
Abstract
Background:
Increasing physical activity (PA) in those who have memory concerns requires innovative approaches.
Objective:
To compare in this randomized controlled trial (RCT) the effects on PA, adherence, and fitness of two approaches to deliver a 6-month home-based PA program in older, inactive individuals at risk of cognitive decline.
Methods:
Individuals (n = 52) aged 60–85 years, inactive with mild cognitive impairment or subjective cognitive decline were recruited from the community and memory clinics. Randomization was to 6 months of 150 min/week moderate intensity PA with either: goal-setting with mentor support; or education and peer contact. A subset of participants (n = 36) continued for a further 6 months. PA, moderate and vigorous PA, and secondary outcomes, fitness, goal performance/satisfaction and self-efficacy were assessed at baseline, 6 and 12 months. Modelling of primary and secondary outcomes was conducted with linear mixed models.
Results:
Participants were mean age (±sd) 70.1 (6.4) years. Six-month retention was 88.5%(n = 46). No significant between-group differences were observed for PA or fitness. Post-hoc combined group data showed a significant, moderate-large effect size increase in PA with time. PA increased by a mean 1,662 (943, 2383) steps/day (95%CI) and 1,320 (603, 2037) steps/day at 6 and 12 months (p < 0.001). Median (quartiles Q1-Q3) 6 and 6–12 month combined group adherence was 88.9 (74.4–95.7)%and 84.6 (73.9–95.4)%respectively.
Conclusion:
In this target group, no differences were detected between groups both intervention strategies were highly effective in increasing PA and fitness.
INTRODUCTION
Even though the benefits of regular physical activity (PA) are well known and supported by a growing body of evidence that PA is beneficial for cognitive health [1], finding effective strategies to increase the adoption and maintenance of PA for older and inactive individuals is an ongoing significant challenge. Much more complex challenges are present when older people have difficulties with memory loss or declining cognitive function that may limit understanding of instructions and execution of tasks, [2, 3] as well as motivation and capacity to change behavior, while often experiencing decline in physical function such as poor fitness, strength, and balance [4, 5]. In our previous work we have been successful in achieving excellent adherence to home-based PA over 6 months [6, 7] and 24 months [8] for older adults with mild cognitive impairment (MCI) or subjective cognitive decline (SCD) at increased risk of Alzheimer’s disease (AD). However, these studies included participants who were already undertaking regular moderate intensity PA. In the current study, we explore whether a modified PA program can lead to the uptake and the adoption of PA in physically inactive individuals in this target group.
Goal-setting is an effective strategy to increase PA in older adults [9, 10]. Personalized goal-setting was rated as a highly positive intervention strategy by participants who were successful in improving their PA profile [11]. The efficacy of an individual goal-oriented approach to behavior change has been demonstrated in community living older adults and in those with mild dementia, with improved goal performance and satisfaction, increased physical and cognitive activity, feasibility, and acceptability by older adults [12–14]. Further, individual goal-oriented cognitive rehabilitation (CR) improved everyday functioning in relation to individual goals targeted in the therapy for people with mild-to-moderate dementia [14]. When mentoring was added to this goal orientation approach there were further benefits in PA, global cognition, memory, and body composition compared to goal-setting alone [13]. Mentorship motivated people to work on goals and was well received [15].
Peer mentoring in older adults is as effective in achieving retention, participation, and increases in fitness as a similar program delivered by young professionals [16]. When peer mentors are volunteers this approach has the potential to be a cost-effective delivery model to increase PA among older adults [16]. Significantly greater long-term increases in moderate and vigorous PA were achieved with peer-delivered PA compared to community delivered PA programs [17]. In a systematic review of 10 studies on peer-delivered interventions the authors concluded that compared to other programs peer delivery was just as effective as professional delivery and more effective than control programs in increasing PA [18].
Combining the strategies of an individual goal-oriented approach developed by Clare and colleagues [12, 14], modified to target PA and physical function (PF) goals, with support from physically active peers to promote increased PA in inactive older adults at risk of cognitive decline is a novel approach. To our knowledge, this is the first study to utilize peer mentoring to promote PA in this target group. The primary aim of this randomized controlled trial (RCT) was to determine if a 6-month home-based PA intervention with individual goal-setting and peer mentors (intervention group) would result in a significantly greater increase in PA compared to the same PA program delivered with standard education and peer contact only (control group) after 6 (short-term) and 12 months (long-term). The long-term effects of this intervention were assessed from a sub-group of participants after 12 months. Secondary aims included evaluation of functional fitness, goal performance, goal satisfaction and program factors at 6 and 12 months. Further, to explore the factors that influence the change in the primary and secondary outcomes.
METHODS
Study design
The protocol for this parallel group single-blind RCT based on CONSORT guidelines (Fig. 1) has been previously published [19]. The study was registered with the Australia New Zealand Clinical Trials Registry registration number ACTRN12613001181796. The trial had two components: mentoring/peer contact training and implementation, and a PA intervention. The main outcomes of the intervention were the change in PA and adherence to the PA program for participants in the PA intervention. Secondary outcomes included functional fitness components, goal performance, goal satisfaction, self-efficacy, and program evaluation. The original protocol was for a 6-month PA intervention with a further 6-months follow-up. Due to recruitment challenges and funding restrictions, the protocol was amended with the trial period limited to 6 months after the first 36 participants. Another 16 participants were recruited for the 6-month intervention period only (the 6-month cohort). Hence a total of 52, participated in the 6-month intervention with a subset (n = 36) following the original protocol with a further 6-month follow-up (the 12-month cohort). These participants were asked to continue with their PA program during the 6–12-month period recording sessions in their PA diaries but without any of the support given in the first 6 months such as workshops or phone calls. Table 1 outlines the components of the intervention and control group programs and highlights the similarities and differences. The methods relevant to this paper are described briefly below.

INDIGO study participant flow from recruitment to the end of the 12-month follow-up.
A comparison of the similarities and differences between the program components of the two study groups in the INDIGO study conducted in Melbourne, Australia
CHAMPS Q, Community Healthy Activities Model Program for Seniors Questionnaire; MI, Motivational Interviewing; BGSI, Bangor Goal-Setting Interview.
Participants
Participants were independent-living older adults aged 60–85 years with memory concerns (without diagnosed dementia) and inactive (doing < 60 min of moderate or vigorous intensity leisure activity a week) [20] with total minutes calculated from screening questions that asked about PA type, duration, frequency and intensity. Screening was completed via telephone and also included: the Telephone Interview for Cognitive Status–Modified (TICS-M) [21], Geriatric Depression Scale 15 (GDS-15) [22], and Revised Physical Activity Readiness Questionnaire (PAR-Q) [23]. Participants were included if they answered “Yes” to the question “Do you have any difficulty with your memory?” They were considered to have subjective cognitive decline (SCD) if they scored in the range of normal control group scores for their age and sex on the Cognitive Battery of the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) [24]. In addition to a “Yes” response to the above question participants who scored below the normal range on the cognitive measure (CERAD) were defined as having MCI.
Exclusion criteria were: scoring less than 19 out of 50 on the TICS-M [21]; more than 5 on the GDS-15; diagnosis of dementia; a Mini-Mental State Examination score (MMSE) < 24 [25]; unstable or life-threatening medical condition; medical condition contra-indicating moderate PA; body mass index (BMI)>37; severe visual or hearing impairment; history of chronic alcohol abuse within the past five years; not fluent in English and inability to attend follow-up visits. Classification of dementia reflected a score of < 24 on the SMMSE or a TICS-M score of < 19. Classification was overseen by a diagnostic group led by a psychiatrist that considered functioning in addition to cognition. The participant’s primary care doctor was asked to approve participation.
Participants were recruited from the Melbourne metropolitan area via web sites and newsletters, memory clinics, seniors groups, and the media. The participants gave informed written consent to participate, and the Melbourne Health Human Research Ethics Committee approved the trial. The study took place at the National Ageing Research Institute, Parkville, Australia.
The physical activity intervention
Both groups received the same program of 150 min of moderate intensity PA per week completed as 3×50-min sessions or 5×30-min sessions to allow for preference and flexibility to fit in with the participant’s routine. The program was progressive, taking up to 8 weeks to reach the full duration of the sessions and moderate intensity (55–65%heart rate reserve). Intensity was monitored using the Borg Perceived Rate of Exertion scale (RPE 10–12) [26]. All participants were given a manual containing the same information about progressive walking, water walking, swimming, and cycling programs and exercise safety. The manual also included an individualized PA program with standardized diaries to record their PA. Diaries were returned monthly by prepaid post. The program was home-based and unsupervised with monitoring via the phone calls and diaries. Details of the program and demonstration of the PA including the frequency, intensity and recording details of the PA in the diaries was outlined in the first face to face workshop session by the same PA facilitator. The manual for the intervention group also included information on the goal setting. The control group were given copies of the workshop slide presentations on the standard education topics.
Goal-orientated PA and mentoring intervention group
The objective of the goal-oriented PA program was to enhance PA self-efficacy and increase PA. The Bangor Goal-Setting Interview (BGSI) [27] modified for use in INDIGO to focus specifically on PA was employed for individual goal identification and goal setting. The interview conducted by the same experienced PA facilitator focused on the 5 individual goals from the PA and PF areas identified in the baseline BGSI. Participants selected 3 personal goals to operationalize and work on during the intervention period. The intervention group’s resource manual also included information on setting SMART goals, the development of strategies to achieve behavior change, practical aids, and action plans to facilitate goal performance.
Intervention group workshops
The program content was delivered over the first 6 months via 3 face-to-face workshops conducted by the PA facilitator and supported by the mentoring program.
The first workshop also attended by mentors was for 2 h, with the content of the first hour outlining the PA program, and a demonstration walk session. In the second hour, the intervention group focused on identifying and prioritizing more specific PA goals, operationalizing goals, and strategies for goal performance. The 2 remaining 1-h workshops were conducted at 8-weekly intervals. Topics included setting SMART goals; evaluating progress; feedback; getting the most out of the mentoring process; identifying barriers to goal performance; developing practical aids to overcome specific barriers; reassessment of goals; identification of effective and ineffective strategies and review of the action plan. These topics were followed up during the mentor calls in between the workshop sessions.
Mentor telephone contact protocol
Each intervention group participant received 6 calls from their mentor at 4-weekly intervals starting at week 2, then weeks 6, 10, 14, 18, and 22 over the 6-month period. Participants were asked about their PA program progress and prompted to complete and return their PA diaries. Mentors used a semi-structured script and employed the techniques of reflective listening and spontaneous discussion to engage participants in working on their relevant goals, gave feedback, and discussed strategies to on how to keep on track. They recorded the number and time spent on calls.
Control group
Standard Education Program Workshops
The control group received a standard education program conducted over 3 workshops scheduled at the same intervals but on separate occasions to the intervention group. The first workshop was for 2 h, also attended by the peer volunteers (PALS), with the content of the first hour outlining the PA program and a demonstration walk session. In the second hour the research staff gave a generic presentation on ‘Healthy Ageing’. The other 2 workshop sessions were conducted as direct information giving sessions with no motivational content for PA and included topics such ’stress and depression’ or ‘enjoying retirement’.
PAL telephone contact protocol
Participants received 6 scripted telephone calls from their peer volunteer (PAL) with the same scheduling as the intervention group. PALS recorded number of calls, asked direct questions about PA progress, and prompted return of the PA diaries but did not give any feedback or motivational advice.
The peer volunteer program
Thirty-two physically active (meeting the PA guidelines of at least 150 min/week of moderate intensity PA [28]) adults aged 50–85 years were recruited from the community via volunteer support groups for seniors and the media in the Melbourne Metropolitan area. Assessments of PA and PA mentoring self-efficacy were completed at baseline, 6 and 12 months after each peer support period [19]. Post baseline peer volunteers were randomly allocated to be trained as either mentors or Physical Activity Liaisons (PALS).
Mentors attended an 8-h face to face training course developed for the trial that focused specifically on the content of the participant intervention program and skills training for the development a motivational interviewing style of counseling. The PALS attended a 3-h face to face training course on the content of the control program only and how to deliver the standard telephone contact to the control group without engaging the participants in any ‘motivational talk’.
Over the period of the trial mentors and PALS were assigned to their respective intervention/control participants via a systematic approach of sequenced lists of mentors/PALS and participants. Both mentors and PALS were assigned to a research team member as a ‘senior mentor’ who provided support via scheduled phone calls during the intervention.
Baseline assessments
Following provision of written consent, baseline assessment covered health (height, weight, BMI), a demographic health and lifestyle questionnaire (illness, injury, falls, medications), PA and fitness, a cognitive and clinical test battery, and a saliva sample for apolipoprotein E epsilon 4 (APOE) genotyping [19]. A goal-setting interview (the BGSI); [27] was conducted.
Physical activity assessment
Physical activity measurement
Pedometers (Yamax CW-700/701 Digi-walker, Yamax Co., Japan) were worn by participants for 7 days to measure their PA. They recorded their daily steps and hours sitting in a diary. Any time during the waking hours that the pedometer was not worn was noted by the participant in a daily diary with the type of activity, time spent in and the intensity of any non-step activity (e.g., water-based activity) recorded. A step count for this activity was estimated based on 100 steps/minute for low moderate intensity (3 MET) and 200 steps/minute for moderate intensity activity, e.g., swimming [29].
Physical activity questionnaires
The CHAMPS PA questionnaire recorded the frequency and duration of activities, with the caloric expenditure (kcals), and minutes per week spent in all, low, moderate, hard, and very hard intensity PA calculated [30]. Moderate and vigorous PA (MVPA) from the CHAMPS questionnaire was determined as the sum of the moderate, hard, and very hard PA.
Self-efficacy questionnaires
PA self-efficacy under adverse events (SEQ) was assessed on a 5-item questionnaire using a 5-point Likert scale [31]. Participant’s rating on a scale of 0–100%of their confidence to complete a specific PA task (150 min/week of moderate intensity PA) was defined as program specific self-efficacy [32].
Fitness assessment
Components of functional fitness were assessed using the following tests [19, 33]: Cardiovascular Fitness: the 6-minute Walk Test [34]; Lower Leg Strength: the Sit-to-Stand Test [35]; Mobility and Agility: the Timed Up and Go Test (TUG) [36]; Dynamic Balance Step Test: stepping one foot at a time on and off a 7.5 cm high step as many times as possible in 15 s [37]; Grip strength: measured with a Smedleys hand dynamometer on the dominant and non-dominant hand [38].
PA adherence
Adherence to the prescribed PA was determined from the return of self-reported PA diaries that recorded the type, frequency, duration, and intensity of the PA. Adherence to the prescribed study PA program was defined as the number of minutes of moderate intensity PA completed relative to the prescribed 150 min/week expressed as a percentage (ADH). Adherence to the prescribed PA and any additional moderate intensity PA that the participants were already doing at baseline was defined as total adherence (TotADH). This variable was included to determine if the prescribed PA replaced previous habitual PA.
Retention
Retention rate was determined as the number of participants assessed at 6 and12 months, expressed as a percentage of the number of participants randomized.
Goal performance and goal satisfaction scores
The modified BGSI was also used as an outcome measure of goal performance and goal satisfaction. In a face to face interview all participants discussed the areas of physical health (PH), PA, PF, and every-day function (EDF) identifying issues to form the basis of goals. They identified 3–5 goals in the area of PF (e.g., strength, agility, fitness, etc.) and/or PA (type, frequency, duration, etc.) and rated their current performance and satisfaction for each goal on a scale of 1–10 (1 = not able to do it/not satisfied at all and 10 = able to do it extremely well/extremely satisfied). A mean score for goal performance was calculated from the sum of the individual goal ratings divided by number of goals set. The mean goal satisfaction score was determined in the same way.
Only the intervention group operationalized their goals and continued to work on these during the intervention.
Importance and readiness to change behavior scores
Self-rating on a scale of 1–10 of the importance and readiness to change behavior in the PF and PA areas was determined at baseline only.
Cognitive and psychological assessment
A battery of cognitive, psychometric, and neuropsychological tests was administered at baseline, 6 and 12 months by an observer blinded to the participant’s group allocation [19]. The Mini-Mental State Examination (SMMSE), a measure of global cognition [25] and the Alzheimer’s Disease Assessment Scale 13–cognitive section (ADAS-cog 13) [39] were used in the modelling in this report to determine if baseline cognitive status influenced the PA results.
Follow-up assessments
All baseline measures were re-assessed at 6 and 12 months except for the APOE4 genotyping for those recruited for 12 months. For those recruited for 6 months only, assessments were at baseline and 6 months.
Program and process evaluation
After 6 and 12 months, participants completed a questionnaire specific to this study to provide feedback on the program. Items were structured so that they answered “yes” or “no” for more general questions and then rated the item on a scale 1–5 with 1 being the least favorable and 5 the most favorable score. Questions asked about enjoyment (e.g., “How enjoyable did you find the PA program?”), understanding (e.g., “Did you find it easy to follow the program we set out for you?”), and helpfulness (e.g., “How helpful did you find. . . ?”). Similarly, specific program components and resources such as the PA program, the information manual, the goal-setting activities, workshops, mentor/PAL phone calls, perceived “knowledge”, “understanding”, and “motivation” shown by mentor/PALS was evaluated. The latter 3 attributes were summed then expressed as a percentage for a mentor/PALS total attributes score.
Workshop adherence and fidelity of the peer volunteer support
Total number of attendances at 3 participant workshops was recorded with workshop adherence calculated as a percentage of workshops attended to workshops scheduled.
Peer volunteer support and fidelity of the phone calls was derived from the total number of successful calls (as defined and recorded by the peer volunteer) the total time of the call and the mean call time. Call compliance was defined as the percent of successful calls made compared to the number of scheduled calls.
Sample size
We estimated that to detect a mean difference of 1,200 steps/day between the groups at 80%power, α= 0.05, 76 participants were needed for each group [19].
Randomization and blinding of observers
On completion of the baseline assessments participants were randomized to either a goal oriented and mentoring PA intervention group or control group according to a list of computer-generated random numbers in varying block sizes using the “ralloc” user-written command implemented in Stata 12 statistical software [40] performed by an investigator not involved in the data collection. Randomization was concealed in envelopes and an independent person completed the allocation of participants to the intervention or control group. This was a single blind study where researchers responsible for the cognitive and clinical assessments were blinded to the treatment allocation.
Statistical analysis
Data were summarized using mean and standard deviation (sd), median and first to third quartiles (Q1, Q3), or counts and proportions as appropriate. Pedometer scores; self-reported PA (all and MVPA); adherence; cardiovascular fitness, balance, mobility (TUG), leg strength, grip strength; goal performance and satisfaction; and self-efficacy were modelled using linear mixed models. All models tested the time by group interaction to determine whether the change over time differed between the two groups. Post hoc, pedometer scores and MVPA analyses assessed potential confounders including (baseline age, sex, APOE4 status, body composition, fitness components, cognition, importance and readiness to change PA, mean total goal performance and satisfaction, self-efficacy, self-efficacy for a walking program, self-efficacy to complete 150 min/week PA, and 6-months total and mean call time, enjoyment of the PA and phone calls) and the method of backward elimination was used to arrive at an adjusted model. Post hoc marginal linear prediction contrasts are provided for changes over time where no group differences were detected. For fitness measures, only age and sex were assessed as potential confounders
Baseline characteristics of the two study duration cohorts were compared and a sensitivity analysis where models were refitted with just the 12-month study cohort were conducted to ensure that conclusions are consistent.
Given the exploratory nature of this trial, multiple adjustments have not been carried out. However, we acknowledge that a considerable number of hypothesis tests have been conducted and as such, caution should be exercised when interpreting significant (and non-significant) results. Statistical modelling was performed using Stata v.15 (StataCorp LLC, College Station, Texas) and statistical significance was set at a p-value < 0.05.
RESULTS
The participant flow through the study is shown in Fig. 1. A total of 52 participants was assessed at baseline and randomized into the two study groups. The number of participants was lower than planned and extension of the recruitment period was limited due to funding restrictions. Thirty-six participants were followed for 12 months. A further 16 were recruited with follow-up truncated at 6 months. Participants who withdrew during the trial were invited to return for the follow-up assessments to allow for an intention-to-treat analysis.
Baseline characteristics
Participants’ baseline characteristics are reported in Table 2A. Mean age (±sd) was 70.1 (6.4) years with 33 (63.5%) of participants being female. The baseline characteristics of the participants recruited for 6 and those recruited for 12 months are shown in Table 2B.
Baseline demographic, health, and PA characteristics of participants in the two study groups in the INDIGO study conducted in Melbourne, Australia
Values are mean and (sd), unless described otherwise. SMMSE denotes Standardized Mini-Mental State Examination score. ‘Low active’ is the number of participants completing less than 150 minutes moderate or vigorous PA (MVPA) /week on the CHAMPS score. Overweight/Obese is defined as BMI > 25.
Baseline characteristics of participants in the cohorts recruited for 6 and 12 months for the INDIGO study conducted in Melbourne, Australia
Values are mean and (sd), unless described otherwise. SMMSE, Standardized Mini-Mental State Examination score; ADAS-cog 13, Alzheimer’s Disease Assessment Scale 13–cognitive; MVPA, moderate and vigorous intensity PA.
Mentor and PAL characteristics
Thirty-two peer volunteers were recruited and trained with 7 (21.9%) withdrawing after randomization but before assignment to a participant, 20 (80%) completed 6 months of support and 19 (76%) completed 12 months. Mean age (±sd) (n = 25) was 65.8 (6.25) years, 15 (60%) were female. Both the mentors and PALS had excellent and similar telephone call-adherence 81.9 (70.4, 93.5)%and 87.2 (77.2, 97.1)%respectively. By design the total call time was higher for the mentors 107 (86.6, 127) minutes compared to PALS 56.7 (45.1, 62.3) minutes (p < 0.001).
Retention of participants
Two participants from the intervention group withdrew before the start of the intervention. A further 2 withdrew from the intervention during the first 6 months but returned for assessments. After 6 months the overall retention (return for assessment) was 88.5%(n = 46) with no significant difference detected between the intervention and control group 84.6%(n = 22) versus 92.3%(n = 24) respectively. For the participants who were in the sub-group for 12 months and were assessed at 12 months (n = 30) retention was 83.3%with no observed significant between group difference in long-term retention 77.8%(n = 14) versus 88.9%(n = 16) for the intervention and control group respectively Fig. 1. However, although returning for follow-up 2 participants in the intervention group discontinued the PA intervention during the first 6 months and another discontinued PA during the second 6 months resulting in a total of 3 discontinuing the intervention over 12 months. The main reasons for not continuing with the intervention or participation in the study (n = 9) over 12 months were “health” (n = 5) (55.6%) and “no longer interested” (22.2%).
In the sub-group who were enrolled for 12 months, 9 (17.3%) withdrew from the study completely or withdrew from the PA intervention resulting in a long-term participation rate of (n = 16) 88.9%in the control group compared to (n = 11) 61.1%in the intervention group (p = 0.054).
Physical activity
Pedometer scores
The pedometer scores of steps/day for both groups at baseline, 6 and 12 months are shown in Table 3. There was no significant difference detected between the control and intervention groups in the pattern of change in steps/day over time (p = 0.129).
PA levels at baseline, 6 and 12 months for the two groups in the INDIGO study conducted in Melbourne, Australia
MVPA, moderate and vigorous intensity PA. Values are raw scores of mean and (±sd) or median scores and (Q1-Q3) where noted. The p value is from the univariable model and reflects the Time×Group interaction p value that tests for a difference over time for the two groups.
In the secondary analysis there was a significant increase in mean steps/day (95%CI) for both groups over time at 6 months 1,662 (943, 2,383) steps/day (p < 0.001) and 1,320 (603, 2,037) steps/day (p < 0.001) at 12 months. When baseline BMI and fitness (walk distance) were included in a multivariable model, both were associated with a significant change in steps/day over time (Fig. 2A). On average, 1 meter more of baseline walk distance on the 6-minute walk test was associated with an increase of 14.6 (3.4, 25.7) steps/day (p = 0.010). Conversely, 1 unit increase in baseline BMI was associated with a decrease of 228.7 (41.1, 416) steps/day (p = 0.017). The model explains 34.4%of the variability in steps/day. The effect size for the total group, Cohen’s f2, of 0.31 for time (the intervention) was medium to large. No associations with potential confounders such as age, sex, cognitive status, self-efficacy, study-time, or APOE4 status were detected. Figure 2a shows the relationship of time and steps/day adjusted for baseline BMI and walk distance for the whole group.

Predictions of steps per day for all participants over time adjusted for baseline BMI and fitness (walk distance) with 95%CIs.
Self-reported physical activity
The raw scores for minutes/week of time spent on all PA and MVPA for the study period are shown in Table 3. For time spent on all PA no significant difference in change over time was detected between the 2 groups (p = 0.082). During the second 6 months of the study the control group continued to increase PA whereas the intervention group had a decline in the rate of change of PA. No significant difference was detected between the 2 groups (p = 0.051).
For both groups combined, however, total time spent in all PA increased significantly on average 220.2 (117.4, 323.1) (p = 0.001) min/week at 6 months and 274.5 (164.9, 383.9) (p < 0.001) min/week at 12 months.
Similarly, for MVPA, no significant difference in change over time was detected between the 2 groups (p = 0.082). A sensitivity analysis to assess the impact of the study-time, as for steps/day, found conclusions to remain the same (p = 0.100).
The MVPA in the secondary analysis increased from baseline over time in both groups (p < 0.001) with the approximated mean increase of 165 (125, 210) min/week and 160 (102, 229) min/week at 6 and 12 months, respectively, from the univariate model. In a multivariable model, younger age at baseline was associated with the increase in MVPA over time (p = 0.002) as were higher baseline cognition (SMMSE) (p = 0.002), and higher baseline goal performance (p = 0.002). When the total time of the PALS/Mentors calls and the enjoyment rating of the PA program over the first 6 months were entered into the model, there was evidence that the relationship of call time to MVPA varied over time. Relative to 12 months, the call time had a stronger positive effect on MVPA at 6 months (p = 0.021) demonstrating that higher total call time in the first 6 months resulted in more MVPA undertaken in the intervention 6 months. Further, the relationship of the enjoyment of the PA program with MVPA varied over time with the enjoyment at 6 months having a stronger positive relationship with MVPA at 12 months (p = 0.033). That is, the more people enjoyed the PA program during the first 6 months the more MVPA they did in the second 6 months. Figure 2b depicts the relationship of time and MVPA adjusted for baseline age, SMMSE, goal performance score, 6 months call time and enjoyment rating for the whole group.
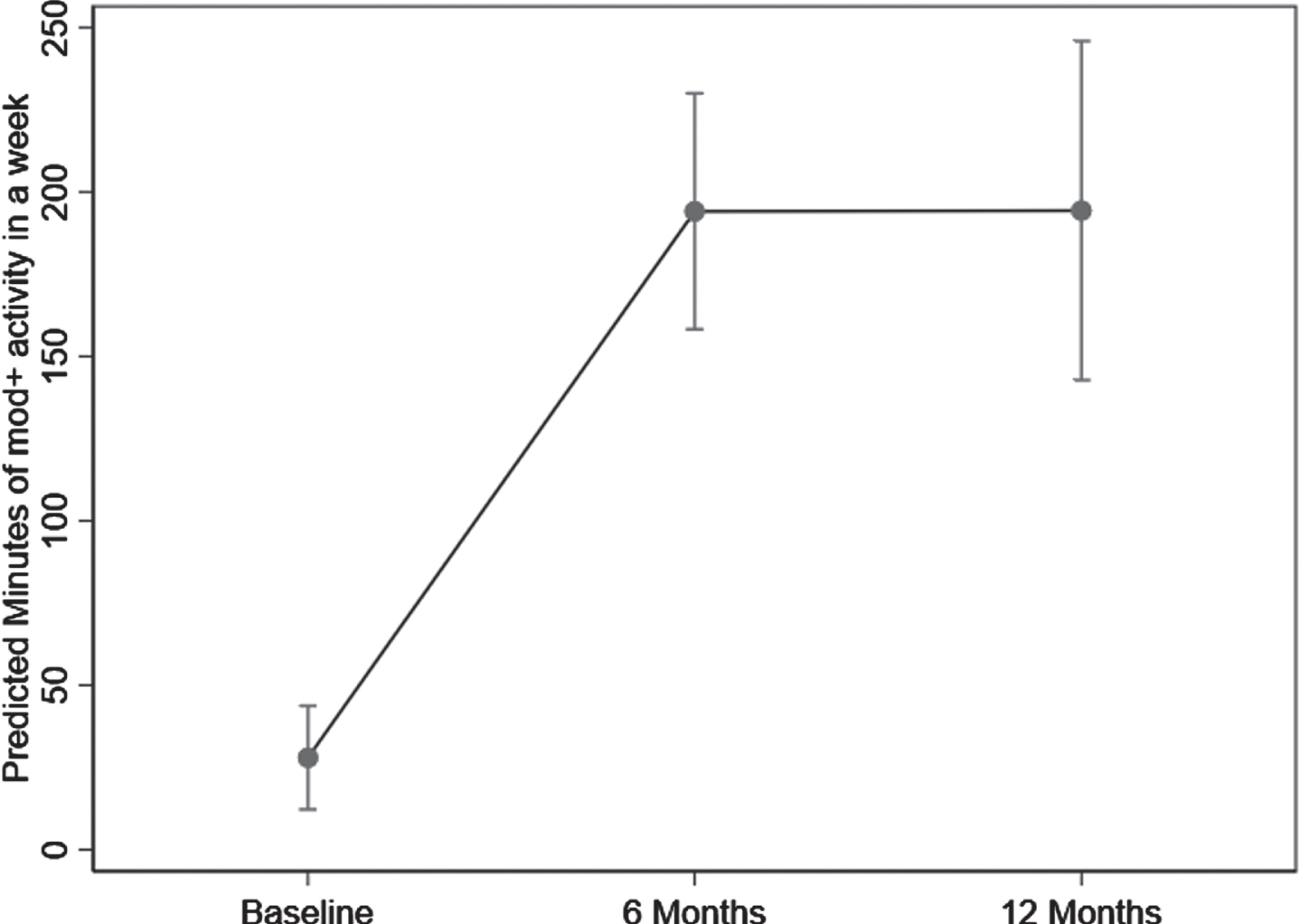
Adjusted predictions of Moderate and Vigorous PA (MVPA) minutes a week for all participants over time with 95%CIs. The model was adjusted for baseline age, SMMSE, mean goal performance score, the time interaction and 6-month call time and the time interaction and 6-month enjoyment score.
Adherence
Both groups achieved high ADH and TotADH (Table 4). Median (Q1-Q3) adherence rates of 87.4 (76.1–95.8)%versus 91.1 (71.7–95.7)%and 84.6 (78.5–92.9)%versus 84.8 (70.1–98.9)%for the control and intervention groups during the 0–6 months and 6–12 months respectively with no significant differences detected. Forty participants (81.6%) had greater than 67%ADH for the first 6 months with 23 (82.1%) maintaining this level during the 6–12-month period with similar numbers in each group. The results for TotADH were consistent with these results for the ADH. ADH was associated with higher baseline goal satisfaction and total call time during the 0–6-month period. One point on baseline goal satisfaction score was associated with a 6.6%increase in ADH (p = 0.012) and 10 min higher total call time was associated with a 1.9%increase in ADH (p = 0.004). The PA intensity RPE for both groups was similar 10.8 (10.5, 11.2) versus 10.9 (10.4, 11.4) for 0–6 months and 10.9 (10.3, 11.4) versus 11.0 (9.9, 12.0) for 6–12 months for the control and intervention groups, respectively. The PA of choice was walking n = 48 (96%).
Results for ADH and TotADH for the two 6-month periods and the overall 12-month period for the two groups in the INDIGO study conducted in Melbourne, Australia
ADH, %Adherence to prescribed program; TotADH, %Total PA adherence. Values are unadjusted mean (±sd), median scores and (Q1-Q3). The p value from the univariable model and reflects the Time×Group interaction p value that tests for a difference over time for the two groups.
Fitness
No significant difference in the change over time was detected between the 2 groups for any of the fitness measures (Table 5). However, for both groups combined cardiovascular fitness, mobility, leg strength, and balance but not grip strength improved significantly with the intervention (p < 0.001). These improvements translate to a mean increase in cardiovascular fitness of approximately 7%and 10%after 6 months and 12 months respectively with corresponding improvements in mobility 11%and 16%; leg strength 18%and 19%; balance 18%and 28%. Women on average walked 56 meters less than men on the 6-minute walk test (p = 0.024) and older age was associated with lower mobility (p = 0.006). Being female and older was associated with poorer grip strength (p < 0.001) and (p = 0.017). No associations with age and sex were detected with other fitness measures.
Cardiovascular fitness, mobility, leg strength, balance, and grip strength results over the intervention period for the control and intervention groups in the INDIGO study conducted in Melbourne, Australia
Values are raw scores of mean and 95%(CI). The p value is from the univariable model and reflects the Time×Group interaction p value that tests for a difference over time for the two groups.
Goal performance and satisfaction
There were no significant differences detected between groups in the pattern of change in goal performance and goal satisfaction over time. Goal performance scores for both groups combined increased significantly over time with on average increases of 3.80 (3.30, 4.30) and 4.00 (3.24, 4.75) (p < 0.001) at 6 and 12 months respectively (Table 6). Goal satisfaction scores had a similar pattern of change with increases of 4.12 (3.57, 4.67) at 6 months and 4.44 (3.63, 5.26) (p < 0.001) at 12 months.
Mean goal performance and goal satisfaction results over the intervention period for the control and intervention groups in the INDIGO study conducted in Melbourne, Australia
Values are raw scores mean and 95%(CI). The p value is from the univariable model and reflects the Time×Group interaction p value that tests for a difference over time for the two groups.
PA self-efficacy
No significant differences were detected between the groups for change over time in PA self-efficacy. For both groups combined PA self-efficacy increased on average by 2.66 (1.26, 4.06) (p < 0.001) and 1.83 (0.28, 3.39) (p = 0.025) over 6 and 12 months, respectively. PA program specific self-efficacy was high at baseline for both groups 96.6 (94.2, 98.8)%and was maintained over time 97.6 (95.0, 100.1)%and 97.3 (95.1, 99.5)%after 6 and 12 months, respectively.
Fidelity and program evaluation
The delivery, attendance, and compliance with aspects of the program was high with similar mean attendance rates for the workshops, 97.4 (92.2, 102)%for the control and 85.9 (73.7, 98.0) for the intervention group. The control group had 96.2%and the intervention group 76.9%participants achieving a 100%attendance at the workshops (p = 0.074). Diligence in following up participants for calls (total attempted calls) was 6.69 (5.84, 7.53) calls for the PALS and 5.11 (4.02, 6.20) calls for the mentors.
At 6 months 24 control and 21 intervention participants completed the program evaluation questionnaire. All respondents reported that the PA program was easy to follow and 95.6%enjoyed their respective programs. The “enjoyment” rating of the PAL/mentor phone calls was high and similar for both groups mean 3.49 (sd 1.27). Reasons why the calls were enjoyable included “positive qualities” of the PALS/mentors (40%) and that they provided motivation and the opportunity to talk about issues (37%). The control group rated the perceived “understanding” shown by their PAL 4.32 (0.57) which was significantly higher than the intervention group’s rating of 4.00 (0.66) for their mentor (p = 0.0005). Further, the “attributes of the PAL” score by the control group was 79.1%and “attributes of the mentor” score by the intervention group was 63.5%.
After 12 months in the program, 96.6%(n = 28) enjoyed the second 6 months with similar high enjoyment ratings. Fifteen (93.8%) in the control and 10 (76.9%) in the intervention group continued with their prescribed PA. No longer receiving calls from their PALS/mentors was not seen as affecting their ability to continue with their PA (reported by 93.8%(n = 15) of the control and 91.7%(n = 11) of the intervention groups). Reasons given for why lack of calls did not affect PA was that PA was a routine or habit 50%, (n = 11) and that participants were now self-motivated 45.4%(n = 5). Having PALS/mentors was still seen as important to promote PA in older adults by 82.8%(n = 24) of participants.
Injury during the PA program
Bursitis in the hip was reported by 2 women in the control group during the first 6 months of the program. They missed 6 and 11 of their prescribed sessions respectively, but the bursitis resolved, and they continued with their PA program for the 12 months.
DISCUSSION
In this target group of inactive, older adults at increased risk for cognitive decline we compared two different approaches, a more intensive approach utilizing goal-setting and an active control, and found both were effective with no significant differences between the groups detected. In this first study in this target group, although we were unable to realize the primary aim of the trial, by combining the data from the two groups we were able to identify key factors salient to future efforts to promote PA in underactive older people at risk for cognitive decline.
Not being able to show differences between groups in peer-led PA interventions is not uncommon [18]. In the current study, there were several possible reasons for this, the most evident being a lack of power. Secondly, it is possible that the two approaches used were too similar either in design or implementation. Table 1 highlights the similarities and differences between the programs and some design elements that may have been contributing factors. In terms of design, both groups were asked to rate their goal performance and satisfaction as outcome measures. Also, both groups monitored their PA progress via their diaries and self-monitoring has been shown to be an effective technique to increase PA and MVPA [41, 42]. With respect to potential similarities in study design, we had processes in place to minimize this, for example both the mentors and PALS received training on their respective roles only and they were regularly advised and supported by senior mentors to keep them on task.
Irrespective of not being able to discriminate between 2 intervention approaches, by combining the groups and examining the changes over time for the outcomes and the factors that were associated with these changes we were able to determine some relevant and novel findings that are salient to the promotion of PA in this group of older adults.
Effects of participation on physical activity
Across the groups as a whole, participation in the intervention increased PA as determined from pedometer steps over time. This change in steps/day exceeded the 1,000 steps/day that has been associated with a lower risk all-cause mortality cardiovascular disease morbidity and mortality [43] and frailty [44]. The magnitude of the change equates to 13–16 min/day or 92–117 min/week of brisk walking [45] and has important health implications. The PA levels in our study reached more than 8,000 steps/day which exceeds the 7,100 steps/day as the minimal amount recommended to achieve health benefits for older adults [46]. Further, in an earlier study in participants with MCI or SCD using the same 6-month PA program we demonstrated a difference of approximately 1,285 steps/day that was associated with improved cognition when compared to usual care after 6 and 18 months [6]. The association of higher baseline aerobic fitness measured by the 6-minute walk and an increase in PA is not surprising [47] nor is the association of higher BMI and lower levels of PA [48]. However, these results suggest that modifiable risk factors, such as low fitness and overweight rather than age, sex, cognitive, and APOE4 status maybe the more relevant barriers to increasing PA in this target group. This highlights the need to identify those who are less fit and overweight and at risk of not achieving increases in PA and to consider additional strategies to overcome these barriers in PA programs. The medium to large effect size of the intervention to increase PA demonstrates that these participants were not only able to adopt a more active lifestyle and maintain this in the long-term but that the magnitude of the change has potential health benefits.
This increase in PA was also supported by the increase in min/week of all intensities of PA as well as the MVPA for both groups. The significant increase in MVPA for both groups over 6 months of 164 min/week and 188 min/week for 12 months exceeds the recommended level of 150 min/week [28] and the target amount of PA for the PA intervention further supporting the efficacy and acceptability of the PA program.
It is possible that factors other than the intervention, may have played a part and been more potent in determining the increase in PA and MVPA as seen with the association of conventional factors such as age, cognition as well as program factors and MVPA in the multivariate model. The observation that younger age, better cognition, and higher goal performance at baseline were associated with higher levels of MVPA is not unexpected as these characteristics would not only support a greater capacity to follow and perform the PA but also to accurately recall the PA for self-reports. Program factors were also associated with increases in MVPA namely more peer support call time over the 6-month intervention associated with greater increases in MVPA over 6 months but not 12 months. As we reported significantly higher call time in the intervention group compared to the control group it is possible that when the calls were ceased in the second 6 months this had more impact on the intervention group than the control resulting in the declining rate of change in MVPA for the intervention group and increasing MVPA for the control group over the second 6 months. Enjoying the initial 6 months of the program was important for the maintaining MVPA during the second 6 months of this study. Both of these findings highlight the importance of providing a positive experience for inactive older people when initiating a PA program to support ongoing behavior change. This finding supports the emerging concept that enjoyment rather self-efficacy is a stronger predictor of increased PA [49, 50]. The results of our program evaluation showing high ratings of enjoyment of the PA program and the peer support calls demonstrate a positive experience for both study groups with the enjoyment attributed to the PALS/Mentor qualities and the motivation providing by being able to talk about issues. It is possible that these qualities, rather than differences in the content (education versus goal orientation) and delivery style may have had a more potent effect on participation thus demonstrating that different strategies can achieve good results.
Other interventions using peer-led delivery did not establish a difference between groups in PA in the short term. In a 4-months PA intervention utilizing a group-mediated behavioral intervention with goal-setting with peer advice and support versus a standard community PA promotion and education both groups had similar increases in PA. However, after 18 months follow-up, the peer-led group had better PA results compared to the standard group [17, 51]. Our study differed from that of Floegel and colleagues [51] in that it was home-based, the peer support was via telephone contact and the follow-up was at 12 months. Our mentors may not have been as interactive thus not achieving the same levels of social connectedness and social support that may partly explain the difference in the long-term results.
Adherence to the physical activity program
The 79%mean adherence rate for the whole group was similar to that observed in our previous studies with similar target groups [7, 8]. The observation that adherence did not change with time is also similar to our previous study where adherence to the same home-based program was consistent over 24 months demonstrating that this type of program is acceptable and sustainable in the long-term for this target group. The current study results are even more remarkable given that the participants were inactive at baseline. These results are also comparable to other PA interventions in those with MCI as a recent meta-analysis reported a 70%mean adherence rate [52]. Only one study in this review reported adherence after the end of the intervention with only 25%continuing exercise after the end of the intervention [53] whereas in the current study over 82%of participants achieved more than a 67%adherence rate underscoring the success of the study to motivate participation. The similar RPE scores for both groups within the range of moderate intensity and the high retention and adherence rates provide further evidence that this level of moderate intensity PA is both feasible and acceptable for this target group. Evidence that the program was adequately resourced and aimed at the appropriate level was demonstrated by the response of 100%of participants that it was easy to follow and high ratings of enjoyment and program components.
The program was also shown to be safe for this target group. Low-level bursitis was reported by two participants but was resolved and these participants continued with the program without further incident.
During the initiation stage of the intervention, that is the first 6 months, having a higher baseline goal satisfaction score was associated with higher adherence. Identifying participants with low goal satisfaction scores and targeting these specific goals at baseline may be a potential strategy to enhance adherence and increase PA. As noted, there was a significant difference in total call time, with the intervention group having a significantly higher total call time than the control group. However, the association of call time with adherence was independent of the group assignment. This further supports the notion that contact time rather than the content of the contact may be a more influential factor in increasing adherence at least in the initiation of PA. The belief of 92%of participants that no calls during the second 6-month period would not affect their adherence, that they were in a routine and were self-motivated was borne out by the maintenance of the adherence during the second 6 months. This suggests that peer-support is more critical in the adoption phase of a PA intervention.
Effects on functional fitness
As the adherence to the program was similar in both groups this was reflected in similar gains in fitness for both groups. Apart from grip strength, we demonstrated significant and substantial short and long-term changes in cardiovascular fitness, leg strength, mobility, and balance which are consistent with improvements of 7–46%in functional fitness reported in a review of health benefits of aerobic PA in aged adults [1]. The magnitude of the change seen in the current study was greater than the improvements in cardiovascular fitness (10%versus 4%) and leg strength (19%versus 10%) in our previous study after 12 months in a more active group using the same PA program [8]. Further, the improvement seen in mobility measured with the TUG score was within the range considered clinically significant (0.8–1.4 s) [54]. This finding of improvements in functional fitness is contrary to the conclusion from a meta-analysis that peer-led PA interventions in older adults may not be as effective in gaining improvements in functional fitness [55]. From the meta-analysis in 13 out of 18 studies, the peers led the PA sessions and 5 studies delivered support in a similar manner to our program. In our study the PA program was set by the research staff for both groups and the peer support was mainly for delivery of the behavior change aspects of the intervention that is the goal orientation or education program. This may partly explain why in this specific target group we were able to demonstrate meaningful changes in functional fitness.
Goal performance and goal satisfaction
Study participants increased their goal performance and goal satisfaction scores significantly over the course of the study with both groups showing similar improvements. The magnitude of the mean change in goal performance of 4.00 and 4.44 for goal satisfaction over 12 months was consistent with results achieved with cognitive rehabilitation in early dementia [56] and higher than the goal performance scores seen when individual goals are targeted in therapy [14]. Further, when mentoring was added to goal setting additional benefits in PA, body composition, global cognition, and memory were achieved compared to goal setting alone in healthy individuals at risk of dementia [13].
Although we were able to demonstrate these significant gains in goal scores, we were unable to demonstrate a superior effect of the goal orientated intervention. As both groups completed the BGSI and selected specific goals related to PA and PF and both then completed the same PA program, it is possible that this exposure for the control group with peer contact was sufficient to promote an increase in goal performance and satisfaction scores of similar magnitudes in both groups. The similar results for PA, adherence, and fitness scores for both groups support this notion. A further reason for lack of discrimination in these results could be that the PALS were more engaging with the participants than the mentors. The PALS were trained to only ask direct questions about PA progress, not engage in any motivational talk and their calls times were lower than the mentors. It is possible that the participants may have found this approach just as engaging and more preferable as the control group seemed to relate more positively to the PALS rating them higher on understanding and positive support for the program than did the intervention group for their mentors. The control group also found their program information more helpful and were more engaged in the education with better attendance at the workshops. Further both groups were asked to record their PA sessions in PA diaries and self-monitoring is a strong motivator for PA behavior change [10, 57]. Thus, similarities between the approaches and program factors may have contributed to our inability to discriminate between the approaches.
Strengths and limitations
A major strength of this study is that we targeted an under-researched at-risk group of inactive older adults to increase PA with an established PA program and a validated goal orientation program. The modifications to the goal orientation program where the goals targeted specific elements of PA allowed the participants to be more focused in their goal setting and actions was a further strength. The use of the pedometer to objectively quantify the total daily amount of ambulatory PA [46] was a strength but also a limitation as it may not have detected very low or slow PA, nor did it not provide a measure of the PA intensity. While the CHAMPS questionnaire enabled us to record PA and estimate the PA intensity, the reliance on self-reported PA in this target group may potentially have been a limitation. The inclusion of program evaluation questions allowed for exploration of program factors that may have influenced behavior change and the outcomes of interest. The similarity between the approaches discussed above was a limitation of the study. This together with slow recruitment, resulting in low numbers of participants in the trial and thus reduced power, were limitations in enabling us to demonstrate between-group differences. The further restriction in numbers with only a sub-group continuing for 12 months limited our ability to demonstrate long-term changes.
In summary, in this inactive target group who are particularly difficult to engage we have provided clear evidence that PA levels and functional fitness can improve and that after an initial stage with peer support the PA can become habitual if it is enjoyable. These improvements were commensurate with health benefits and this increase was achieved even with a less intensive intervention. If these results are substantiated in future studies this has implications for PA promotion in that fewer community resources may be needed which may lead to more cost-effective programs. Also, this less intense approach provides another option that researchers and practitioners can utilize in research or implementation programs where some individuals may do better with one approach or another. Hence, having a range of effective options and providing individuals with a choice to select what suits them best may potentially enhance the uptake of PA. Further, community peer volunteers successfully delivered and provided acceptable, effective support for this target group and as such their value as a resource and delivery strategy should be economically evaluated. Barriers to participation identified in this study such as being overweight or having low fitness levels should be a focus of future programs with the development of strategies to overcome or minimize these. We have also highlighted novel theoretical constructs in the promotion of PA uptake and adherence such as enjoyment particularly in the initial stages and program factors including social support provided by the peer volunteers. This support was provided predominantly via phone, but other forms of communication deserve exploration such as emails and online social media. These findings have implications for translation into the community and should be explored further to ensure that intervention strategies are relevant to this target group. Due to the limitations outlined above these results are somewhat tentative until confirmed in a larger adequately powered intervention study. Recruitment is challenging for such studies and innovative strategies may be required to attract participants. We further recommend that future studies be conducted where the intervention is distinctly different from the control condition and avoids or minimizes any overlapping methods.
CONCLUSION
In this inactive target group at risk of cognitive decline, no differences were detected between groups in PA uptake, hence we were unable to confirm our hypothesis that the novel PA intervention utilizing individual goal-setting and peer mentors was superior to the control program. Instead, both approaches were highly effective in increasing PA and fitness in the short and long-term. Our study demonstrates that programs supported by peer volunteers are acceptable and effective and the findings suggest the less intensive peer contact maybe sufficient to improve PA levels. This approach should be explored in larger targeted implementation studies.
Footnotes
ACKNOWLEDGMENTS
We are most grateful to all the participants, mentors, and peer contact volunteers for their time and dedication to this study and to our research staff, Anita Goh, Ellen Gaffy, and Stephanie Perin for their contributions to the coordination, data collection and conduct of the project.
This trial was supported by a project grant from the National Health and Medical Research Council (1045530) to NL, KC, CE-B, KE, EC, HA, LC, DL, DA, LF, OA, and DL. We also acknowledge financial support from the NHMRC Centre of Research Excellence in Cognitive Health (CRE 1100579). The funding bodies had no role in the design of the study or the collection, analysis, interpretation of data or in writing the manuscript.