
Abstract
Background:
Few studies have investigated the association between cognition and brain volume associated with cerebral small vessel disease (CSVD).
Objective:
We investigated the association between cognition and brain volume and neuroimaging markers of CSVD in a community-dwelling population.
Methods:
Participants (n = 993, age≥35 years) from the community-based Shunyi Study were included to investigate the association between neuroimaging markers and cognition cross-sectionally. Magnetic resonance imaging markers included brain volume measurements of the total cerebrum, white matter, gray matter, and CSVD imaging markers. Cognitive performance was assessed using neuropsychological tests of the Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), Fuld Object Memory, digit span, Trail Making Test (TMT)-A, and TMT-B.
Results:
For brain volume measurement, subcortical white matter fraction was positively associated with MMSE score (β= 0.034, p = 0.0062) and MoCA score (β= 0.034, p = 0.0174), and negatively associated with TMT-A and TMT-B completion time (β= –2.319, p = 0.0002; β= –2.827, p = 0.0073, respectively). For evaluation of CSVD imaging markers, the presence of lacunes was positively associated with TMT-B completion time (β= 17.241, p = 0.0028).
Conclusion:
In community-dwelling populations, reduced white matter volumes, as a consequence of aging and vascular damage, are associated with worse global cognition and executive function. Our findings provide potential insights into the correlation between cognition and CSVD-associated subcortical white matter injury.
Keywords
INTRODUCTION
Cerebral small vessel disease (CSVD) is one of the most prevalent pathological processes that affect cerebral arterioles, perforating arteries, capillaries, and venules, leading to a spectrum of clinical and neuroimaging findings. Typical CSVD lesions detected on brain imaging include white matter hyperintensities (WMHs) of presumed vascular origin, lacunes, cerebral microbleeds (CMBs), perivascular spaces (PVS), cortical superficial siderosis, cerebral microinfarcts, and brain atrophy [1, 2]. The etiologies of CSVD imaging findings vary, and CSVD causes both ischemic and hemorrhagic cerebral vascular disease. CSVD also contributes to various etiologies of cognitive impairment [3]. Strategic lacunar infarcts, particularly those located in the thalamus or putamen, can present with cognitive deficits, which are sudden in onset with cerebral vascular events [4]. Extensive white matter hyperintensity burden is revealed to be a risk factor for dementia, particularly worsening cognitive speed and executive function [5]. The presence of multiple lobar cerebral microbleeds is also associated with worse information processing and executive function [6]. Additionally, CSVD is associated with brain atrophy that contributes to cognitive impairment [7, 8].
Increased age is a shared risk factor for both CSVD and neurodegenerative diseases. Concurrent pathological findings of cerebrovascular disease are common among patients with neurodegenerative dementia, and the presence of cerebrovascular disease doubles the risk of developing dementia [9]. The Rotterdam Study, a prospective, population-based study, showed cognitive decline restricted to individuals with new silent infarcts at follow-up [10]. In addition, the Nun Study demonstrated that participants with Alzheimer’s disease pathological findings were more likely to develop dementia when they had concurrent infarcts [11]. Nevertheless, subcortical white matter is thought to be more vulnerable to CSVD, while cortical thinning is considered a marker of neurodegenerative cognitive impairment [12]. Since some cerebrovascular risk factors are clinically modifiable and their elimination could lower the chance of developing dementia, it is reasonable to investigate the characteristics of CSVD-associated subcortical structural damage and cognitive decline in community populations, which could provide neurologists with new evidence on clinical decision-making in the care of patients with cognitive decline.
CSVD radiological markers are frequently detected in symptom-free individuals. This reminds us of an interesting question regarding the association between incidental detection of CSVD imaging markers and cognition in the general population. Several published population-based studies have shown that radiological markers of CSVD are associated with cognitive impairment in Western countries [6, 14]. However, few studies have investigated the correlation between CSVD and brain volume, particularly the subcortical white matter volume, and their potential association with cognition. Additionally, our previous study showed that there was a heavier burden of lacunes; however, a relatively lower prevalence of cerebral microbleeds in the included Chinese population [15]. The association between neuroimaging findings and cognition in this population remains an intriguing query. In this study, we performed brain imaging and cognitive tests in a community population in a suburban area of Beijing, China. We hypothesized that CSVD imaging markers and concurrent brain volume are associated with cognition.
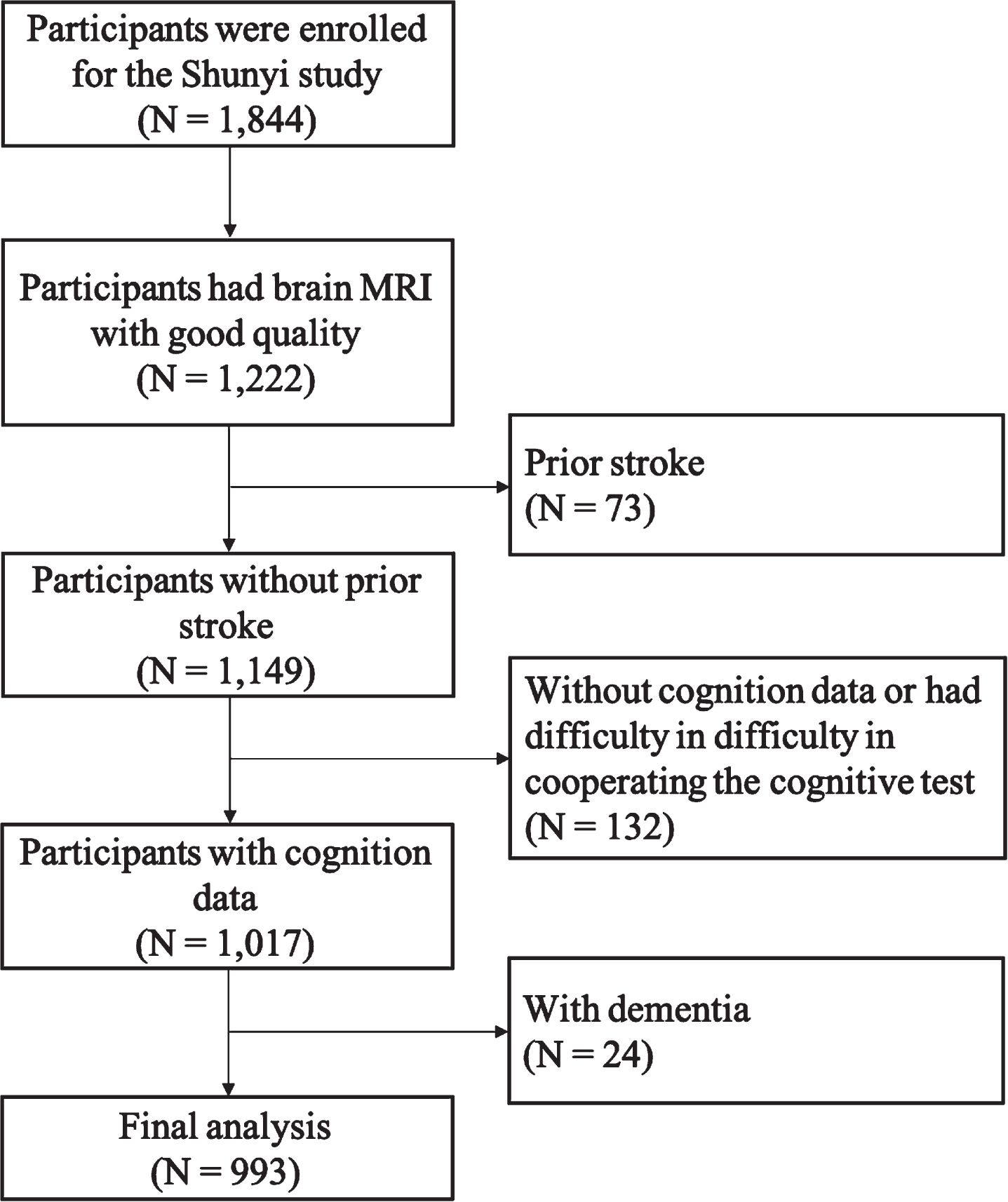
Study flow chart.
METHODS
Participants
The Shunyi Study is an ongoing community-based cohort study conducted in a suburban area near Beijing. From June 2013 to April 2016, all inhabitants aged 35 years or older from five randomly chosen villages of Shunyi were invited to participate in this study, and 1,844 individuals agreed to participate. Baseline assessments for each participant included structured questionnaires, physical examinations, and laboratory tests. Of the 1,323 participants who had a brain magnetic resonance imaging (MRI) scan, 1,222 had good MRI imaging data. Seventy-three participants with prior stroke; 132 without cognitive data or difficulty in cooperating to cognitive test (due to vision, hearing, or joint problems); and 24 with dementia were excluded. Finally, 993 participants were included in the analysis. All participants provided written informed consent. The Ethics Committee at Peking Union Medical College Hospital approved all the study protocols [13].
Brain MRI acquisition and analysis
Brain MRI was performed using a single 3-T Siemens Skyra scanner (Siemens, Erlangen, Germany). Based on published criteria, recognized imaging markers of CSVD were recorded [16].
WMHs are mostly symmetrical hyperintensities on both T2-weighted sequences and fluid-attenuated inversion recovery sequences, and isointensities or faint hypointensities on T1-weighted sequences. The hypointensities on T1-weighted sequences are usually not as hypointense as the cerebrospinal fluid (CSF). Based on the Fazekas score, periventricular white matter hyperintensities (PVWMHs) and deep white matter hyperintensities (DWMHs) were rated separately on FLAIR sequences [17]. Participants with severe total WMHs were defined as those with either PVWMH or DWMH rated more than 2 on the Fazekas score. WMHs were automatically segmented using the lesion growth algorithm as implemented in the LST toolbox (http://www.statistical-modeling.de/lst.html) for SPM at κ= 0.15.
Lacunes were defined as round or ovoid fluid-like signal lesions ranging from 3 mm to 15 mm in diameter located in the basal ganglia or white matter. Lacunes were identified on three-dimensional T1-weighted sequences and reconfirmed on T2-weighted and FLAIR sequences.
CMBs were defined as round or ovoid lesions of signal voids within the brain parenchyma that were detectable on T2*-weighted gradient-recalled echo or susceptibility-weighted imaging (SWI) sequences, and commonly invisible on T1-weighted or T2-weighted sequences [18]. CMBs were identified on SWIs, and the number of CMBs was recorded according to their topographic distribution in the brain [19].
Dilated PVS is defined as CSF-like signal lesions and can be round, ovoid, or linear. The round or ovoid dilated PVSs are generally smaller than the lacunes (smaller than 3 mm). Dilated PVS in the basal ganglia (PVS-BG) and white matter (PVS-WM) were recorded separately. Dilated PVS-WM was scored as follows: degree 1, < 10 PVS in the total white matter volume; degree 2, > 10 PVS in the total white matter volume and < 10 PVS in the slice containing the greatest number of PVSs; degree 3, 10–20 PVS in the slice containing the greatest number of PVSs; and degree 4, > 20 PVS in the slice containing the greatest number of PVSs. Dilated PVS-BG was scored as follows: degree 1, < 5 PVS; degree 2, 5–10 PVS; degree 3, > 10 PVS, but still numerable; and degree 4, innumerable PVS. Severe PVS-WM or PVS-BG was defined as degrees 2 and 3 in the white matter and basal ganglia, respectively.
Three-dimensional T1-weighted images were segmented automatically with computer assistance to generate a probability map of gray matter, white matter, and CSF. The total intracranial volume was defined as the sum of the total gray matter, total white matter, and CSF volume. The brain parenchymal fraction (BPF) was defined as the ratio of brain tissue volume (grey matter and white matter volume) to intracranial volume.
Four well-trained neurologists who were blinded to all clinical data independently rated WMHs, lacunes, CMBs, and PVS. After an interval of longer than 1 month, brain images of 50 randomly selected individuals were read for the second time to assess intra-rater agreement. Kappa values for the intra-rater agreements were 0.84, 0.89, 0.73, 0.90, 0.71, and 0.61 for PVWMHs, DWMHs, lacunes, CMBs, PVS-BG, and PVS-WM, respectively.
Cognitive assessments
The Chinese version of the Mini-Mental State Examination (cMMSE) and the Chinese version of the Montreal Cognitive Assessment (MoCA) adapted from Ziad Nasreddine were used to assess global cognition that evaluate a broad array of cognitive domains [20, 21]. Fuld object memory evaluation (FOM) was used to evaluate episodic memory and learning [22]. The digit span test (forward and backward) was used to evaluate working memory and attention [23]. Trail Making Tests A and B (TMT-A and TMT-B) were used to assess executive function. To achieve high quantitation quality TMT-A/B test results, we used a digital mental state detection system with multiple channels to record the test. Digital mental state detection system (patent NO. CN 103956171 B) is a software system with a built-in digital TMT program deployed on a commercial computer. The computer is connected to a Wacom pen display (Wacom 2016) to present and conduct the test. When conducting the test, the system logs pen tip coordinates with a timestamp; thus, we can calculate TMT-related measurements after the test.
Statistical analyses
Continuous variables are expressed as mean and standard deviation (SD), and categorical variables are expressed as frequencies and proportions. The correlation between CSVD imaging markers or brain volume and cognition was evaluated using general linear model analyses with each CSVD marker (WMH volumes, severity of WMH, presence of lacunes, presence of CMBs, severity of PVS-WM, severity of PVS-BG), or brain volume (BPF, subcortical white matter fraction, cortical gray matter fraction, and hippocampal fraction) as determinants and cognition (MMSE score, MoCA score, FOM score, digit span score, and time to complete TMT-A, TMT-B, and the ratio of TMT-B/TMT-A) as outcome variables. The models were adjusted for age; sex; educational level; and vascular risk factors (hypertension, diabetes mellitus, hyperlipidemia, current smoking, and current drinking status). In the multivariate model, the z-scores of the MMSE, MoCA, FOM, and digit span tests were used. Statistical significance was defined as p < 0.05. Statistical analyses were conducted using SAS version 9.4 (SAS Institute, Inc., Cary, NC, United States).
RESULTS
Demographic and imaging characteristics
Of the 993 participants included in the final analysis, the mean (SD) age was 55.3±9.2. years (range, 35–80 years), and 34.7%were male. A total of 672 (68.2%) participants completed junior school or higher education. The prevalence of cardiovascular risk factors was as follows: current smoking, 22.3%; current drinking, 23.0%; hypertension, 49.3%; diabetes mellitus, 15.5%; and hyperlipidemia, 48.2%. The mean body mass index was 26.7 (6.0) (Table 1).
Baseline characteristics
*709 participants completed both the TMT-A and TMT-B tests. §944 participants completed the FOM test. ‡993 participants. BMI, body mass index; DM, diabetes mellitus; SBP, systolic blood pressure; DBP, diastolic blood pressure; ICV, intracranial volume; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; FOM, Fuld object memory evaluation; TMT, Trail Making Test; CSVD, cerebral small vessel disease; WMH, white matter hyperintensities; PVWMH, periventricular white matter hyperintensities; DWMH, deep white matter hyperintensities; CMBs, cerebral microbleeds; PVS, perivascular space; WM, white matter; GM, gray matter; BG, basal ganglia; BPF, brain parenchymal fraction.
Severe WMH was observed in 182 (18.3%) brain images of the participants. Lacunes, CMBs, severe PVS-BG, and severe PVS-WM were found in 137 (13.8%), 94 (9.5%), 137 (13.8%), and 147 (14.8%) participants, respectively. The mean MMSE and MoCA scores were 26.6 (SD 3.1) and 19.3 (SD 4.8), respectively. The mean FOM score was 15.1 (SD 2.5). The mean score of the digit span was 9.8 (SD 3.2). The mean TMT-A completion time was 69.5 (SD 41.9) s, and the mean TMT-B completion time was 105 (SD 63.4) s (Table 1).
Associations between imaging markers of CSVD and cognition
After adjustment for age, sex, cardiovascular risk factors, education level, and apolipoprotein E ɛ4 status, the presence of lacunes increased TMT-B completion time (β= 17.241, p = 0.0028). WMH, CMBs, and PVS were not found to be associated with cognition (Table 2).
Correlation between CSVD imaging markers and cognition
Adjusted by age, sex, educational level, vascular risk factors, and APOE ɛ4 status. §944 participants completed the FOM test. ‡Digit span test of 993 participants. *709 participants completed both the TMT-A and TMT-B tests. *Uncorrected p < 0.05. **Surviving a false discovery rate (FDR)-corrected threshold of p(FDR) = 0.05. WMH, white matter hyperintensities; PVWMH, periventricular white matter hyperintensities; DWMH, deep white matter hyperintensities; CMBs, cerebral microbleeds; PVS, perivascular space; WM, white matter; BG, basal ganglia; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; FOM, Fuld Object Memory Evaluation; TMT, Trail Making Test.
Associations between brain volumes and cognition
For brain volume, subcortical white matter fraction was positively associated with MMSE score (β= 0.034, p = 0.0062) and MoCA score (β= 0.034, p = 0.0174), and negatively associated with TMT-A completion time (β= –2.319, p = 0.0002) and TMT-B completion time (β= –2.827, p = 0.0073) (Table 3). In subgroup aged < 55 years, subcortical white matter fraction was associated with MMSE score (β= 0.043, p = 0.0089) and MoCA score (β= 0.067, p = 0.0048), and negatively associated with TMT-A completion time (β= –1.994, p = 0.0060) and TMT-B completion time (β= –3.739, p = 0.0017) (Supplementary Table 1). In subgroup aged≥55 years, subcortical white matter fraction was associated with MMSE score (β= 0.036, p = 0.0446) and MoCA score (β= 0.036, p = 0.0494), and negatively associated with TMT-A completion time (β= –3.054, p = 0.0032) (Supplementary Table 2). Neither whole cortical GM volumes nor GM volumes of any lobe were found to be associated with cognition (Table 3).
Correlation between brain volumes and cognition
Adjusted by age, sex, educational level, vascular risk factors, and APOE ɛ4 status. §944 participants completed the FOM test ‡ Digit span test of 993 participants. *709 participants completed both the TMT-A and TMT-B tests. *Uncorrected p < 0.05. **Surviving a false discovery rate (FDR)-corrected threshold of p(FDR) = 0.05. BPF, brain parenchymal fraction; WM, white matter; GM, gray matter; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; FOM, Fuld Object Memory Evaluation; TMT, Trail Making Test.
Additionally, WMH volume (β= –0.300, p < 0.0001), severe WMH (β= –0.512, p = 0.0007), presence of lacunes (β= –0.865, p < 0.0001), and higher burden of CMBs (1-2 CMBs: β= ––0.577, p = 0.0054;≥3 CMBs: β= –1.280, p = 0.0007) were negatively associated with white matter volume (Supplementary Table 3).
DISCUSSION
In this community-based study, we focused on the potential association between asymptomatic CSVD imaging markers and cognition. We found that reduced subcortical white matter fraction was the major factor contributing to worse global cognition. Further analysis of the specific cognitive domain tests showed that reduced subcortical white matter fraction was predominantly associated with poor performance in executive function tests, and the presence of lacunes was also linked to worse executive function. Our findings provide new insights into the potential correlation between cognition and CSVD-associated subcortical white matter damage.
Compared with vascular dementia, Alzheimer’s disease has attracted more attention, and cognitive impairment is more closely linked to neuronal loss and cortical degeneration. Brain volume loss, particularly hippocampal volume loss and entorhinal and medial temporal cortical thinning, have been regarded as brain imaging markers of neurodegenerative dementia [12]. However, white matter occupied roughly half of the brain volume, and the association between white matter volume and cognition has received relatively little attention. In contrast to previous population-based CSVD studies [24, 25], the mean age of the population in the current study was younger, and the burden of CSVD imaging markers was lower [15]. In addition to CSVD imaging markers, we found that brain volumes, particularly white matter volumes, were positively associated with global cognition. White matter volumes were predominantly associated with executive function but had no obvious effect on memory. In the younger subpopulation which did not exhibit severe CSVD burden, reduced white matter volume was also significantly associated with worse executive function. Executive function has been significantly associated with WMH in previous studies [26]. In this study, WMH had already shown a tendency to worsen executive function. Previous evidence has shown that hypertension is associated with reduced brain volume and increased WMH volume [27], and the WMH was considered as the imaging appearance of axonal loss and demyelination, which was supposed to be predominantly caused by CSVD [28]. Our previous data showed that a higher burden of CMBs was associated with reduced white matter volume [29]. In the population included in this study, we also found that CSVD markers, including WMH, lacunes, and CMBs, were associated with reduced white matter volume. Thus, the reduced white matter volume was supposed to be an imaging finding indicating the underlying cerebral vascular pathological changes, reflecting the combined effects of ischemic and hemorrhagic CSVD imaging markers, and the conjugated consequence of the aging process and vascular damage. In addition, even in relatively young population which were not showing severe burden of traditional CSVD imaging markers, the reduced white matter volume could be a sensitive CSVD-related imaging marker that associated with cognition. However, the correlation between white matter volume and CSVD requires long-term follow-up for further investigation. In our previous published study on the prevalence of CSVD markers, we noticed that the prevalence of CSVD markers is different between the population in this study and populations in other studies [15]. The probable reason is the higher prevalence of hypertension and lower control rate in this population. In addition, a previous study showed that confluent WMHs were more common in non-white populations, including Asians [30].
Strategic lacunar infarcts, particularly those located in the deep gray nuclei, can lead to a stepwise deterioration of cognition [4]. However, the lacunes occasionally detected in this community population were symptom-free; therefore, it was reasonable to assume that these lacunes were located in non-strategic regions. The presence of silent lacunes increased the TMT-B completion time, however, did not increase the TMT-B/A ratio. Compared with the TMT-A test, the TMT-B test required more cognitive control related to psychomotor speed [31]. In addition, an abnormally high TMT-B/A ratio might be due to motor control rather than true cognitive dysfunction [32]. Collectively, the increase in the completion time of the TMT-B test and the normal TMT-B/A ratio indicated that participants with silent lacunes had slower psychomotor speed, which was also consistent with the findings of the Rotterdam study [10, 13]. Previous studies have shown that the presence of CMBs is associated with cognitive impairment in elderly people [6, 34]. However, the presence of CMBs did not affect cognition in this population. This might be owing to the mean age of this population was younger, and the prevalence of CMBs was lower than that in other studies. The results of previous studies on the correlation between PVS and cognitive impairment are ambiguous [33]. In this study, the presence of PVS was not independently associated with cognition. Nevertheless, long-term follow-up is required to investigate the correlation between the burden or new occurrence of CSVD imaging markers and the lifetime prevalence of dementia.
This study provided community population data to investigate the association between cognition and CSVD imaging markers and brain volumes. The results showed that white matter volume that received relatively less attention in neurodegenerative dementia research might be a new insight for studying CSVD-associated cognitive impairment. However, this study was a cross-sectional study that collected the baseline data of this population. At this time point, the participants were clinically asymptomatic. To further study the potential correlation between cognitive impairment and CSVD-associated neuroimaging findings, long-term follow-up will be conducted in this population. This study was based on a suburban community population. Compared with comprehensive cognitive assessments in specialized memory clinics, participants simply received MMSE and MoCA as global cognitive function tests and few specific cognitive domain tests that merely included memory, executive function, and attention. Although results have already shown that white matter volume is related to executive function but not memory, more comprehensive cognitive assessments should be completed for further investigation in future long-term follow-up.
CONCLUSION
This study demonstrated that reduced white matter volumes were associated with worse performance in global cognitive tests. Further specific cognitive domain tests showed that reduced white matter volumes and the presence of lacunes were associated with worse executive function and psychomotor speed. These findings provide new insights into the significance of white matter volumes in cognition. Long-term follow-up is required to investigate the correlation between cognitive decline and age-related reduction in white matter volume and to further determine the role of CSVD in the shrinkage of white matter.
Footnotes
ACKNOWLEDGMENTS
This study was supported by the National Natural Science Foundation of China (No. 81901224, 81971138), the Strategic Priority Research Program “Biological basis of aging and therapeutic strategies” of the Chinese Academy of Sciences (No. XDB39040300), and the project of China Foundation for International Medical Exchange “Innovative thinking research funding” (No. CIMF-Z-2016-20-1801).