
Abstract
Alzheimer’s disease (AD) is the leading cause of cognitive impairment in the elderly. Recent evidence suggests that preventive interventional trials could significantly reduce the risk for development of dementia. Periodontitis is the most common dental disease characterized by chronic inflammation and loss of alveolar bone and perialveolar attachment of teeth. Growing number of studies propose a potential link between periodontitis and neurodegeneration. In the first part of the paper, we overview case-control studies analyzing the prevalence of periodontitis among AD patients and healthy controls. Second, we survey observational libraries and cross-sectional studies investigating the risk of cognitive decline in patients with periodontitis. Next, we describe the current view on the mechanism of periodontitis linked neural damage, highlighting bacterial invasion of neural tissue from dental plaques, and periodontitis induced systemic inflammation resulting in a neuroinflammatory process. Later, we summarize reports connecting the four most common periodontal pathogens to AD pathology. Finally, we provide a practical guide for further prevalence and interventional studies on the management of cognitively high-risk patients with and without periodontitis. In this section, we highlight strategies for risk control, patient information, dental evaluation, reporting protocol and dental procedures in the clinical management of patients with a risk for periodontitis and with diagnosed periodontitis. In conclusion, our review summarizes the current view on the association between AD and periodontitis and provides a research and intervention strategy for harmonized interventional trials and for further case-control or cross-sectional studies.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is the leading cause of cognitive decline affecting millions of people worldwide [1]. Symptoms usually occur at in the 60s and 70s of patients, starting with the loss of episodic memory functions, impairment of visuo-spatial skills, and orientation difficulties. AD is characterized by the pathologic accumulation of hyperphosphorylated tau neurofibrils and amyloid plaques in the neural tissue leading to progressive neurodegeneration [2]. Histology and molecular studies revealed that the pathologic process starts with the formation of extracellular amyloid deposits, and it leads to changes in the production, phosphorylation, cleavage, and elimination of tau. The proposed phenomenon is known as the amyloid cascade theory [3]. A relatively novel idea that the early changes in the misfolding process of pathologic proteins are highly influenced by inflammatory mechanisms shifting the anti-inflammatory processes into a pro-inflammatory state. It is defined as the inflammatory hypothesis of AD [4]. Seemingly, only 1–3%of AD cases are characterized by the mutation of a single gene typically leading to prominent changes of amyloid metabolism and resulting in the familial forms of AD [5]. In most patients, genetic risk and environmental factors both contribute to the pathologic process.
While the deterioration of cognitive abilities is currently not treatable, growing body of evidence proposes the beneficial effect of personalized interventional therapy on the prevention of AD. A 2-year Finnish multidomain interventional trial applying diet changes, regular exercise, cognitive training, and monitoring of cardiovascular risk factors demonstrated that personalized intervention can significantly improve or maintain the cognitive functions of elderly individuals [6]. This has been reinforced by a meta-analysis of population-based European and American studies founding that approximately 30%of AD cases is caused by modifiable conditions including diabetes, midlife obesity, midlife hypertension, depression, smoking, physical inactivity, and low educational background [7]. Additional but less known factors might be important contributors as well such as kidney disease [8], hearing loss [9], sleep apnea [10], anxiety [11], early menopause [12], and epileptic seizures and epileptiform activity [13]. Oral diseases might be potential candidates due to the high population prevalence and the interaction with inflammatory mediators [14].
Periodontal disease or periodontitis (PD) is the most common oral condition affecting approximately 20–50%of human population [15]. PD is a chronic inflammatory disease of the periodontium resulting in loss of perialveolar ligaments and alveolar bony material. This process is primary related to the accumulation of pathogenic bacteria in subgingival dental plaques [16]. The continuous inflammation results in apical migration of the gingival junction forming periodontal pockets serving as continuous reservoir for the pathogenic bacteria. PD progresses slowly and long-term outcome depends on the speed of bacterial accumulation of the dental plaques [15]. Untreated PD may lead to chronic inflammation and increased tooth mobility [17]. The risk factors of PD are shared with AD in a large extent including aging, smoking, female hormonal changes, diabetes, obesity, and chronic stress [1, 15]. While it can easily lead to tooth loss and therefore significantly affecting the quality of life, it also associates with numerous physical conditions. A meta-analysis of 9 studies found that PD increases the risk of cardiovascular disease with 19%and the elevation is more prominent at the age > 65 reaching 44%relative risk [18]. A prospective cohort study analyzing 628 subjects identified that diabetic patients with severe PD have 3.2-times elevated mortality in a 11-year follow-up [19]. Observational studies also found that PD patients have a significantly higher risk for developing chronic kidney disease [20], respiratory diseases [21], and gastrointestinal cancers [22]. Since AD and PD share many risk factors and they associate with similar chronic physical conditions, it is intriguing to analyze their potential connection in the pathophysiology of AD.
The aim of the current opinion review is to summarize the results of studies on the prevalence of cognitive decline among patients with oral diseases and prevalence of PD in AD patients. Furthermore, we also highlight the possible pathologic mechanisms linking PD and AD with the description of the potential bacterial candidates. We also propose exact promising therapeutic approaches with a practical guide, potentially serving as a basis for further interventional studies.
PREVALENCE OF ORAL DISEASES IN ALZHEIMER’S DISEASE
Patients with cognitive decline have a higher chance for impaired physical condition since neurodegenerative diseases like AD significantly affect self-care, motor, and autonomic functions. This leaves us with patients who are either unable or uninterested in carrying out daily hygienic tasks and in addition, some pharmacological treatment given to AD patients decrease salivary flow and increase risk of dental caries as well as xerosotomia and candidiasis [23]. In our analysis on the existing literature, we searched studies identifying periodontal (or unhealthy dental state in general) status in AD patients. A search for “Periodontitis” and “Alzheimer” in PubMed yielded 171 results (years 2000–2020), and we selected papers for review based on the following inclusion criteria: 1) case-control studies with at least 40 subjects; 2) papers with meta-analysis method; 3) compared subject groups consist of healthy controls versus patients with AD spectrum disease (AD or amnestic type mild cognitive impairment (MCI)); 4) original peer-reviewed articles published in academic journals with impact factors. Cohort or cross-sectional studies were not included. We preferred the case-control design since databases on AD patients and healthy controls containing dental records are barely available. 13 studies (10 case-control and 3 meta-analysis) met the proposed criteria.
A case-control study [24] including 70 AD patients and 36 healthy controls reported that tooth loss in the AD group was 2.5-times more frequent than in the control group, and AD patients had 3 times more filled teeth and dental caries than the control group. It was found that the age and presence of AD were strong predictive factors for diminished condition of oral health. Poor periodontal health was also observed in the AD group compared to healthy controls [24]. Another study [25] investigated the oral health of 154 patients with neurocognitive decline (ranging from MCI to AD) and concluded that PD was associated with early cognitive impairment and AD, highlighting the increased number of deep periodontal pockets (OR = 8.43) and dental caries (OR = 3.36) in the neurodegenerative cases compared to controls [25].
A handful of systematic meta-analysis papers have recently been published to help determine whether the available evidence supports the higher incidence of PD in dementia [26–29]. A study of Gusman et al. [27] analyzed 4 reports (3 case-control and 1 cross-sectional) revealed significantly higher occurrence of PD in dementia; however, with the removal of the cross-sectional report, results appeared non-significant. The report of Maldonado et al. included 5 studies (3 case-controls and 2 cross-sectionals) and demonstrated that AD patients show significantly worse periodontal variables [28]. A recent paper from Asher et al. analyzed 16 studies and demonstrated that partial tooth loss was associated with high risk of cognitive impairment. It also states that the overall quality of evidence is low [29]. These reports agreed that most of the reviewed studies conducted only a point-analysis with various dental methodology, so it was impossible to rule out the deterministic role of impaired dental status in cognitive impairment. They also concluded that well designed, large sample size, longitudinal studies were needed to confirm the correlation between the development of AD and presence of PD [30].
In one such longitudinal study [31], the serum IG levels of bacteria (recognized as PD pathogens) were measured in 219 subjects. Although it is known that the physiological antibody responses to periodontal bacteria are influenced by many different factors beyond the clinical periodontal status (such as race/ethnicity, smoking habits, and likely also unmeasured health behaviors), the study found that patients with cognitive decline had higher serum IgG levels to common periodontal microbiota [31].
All case-control studies (see Table 1) compared cognitively impaired individuals to healthy controls with group comparisons focusing on dental status as dependent variable. All converge on a consensus of declined periodontal health in patients with AD spectrum disorders compared to their age matched controls. The cited reports used mostly retrospective approach and did not analyze cognitively normal patients with PD in a prospective follow-up. It should be noted that all studies propose statements regarding the need for further investigation, mainly prospective longitudinal to reveal the role and importance of PD in the progression of AD.
Summary of case- control studies analyzing the presence of periodontitis in Alzheimer’s disease spectrum patients
AD, Alzheimer’s disease; MCI, mild cognitive impairment; SCD, subjective cognitive decline; PD, periodontitis; CRP, C-reactive protein; IL-6, interleukin 6; MMSE, Mini-Mental State Examination; CI, cognitive impairment.
RISK OF COGNITIVE DECLINE IN PATIENTS WITH ORAL DISEASES
Oral diseases like caries, PD, oral cancers, oro-dental trauma, cleft lip and palate, and noma pose a prominent health burden for all countries, affecting approximately half of the human population [39]. Oral diseases frequently associate to higher occurrence of many physical conditions [15] and seemingly to neurological disorders as well.
To fully understand the causative direction of PD-AD link, the frequency of cognitive decline in patients with decreased oral health but normal cognitive status must be investigated. If AD patients were found to have a higher incidence of periodontal characteristic (as it was shown in the previous section of this paper), but we cannot find an increased rate of cognitive decline among patients with known oral diseases, we cannot attribute the inflammatory component of PD to the neurocognitive decline. To investigate this link, from the 171 previously described results we selected studies using the following criteria: 1) matched-cohort or cross-sectional observational studies with at least 40 subjects; 2) papers with meta-analysis method; 3) compared subject groups consist of healthy controls versus patients with PD; 4) original peer-reviewed articles published in academic journals with impact factors. We preferred the matched-cohort or cross-sectional observational design since large databases containing dental records are available on cognitively normal individuals. Twelve studies met the proposed criteria (see Table 2). Studies with meta-analysis were not available.
Summary of matched-cohort and cross-sectional observational studies analyzing the risk of cognitive decline in patients with oral diseases
CP, chronic periodontitis; AD, Alzheimer’s disease; PD, periodontitis; PI, periodontal inflammation.
Six studies applied retrospective approach. A nationwide population based matched-cohort study analyzing cognitive decline in patients with confirmed dental diseases was conducted in Taiwan. This impressively large study [40] included 9,291 patients aged 50 + who had been newly diagnosed with chronic PD. This sample was compared to 18,672 patients without PD, matched according to sex, age, and index years (1:2 ratio). Both groups were followed from the index date until the diagnosis of AD, death, or 31 December 2013. While the study found that there is no significant difference between the groups regarding 1-year risk of AD development after chronic PD exposure, 10-year PD CP exposure was associated with a 1.707-fold increase in the risk of developing AD [40]. The Third National Health and Nutrition Examination Survey (NHANES-III) containing medical data of 2,355 individuals revealed that high level of Porphyriomonas gingivalis (P. gingivalis) antibody was significantly connected to lower performance on delayed verbal memory (OR: 3.01) [41]. A second analysis of the same cohort examined the relationship between oral health indicators (gingival bleeding, loss of periodontal attachment, loss of teeth) and cognitive function (measured with Symbol Digit Substitution Test, Serial Digit Learning Test and Story Recall test) among 5,138 participants. After covariate adjustment, gingival bleeding and loss of periodontal attachment was associated with impairment in digit substitution performance and gingival bleeding was connected to decreased ability of digit learning [42]. An impressively robust report of the National Health Insurance Service-National Health Screening Retrospective Cohort database of South Korea analyzed 10,115 patients with chronic PD and 10,115 age- and sex-matched control subjects. Severe PD was significantly associated to increased risk for AD (hazard ratio (HR):1.08) and other forms of dementia (HR: 1.24 for vascular dementia and 1.16 for mixed dementia) [43]. A report on the analysis of the Korean Longitudinal Study on Cognitive Aging and Dementia (KLOSCAD) included 441 participants and demonstrated that higher number of functional teeth and functional occlusal units were associated with lower odds ratio (OR) of cognitive impairment (OR: 0.955 and 0.9, respectively) [44]. A Danish report analyzing 70-year-old individuals found that subjects with periodontal inflammation, with lower number of teeth have lower mean of Digit Symbol and Block Design score [45].
Six prospective studies are available. A report of Stein et al., analyzing the results of Nun study involving 144 individuals, demonstrated that lower number of teeth (range 1–9) associate with faster decline in cognitive scores measured with Delayed Word Recall test [46]. The Veteran Affairs Dental Longitudinal Study followed 597 participants during 32 years with a regular, 3-yearly repeated dental examination. Each tooth loss per decade was associated with increased decline in Mini-Mental State Examination Score (HR: 1.09). Alveolar bone loss (HR: 1.03) and probing pocket depth (HR: 1.04) had an accelerating effect as well [47]. A serum antibody experiment using the Biologically Resilient Adults in Neurological Studies database examined 158 participants. 81 developed dementia and 77 remained cognitively intact in the years of follow-up. Baseline antibody level against Fusobacterium nucleatum and Prevotella intermedia was significantly increased among individuals developing dementia [48]. A cross-sectional analysis nested within a study community dwelling elderly resident in South Korea revealed that fewer number of teeth was significantly connected to higher risk for developing AD in a 2.4-year follow-up [49]. A French observation in the region of Gironde following elderly at the age of 66–80 in a 15-year long period demonstrated 1.13 adjusted HR for number of missing teeth > 11 [50]. A study of Okamoto et al. examined 2,335 cognitively intact individuals in a 5-year long prospective setup and found 1.02 OR for mild memory impairment per 1 tooth loss at baseline [51]
While there is a clear need for further longitudinal follow-up studies on patients with dental diseases, the above studies already indicate that dental disorders might contribute to the development of cognitive decline. Unfortunately, studies with meta-analysis on the risk of cognitive impairment among patients with PD are not available. Since PD affects an estimated 11.2%of the world’s population [52], individual effect of PD should be analyzed in longitudinal studies.
THE POTENTIAL LINK BETWEEN ORAL DISEASES AND NEURODEGENERATION
There are a few explanations that connect a chronic peripheral inflammatory disease to degeneration of the neural system, but two have been placed as the central pillars of the neuroinflammatory hypothesis connected to oral microbiome. These are (1) local invasion of pathogens in the central nervous system (CNS), and (2) bacteria related effect of inflammatory proteins and activated microglia inducing amyloid cascade.
Local invasion of pathogens
In 1884, Robert Koch formulated the famous Koch’s postulates [53], which allowed microbiologists ever since to produce absolute proof that a specific microorganism causes a specific disease, revolutionizing the field of microbiology. However, with our advancing knowledge of human pathology, especially multifactorial diseases, we now know that Koch’s postulates do not hold for chronic diseases of possible microbial etiology, or for those that are multifactorial in origin. When considering diseases that begin taking effect at advanced age, a pathogen acting earlier in life might cause its damage via a “hit-and-run” mechanism [54] or could eventually be present only at a low concentration beneath the threshold needed to identify the organism at all. In multifactorial diseases, the causative organism might be missing if the disease is caused by some other factors [54]. Since AD is a multifactorial disease, it is intriguing to analyze the presence of specific bacteria whit a potential biological background to participate in the neurodegenerative process.
Two routes by which it might be possible for pathogenic bacteria present in the oral cavity to enter the CNS are thought to be the intravascular route and via peripheral nerves. Evidence gathered for these routes has been obtained from studies associating each specific organism with AD and will be described in further detail in the “High risk pathogens” section of this paper. Bacteraemia of oral origin can occur during many daily dental’s and nondental manipulations, and when pathogenic members of the microbiota are released from their microenvironment, they can migrate through our systemic circulation intracellularly. Under the intravascular route, we can point at monocytes or macrophages for functioning as vehicles that transport the pathogens into the CNS. Maclnyte et al. [55], showed that monocytes infected with periodontal pathogens can stimulate transendothelial entry of monocytes through human brain endothelial cells, via upregulation of adhesion molecules on both receptor and cell. When Chlamydia pneumoniae infected a cell sample, researchers witnessed an increase in expression of adhesion molecules such as ICAM-1 and VCAM-1, and similarly bacterial colonization of monocytes increased integrin (LFA-1 and MAC-1) expression. With these two key components increased because of alerted molecular expression, a 3-fold rise in migration of monocytes was detected through this blood-brain barrier model. Data collected in a study on the topic [56], suggested that a compensatory response was observed to maintain barrier integrity at the adherent junction, where downregulation of junctional proteins increased permeability. A 72-hour measurement of these proteins was done [56] and found that permeability changes were transient. These finding suggest that an increased chance of transmigration of monocytes through blood-brain barrier, could be the cause of neurodegeneration.
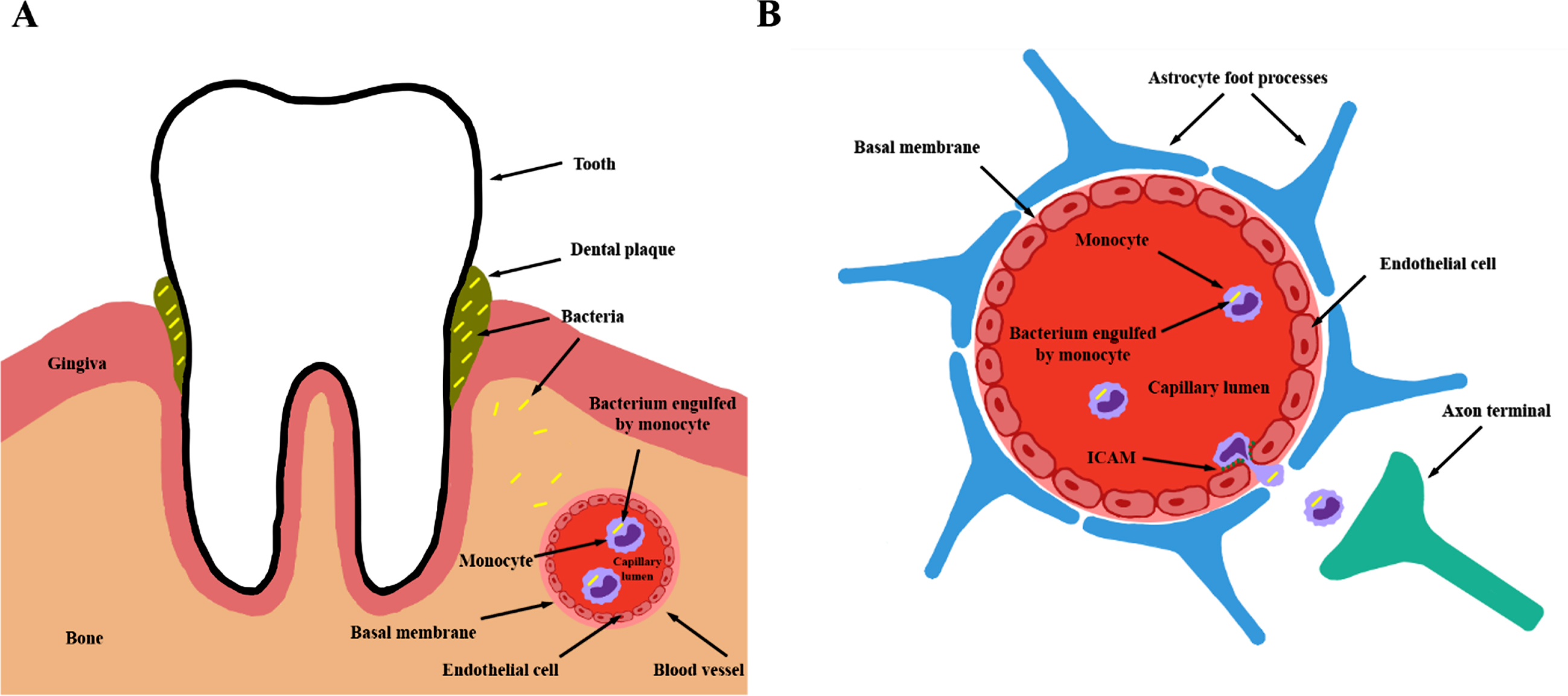
The intravascular route for bacterial invasion of central nervous system. A) Periodontal bacteria are able to invade alveolar capillaries and monocytes serve as transportation vehicles between alveolar and cerebral arteries. B) Infected monocytes could overexpress adhesion molecules like ICAM resulting in accelerated transendothelial entry of periodontal bacteria to neural tissue through blood-brain barrier.
The entry of pathogens to the CNS via the peripheral nerve route has been illustrated in Riviere’s studies that showed that certain spirochete species were detected in the trigeminal ganglia and pons, highlighting the ability of oral bacteria to invade CNS via peripheral nerves [57]. This suggestion is supported by finding oral treponemas in the trigeminal ganglia in both AD and control patients [58, 59]. Treponemas were found to be concentrated in foci and their histological location was identified by PCR analysis. Although the initial point of entry cannot be determined, a suggestion has been laid forth that Treponema originating from the oral cavity can invade both peripheral nervous system and CNS [58]. Another study supporting this hypothesis was investigating the immune infiltrates in the brain induced by peripheral stimulation. This was done by injecting L. monocytogenes into the oral mucosa of mice and goat. After just 6 days, 47/65 (72%) of mice developed signs of CNS inflammation. Further investigation found mononuclear infiltrations all along the entire trigeminal nerve from the lips to the medulla [60].
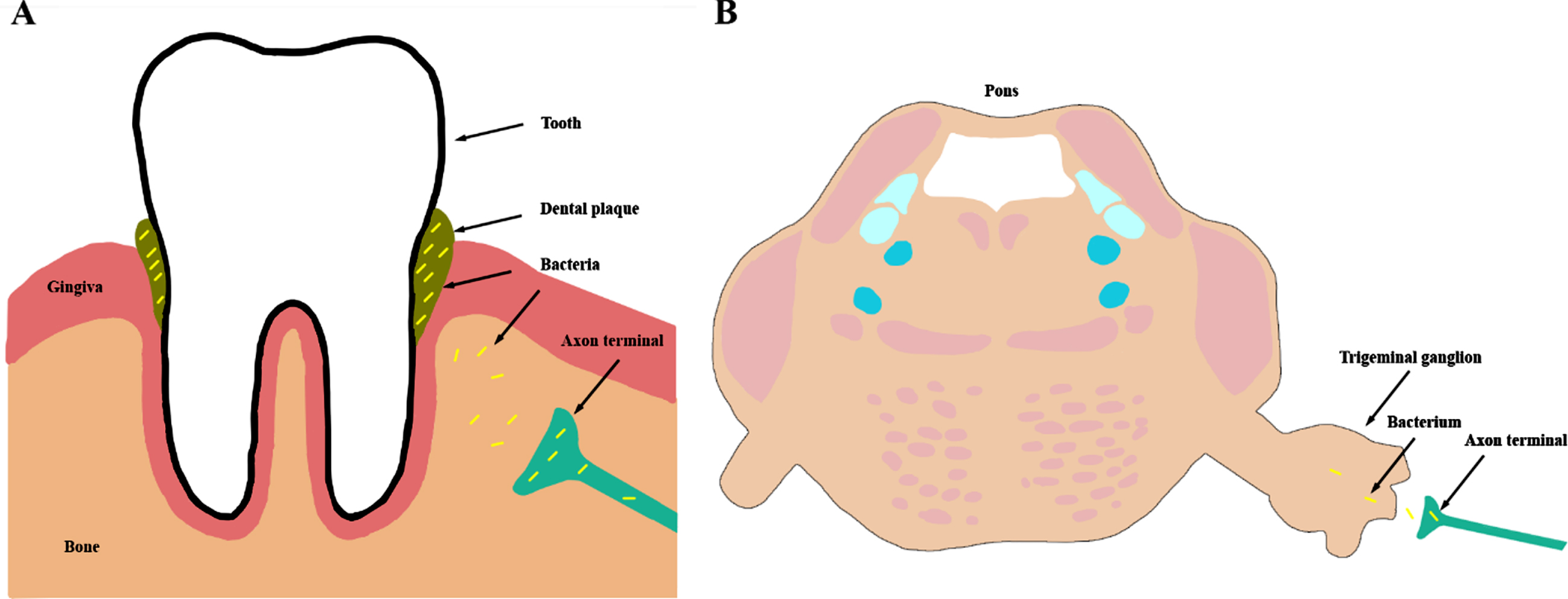
Peripheral neural route for bacterial invasion of central nervous system. A) Red complex bacteria of periodontal plaques invade axon terminals. Alveolar tissue is highly innervated by sensory branches of trigeminal nerve. B) Fibers of trigeminal nerve terminate in intracranial ganglia providing an ideal environment for the survival of periodontal bacteria. Ganglionic axons could serve as a potential route toward the brain stem nuclei for bacterial invasion.
Once in the brain, periodontal bacteria that are rich in lipopolysaccharides (LPS) are capable of stimulating cytokine production and further potentiating AD neuropathology mechanisms, such as priming of microglia in response to amyloid-β (Aβ), dysregulation of amyloid-β protein precursor (AβPP) and Aβ and initiating a neurotoxic loop [61] that changes from physiological to pathological when the intended neuroprotective functions of glial cells contribute to exacerbation of AD pathology. The presence of primed (activated) microglia can be attributed to either local or systemic inflammatory responses. These primed microglia are hypothesized to be a key part of AD neuropathology via inducing a higher production of inflammatory mediators and chronic overreaction to subsequent stimuli [62].
Over prolonged periods of time, such as those during chronic PD infections, the presence of pathogenic bacteria in the CNS can increase the levels of inflammatory products that may directly contribute to neurodegeneration via injury of surrounding noninfected cells resulting in in neuronal loss [63].
Inflammatory amyloid cascade and oral pathogens
As suggested earlier, a second mechanism exists through which periodontal pathogenic bacteria can induce further neurodegeneration and propagate AD in the brain. This mechanism does not include invasion of pathogens into the CNS directly, but the same effect is achieved through a PD derived increase of inflammatory molecules in the brain.
Cytokines are known to play a key role in any inflammatory response, and this is true for the neuroinflammation involved in modulating CNS function in AD pathology. These cytokines are relatively large hydrophilic molecules that cannot cross the blood–brain barrier directly and as such their action on the brain cannot be direct but requires intermediate molecules. The way these cytokines affect brain function has been studied intensively over the past decade. Activation of vagal afferents by cytokines offers a rapid signaling mechanism into the CNS, and this suggestion has been moved to the front of the possible mechanisms list with studies done on c-fos expression and vagotomy experiments [64]. When considering cytokine-induced hypothalamic-pituitary-adrenal axis activation, peripheral cytokines have been proposed to activate the nucleus of solitary tract via vagal afferents, this message continuing to the paraventricular nucleus of the hypothalamus through a noradrenergic pathway [65]. However, a totally exclusive neural transmission cannot account for the fact that elimination of brain cytokines repeals the key aspects of the acute phase response (such as behavioral depression or fever). It has therefore been proposed by Danzer et al. 2000 [64] that activation of the vagal afferents by peripheral cytokines will induce a brain cytokine message that is responsible for the neuroinflammatory response. There is now sufficient evidence [64] to accept that cytokines can enter the brain from circumventricular organs (bypassing the blood-brain barrier) and the choroid plexus and propagate throughout the brain by extracellular diffusion to reach their target cells. It is now tempting to suggest that the humoral pathway is responsible for the passage of cytokines into the brain and the function of the neural pathway is to further sensitize and modulate target brain areas to increase or alter the effects of diffusing cytokines [64].
The host response triggered by PD results in increased levels of inflammatory molecules such as TNFα, IL1β, IL6, IL8, and CRP. We will not go over the role of each specific chemokine in the inflammatory amyloid cascade hypothesis of AD but refer readers to a great review on this topic that was published by [66]. However, it is worth mentioning that TNF- α, IL-1, and IL-6 play a role in inducing cleavage of AβPP into Aβ, and that the mere presence of Aβ plaques increase the local concentration of these inflammatory cytokines, resulting in a feedback cascade that propagates AD. Since these cytokines may act on already primed glial cells resulting in an amplified reaction, we can piece together the “Amyloid Cascade Hypothesis” with the “Neuroinflammatory Hypothesis”. A test of this combined mechanism would require examination whether PD affects the progression of AD regarding time or severity. According to the model proposed by Kamer et al. [57], periodontal bacteria induce production of pro-inflammatory cytokines and C-reactive protein (CRP) which stimulate glial cells to produce Aβ42 and hyperphosphorylated tau protein which results, in further production of inflammatory molecules. Thus, a vicious circle is established by the double role of these cytokines in activating pathways leading to neurodegeneration [57].

The systemic inflammatory mechanism of periodontal bacteria induced neurodegenerative process. A) Bacterial lipopolysaccharides released from gingival plaques induce systemic immune response resulting in the elevation of numerous cytokines as IL-6 or IL-8. B) Cytokines may leak into neural tissue in circumventricular organs, where blood-brain barrier is absent. Chronic neural presence of cytokines could lead to a constant activation of microglia resulting in changes of amyloid clearance mechanism. Long-term stimulation of microglia associates with increased formation of extracellular amyloid plaques. Parallelly, cytokine level increases in neural tissue due to the release from microglia. The described process terminates in a vitious circle where cytokines stimulate microglia, and it releases more cytokines. Overactivation of microglia results in increased amyloid burden and amyloid plaques serve as stimulator of microglial cells.
Activated microglia (over)release many inflammatory mediators in the brain including cytokines, prostaglandins, and acute phase proteins. The dysregulated handling and metabolism of Aβ aggregates and AβPP is of paramount importance in AD pathogenesis. A peripheral inflammation such as periodontitis can increase cytokine production that alter the regulation of AβPP and Aβ. Griffin et al. [67] suggested that IL-1 is critical to the processing of AβPP and tilts the scale on the function of microglia to ensure continued Aβ deposition and the cyclical continuation of inflammatory response and cytokine overexpression [63]. The local CNS levels of IFN-gamma and TNFα are also increased during chronic systemic inflammation or during bacterial colonization of CNS tissue. These inflammatory mediators also trigger Aβ peptide production and alter the metabolism of Aβ and AβPP, in addition to inhibiting soluble AβPP secretion [68]. Beta-secretase, a protease that is responsible for cleaving AβPP into its toxic Aβ peptides, was shown to have its concentration increased by local inflammatory mediators [69].
In the above-mentioned vicious cycle Aβ aggregation further triggers the activation of microglial cells which in response produce acute-phase proteins, complement components, prostaglandins, and cytokines that further stimulate Aβ production and aggregation. This response may be more injurious than the plaques and tangles to which inflammatory processes are responding, resulting in neural damage [63]. To further increase the devastating potential of this neurotoxic loop, other proinflammatory cytokines such as IL-6 and TNF-α can stimulate further Aβ production, aggregation, and toxicity [63].
HIGH RISK PATHOGENS
An observational study conducted on patients with both active chronic PD and AD, suggested that after a 6-month period, a significant decline in cognition was found among AD patients with periodontitis in comparison to AD patients without active chronic PD, suggesting a link between neural degeneration and the presence of periodontal pathogens [14]. When attempting to correlating AD with PD, we should try to pinpoint the specific bacteria that provide a connecting link. In a consensus report written in 1996, P. gingivalis, A. actinomycetemcomitans, and T. forsythia were reported to be the three critical periodontal pathogens [70]. A study was even conducted in 2009 suggesting elevated levels of TNF and antibodies against these three bacteria were found in patients with AD (72%of AD subjects were found with at least 1 antibody compared to 38%of control) [71]. Another study claimed PD to be a polybacterial consortium focusing on P. gingivalis, T. denticola, and T. forsythia, and a claim for correlation between these “red complex pathogens” to AD was strengthened through many studies conducted in the past decades observing more oral pathogens (or inflammatory signals that mediate oral-inflammation) in AD patients’ CNS [70–72]. Since the above mentioned four bacteria form the “red complex” pathogens of PD, we highlight studies on these in relation to AD.
Spirochetes (Treponemas)
Spirochetes are well-known and defined periodontal pathogens with 60 different species of Treponema observed in subgingival pockets of patients with diagnosed periodontitis [73]. We can estimate that spirochetes account for 10%of the bacterial diversity found in host tissue in a periodontal environment, and when accounting for inflamed pockets, Spirochetes as a group account for 20%to 50%[74]. This number changes between individuals, where characteristics such as socio-economical background or even host genetics have a key role in the precise composition of the microbiome [75].
PCR analysis of 16 AD brains found six different periodontal Treponemas (T. denticola, T. pectinovorum, T. vincenti, T. amylovorum, T. maltophilum, T. medium, and T. socranskii) in 14 of the studied brain, while only 4/18 of controls [58]. T. denticola and T. vincenti were found in a statistically significant portion of PD patients as opposed to normal subjects [76, 77]. In addition, newly observed spirochetes were also found in these samples (T. pecitonovorum and T. socranskii) [74]. It is important to note that when assessing what subtype of spirochete would be a key component in the PD and AD link, we must consider a possibility of coinfection of multiple treponemas, and that they exhibit frequent pleomorphism in host tissue [58, 78].
The effects of Treponemal spirochetes on human brains have been investigated for a while (the first paper was published in 1913), with Treponema pallidum in its atrophic form suggested to be a major cause for slowly progressive dementia, cortical atrophy, and even local amyloidosis in the brain of general paralysis cases [79]. In another study, 60 patients with atrophic general paresis were analyzed and a correlation was found between an increase in spirochetes and spirochetal plaques (mostly hippocampal and frontal cortex), and the severity of cortical atrophy [80]. Treponema infections can increase TNF productions by macrophages, with spirochetal lipoproteins having a key role in both local and systemic inflammation induced by the bacteria. In such treponema mediated inflammations, CRP and serum amyloid A levels were elevated [81], with increased CRP being correlated statistically to AD and dementia in a 25 year follow up study [82].
To establish a bacterial link between PD and AD, evidence must be found of periodontal pathogens in confirmed AD patients. In a meta-analysis, in 91.1%(451/495) of AD patients were positive for Spirochete markers, while all 185 control samples were negative [73]. A strong statistical correlation was shown between AD and oral Treponemas, not only because there was a much higher prevalence of Treponema DNA found in the brains of AD patients than controls, but there was also a much more diverse range of Treponemal species [60]. While Spirochetes offer a possible bacterial link between low grade oral inflammatory disease and AD, more research is needed to finalize a conclusion.
Porphyromonas gingivalis
Periodontal tissue is known to exhibit a wide range of bacterial species. Strong evidence has accumulated to suggest that P. gingivalis is a key player in PD. P. gingivalis can be found with greater frequency and at elevated levels in diseased sites [83–86]. In one study, 301 patients were examined, and a significant correlation was shown between the prevalence of P. gingivalis and periodontitis. Among PD patients 79%(103/130) tested positive for the pathogen, in contrast to 25%(46/181) positivity of healthy patients [87]. Statistical analysis suggested that the odds ratio for being infected with P. gingivalis was 11.2 times greater in patients with periodontitis than the control group.
P. gingivalis is known to be a very resilient pathogen, which might explain why even a low amount in the brain for a duration of over 3 decades could be enough to contribute to local inflammation [88]. Two key molecules that are essential for the survival of P. gingivalis and its pathogenicity are Kgp and RgpA/B. They are known to play a critical role in the inactivation of host defense, nutrient acquisition, and host colonization. In a study published in 2019, 53 middle temporal gyri samples from AD brains were analyzed and 51 (96%) tested positive for RgpB and 49 (91%) for Kgp [89].
In a study conducted to examine the possible relation between P. gingivalis and AD, in mice infected with oral P. gingivalis the production of Aβ plaques was increased and colonization of the bacteria in the brain could be spotted [90]. Another study found that in 4/10 AD postmortem brain sections labelled with mouse anti-P. gingivalis, strong cellular attachment to the surface membrane was observed, as opposed to none in the normal brains. This might be considered a cause of AD patients having an increased risk of secondary chronic infection with P. gingivalis [91].
LPS from P. gingivalis had been shown in AD brains but not in non-AD brains [91]. It has been suggested that P. gingivalis and gingipains (trypsin-like cysteine proteinases) play a key role in the pathogenesis of AD by demonstrating their presence in rat brain [79] and showing that in vivo gingipain inhibitors block gingipain-induced neural decline, as well as significantly reduce host Aβ1–42 response to P. gingivalis and decrease the bacterial load in the mouse brain [90].
In one study [92] finalized in 2019, 20 AD patients were examined for mental status and oral microbiota. Significant association between salivary presence of P. gingivalis and a lower score on the Mini-Mental State Examination (MMSE) was found [92]. To further strengthen the claim that P. gingivalis is a key mediator between PD and AD, a periodontal infection model in an ApoE4 -/- mice was used [93] and it was shown that P. gingivalis is more efficient and effective in accessing the CNS than T. denticola and T. forsythia.
Aggregatibacter actinomycetemcomitans and Tannerella forsythia
In 1996 a consensus report [70] set out to determine which are the core periodontal pathogens, and two of the bacteria named in this report due to their common occurrence in PD patients were T. forysthia and A. actinomycetemcomitans.
Fast forward to the year 2019, and a group of Korean researchers have suggested the exact molecular mechanism through which Actinomycetecomitans causes its neuroinflammatory effects [94]. Injection of this pathogens outer membrane vesicle was shown to increase expression of TNF-α in mouse brain [94]. The correlation between AD and TNF-α levels was established a decade earlier when Kamer et al. [71], showed that AD patients have elevated levels of this inflammatory marker. The alteration in host gene regulation (mainly via microRNAs that originate from the outer membrane vesicle of the pathogen) in response to the presence of A. actinomycetecomitans indicates a possible pathway of how a pathogen specific systemic inflammation would increase the burden of neuroinflammation [94].
The function of cytokines and chemokines in AD has been listed in the work of Lee et al. [95]. If our goal is to connect the neurodegenerative effect of these cytokines to the increased presence of them in response to a systemic bacterial assault, we need to find a potential increase of inflammatory markers in response to Periodontal pathogens. One study from 2015 showed that A. actinomycetecomitans causes severe cytokine release in macrophages and induces cell death [96]. The mechanism for this was proposed to be via activation of NLRP3, an inflammasome prone to activation from microbial stimulus. NLRP3 was also shown to play a role in the alteration of macrophage phenotype and influence Aβ deposition, both pathognomonic for AD [97]. As a conclusion to the finding of the inflammasomes role in neural decline, the Actinomycetecomitans –caspase 1- NLRP3 axis was suggested to represent a possible novel therapeutic option for AD [97].
Aside from inflammatory markers, antibody levels can also be used to assess the effect of pathogens on the neural decline seen in AD (or MCI) patients. One study [98] focusing on a group of bacteria (including A. actinomyetecomitans) showed that antibody levels of AD patients at baseline were matching the levels found in chronic periodontitis patients. This demonstrated that, possibly, elevated antibodies levels years before cognitive decline could be a potential marker for AD [98].
Díaz-Zúñiga et al. [98], were studying the serotype of A. actinomyetecomitans that has the strongest effect on the CNS. This is especially important since the same report [70] that stated that A. actinomyetecomitans is widespread in most PD patients, also claimed that some types of A. actinomycetemcomitans have a closer relationship with destructive periodontal disease than other clonal types. Serotype B was found to be that one that induces the largest inflammatory response in microglia or hippocampal cell cultures [98]. Actinomyetecomitans serotype B LPS was shown to induce neural shrinking and increase extracellular Aβ1–42 formation, both characteristics of AD.
It is commonly accepted today T. forsythia constitutes a part of the “red complex pathogens” that form the most pathogenic bacterial complex in the oral cavity [72, 99]. When quantifying these bacteria, a group of researchers studied 40 patients [100] with confirmed PD and found that T. forsythia was found in high amounts (60%) in the PD group compared to healthy controls. When subtyping periodontitis to different clinical groups, T. forsythia was found to be 4-fold higher in chronic periodontitis (the subtype of PD most relevant to the link between systemic inflammatory and neural degeneration) than in aggressive PD [100]. This chronic inflammatory response to the presence of T. forsythia is hypothesized to play a role in the propagation of AD [101].
CONCERNS ON THE ROLE OF PD IN COGNITIVE DECLINE
AD is a multifactorial disease where probably numerous physical conditions contribute to the pathogenesis [7–13]. Plenty of scientific studies linked cardiovascular diseases, metabolic disorders, depression, sleep problems, or epilepsy to the neurodegenerative process; however, the causative role is frequently questionable and the “which comes first” questions are barely answered [102, 103]. An important limiting factor for causability studies that there are plenty of overlaps between the described conditions and neurocognitive disorders. They frequently share similar genetic background: apo4 and MTFR are crucial genes in AD and cardiovascular diseases [104]; CALHM1 gene associates with higher excitability of hippocampal neurons and it is a genetic risk factor of AD [105]; 13 from 31 typical genes of major depression alternate with the known genes of AD [106]. Overlap could be demonstrated in the risk studies as well: hypertension is a well-known risk factor of heart attack and dementia according to the Framingham study [107] and CAIDE score studies [108]; while obesity associates with poor sleep quality and insomnia [109], it is a common risk factor of AD [110]. Furthermore, the common shared etiology is represented well the by the socioeconomic status of patients with the various proposed conditions. People with higher education and better financial and social background follow a healthier lifestyle and a more advanced self-attention including better nutritional quality (organic foods, low intake of omega-6 and simple sugars, higher vitamin intake), regular physical exercise regime, less amount of stress, better access to adequate medical examination and screening methods and they have more time to engage with various types of social activities to maintain and fuel cognitive functions. These people have lower chance for developing dementia and parallelly, they are more protected against cardiovascular or metabolic conditions [111].
Since there is a great overlap between the genetic background, risk profile and socioeconomic status of patients with dementia and with physical diseases, it is intriguing to postulate that the association between the described medical conditions and AD is only an epiphenomenon. However, not all the patients with midlife depression or severe cardiovascular diseases develop dementia [112]. Furthermore, patients with AD show highly variable risk profiles [113]. These observations suggests that the mentioned physical conditions might have a substantial or mild role in the neurodegeneration. According to the current scientific view, the mild synergistic role is the most acceptable [104]. It is also known as bidirectional relationship: while physical conditions can change the cleavage and elimination of toxic brain products, neurodegeneration associate with the destruction of functionally important brain areas resulting in the dysregulation of physiological processes (e.g., autonomic blood pressure regulation, sleep homeostasis, mood regulator neurotransmitter systems, hormone system). For instance, patients with AD suffer from various sleep disorders, seemingly patients with midlife insomnia show higher risk for dementia [114].
Similar questions are could be raised based on the previously reviewed studies on the association of PD and AD. They share common genetic profiles (e.g., polymorphisms of IL-6 and IL-10 genes are risk factors for both conditions) [115], similar risk factors are detected (e.g., obesity, aging, smoking) [1, 15] and poor socioeconomic status associate with higher prevalence of PD [116] and AD [117]. Studies analyzing AD patients regarding the prevalence of PD (Table 1) are not able to properly address the conceptualized concerns, since patients with AD probably dedicate less attention to oral hygiene and suffer from many comorbid physical conditions. Prospective cross-sectional studies analyzing the long-term cognitive profile of PD patients (Table 2) are better candidates; unfortunately, risk profiles and socioeconomic status of these patients were not reported. While currently the exact role of PD in cognitive decline is not addressable, some reports suggest plausible association. Since not all PD patients develop AD and there are great variabilities among PD patients regarding the risk factors and extent of dental inflammation [118], causative relationship might be hypothesized. Bases on the observations showing colonization of brain tissues with common PD pathogens, bidirectional, mild synergistic effect of PD seems to be feasible in the development of cognitive decline [119]. Likely, presence of PD could exaggerate other pathologic processes via the neuroinflammatory mechanisms resulting in various types of neuropsychiatric disorders (e.g., migraine, major depression, multiple sclerosis) [120], not AD only. To properly address the direction of causative role in cognitive impairment, unified reporting is mandatory for PD studies to generate numeric databanks for large sample statistical analyses.
CLINICAL RECOMMENDATIONS FOR PROSPECTIVE RISK ANALYSIS AND INTERVENTIONAL STUDIES
Although numerous reports link PD to cognitive impairment, no prospective PD intervention studies have evaluated dementia outcomes. A search for “Periodontitis” and “Alzheimer” and “Treatment” in PubMed yielded 77 results (years 2000–2020). Human studies or randomized clinical trials on the treatment of PD in the prevention of dementia are absent. However, based on prevalence studies and the inflammatory effect of PD, it seems reasonable to postulate that PD might represent an individual risk factor for the development of cognitive decline. Thus, we propose a clinical recommendation guide for further PD interventional trials in the prevention of dementia.
Patients with risk of dementia without a previous diagnosis of periodontitis
Recognition of high-risk patients
Recognition of high-risk individuals for further development of cognitive impairment is mandatory for modern health systems. Individuals without subjective decline on cognitive functions might represent a risk group for AD in the following cases: age > 65, family history of dementia, education years < 10, APOE4 carriers, smokers, diagnosis of atherosclerosis, hypertension, high level of low-density lipoprotein (LDL), high level of homocysteine, diagnosis of diabetes, midlife obesity [121]. Patients with a diagnosis of MCI have significantly elevated risk compared to previous subjects [122].
Patient information
Dental and medical professionals should strongly cooperate to increase compliance of patients and effectivity of potential dental care. Patients with a risk of dementia should be informed that poor dental health associates with increased risk for cognitive impairment. Importance of proper oral hygiene must be emphasized in all medical check-ups. Patients with known risk factors of dementia should consider a dental evaluation if they have not done so in the past 12 months (it is illustrated by a key point taken from the world cohort study [123] that the risk for developing dementia was 89%greater in those who had not seen their dentist within the last 12 months compared to those who had seen their dentist two or more times). Patients should be informed that PD is often asymptomatic and does not associate with systemic signs of infections (e.g., fever, flu like symptoms) or with prominent changes of blood test values (e.g., leukocytosis, significantly increased CRP). Patients should be also educated about the common physical signs of PD as swollen gums, bleeding gums (spontaneously or following brushing or flossing), pus between teeth and gums, increased space between teeth and gums, sensation of bad taste or bad oral odor, change in tooth sensation during biting, spontaneous oral pain or mastication associated oral pain.
Dental evaluation
Periodontal evaluation of patients with high dementia risk should include a comprehensive examination of periodontal tissues. Dental medical history should be updated. Presence of diseases associating to higher occurrence of PD (Chediak-Higashi syndrome, agranulocytosis, leukocyte adhesion deficiency, Down syndrome, Papillon Lefevre syndrome, cyclin neutropenia) needs special attention in dental records [124]. Plaque and bleeding on probing (BoP) should be assessed by trained examiners, probing depths, and clinical attachment level (CAL) should be recorded and both full-mouth and site-specific stability should be determined. Radiography (dental status x-ray) should be applied in all suspicious cases to detect potential bone loss. Oral hygiene instruction regarding appropriate frequency, technique and use of potential aids such as interdental brushes should be tailored to patients’ needs individually.
Intervention procedures should be performed to prevent biofilm formation, which is the major cause of chronic PD. This is best achieved by replacing insufficient restorations having leakage and/or overhangs, thereby creating cleansable surfaces. Reducing plaque retention can be reached by restoring natural tooth contour and contact points with the necessary restorations. Once the pro-plaque accumulating factors are eliminated regular professional dental hygiene treatment can help in maintaining the oral health at an acceptable level without having acute and chronic inflammation.
Risk control
Risk profile of PD should be recorded by medical and dental check ups yearly. The following risk factors must be included: smoking, diabetes, family history of PD, obesity, depression, physical inactivity. Evaluation might be performed in a cooperation with dementia care professionals using standardized diagnostic tools for mood (e.g., Geriatric Depression Scale, Beck Depression Inventory, Hamilton Rating Scale for Depression) and physical inactivity (e.g., International Physical Inactivity Questionnaire, Global Physical Activity Questionnaire). Patients with a risk factor should be informed that they might have elevated risk for the development of PD.
All patients should be informed about the potential lifestyle intervention possibilities to prevent PD. Patients with a risk for dementia who smoke tobacco should discontinue this habit. Diabetes should be strictly monitored with regular blood testing (blood sugar level, Hemoglobin A1C) and properly controlled by a health professional trained in diabetes. Antidiabetic drugs having a potential beneficial effect in the prevention of cognitive impairment (intranasal insulin, metformin, GLP-1 agonist) should be prioritized [125]. Lifestyle interventions should be initiated in patients with obesity and physical inactivity. The nutritional intervention could be based on the Finnish Nutrition Recommendations since beneficial effect has been proved by many prospective interventional trials [126–127]. The exact nutrition protocol is characterized in the study of Souminen et al. [128]. Mediterranean diet or Dietary Approach to Systolic Hypertension could represent reasonable choices as well [129]. Intervention plan for physical exercise protocol could be based on the 2007 ACSM/AHA recommendations. The exact strategy is described in the paper of Nelson et al. [130]. Patients with low mood should be referred to trained psychologists or psychiatrists having experience in the prevention of cognitive decline. Behavioral therapy should be prioritized, and antidepressants might have negative adverse effects due to the increase of vascular events [131]. If antidepressant therapy is mandatory, citalopram might represent a reasonable choice since anti-amyloid effect has been proved in clinical trials [132]. However, long-term treatment beyond 12 weeks with antidepressants is not advised [133].
Patients with risk of dementia and a diagnosis of periodontitis
Patient information
Patients with newly diagnosed PD should be informed that there may be an increased risk for AD dementia. Patients should be informed that treatment for PD is available, and inflammation might be reduced but not completely cured. A plan to reduce the effect of possible contributors of PD (smoking, diabetes, obesity, low mood, physical inactivity) should be advised, as we have demonstrated in the “Risk control” section.
Classification and reporting of PD parameters
A consensus on the definition of periodontitis case is crucial. We propose to use the current consensus statement of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions [16]. PD could be identified in the following case: 1) interdental CAL is detectable at≥2 non-adjacent teeth, or 2) Buccal or oral CAL≥3 mm with pocketing > 3 mm is detectable at≥2 teeth. Further important criteria for case definition are that the assessed CAL is not associated with non-periodontal causes (gingival recession of traumatic origin, cervical dental caries, CAL on the distal surface of second molar associating with malposition or extraction of third molar, endodontic lesion draining through marginal periodontium, vertical root fracture). We propose to report if periodontitis occurs in a necrotizing form or associate with severe systemic diseases.
For risk analysis, description of PD status with a unified staging form is mandatory to estimate the contribution of periodontal disease in cognitive impairment. We propose to use a system based on the current staging protocol of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions (see Table 3). Our proposed score could be applied during dental visits, since the system includes easily administrable parameters measuring general PD risk as well. The major aim of the staging system is to estimate the severity of PD with measurable dental parameters and highlight parallelly the potential contributors of PD. The reporting protocol is based on the current recommendations of PD care and on the previously reported parameters of case-control and cross-sectional studies on the association of PD and AD.
Periodontitis reporting protocol for cognitive risk analysis studies and for prospective interventional trials. Severity could be reported with clinical attachment level (CAL), radiographic bone loss (RBL), and with tooth loss (TL). Reporting of exact numbers for CAL, RBL, and TL is advised to provide possibility for correlation analysis with cognitive and neuroimaging scores. Maximum probing depth should be reported too since it is frequently used in previous risk and cohort studies. Extent and distribution of PD should be reported too to create more numeric parameters for further statistical analysis. Type of periodontitis might distinguish various outcomes. Risk profile could be easily administered and helps to identify the common contributors of periodontitis and cognitive decline
Dental treatment
The aim of treatment of PD is to reach a stable, inflammation free stage of periodontium (supportive structures of teeth) to provide ability for proper tissue regeneration. During the treatment procedure called scaling, sites showing signs of stability or inflammation without disease progression must undergo supragingival removal. This can be done with a variety of tools and approaches. To minimize the number of bacterial deposits, the specific features that are likely to retain plaque and calculus should be eliminated. In addition, several additional measures are proposed to minimize plaque accumulation and inflammation, including additional antimicrobials and lasers. Indicators of active disease require retreatment including signs of inflammation (e.g., BoP) and an increase in CAL. Subgingival debridement is also recommended at sites greater than 4 mm regardless of signs of inflammation or recurrent disease, as the risk of relapse increases with deeper probing depth measurements. Periodontal healing occurred even in the presence of calculus, provided the subgingival bacterial plaque was removed. From this, we learned that although calculus removal is important because it is a major plaque-retaining factor, intentional removal of root material and contaminated cement is not necessary for successful treatment. Thus, the term root planing is often referred to today as debridement. Most studies in the 1970s and 1980s were conducted with hand tools, including curettes, scales, and hoes, and this was considered the gold standard. Since the 1990s, the use of powered instruments has become increasingly popular, claiming increased efficiency and effectiveness. Adverse effects after non-surgical removal may include patient discomfort, damage to the root surface, and sensitivity of the root surface. Excessive removal should be avoided at shallow probe depths (< 3 mm) to avoid trauma, subsequent loss of binding, and root surface sensitivity. In the treatment of deep pockets (probing depth > 6 mm), surgical procedures as open-wing debridement, should be considered since they might result in greater probe depth reduction and clinical binding gains. Flap surgery might help in the cleaning of vulnerable surfaces. With soft tissue graft techniques, gum recession could be significantly reduced, and we are able to cover exposed routes. In alveolar tooth loss, bone grafting helps to prevent tooth loss and serves as a platform for renewal of natural bone tissues. Guided tissue regeneration and tissue-stimulating proteins also support the regrowth of natural alveolar bone tissues. While there are variety of possible treatment strategies, re-evaluation of PD stages with the proposed protocol is mandatory to accurately report therapeutic effect in prospective interventional trials preferably in yearly basis. Changes in PD risk profile could be easily administered.
DISCUSSION AND CONCLUSION
AD is a devastating neurodegenerative disorder and the leading cause of cognitive impairment. Recent studies demonstrated that with early recognition and proper control of risk factors, we can significantly delay the occurrence of dementia or prevention of cognitive decline is also reachable. PD is the most frequent dental disease sharing many modifiable risk factors with AD.
Case-control studies revealed that PD has a higher prevalence among AD patients. However, recent meta-analyses propose that the exact role of PD in dementia is barely measurable since they differ significantly in the methodology, especially in the reporting protocol of dental status [29]. While plenty of prevalence studies use the periodontitis term [25, 38], exact definition of periodontitis is rarely described. Others analyze the occurrence of poor general dental health among dementia patients [24, 34]; however, they also reveal periodontal parameters like tooth loss or pocket depths. In case-control studies, analysis of periodontal bacterial linked inflammatory markers is also common [31–33, 35–36], but periodontal status is reported with various parameters or not reported at all. Matched-cohort and observational retro- and prospective studies clearly suggest the role of PD in neurodegenerative disorders. Unfortunately, meta-analysis studies are not available, and comparison of results is complicated since reports use different parameters to report PD status. Exact definition of PD is defined only in one of these studies [40], where severity or staging of PD is not reported. In many studies, diagnostic procedure to describe PD is not highlighted and PD severity is measured only with the number of teeth [43–47, 49–51]. Some studies measured serum antibody levels against PD bacteria without proper measurement of dental status [41, 48].
While there are large variety in reporting methodology by reports focusing on the link of AD and PD, physiology studies have revealed potential mechanisms for the periodontal bacterial contribution in neurodegeneration. Seemingly, pathogens of periodontal plaques can reach the neural tissue via an intravascular route with monocytes [55] or via the peripheral sensory alveolar branches of trigeminal nerve and its ganglia [58]. Systematic cytokine response for periodontal bacteremia was highlighted too [57], resulting in a vitious circle between cytokine release, microglia activation, and amyloid formation [68]. These possible mechanisms are reinforced by human studies finding elevated level of antibodies and cytokines against periodontal bacteria [31–33, 48] and by clinical reports showing elevated occurrence of red complex pathogens of PD in human brain tissues. Seemingly, four species have prioritized role in PD-linked neurodegeneration: Spirochetes [73], P. gingivalis, A. actinomycetans [98], and T. forsythia [102]. Based on the previously described observations, it is intriguing to plan further studies to analyze the role of PD in cognitive impairment and to measure the effect of PD treatment in interventional trials of AD. However, unified clinical strategy and reporting of PD status is mandatory to increase comparability and reproducibility.
In the current review, we provide a strategy to manage patients with elevated risk for dementia and without PD. Education of patients about PD, risk reduction and improvement of oral hygiene and promotion of dental visits might be crucial to decrease PD and dementia burden parallelly. Since risk factors of AD and PD highly overlap, these strategies serve well the prevention of both diseases. In patients with PD, uniformized reporting of dental and PD status could be key for further cross-sectional risk studies and interventional trials. We propose a PD reporting protocol (Table 3) containing the following features: 4-stage model for assessing severity based on three clinical parameters (CAL, RBL, TL); maximum probing depth to provide opportunity to compare results to previous reports; description of extent and PD type to reveal PD profile; and risk profile administrable by dentists. The proposed protocol is summarized in Table 4.
Summary of strategies in the management of high-risk individuals for cognitive decline with and without periodontitis
PD, periodontitis; BMI, body mass index; AD, Alzheimer’s disease; CAL, clinical attachment level; BoP, bleeding on probing; TL, tooth loss; RBL, radiographic bone loss.
In conclusion, we can propose that PD might be an important contributor of neurodegeneration. Further studies are needed with prospective follow-up to measure the impact of PD status on cognitive outcome. Strict reporting of PD parameters is mandatory to reveal exact effect of dental health and to make comparison available with established biomarkers of neurodegeneration (e.g., cerebrospinal fluid, neuroimaging, neuropsychology). Patients with high dementia risk might benefit from PD prevention and treatment strategies and these can be important contributors of prevention trials.
Footnotes
ACKNOWLEDGMENTS
Our research was supported by the National Brain Research Program I, II (KTIA_NAP_13-1-2013-0001; 2017-1.2.1-NKP-2017-00002); Hungarian Scientific Research Fund 2019 of the National Research, Development and Innovation Office (PD- 132652); Janos Bolyai Research Scholarship of the Hungarian Academy of Sciences (bo_78_20_2020); EU Joint Programme- Neurodegenerative Disease Research (JPND) project (National Research, Development and Innovation Office, Hungary, 2019-2.1.7-ERA-NET-2020-00006); New National Excellence Program of the Ministry for Innovation and Technology from the Source of the National Research, Development and Innovation Found (ÚNKP-20-5).