombia). Only subjects at a presymptomatic disease stage were included in the study, defined by: 1) the absence of history of ischemic or hemorrhagic strokes and 2) the absence of dementia, as determined based on neurological examination and a score lower than 2 on the Functional Assessment Staging (FAST) [32]. Participants with incomplete MRI scan, neuropsychological testing, or cardiovascular risks assessment were excluded from the study. The data was collected in a double-bind fashion and genotyping for PSEN1 E280A and NOTCH3 mutations was performed after data collection was completed to determine group status (i.e., carrier versus non-carrier) [33, 34]. All participants provided informed consent and study procedures were approved by the Bioethics Committee of the University of Antioquia.
Computation of the Framingham risk profile
The Framingham general cardiovascular disease risk profile (FCRP) is a multivariate risk score derived from the examination of data from the Framingham Heart Study and providing a sex- and age-specific estimate of the 10-year absolute risk for subsequent cardiovascular events [35]. While this score usually encompasses laboratory measures of cholesterol, D’Agostino and colleagues (2008) also propose a score based on non-laboratory (or office-based) measures taking into account age, sex, systolic blood pressure, treatment for hypertension, current smoking, diabetes status, and body mass index (BMI). The laboratory and non-laboratory-based FCRP scores both show good discrimination and calibration in predicting subsequent cardiovascular events [35, 36] and have been widely used in the literature as a global measure of cardiovascular risks [37, 38].
Using standard questionnaires and examination procedures, the following cardiovascular risk factors were assessed in all study participants: systolic and diastolic blood pressure, treatment for hypertension, BMI, smoking status, and diabetes mellitus status. These variables were entered in a standard equation, together with sex and age, to obtain the final non-laboratory FCRP score [39]. This data was collected during the clinical visit of the study, which took place within three months of the neuropsychological and neuroimaging study visits.
Assessment of cognitive functioning
Participants underwent a detailed neuropsychological evaluation. Cognitive status was evaluated with the Mini-Mental State Examination (MMSE) [40]. Global cognitive functioning was assessed with the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) neuropsychological battery Total Score [41–43]. Specific cognitive domains were assessed with the following tests: Memory (CERAD Word List Learning Total Immediate Recall, Delayed Recall, and Recognition); Language (CERAD Verbal Fluency and abbreviated Boston Naming); Processing Speed (WAIS-III Digit-Symbol Coding and Trail Making Test A) [44, 45]; and Executive Function (Letter Fluency, Trail Making Test B, Wisconsin Card Sorting Test–perseveration errors and Letter-Number sequencing) [44–46]. Performance on each test was converted to a Z-score, using the mean performance of non-carrier individuals. To create domain-specific composite scores, Z-scores were averaged across tests included within each cognitive domain.
MRI acquisition
MRI scans were performed at the Hospital Pablo Tobón Uribe (Medellín, Colombia) on a Siemens 3.0 Tesla scanner. The scanning protocol included a high-resolution T1-weighted magnetization prepared rapid acquisition gradient echo (MPRAGE; repetition time [TR]/echo time [TE]: 2000/2.45 ms; resolution: 0.96*0.96*0.96), a T2-susceptibility weighted imaging (SWI; TR/TE: 27/20 ms, resolution: 0.76*0.76*1.8), a T2-weighted gradient-echo (GRE; TR/TE: 639/20 ms, resolution: 0.94*0.94*3.3), a T2-turbo spin-echo (TSE: TR/TE: 4700/94 ms, resolution: 0.36*0.36*3.0), and a T2-fluid attenuation inversion recovery (FLAIR; TR/TE: 8000/81 ms, resolution: 0.68*0.68*5.0).
Quantification of structural MRI features
Structural MRI markers of cerebral small vessel disease, including cerebral microbleeds (CMB), lacunes, and enlarged perivascular spaces (EPVS) in the basal ganglia (EPVS-BG) and centrum semiovale (EPVS-CSO), were quantified on MRI images according to published consensus guidelines (STRIVE) and protocols (Fig. 1) [47, 48]. The volume of WMH was obtained using FreeSurfer (version 6.0) [49, 50] and normalized to the total brain volume (nWMH). The severity of periventricular WMH was also rated on FLAIR images using the Fazekas scale [51].
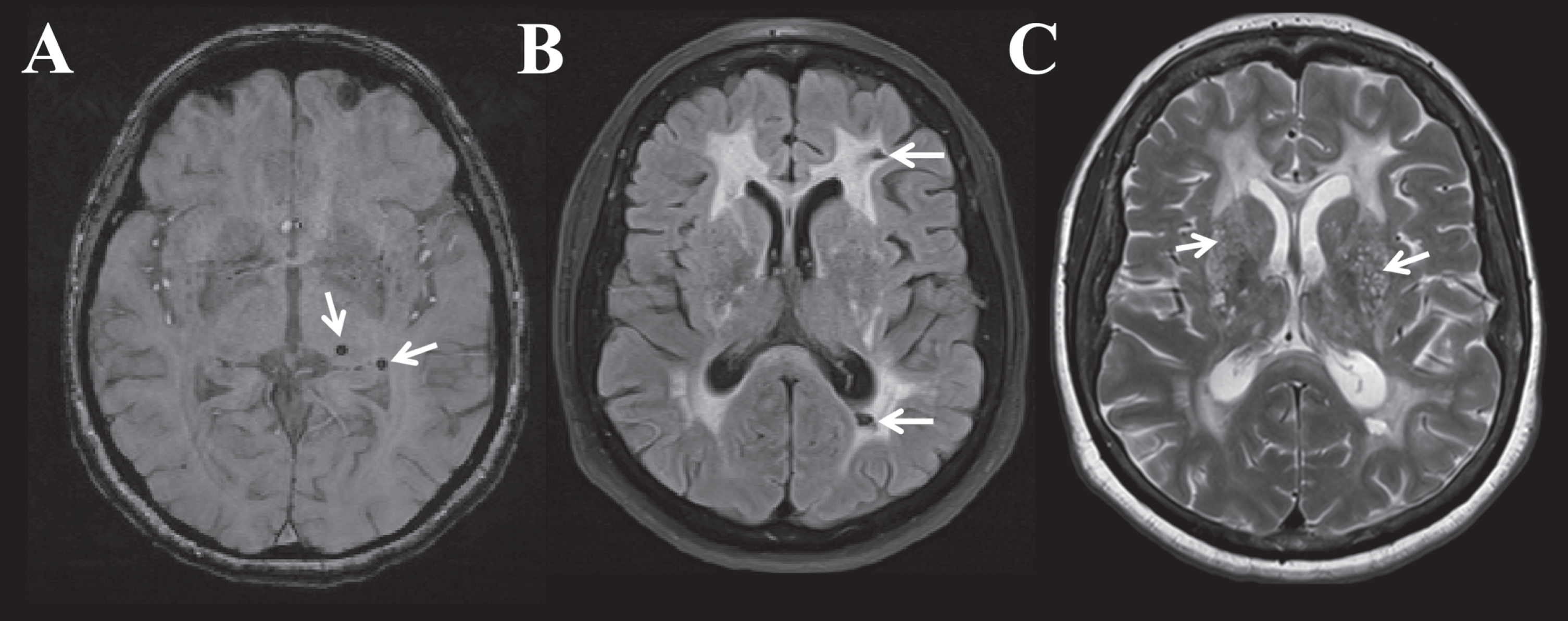
Illustration of quantified structural neuroimaging markers of cerebral small vessel disease. A) Cerebral microbleeds (CMB) identified by white arrows on a susceptibility weighted imaging (SWI) sequence; B) Lacunes and extensive white matter hyperintensity identified by white arrows on a fluid-attenuated inversion recovery (FLAIR) sequence; C) Enlarged perivascular space (EPVS) in the basal ganglia identified by white arrows on a T2 TSE sequence.
To obtain an estimation of whole-brain atrophy, we computed the brain parenchymal fraction, consisting in a ratio of the total brain volume to the estimated total intracranial volume. Medial temporal lobe atrophy was estimated using the normalized hippocampal volume (nHC), consisting in a ratio of the bilateral hippocampal volume to the estimated total intracranial volume. All volumetric measures were obtained using FreeSurfer (version 6.0) [49, 50].
Finally, a SVD Sum Score (an ordinal score representing the overall severity of the “SVD state”) was calculated in each participant [52, 53]. The SVD Sum Score was computed as follow: 1) one point was awarded for the presence of 1 or more CMB; 2) one point was awarded for the presence of 1 or more lacunes; 3) one point was awarded for the presence of extensive WMH in the periventricular region (i.e., Fazekas grade > 2), and 4) one point was awarded for the presence of moderate to severe EPVS in the basal ganglia (EPVS-BG ratings > 2).
Statistical analysis
Groups were contrasted on demographic variables and individual cardiovascular risk factors using one-way ANOVAs for continuous variables and chi-square tests for dichotomous variables. Group differences on the FCRP score were assessed using an ANCOVA, controlling for age and sex. Group differences on cognitive scores were assessed using ANCOVAs, controlling for age and education. All pairwise comparisons were assessed using Bonferroni’s multiple comparisons post-hoc tests.
Group differences on neuroimaging markers were assessed using generalized linear models (GLMs), which allows a more flexible modeling of data with non-parametric distributions, with group as a factor and age and sex as additional covariates. GLMs were fitted with a Gaussian distribution for parametric continuous variables (nHC, BPF), a quasi-Poisson distribution for count variables (CMB and lacune), a Gamma distribution with a log link function for non-parametric continuous variables (nWMH), and an ordinal logistic distribution for ordinal variables (EPVS-CSO or -BG, SVD Sum Score). Main effects were assessed with Likelihood Ratio Chi-square tests (LRT) and pairwise comparisons with Bonferroni’s multiple comparisons post-hoc tests.
The influence of the FCRP score on neuroimaging markers was assessed in each group separately using GLMs fitted as previously described, with neuroimaging markers as the outcome variable and the FCRP score as the predictor. To avoid potential confound associated with more advanced disease progression, age was included in each model as an additional covariate. Model fit was assessed with the McFadden Pseudo-R2 obtained with the “PseudoR2” function in R (version 6.3) [54]. Finally, the influence of the FCRP score on cognitive performance was assessed in each group separately in multivariable linear regression models, with age and education as additional covariates. For each observed significant effect associated with the FCRP score, we computed post-hoc exploratory analyses to determine which cardiovascular risk factors contributed to the findings. For this purpose, we used similar GLMs as previously described, but including each individual cardiovascular risk factor as predictors instead of the global FCRP score.
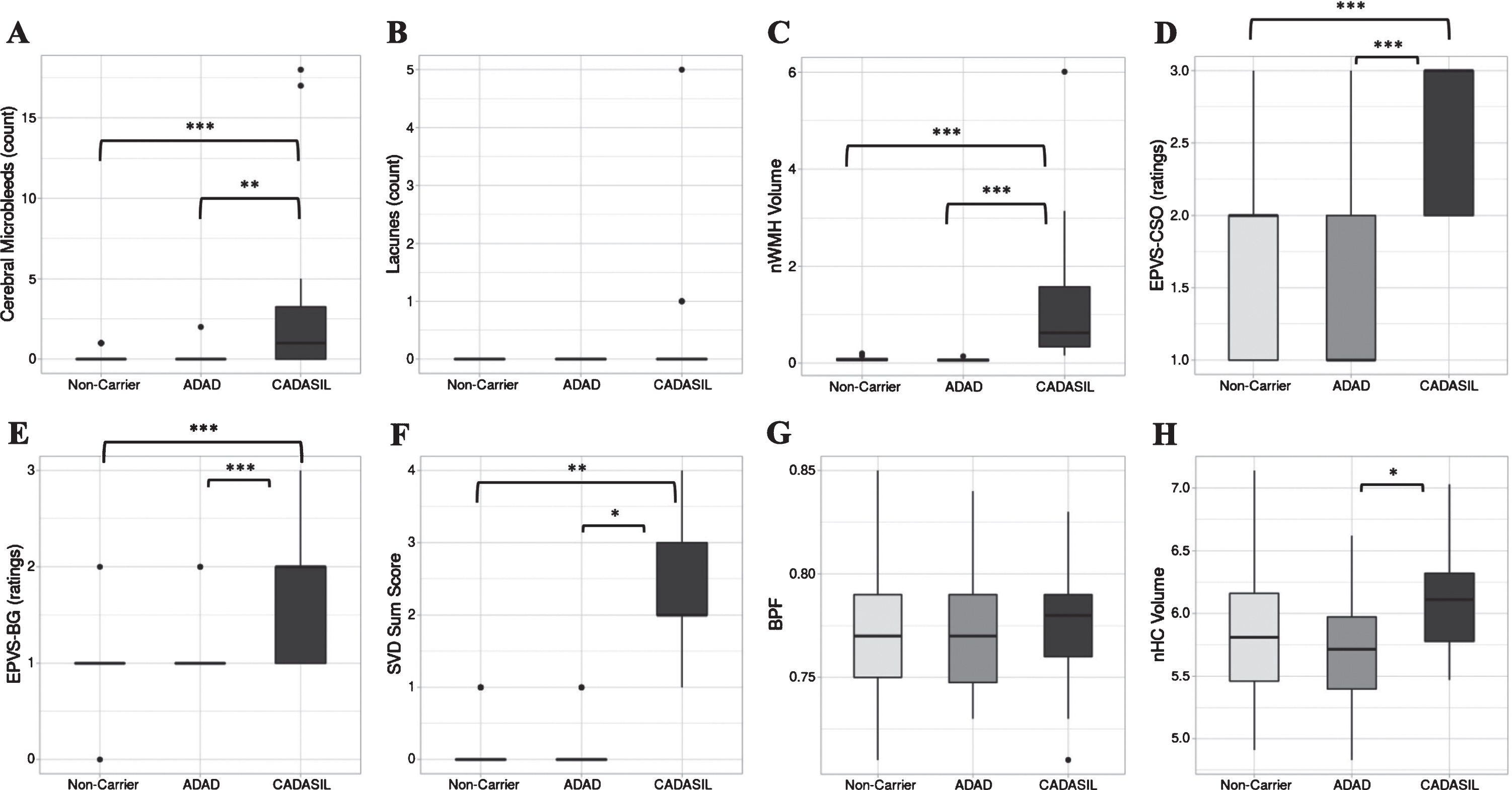
Boxplots illustrating differences in quantified MRI markers across groups. A) CMB, cerebral microbleed count; B) Lacune count; C) nWMH, normalized white matter hyperintensity volume; D) EPVS CSO, ratings of perivascular space enlargement in the centrum semiovale; E) EPVS BG, ratings of perivascular space enlargement in the basal ganglia; F) SVD Sum Score, score representing the overall burden of MRI markers of small vessel disease; G) BPF, brain parenchymal fraction; H) nHC, normalized hippocampal volume. Group differences analyses were performed using generalized linear models, with age and sex as additional covariates. *p < 0.05, **p < 0.01, ***p < 0.001.
RESULTS
Group differences in demographic, cardiovascular, and cognitive features
Demographic, cardiovascular, and cognitive characteristics of each group are summarized in Table 1. Groups were equivalent in terms of years of education, but a significant group effect was observed for age (p = 0.012). Post-hoc analyses revealed that presymptomatic ADAD subjects were, on average, younger than presymptomatic CADASIL subjects (p = 0.012). There was also a significant group effect for sex representation (p = 0.011), driven by an overrepresentation of the female sex in the presymptomatic CADASIL group as opposed to the non-carrier group (p = 0.003). Groups did not differ on individual cardiovascular risk factors or on the FCRP score after controlling for age and sex.
After controlling for age and education, a significant group effect was observed on the MMSE (p = 0.004), CERAD Total Score (p < 0.001), Memory Composite (p = 0.001), Processing Speed Composite (p = 0.002) and Executive Function Composite (p < 0.001), but not on the Language Composite. Post-hoc analyses revealed a significantly lower MMSE score for presymptomatic ADAD compared to non-carriers (p = 0.003). Both presymptomatic ADAD (p = 0.002) and presymptomatic CADASIL (p = 0.007) subjects had lower CERAD Total Score compared to non-carriers. The Memory Composite score was also reduced in both presymptomatic ADAD (p = 0.003) and presymptomatic CADASIL (p = 0.03) subjects compared to non-carriers. The Processing Speed Composite was significantly reduced in presymptomatic CADASIL subjects compared to non-carriers (p = 0.002). Finally, the Executive Function Composite was significantly reduced in presymptomatic CADASIL subjects compared to both presymptomatic ADAD subjects (p =0.02) and non-carriers (p < 0.001).
Summary of demographic, clinical, and cognitive characteristics
Presented values are mean±SD, unless otherwise specified. n (%), number of subjects presenting with the listed condition (representative percentage of the group). Group differences on continuous variable (age, years of education, systolic blood pressure, body mass index) were assessed using one-way ANOVAs, with Bonferroni’s post-hoc tests. Group differences on dichotomous variables (sex, hypertension treatment, diabetes, and tobacco use) were assessed using chi-square tests. Group differences on the Framingham Risk Profile (FCRP) score were assessed using an ANCOVA, controlling for age and sex, with Bonferroni’s post-hoc tests. Group differences in cognitive performance (MMSE, CERAD Total Score and domain-specific cognitive scores) were assessed using ANCOVAs, controlling for age and education, with Bonferroni’s post-hoc tests. Because domain-specific cognitive scores were obtained using the performance of the non-carriers group as a reference, the mean for non-carrier subjects on all domain-specific composite scores is 0. apresymptomatic autosomal dominant Alzheimer’s disease (ADAD) group, bpresymptomatic CADASIL group, cnon-carriers group;*p < 0.05, **p < 0.01, ***p < 0.001.
Group differences in quantified neuroimaging markers
Non-carriers and presymptomatic ADAD subjects presented with scarce or absent MRI markers of cerebral small vessel disease. None of the presymptomatic ADAD (0%) or non-carrier (0%) subjects presented with lacunes, whereas only one presymptomatic ADAD subject (5%) and four non-carriers (9%) presented with a single cerebral microbleed. The SVD Sum Score was generally low in presymptomatic ADAD and non-carrier subjects: the vast majority of presymptomatic ADAD (85%) and non-carriers (89%) had a SVD Sum Score of “0”, while three presymptomatic ADAD (15%) and five non-carrier (11%) subjects presented a SVD Sum Score of “1”.
After adjusting for differences in age and sex, analyses revealed a significant group effect for the CMB count (p < 0.001), nWMH volume (p < 0.001), EPVS-CSO ratings (p < 0.001), EPVS-BG ratings (p < 0.001), SVD Sum Score (p < 0.001), and nHC volume (p = 0.04). The lacune count and BPF did not significantly differ across groups. Post-hoc analyses revealed that, as expected, presymptomatic CADASIL subjects presented an increased severity of MRI markers of cerebral small vessel disease as opposed to both presymptomatic ADAD and non-carrier subjects, including a greater CMB count, nWMH volume, EPVS-CSO and EPVS-BG ratings, and SVD Sum Score (see Fig. 2). Presymptomatic subjects with ADAD had a lower nHC volume than presymptomatic subjects with CADASIL (p = 0.047) but did not differ from non-carriers on any of the examined structural MRI markers after accounting for age and sex.
Associations between the FCRP and neuroimaging markers
Because of the low variance in MRI markers of cerebral small vessel disease in presymptomatic ADAD and non-carrier subjects, generalized linear models examining associations between the FCRP score and these markers were only examined in the presymptomatic CADASIL group. In presymptomatic subjects with CADASIL, the FCRP score significantly contributed to the explained variance in CMB (p < 0.001), lacunes (p < 0.001), EPVS-BG (p = 0.04), and SVD Sum Score (p = 0.03) after adjusting for age but did not significantly relate to nWMH volume or EPVS-CSO (Table 2). Exploratory analyses to determine which individual cardiovascular risk factors contributed to these observed effects revealed that systolic blood pressure (B = 0.05, 95%CI = 0.03–0.06, p < 0.001) and BMI (B = 0.20, 95%CI = 0.11–0.29, p < 0.001) were the only cardiovascular risk factors independently contributing to the variance in CMB after adjusting for age. The presence of lacunes was influenced by systolic blood pressure (B = 0.12, 95%CI = 0.04–0.21, p = 0.006), BMI (B = 0.45, 95%CI = 0.11–0.797, p = 0.009), and smoking (B = 2.00, 95%CI = 0.1–4.00, p = 0.049). In contrast, both EPVS-BG and the SVD Sum Score were not significantly associated with any individual cardiovascular risk factors (p < 0.05 for all) suggesting that these markers were more strongly related to the global burden of cardiovascular risk.
After adjusting for age, analyses looking at associations between the FCRP score and MRI markers of neurodegeneration in all three groups (Table 2) revealed a negative association between the FCRP and nHC volume in presymptomatic CADASIL subjects (p = 0.03). In contrast, no association reached statistical significance in the presymptomatic ADAD or non-carrier group.
Summary of regression models for the prediction of neuroimaging markers
Summary of generalized linear regression models evaluating the predictive value of the Framingham general cardiovascular risk profile (FCRP) score on structural neuroimaging measures of cerebral small vessel disease and neurodegeneration after adjusting for age. Because of the low variance of MRI markers of cerebral small vessel disease in ADAD and non-carrier subjects, these models were only evaluated in presymptomatic CADASIL subjects. Overall model fit and predictive power were assessed using the McFadden Pseudo-R2. For each variable included in the models, the presented value is the Unstandardized B Coefficient [95%Wald Confidence Intervals]. CMB, count of cerebral microbleeds; Lacune, count of lacunes, nWMH, normalized volume of white matter hyperintensity; EPVS-CSO, ratings of enlarged perivascular spaces in the centrum semiovale; EPVS-BG, ratings of enlarged perivascular spaces in the basal ganglia; SVD Sum Score, ordinal score representing the overall burden of MRI markers of cerebral small vessel disease; BPF, brain parenchymal fraction; nHC, normalized hippocampal volume. *p < 0.05, **p < 0.01, ***p < 0.001.
Associations between the FCRP and cognitive performance
In presymptomatic subjects with ADAD or CADASIL, the FCRP score did not independently contribute to the variance in performance across all cognitive domains (Table 3). In contrast, a significant negative association between the FCRP score and performance on the Executive Function composite was noted in non-carriers (p = 0.02).
Summary of regression models for the prediction of cognitive performance
Summary of general linear regression models evaluating the predictive value of the Framingham general cardiovascular risk profile (FCRP) score on cognitive performance after adjusting for age and education for each group separately. For each variable included in the models, the presented value is the Unstandardized B Coefficient [95%Confidence Intervals]. MMSE, Mini-Mental State Examination; CERAD Total Score, total score on the neuropsychological battery of the Consortium to Establish a Registry for Alzheimer’s Disease; Proc. Speed, processing speed. *p < 0.05, **p < 0.01, ***p < 0.001.
DISCUSSION
This present study examined associations of the global cardiovascular risk profile with structural neuroimaging markers and cognitive functioning in presymptomatic individuals with CADASIL and ADAD. This study resulted in two main findings. First, our results suggest that the global cardiovascular risk profile influences the neuroimaging profile in presymptomatic subjects with CADASIL, but not in presymptomatic subjects with ADAD or in non-carriers. Second, our results highlight an absence of association between the cardiovascular risks profile and cognition in the presymptomatic stages of both CADASIL and ADAD.
This study contributes to the characterization of early and disease-specific neuroimaging and cognitive features in the presymptomatic stages of ADAD and CADASIL. We found an increased presence of CMB, lacunes, WMH, and EPVS in presymptomatic individuals with CADASIL, consistent with the presence of cerebral small vessel disease and with previous reports in this population [19, 55]. In contrast, we observed a low occurrence of MRI markers of cerebral small vessel disease in presymptomatic ADAD and non-carrier individuals. Previous studies have examined the frequency of CMB in ADAD, with prevalence estimates ranging from 14%to 25%[28, 57]. Research work from Lee and colleagues found that CMB were more prevalent in ADAD than in non-carriers, and more frequently affected subjects that were older (i.e., mid-forties), had lower cognitive functioning, and were closer to estimated age of symptoms onset [28, 56]. This suggests that CMB might be more common at later stages in the disease trajectory of ADAD, which could explain their relatively low frequency (5%) in our cohort of presymptomatic ADAD individuals [56]. While the presence of WMH has been proposed as a potential accompanying feature of ADAD [28, 58], we did not find a significant difference in the normalized WMH volume between presymptomatic PSEN1 mutation carriers and non-carriers, also suggesting that WMH might be a later event in the disease trajectory. Presymptomatic subjects with ADAD had a lower nHC volume than presymptomatic subjects with CADASIL but did not differ from non-carriers. The global brain volume did not differ across all three groups, which is consistent with previous findings in non-demented PSEN1 and NOTCH3 [59] mutation carriers. Although previous reports have described diffuse or regional brain atrophy in CADASIL and ADAD [60–62], discrepancies in results could be explained by differences in genotypes, demographics, and disease stages between studied samples. When characterizing cognitive functioning across groups, presymptomatic individuals with CADASIL exhibited impairment across a broad range of cognitive functions as opposed to non-carriers, with predominant impairments in executive function and processing speed. This finding aligns with previous reports describing executive and processing speed deficits as an early and chief cognitive manifestation in CADASIL and other forms of vascular cognitive impairment [34, 63]. In contrast to non-carrier subjects, presymptomatic individuals with ADAD showed a reduced performance in global cognitive functioning and memory, corroborating the predominance of memory impairment in this population [64]. With the exception of a greater impairment in executive function for the CADASIL group, presymptomatic individuals with CADASIL and ADAD otherwise presented a globally similar cognitive profile.
The main objective of this study was to explore associations between the global cardiovascular risk profile and the neuroimaging or cognitive presentation of individuals at early stages of CADASIL, in parallel to associations found in the early stages of ADAD and in non-carriers. In presymptomatic patients with CADASIL, our results highlight an influence of the FCRP score on multiple MRI markers of cerebral small vessel disease after accounting for age, including the CMB count, lacune count, and EPVS in the basal ganglia. Consistently, a higher FCRP score was related to an increased severity of the overall burden of MRI markers of cerebral small vessel disease in presymptomatic subjects with CADASIL, as quantified via an SVD Sum Score. Exploratory post-hoc analyses revealed that both a higher count of CMB and lacunes were independently associated with higher BMI and systolic blood pressure after adjusting for age, whereas smoking was selectively related to the presence of lacunes. In contrast, no individual cardiovascular risk factor was independently related to the variance in EPVS in the basal ganglia or in SVD Sum Score, indicating a more global effect of cardiovascular risk factors on these two markers. While the influence of the global cardiovascular risk profile has not been explicitly investigated in CADASIL, our results are consistent with previous studies linking hypertension and smoking to a younger onset and increased severity of white matter lesions in this clinical population [62, 65–68]. We did not observe any relationships between the FCRP score and WMH in our CADASIL cohort, which converges with the results from Singhal et al. (2004) showing an absence of association between cardiovascular risk factors and WMH in CADASIL [67], possibly reflecting the predominantly nonatheromatous etiology of WMH in this clinical population. Because of the low occurrence of MRI markers of cerebral small vessel disease in presymptomatic ADAD subjects and in non-carriers, we could not reliably examine relationships with the FCRP score in these two groups. It is important to note that patients with ADAD differ from those with sporadic forms of AD by their younger age of disease onset and a lesser presence of mixed neuropathology. For instance, patients with sporadic AD are more likely to present markers of cerebrovascular disease, including lacunes and parenchymal arteriosclerosis than patients with ADAD [29]. As such, our current observations and findings may not be generalizable to the more common sporadic late onset AD (LOAD).
When examining associations between the global cardiovascular risk profile and hippocampal or whole-brain volume across all three groups, an association was found between a higher FCRP score and reduced hippocampal volume in presymptomatic subjects with CADASIL. In contrast, there was no significant association between the FCRP and volumetric measures in presymptomatic subjects with ADAD or in non-carriers. This interesting observation suggests that cardiovascular risk factors might affect the structural integrity of medial temporal lobe regions susceptible to AD pathology in subjects with cerebral small vessel disease, pointing to the relevance of vascular contributions to cognitive impairment and dementia. Unexpectedly, we also observed a positive association between age and hippocampal volume in the cohort of presymptomatic subjects with CADASIL. While seemingly counterintuitive, this finding is consistent with results from an earlier study suggesting that extensive white matter hyperintensity may be associated with an increase in brain volume in patients with CADASIL, most likely due to inflammation and a global increase in the water content of brain tissues [69]. It is thus possible that patients with CADASIL show an increase in brain volume until the occurrence of significant neuronal death, axonal loss, or demyelination eventually leading to atrophy and a reduction in brain volume. Future studies should aim to clarify the trajectory of regional and global changes in brain volume in CADASIL, from the asymptomatic to symptomatic disease stages.
When looking at associations with cognitive performance, the FCRP score did not relate to performance across all cognitive domains in both the presymptomatic CADASIL and ADAD group. As such, while a higher FCRP score appears to enhance cerebrovascular lesions in the presymptomatic stages of CADASIL, this effect does not translate into a worsening of cognition, at least in these early disease stages. The observation that a higher cardiovascular risk profile promotes the severity of cerebral small vessel disease in presymptomatic individuals with CADASIL without a deleterious impact on cognition could reveal a window of opportunity for therapeutic interventions aiming at controlling cardiovascular risk factors before the appearance of cognitive decline. In contrast, an association between the FCRP score and executive function performance was noted in non-carriers, which aligns with results from several large-scale studies linking cardiovascular risk factors to executive functioning in cognitively normal middle-age and elderly individuals [70–74]. The differential association between cardiovascular risk and cognition across groups possibly reflect distinct mechanisms underlying cognitive functioning in healthy non-carrier subjects, as opposed to NOTCH3 or PSEN1 mutation carriers. Previous studies have suggested that the deleterious effect of cardiovascular risk factors on cognition might be linked to ensuing structural brain alterations, including gray matter atrophy, white matter lesion, and damage to subcortical white matter microstructure [75]. An alternative mechanism linking cardiovascular risk factors to poorer cognitive performance consists in the disruption of the frontoparietal brain network, a network involved in the regulation of executive function [76]. Finally, another factor possibly contributing to the negative association between cardiovascular risk factors and cognition involves compromised cerebral blood flow, which may in turn promote the progression of cerebral small vessel disease and compromise cognitive performance [77].
The strength of this study lies in the combined characterization of the impact of the global cardiovascular risk burden on early neuroimaging and cognitive features of two rare hereditary disorders leading to the early onset of dementia. However, this study has several limitations. The main limitation consists in the small sample size of our cohorts, a common issue in CADASIL or ADAD research due to the rarity of these conditions. Our small sample size limited the evaluation of other factors potentially modulating disease severity (e.g., APOE ɛ4 status). Because this study only included ADAD and CADASIL individuals at a presymptomatic disease stage, these subjects are young of age and present a low severity and occurrence of cardiovascular risks. A larger cohort presenting more variation in cardiovascular health might allow uncovering additional effects that were not detected in this study. These findings therefore need replication in larger samples. While the validity of the FCRP score is well established for the prediction of subsequent cardiovascular diseases, it does not take into account other health factors potentially relevant to the presence of cerebral small vessel disease and neurodegeneration. Various laboratory measures (e.g., cholesterol or homocysteine levels), medical conditions (e.g., atrial fibrillation), and lifestyle factors (e.g., alcohol consumption, exercise levels) have been associated with cardiovascular health and could contribute, directly or indirectly, to our findings. Finally, our analyses only included structural neuroimaging markers. There is a growing recognition that microscopic white matter lesions, which cannot be adequately visualized on structural MRI, significantly contribute to cognitive impairment and to the risk for cerebrovascular disease. Future studies should aim to evaluate the influence of cardiovascular risk factors on neuroimaging markers that are more sensitive to cerebral small vessel disease or to neurodegenerative pathology, such as diffusion tensor imaging [78] or positron emission tomography. Longitudinal studies are also needed to determine if the cardiovascular risk profile influences the clinical trajectory of these diseases, by enhancing the progression of brain lesions or cognitive decline over time.
To conclude, our findings suggest that the global cardiovascular risk profile contributes to the phenotypic variability of the early stages of CADASIL by promoting the severity of cerebral small vessel disease. This effect seems specific to CADASIL, as we did not observe significant markers of cerebral small vessel disease in presymptomatic ADAD or non-carrier individuals. Patients with CADASIL and vascular forms of cognitive impairment might thus particularly benefit from early interventions aimed at controlling cardiovascular risks.
Footnotes
ACKNOWLEDGMENTS
We warmly thank patients and families who have devoted their time and effort to participate to this project. We also thank Heirangi Torrico-Teave for her help with data retrieval.
This research was supported by grants cofounded by the National Institute of Neurological Disorders and Stroke and the National Institute on Aging (RF1NS110048 (JFAV), UH3NS100121 (JFAV), R01 AG054671 (YTQ)), the NIH Office of the Director (YTQ, DP5OD019833), the CureCADASIL Research Alliance Program (JFAV), COLCIENCIAS (FL), CODI University of Antioquia (FL), the Alzheimer’s Association (YTQ), and the Massachusetts General Hospital ECOR (YTQ, 1200-228010 and 1200-228767). DS received postdoctoral funding from the American Heart Association (20POST35110047) and the Fonds de recherche du Québec - Santé (254389).