
Abstract
Background:
Cancer-related cognitive impairment (CRCI), a frequent effect of cancer and its treatments, shares common cognitive symptoms with dementia syndromes. Cross-sectional studies demonstrate an inverse relationship between cancer and dementia. However, the longitudinal relationship between dementia decline and cancer has not been investigated.
Objective:
To evaluate the association between cancer and longitudinal progression of dementia.
Methods:
We extracted electronic health record data from July 2003 to February 2020 from a single academic medical center. We identified dementia and cancer history prior to dementia using ICD-9/10 codes. We measured cognitive decline with the Alabama Brief Cognitive Screener (ABCs). We used adjusted linear mixed models to estimate baseline cognition and rate of progression by cancer history, including differences by race.
Results:
The study included 3,809 participants with dementia, of which 672 (17.6%) had cancer history. Those with cancer history had higher baseline cognition (β: 1.07, 95% CI: 0.45, 1.69), but similar rate of decline. Non-Hispanic Blacks had lower cognitive scores at baseline and throughout follow-up regardless of cancer status compared to non-Hispanic Whites and other races/ethnicities with and without cancer history.
Conclusion:
In this longitudinal retrospective study, participants with cancer history demonstrate better cognition at dementia diagnosis and no difference in cognitive decline than those without cancer history. Smoking and comorbidities attenuate this association and results indicate non-Hispanic Blacks have worse cognitive outcomes in dementia regardless of cancer history than other race/ethnicity groups. Further exploration of the role of smoking, comorbidities, and race/ethnicity on cancer and dementia-related cognitive decline is needed.
INTRODUCTION
Cancer and Alzheimer’s disease (AD), the most common form of dementia, are prevalent aging-related diseases in adults aged 65 years and older; approximately 1 in 8 males and 1 in 10 females will develop cancer from age 60–69, and approximately 1 in 10 older adults has AD [1, 2]. The prevalence of cancer and AD both increase with age, such that for those ≥70 years of age, approximately 1 in 3 males and 1 in 4 females will develop cancer, and approximately 14% of those ≥71 years of age have any dementia syndrome [1, 2]. By 2030, 20% of the population will be 65 years and older (older adult); this increase in the number of older adults will further increase prevalence of aging-related diseases, such as cancer and dementia [3].
Cancer and dementia share common risk factors beyond age, such as cardiovascular disorders (i.e., hypertension, diabetes), and share several comorbidities, including depression [1, 4–6]. Many older adults are also taking medications known to be anti-cholinergic and negatively affect cognition [7–9]. Cognitive impairment can also occur as a result of cancer and its treatments, with symptoms similar to those experienced in dementia patients [10–12]. Given these findings, it might be assumed that cancer and dementia would overlap, but several cross-sectional studies indicate a bidirectional inverse relationship between cancer and AD [13, 14]. Other studies demonstrate a similar association between any cancer and any dementia syndrome [15, 16]. Only one study examines the association between cancer and AD or dementia longitudinally, and indicates a similar inverse association [17]. A previous study from our group examining the longitudinal association between cancer and progression of AD concludes that those with self-reported cancer history demonstrate better cognition early in the AD disease course compared to those without self-reported cancer history, but the two groups experience similar rates of cognitive decline [18]. This previous study utilizes data from the Alzheimer’s Disease Neuroimaging Initiative (ADNI), a longitudinal, observational study with primarily White, healthy, and highly educated participants. Additionally, the study utilizes self-reported cancer history to determine cancer status, and does not adjust for use of anti-dementia medications, which are known to reduce cognitive decline [18, 19]. Given the recognized racial and ethnic disparities in AD [20–23], it is also unknown if our prior findings apply in a more diverse cohort. Therefore, the objective of this study was to examine the association between cancer and longitudinal progression of dementia using data from the electronic health record (EHR) from a large academic medical center in the Southeast while adjusting for important covariates.
METHODS
Study population
We obtained data from the EHR at the University of Alabama at Birmingham (UAB) from July 2003 to February 2020. UAB’s standing as a large academic medical center, the site of the only National Cancer Institute (NCI) designated Comprehensive Cancer Center in four states—Alabama, Mississippi, Louisiana, and Arkansas—and the site of a Memory Disorders Clinic with neurologists and advanced-practice nurses specifically trained in diagnosing, treating, and researching all-cause dementia made it well suited to examine the longitudinal association between cancer and cognition in dementia. We included participants meeting the following criteria: 1) an International Classification of Disease (ICD)-9 or ICD-10 diagnosis code of all-cause dementia in any position on the diagnosis and/or problems list (see the Supplementary Material for specific ICD-9 and ICD-10 codes), 2) one or more cognitive test scores using the Alabama Brief Cognitive Screener (ABCs, described below), and 3) 50 years old or older at the date of dementia diagnosis [24]. We conducted a chart review of 10% of the patients diagnosed with dementia, not otherwise specified (NOS) (see the Supplementary Material for specific ICD-9/10 codes) to verify subtype based on chart notes [24]. Most dementias, regardless of subtype, were billed as dementia, NOS [24]. However, chart notes provided clarity on underlying subtype, which is important given pathological and cognitive differences among dementia subtypes [1, 25]. We excluded participants with cancers of the central nervous system (CNS) due to the potential for negative cognitive consequences related to CNS tumors and the inability to extrapolate cancer-related cognitive impairment (CRCI) from brain tumor induced cognitive impairment. The UAB IRB approved this study.
Primary outcome: Alabama Brief Cognitive Screener (ABCs)
We chose the ABCs, a validated cognitive assessment tool developed by Geldmacher et al. to globally assess cognition (including measures of orientation, memory, concentration, naming, and repetition) in the ambulatory clinic, as the primary outcome [26]. We chose the ABCs because it has demonstrated good internal consistency (Chronbach’s alpha = 0.85), resembled scoring on the Mini-Mental State Examination, and was typically performed serially every 6 months in the clinic [26]. A clinically meaningful difference on the ABCs is considered to be a change of 1–3 points.
Primary exposure: Cancer diagnosis history
We assigned prior diagnosis of cancer as the primary exposure. We identified cancer diagnosis by assessing participant records for the presence of an ICD-9/10 diagnosis code of non-CNS cancer in any position on the diagnosis list, problems list, and/or the UAB tumor registry prior to dementia diagnosis (see Supplementary Material for specific cancer ICD-9/10 codes). The UAB tumor registry included all patients diagnosed with cancer at UAB. We converted all Systematized Nomenclature of Medicine Clinical Terms (SNOMED) codes in the diagnosis and/or problems lists to ICD-10 codes. We excluded patients who developed any subsequent cancer after dementia diagnosis. We created an all-cancer variable which excluded participants with only non-melanoma skin cancer and the following specific cancer variables: breast, prostate, colorectal, testicular, cervical, lung, and all other cancers. Finally, we created an additional variable for those with two or more cancers. Unfortunately, cancer treatment and cancer staging data are not consistently available in the EHR.
Covariates
Demographics, health behaviors, and socioeconomic factors
We collected demographic information on the dementia diagnosis date including the following: age, race, ethnicity, sex, and marital status. We collapsed race and ethnicity to create a categorical variable with three levels: non-Hispanic White, non-Hispanic Black, and other. The EHR did not collect smoking status at all visits, but when collected it was a free-text entry. We used the smoking status on or closest to dementia diagnosis to categorize participants as ‘ever’ or ‘never’ smoker based on the free-text responses. We collected insurance status at dementia diagnosis and collapsed into categories of private, government, and other insurance. We utilized the height and weight information closest to and within 12 months of the dementia diagnosis to calculate body mass index (BMI). We reviewed the BMI values and replaced those that were impossible or exceedingly inconsistent with other recent visits with the value next closest to the dementia diagnosis.
We calculated the Neighborhood Deprivation Index (NDI) to assess socioeconomic status [27]. In doing so, we used ZIP codes at dementia diagnosis and merged with county FIPS codes to create 9-digit ZIP codes. We then merged 9-digit ZIP code with 2019 American Community Survey 5-year estimates of percentage of female-headed households and percentage of households below the poverty line. We divided both percentages by 10 and took the mean of the two variables to create the NDI score for each participant’s 9-digit ZIP code area. We utilized 9-digit ZIP code rather than census tracts based on prior work by Ross and Mirowsky noting that ZIP codes are the “next best approximation to a neighborhood” if census tracts are unavailable as in the EHR [28]. We divided NDI into quartiles for stratified models.
Comorbidities
We identified participants with depression based on diagnosis codes and medications using a previously described algorithm [29]. We identified specific ICD-9/10 codes (see the Supplementary Material) from the diagnosis list or problems list for each participant on or at any time prior to the dementia diagnosis. We also identified medications for depression (see the Supplementary Material) from the medication list on or at any time prior to the dementia diagnosis. We classified participants with either a depression diagnosis or a medication for depression as having depression and all others as not having depression.
We created a vascular propensity score to adjust for vascular risk factors [30–32]. We included the propensity score as a covariate, rather than as a weight, in the main analyses described below. This approach and its rigor has been described elsewhere [31, 32]. We used logistic regression to determine the probability of having cancer (using the all-cancer variable) with smoking status, diabetes status, hypertension status, and BMI as predictors. We excluded participants missing any vascular predictors. We classified diabetes and hypertension using diagnoses, medications, and vital signs/lab values. For diagnoses, we examined the diagnosis list and problems list on or at any time prior to dementia diagnosis for ICD-9/10 codes for diabetes and hypertension (see the Supplementary Material for specific codes). For medications, we examined the medication lists on or at any time prior to dementia diagnosis for medications prescribed for diabetes and hypertension (see the Supplementary Material for specific medications). For vital signs/lab values, we used levels of systolic blood pressure, diastolic blood pressure, and blood glucose on or closest to and within 12 months of the dementia diagnosis. We compared extreme values to other visits and used the next closest value if impossible or exceedingly inconsistent with other recent visits. We classified hypertension as a systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg and diabetes as a random glucose of ≥200 mg/dL. We created overall diabetes and hypertension variables whereby presence of a diagnosis code, a medication, or above the threshold for vital signs/lab values indicated presence of the disease and absence of all three indicated absence of the disease. We used this multi-level approach as it is often used for classification of chronic conditions in studies utilizing administrative claims-based data [33].
Anti-cholinergic burden
We calculated anti-cholinergic burden using a previously described algorithm [7]. Briefly, we assigned an anti-cholinergic score to individual medications on or at any time prior to dementia diagnosis and totaled the score for each participant to determine overall Anti-Cholinergic Burden (ACB) score on dementia diagnosis. We considered a clinically significant ACB to be a total score of ≥3. The ACB was the most widely used scale for this purpose, having been used in several studies to predict cognitive impairment, and compared well to other similar scales [9].
Dementia-related medications
We created a dementia medication variable by searching each participant’s medication list on or after the dementia diagnosis. We classified any participants prescribed donepezil (Aricept), galantamine (Razadyne), rivastigmine (Exelon), memantine (Namenda), and/or donepezil + memantine (Namzaric) as taking a dementia medication.
Statistical analysis
We examined differences in participant characteristics between those with and without cancer history using chi-square tests and t-tests for categorical and continuous variables, respectively. We used Fisher’s exact tests where expected sample size was insufficient for categorical variables. To assess differences in baseline cognition and cognitive progression among cancer groups, we used hierarchical linear mixed effects models with a random effect for time [34]. Participants with only one ABCs score contributed to estimation of the model intercept and participants with two or more scores contributed to estimation of both the intercept and slope. We adjusted initial models for basic demographics including: age at dementia diagnosis, race, and sex. Next, we further adjusted for socioeconomic variables: NDI and insurance status. We adjusted the final model for all previous variables and anticholinergic burden, depression, vascular propensity score, and dementia medication use. Continuous variables age at dementia diagnosis, NDI, total anti-cholinergic burden, and vascular propensity score were centered on the group mean by all-cancer group. Model results included an intercept (or the baseline effect of cancer), which described the difference in baseline cognitive score based on cancer history status, and the slope (or the cancer by time effect), which described the difference in cognitive decline over time based on cancer history status. We performed separate analyses for specific cancer groups with sufficient sample size (n = 20). We evaluated interaction by race and NDI in the all-cancer model. We stratified models if the race/NDI interactions were significant. We set statistical significance at α= 0.05 and we conducted analyses using SAS 9.4 (SAS Institute, Inc., Cary, NC) and RStudio 1.2.5033.
RESULTS
Our study sample included 3,809 participants with dementia, of which 672 (17.6%) and 3,137 (82.4%) did and did not have history of cancer, respectively. Of the 672 with history of any cancer, 29 (4.3%) had history of only colorectal cancer, 66 (9.8%) only breast cancer, 16 (2.4%) only lung cancer, 65 (9.7%) only prostate cancer, 356 (53.0%) had history of other cancers, and 139 (20.7%) had history of two or more cancers (Fig. 1). Of those with history of cancer, 140 were missing date of cancer diagnosis and therefore missing time before dementia diagnosis. For remaining participants, the mean time between cancer diagnosis and dementia diagnosis was 2.9 years±2.2 years. The minimum time was 0 years and the maximum time was 12.2 years. Those with history of any cancer were significantly older (76.4 versus 73.2 years, p < 0.001), more likely to be widowed (26.2% versus 20.7%, p = 0.027), had lower NDI score (0.79 versus 0.84, p = 0.036), more likely to be on a government insurance plan (90.5% versus 84.7%, p = 0.001), and more likely to be an ever smoker (47.1% versus 42.9%, p = 0.046) than those without history of cancer (Table 1). Participants with history of cancer were more likely to have depression (72.2% versus 68.9%, p < 0.001), hypertension (89.3% versus 81.4%, p < 0.001), and diabetes (33.3% versus 24.9%, p < 0.001), had higher mean total ACB (6.9 versus 3.8, p < 0.001) and vascular propensity scores (0.19 versus 0.17, p < 0.001), and were less likely to be on a dementia medication (57.4 versus 62.1, p = 0.026) than those without history of cancer (Table 1). Approximately 1,480 participants had only one ABCs score. The median (inter-quartile range) of visits was 2 (1–4). Overall, mean ABCs score was 20.3±6.5 and ranged from 0–30. Among those with and without history of cancer, mean ABCs score was 21.5±6.1 and 20.1±6.5, respectively. The range for both cancer history groups was 0–30.

Flow Chart of Participant Categorization. Those with only history of non-melanoma skin cancer were not included in the cancer group.
Participant Characteristics by Cancer History Status. Cancer indicates participants with any cancer excluding cancers of the central nervous system and non-melanoma skin cancer. No Cancer indicates participants without any cancer but may have non-melanoma skin cancer. Evaluated using t-tests and chi-square tests / Fisher’s exact tests (where necessary) for continuous and categorical variables, respectively. Significance set at α= 0.05
†NDI, neighborhood deprivation index based on algorithm published by Ross et al. [27, 28]; BMI, body mass index calculated using height/weight closest to dementia diagnosis within 1 year of diagnosis; SBP, systolic blood pressure, on or closest to dementia diagnosis within 1 year of diagnosis; DBP, diastolic blood pressure, on or closest to dementia diagnosis within 1 year of diagnosis; glucose level, on or closest to dementia diagnosis within 1 year of diagnosis; depression, based on algorithm published by Trinh et al. [29]; dementia medication, donepezil (Aricept), galantamine (Razadyne), rivastigmine (Exelon), memantine (Namenda), and/or donepezil + memantine (Namzaric); hypertension, based on SBP ≥140 mmHg / DBP ≥90 mmHg, diagnosis of hypertension prior to dementia diagnosis, and/or presence of hypertensive medications prior to dementia diagnosis; diabetes, based on glucose of ≥200 mg/dL, diagnosis of diabetes prior to dementia diagnosis, and/or presence of diabetic medications prior to dementia diagnosis; total anticholinergic burden, prior to dementia diagnosis based on algorithm published by Boustani et al. [7]; vascular propensity score, propensity of cancer exposure based on smoking status, BMI, hypertension status, and diabetes status. ‡Other includes Creutzfeldt-Jakob disease, Huntington’s disease, drug-induced dementia.
Dementia codes differed cancer history versus no cancer history (AD: 17.6% versus 22.9%; Alcohol-induced: 0.3% versus 0.2%; Dementia with Lewy bodies: 2.5% versus 4.0; Frontotemporal: 2.2% versus 4.2%; Vascular: 6.7% versus 6.1%; Not otherwise specified: 70.4% versus 62.6%; Other: 0.3% versus 0.0%; p < 0.001). Dementia, NOS was the most common code in each group, though there was a larger proportion of Dementia NOS in participants with history of cancer than those without (70.4% versus 62.6%). In our chart review of the 10% Dementia NOS cases, 74 (27.4%) had AD, 63 (23.3%) had subtype still unable to be identified, and 133 (49.3%) had dementia of another subtype (vascular, Parkinson’s-related, dementia with Lewy bodies, mixed, etc.)
Effects of cancer history on baseline cognition and cognitive progression
Our initial model adjusted for group-centered age at dementia diagnosis, race, and sex revealed that those with any cancer history began with cognition 1.28 (95% CI: 0.71, 1.84) points higher on the ABCs and progressed 0.41 (95% CI: 0.11, 0.71) points per year slower than those without any cancer history (Table 2). By cancer site, no significant results were present for baseline cognition or cognitive progression with exception of those with history of other cancers. Participants with history of two or more cancers began with baseline cognition 1.85 (95% CI: –3.03, –0.68) points lower and progressed 0.46 (95% CI: –0.12, 1.04) points per year slower than those without cancer history (Table 2).
Estimates of Cognitive Performance at Baseline and Decline Over Time by Cancer History Status. Estimated using linear mixed effects models with random effect for time. Cognition measured using the Alabama Brief Cognitive Screener (ABCs). Significance set at α= 0.05. Intercept indicates the mean difference in ABCs score based on cancer status; slope indicates the mean difference in decline on the ABCs per year based on cancer status
†Adjusted for sex, race, and age at dementia diagnosis. ‡Adjusted for all variables in Model 1 plus neighborhood deprivation index and insurance status. ¥Adjusted for all variables in Model 2 plus total anti-cholinergic burden before dementia diagnosis, vascular propensity score on or before dementia diagnosis, depression status on or before dementia diagnosis, and taking a dementia medication on or before dementia diagnosis.
After adjustment for socioeconomic factors, group-centered NDI and insurance status, results remained relatively unchanged. Participants with any cancer history began with cognition 1.28 (95% CI: 0.71, 1.86) points higher and progressed 0.40 (95% CI: 0.08, 0.71) points per year slower than those without any cancer history (Table 2). Analysis by cancer site maintained non-significant results for both baseline cognition and cognitive progression again with exception of those with history of other cancers. Similar to the initial model, participants with history of two or more cancers began with baseline cognition 2.04 (95% CI: –3.23, –0.86) points lower than those without cancer history (Table 2).
Results attenuated after further adjustment for group-centered total anti-cholinergic burden, group centered vascular propensity score, depression, and dementia medication. Participants with any cancer history began with cognition 1.07 (95% CI: 0.45, 1.69) points higher and progressed 0.26 (95% CI: –0.07, 0.59) points per year slower than those without history of any cancer (Table 2). Participants with history of other cancers began with cognition 1.02 (95% CI: 0.21, 1.84) points higher and progressed 0.54 (95% CI: 0.10, 0.97) points per year slower than those without history of any cancer. For participants with history of two or more cancers, results exhibited a similar pattern compared to the prior models where those with history of two or more cancers began 1.52 (95% CI: –2.79, –0.25) points lower and progressed 0.31 (95% CI: –0.31, 0.93) points per year slower than those without cancer history (Table 2). Figure 2 depicts the predicted baseline score and progression over time for each cancer group compared to the no cancer group.
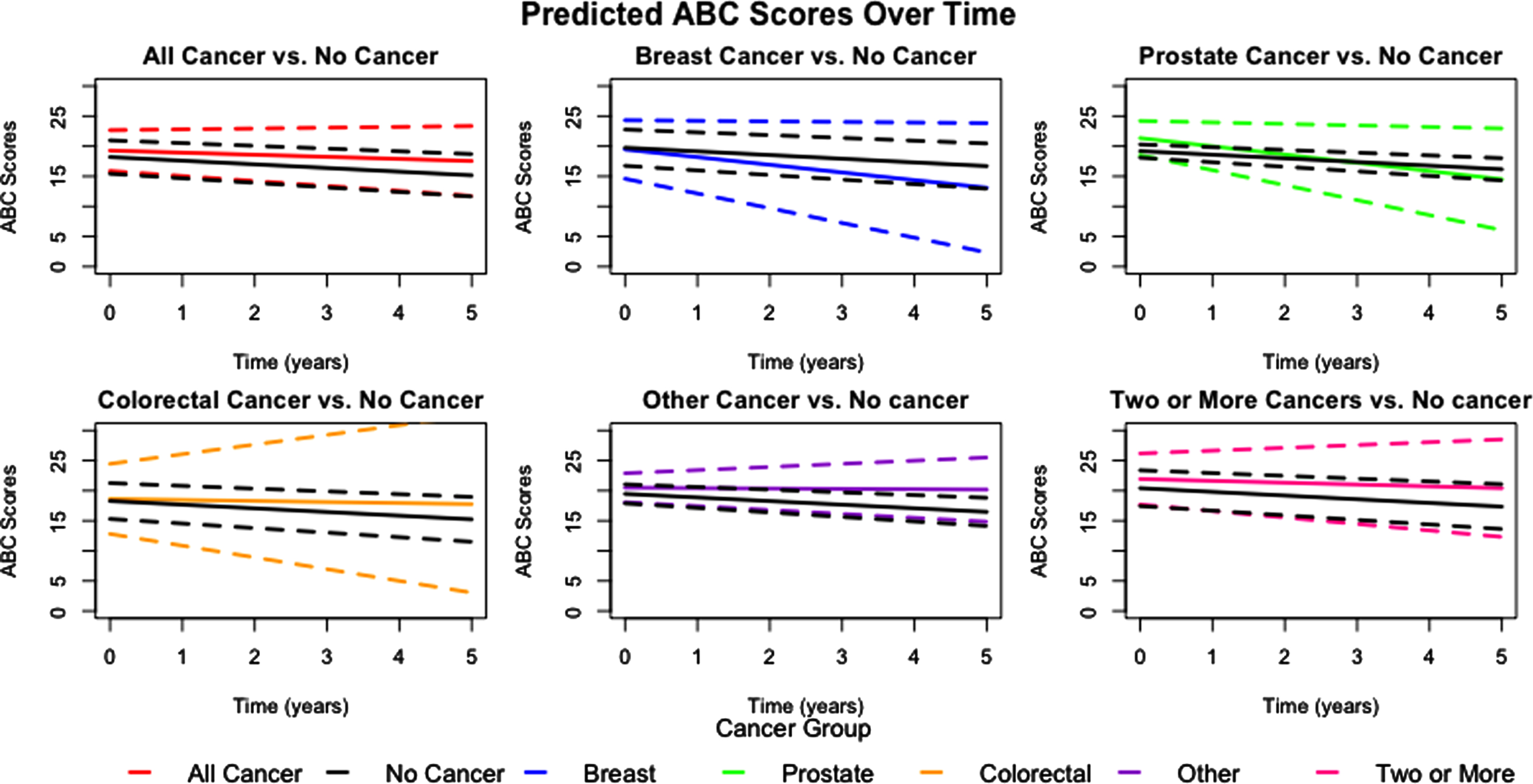
Predicted Alabama Brief Cognitive Screener (ABCs) Scores Over Time by Cancer History Group. Dementia patients with history of any cancer (excluding those with central nervous system cancers or only non-melanoma skin cancer) demonstrate better baseline cognitive score and slower decline over time compared to the dementia patients in the group with no cancer history. Similar associations are seen for those with history of other cancers and two or more cancers. Dashed lines indicate 95% confidence intervals.
We noted significant interaction by race and NDI in the all-cancer model (race: p = 0.030, NDI: p = 0.022). As a result, we stratified models by race/ethnicity and observed that regardless of cancer status, non-Hispanic Whites began with better cognition than other race/ethnicity groups. Non-Hispanic Whites with positive cancer history began higher and declined slower than non-Hispanic Whites with negative cancer history. However, we found that among non-Hispanic Blacks, cancer status did not result in differences in cognitive baseline or decline. Interestingly, we noted that while non-Hispanic Blacks began lower than either of the remaining race/ethnicity groups, their cognitive decline was not as fast. Finally, participants of other race/ethnicity demonstrated similar baseline cognition to non-Hispanic Whites, but those with positive cancer history declined faster than those with negative cancer history (Fig. 3). After stratification by NDI, we observed that participants in quartiles 1 and 2 (i.e., less disadvantaged) began with cognition lower than those in quartiles 3 and 4. Participants in quartiles 1, 2, and 3 with positive cancer history declined slower than participants with negative cancer history in their respective quartiles. Participants in quartile 4 declined similarly regardless of cancer status (Fig. 4).
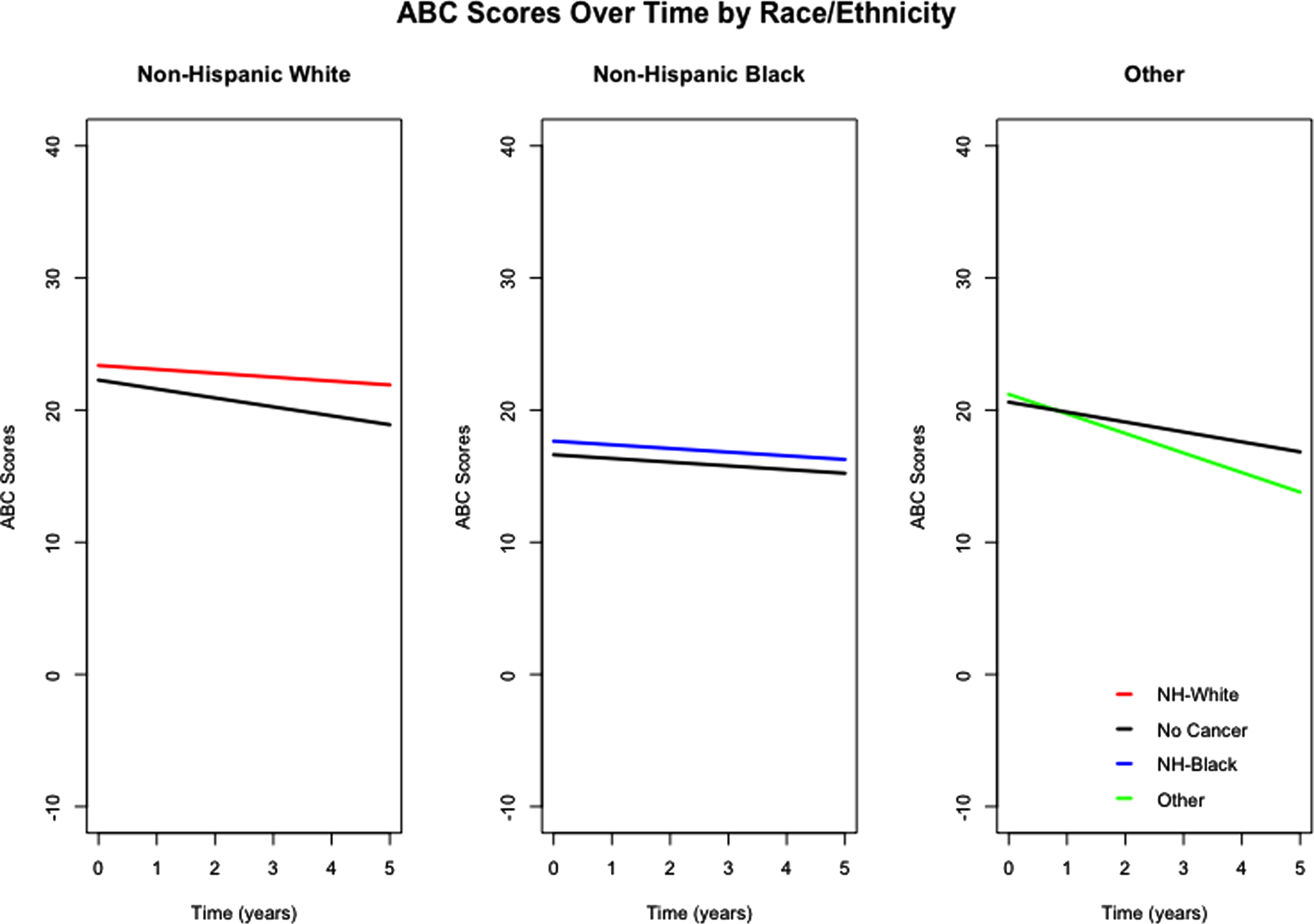
Predicted Alabama Brief Cognitive Screener (ABCs) Scores Over Time by Race/Ethnicity in Those with Any Cancer History. Non-Hispanic Black participants with dementia regardless of cancer history (excluding those with central nervous system cancers or only non-melanoma skin cancer) begin with lower cognition at baseline and progress slower than non-Hispanic Black participants without cancer history, non-Hispanic White participants with and without cancer history, and participants of other races/ethnicities with and without cancer history.

Predicted Alabama Brief Cognitive Screener (ABCs) Scores Over Time by NDI Quartiles in Those with Any Cancer History. Dementia patients with cancer history in lower NDI quartiles, corresponding to decreasing neighborhood deprivation, demonstrate similar cognitive scores at baseline, but slower decline compared to those without cancer history. Dementia patients with cancer history in higher NDI quartiles demonstrate higher cognitive scores at baseline and slower decline with similar decline seen in the highest quartile.
DISCUSSION
Our analysis of EHR data from a large academic medical center in the Southeast US revealed an approximate 1.1-point higher cognitive score at baseline (intercept) and an approximate 0.5-point slower decline (slope) in cognitive score for those with any cancer history compared to those without cancer history. For those with two or more cancers, the results were opposite indicating an approximate 1.5-point lower cognitive score at baseline and an approximate 0.3-point slower decline in cognitive score compared to those without cancer history. Furthermore, interaction between race/ethnicity and socioeconomic status was present in the relationship between cancer history and cognition/cognitive progression. Cancer status did not result in cognitive differences at baseline or over time among non-Hispanic Blacks. However, non-Hispanic Blacks began with cognition lower than other race/ethnicity groups regardless of cancer status, and cognitive decline differed based on cancer status among other race/ethnicity groups. Furthermore, those in higher quartiles of NDI (i.e., more disadvantaged) began at a higher baseline cognitive score and positive cancer history resulted in slower cognitive decline compared to those with negative cancer history regardless of NDI quartile.
These results are consistent with those from our prior work in the Alzheimer’s Disease Neuroimaging Initiative (ADNI) dataset [18]. Specifically, our prior study indicated clinically significant better baseline cognition. This effect was only seen in those with mild cognitive impairment (MCI), but not AD. The current study also reveals significantly better baseline cognition, but the cognitive decline results differ between the two studies. Among the MCI and AD patients in the prior study, no difference in decline over time was observed by cancer history status. However, the current study suggests slower decline for those with a previous cancer diagnosis compared to those without a previous cancer diagnosis. Some of these differences may be explained by the current study addressing many of the prior study’s important limitations [18].
In contrast to the prior study, this effect was seen in those with dementia and not strictly MCI, but the average baseline ABCs score in our sample was 20–25, corresponding to milder impairment relatively similar to the ADNI cohort. In the prior study, no cognitive differences between the cancer and no cancer groups were observed among those with AD. Unfortunately, coding of AD and specific dementia codes in the EHR is imperfect and frequently recorded as a non-specific dementia NOS code [35]. This was further corroborated specifically for the UAB EHR by physicians in the UAB Memory Disorders Clinic. Therefore, the current study was limited to an analysis of dementia overall. Despite the inability to study AD specifically, previous studies have also demonstrated an inverse cross-sectional relationship in all-cause dementia and cancer, making the current results commensurate with studies assessing only AD [15, 16]. The lack of an effect between the AD sample from the prior study and the observance of an effect in the current sample may be due to the inclusion of a more diverse sample, real-world patients, and/or a slightly more cognitively diminished sample of patients, rather than those willing and able to enroll in an AD observational study. The current sample did include a majority with dementia NOS, potentially driving the results. After chart review, approximately 23% of these remained with no definitive pathology, thus potentially increasing the overall prevalence of each specific dementia type. Thus, the prevalence of each dementia subtype is likely an underestimate. Future studies should corroborate these findings in specific dementia subtypes.
Clinical significance on the ABCs is approximately a 1–3 point difference [26, 36]. In the current analysis, after adjustment we observed an approximate 1.1-point difference in baseline cognition on the ABCs between those with and without cancer history, indicating that having had cancer results in improved cognition at dementia diagnosis. Also, after adjustment we observed an approximate 0.5-point difference in decline per year where patients with cancer history decline more slowly. This observed rate of decline may not result in a clinically significant change over one year of follow-up but will reach clinical significance after two years. Since dementia patients typically live an average of 4–8 years post-diagnosis, this effect requires further exploration as to its causes and possible interventions [1]. However, these results seem to be somewhat attenuated by risk factors and comorbidities. Prior to adjustment for these confounders, we observed a clinically and statistically significant approximate 1.3-point higher baseline cognitive score and statistically significant 0.5-point slower cognitive decline per year between those with and without cancer history. Investigation into the role of comorbidities and smoking on cognition after cancer is necessary to elucidate mechanisms of this attenuation and to identify potential areas for intervention.
Several factors may be driving these results. The overall effect on cognition may be due to differing cancer treatments, improved social support in cancer survivors, or increased access to the healthcare system following cancer diagnosis and treatment, which we were unable to assess in our analysis. Kelly et al. conducted a systematic review assessing social support in healthy older adults and concluded that increased social activity, larger social networks, and improved social support result in better cognition [37]. Other studies have indicated that satisfaction with social support, having social networks/higher quality of these networks, and higher levels of social support offer improved cancer-related outcomes [38–40]. The American Cancer Society has released Survivorship Care Guidelines for colorectal, breast, prostate, and head/neck cancer, which each suggest routine history and physical and assessment of long-term/late psychosocial effects of these cancers throughout the first year following treatment completion [41–44]. With these routine examinations, primary care physicians may be more likely to capture dementia syndromes early due to patients with cancer history’s routine contact with the healthcare system. Diagnoses of dementia have commonly been missed or delayed in primary care settings; but since patients had prior cancer, primary care physicians may be more aware of or responsive to cognitive issues [45]. The median number of outpatient visits between first reported cancer diagnosis and dementia was 37 (Inter-quartile range: 16–76) supporting the hypothesis that patients with cancer history may have frequent contact with the health system. An additional analysis of specialty dementia care use by cancer history is planned in this sample. It is also possible that there may be a survivor bias where cancer patients who survive are different from those who did not and cancer patients who did and did not develop dementia. Future studies should examine cognitive change among cancer survivors who did not develop dementia for comparison.
Finally, known racial and ethnic differences exist in cancer and dementia [20–23, 46–48]. Disparities were also noted in this study. Non-Hispanic Blacks had similar cognition at baseline and over time regardless of cancer status but were lower than all other race/ethnicity groups, again regardless of cancer status. Cognitive decline among non-Hispanic Blacks was also relatively constant compared to other race/ethnicity groups. This may indicate that non-Hispanic Blacks were diagnosed later in the disease course and therefore did not have as much cognitive function to lose over time. Given follow-up guidelines for patients with cancer, non-Hispanic Blacks with positive cancer history would be expected to have begun with higher cognition and decline slower than non-Hispanic Blacks with negative cancer history, similar to the overall results and to results in non-Hispanic Whites and ‘other’ race/ethnicities [41–44]. Therefore, non-Hispanic Blacks may not have been followed according to guidelines and/or incompletely followed. Prior evidence indicated that Blacks were less likely to receive National Comprehensive Cancer Network (NCCN) guideline care during cancer treatment [49, 50]. Likewise, guideline care may have been subpar after cancer treatment. Interventions at the point of care for non-Hispanic Blacks could alleviate disparities in cognition in both dementia and cancer. Additionally, lay navigators have been implemented for navigating end-of-life decisions and other distressing patient concerns during cancer treatment [51, 52]. Lay navigation showed benefit for both older Blacks and Whites [53]. Expanding lay navigation programs to include navigation during cancer survivorship including issues such as subjective cognitive complaints and engaging survivors in proper follow-up during cancer survivorship may improve cognitive outcomes. Another potential driver of these disparities may be that factors which help to preserve cognition in dementia, such as cognitive reserve and education, may have been lower among non-Hispanic Blacks, resulting in a rapid depletion of cognition with less room for further decline compared to other race/ethnicity groups [54–56]. However, those in the ‘other’ race/ethnicity group should have demonstrated a similar trend, given evidence of lower cognitive reserve and education among other minority groups. The ‘other’ race/ethnicity group was relatively small, though, and results may differ in a larger sample. Small sample size may also explain why, among the ‘other’ race/ethnic group, results were opposite the overall and non-Hispanic White/non-Hispanic Black groups. Non-Hispanic Blacks may also have differential cancer-related survival bias whereby Blacks are more likely to not survive cancer and/or more likely to have long-term side effects of cancer due to differences in care. Future studies should not only examine survival bias as mentioned above, but also should examine racial disparities in this association. Moreover, socioeconomic status may modify the association between cancer and cognition in dementia. Higher quartiles of NDI resulted in higher baseline cognitive scores, but positive cancer history resulted in slower decline regardless of NDI quartile. Those in higher quartiles represent ZIP codes with higher rates of poverty and female-headed households compared to those in lower quartiles. Therefore, it seems more likely that participants from more disadvantaged backgrounds could begin at a lower baseline cognitive score than those in lower quartiles [57, 58]. Many of the participants in this study lived in ZIP codes in Alabama and around the Birmingham area. The homogeneity of this sample may have, therefore, led to the observed trends. This association should be evaluated in a more geographically heterogeneous sample.
This study has several strengths. First, it provides initial evidence of the benefits of examining the association between cancer and dementia progression in a more externally representative population, but even larger studies are still needed with decreased likelihood of selection bias. Additionally, participants came from an unselected ambulatory clinic population so external validity also includes individuals seeking care for dementia rather than those meeting entry criteria for an AD observational study. Previous studies have shown that approximately 75% of AD patients in the clinic are not eligible for clinical trials or observational studies, so use of a clinic population further improves generalizability of the current results [59, 60]. Secondly, it utilizes diagnoses of cancer rather than self-reported cancer history, reducing information bias. This study was also able to assess several potential covariates such as comorbidities, anticholinergic burden, and cardiovascular risk factors, which limits the possibility of residual confounding. This study examined individuals at the dementia stage rather than at early, mild stages of impairment, which expands upon our prior analysis. This study was also able to examine interaction by important racial and socioeconomic variables.
Despite its strengths, this study is not without limitations. First, this effect was observed among patients with any cancer. While specific cancer types were evaluated, sample size for each group was relatively small. Similar analyses with larger sample sizes of specific cancers are needed. Secondly, timing of cancer diagnosis relative to dementia diagnosis may be somewhat inaccurate. Some of these patients may not have received cancer care at UAB, so their cancer diagnosis may have been entered into UAB’s EHR at their first encounter to UAB’s health system, which may have been for a separate health issue. Also, patients with cancer may have received many different treatments and may have been diagnosed at different cancer stages, but many did not have complete cancer treatment or staging information. Treatment and staging may be an important confounding factor in this association which are unavailable in the EHR. A follow-up analysis is planned to assess specifics of cancer treatment on dementia progression in this sample. Some participants may have been taking dementia-related medications prior to dementia diagnosis, as they may be prescribed earlier in the disease process [61]. Furthermore, it was not possible to know the specific type of dementia for a subset of participants. Frequently, these dementias are billed as dementia NOS, rather than the specific subtype. The chart review does alleviate some of these concerns because most of the 10% review sample diagnosed with dementia, NOS had specific subtypes noted in their chart notes. Despite about 23% still not having discernable subtype listed, it is not expected that this would alter results, as these participants were diagnosed with a dementia syndrome. Also, identification of BMI was not perfect as many were not performed on the dementia diagnosis date. We restricted measurements to within one year of diagnosis to minimize this limitation, similar to the one-year timeframe for identification of comorbidities used in administrative claims-based studies [62, 63]. Identification of smoking was also imperfect as many were not performed on the dementia diagnosis date and many were greater than one year out from the diagnosis date. However, smoking categorization as ‘ever’ or ‘never’ smoker addresses some of this limitation. Additionally, some individuals in the other cancer group may have had two or more other types of cancer. Moreover, cancer diagnoses or diagnoses of comorbidities could still have been missed due to lack of documentation in the diagnosis list, problem list, or tumor registry, resulting in information bias. This could be non-differential between cancer groups and would bias results away from the null. It is expected that those seen and treated at UAB were present in the diagnosis list and/or tumor registry, but those who received cancer care outside UAB may not have been documented in the record. Finally, some medications used as a component of the depression identification algorithm may overlap with treatment of pain in cancer patients and/or hot flashes in breast cancer patients. However, pain is also a known contributor to both cognitive impairment and depression so it is not expected to considerably alter the results [64, 65]. If so, this would be non-differential and bias results toward the null.
Conclusion
CRCI can have negative effects on patients’ well-being, but the longitudinal association between CRCI and dementia progression has been understudied. Expanding on our previous work, we found that baseline cognition is significantly higher and cognitive decline slower in those with a history of cancer compared to those without. These results per year were clinically significant prior to adjusting for potential confounders, and it appears that smoking and comorbidities play a role in attenuating the association. Though, over time, become clinically significant despite the role of smoking and comorbidities. Further explorations on the reasons for this underlying association are needed, such as studies including more socioeconomic variables/geographic variability, information on cancer staging and death information for competing risk, and larger samples of specific cancer types.
Footnotes
ACKNOWLEDGMENTS
The authors would like to acknowledge and thank Ayme Miles with the Informatics Institute in the School of Medicine at the University of Alabama at Birmingham for assisting with obtaining and compiling data from the electronic health record.
M. Fowler received support for this project from NIH R01 AG057684 (R. Kennedy, PI). M. Fowler is currently funded by Agency for Healthcare Research and Quality 5T32HS013852. N. Wright is supported by K01AR068400.