
Abstract
Background:
Dementia and hyperhidrosis (HH) are common in the elderly while there is little research to investigate the association between them.
Objective:
To clarify a possible association between HH and dementia in population of adults ≥65 years old in China.
Methods:
A cross-sectional survey for elderly adults ≥65 years old was conducted from April to December 2019. A total of 5,958 participants were analyzed after two phases investigation. Goodness-of-fit tests (Pearson and deviance) were used to estimate the dispersion parameter and examine the adequacy of the models. Logistic and linear regression analyses were used to evaluate the association between HH and dementia.
Results:
The overall prevalence of all-cause dementia was 10.17%, that of dementia with Lewy bodies (DLB) was 1.41%, and HH was 14.97%. Prevalence rates of HH were higher in participants with dementia and DLB. There was a significant positive relationship between HH duration and MMSE score (r = 0.207, p < 0.001, Durbin-Watson test = 1.806). Participants with HH were 1.275 (95% CI: 1.015–1.601, p = 0.037) times to have dementia, and 3.616 (95% CI: 2.267–5.767, p < 0.001) times to suffer from DLB than those without HH. Pearson and deviance chi square tests did not indicate overdispersion (p > 0.05 in the logistic regression models).
Conclusion:
HH was common in the Chinese population ≥65 years old. It can increase the risk of dementia, particularly in DLB, in the elderly. It is important to improve the awareness of HH among dermatologists and neurologists.
Keywords
INTRODUCTION
Hyperhidrosis (HH) is a disorder characterized by pathological excessive sweating in which the degree of sweating exceeds the physiological needs of body temperature regulation. HH may stem from a complex dysfunction of the autonomic nervous system (ANS), resulting in the neurogenic overactivity of otherwise normal eccrine sweat glands. HH affects patients’ quality of life, resulting in social and work impairments as well as emotional distress [1]. Frequency estimates from population-based studies typically range from less than 0.6% to approximately 5% [2, 3], but reached up to 16.7% in a study in Poland [4]. HH is classified as either primary or secondary. Approximately 93% of patients with HH are characterized as having primary HH, of whom > 90% have a typical focal and bilateral distribution affecting the axillae, palms, soles, and/or craniofacial areas. Secondary HH presents in a more generalized and asymmetric distribution and is caused by various underlying diseases or medications. Traditional perspectives include that HH is common among infants, teenagers, and young adults [1], primary HH is more common than secondary, and that females tend to be more susceptible. To date, symptom improvement of the clinical characteristics of HH in older adults has not been studied, particularly in China, and it remains unclear whether the incidence of HH is actually higher in females.
Dementia is one of the primary cognitive disorders associated with disability and mortality among elderly adults. The number of patients with dementia in China accounts for approximately 25% of the entire population, with the overall prevalence of dementia in Chinese people aged 60 years and older at 5.30% (4.30%–6.30%) [5], creating a large public health challenge. Recent studies revealed that there may be a reciprocal effect of ANS and dementia [6]. ANS dysfunction is associated with alpha-synuclein disease and is a common feature of Lewy body disease (LBD), represented by Parkinson’s disease (PD), dementia with Lewy bodies (DLB), and multiple system atrophy (MSA).
In a comparative study, using twenty DLB and twenty age-matched MSA and PD subjects, the Composite Autonomic Scoring Scale (CASS) sudomotor scores for DLB, MSA, and PD subjects were 1.6±1.2, 2.5±0.7, and 0.9±0.8 (p < 0.001), respectively, and ANS dysfunction was demonstrated to be frequent in those with DLB, with severity intermediate between that of MSA and PD. A cohort of 100 patients with PD demonstrated that earlier development of each ANS dysfunction or symptom was associated with a significantly higher risk of reaching a disease milestone and a shorter survival time [7]. Studies have shown that HH can impact life quality comparable to that seen in patients with chronic diseases, leading to higher rates of anxiety, depression, and other illnesses, but few people focus on the relationship between HH and dementia. Given that HH is a type of ANS dysfunction, it may be linked to the occurrence of dementia. Dementia and HH are two common diseases in the elderly, but the role of HH in dementia is currently unknown.
Therefore, the current study aims to explore the prevalence of HH in a Chinese population of subjects≥65 years old and to reveal the association between HH and dementia. This will promote HH being used as a clinical screening tool to help identify dementia and to provide strong support for improving awareness of HH.
MATERIALS AND METHODS
Participants
The current study is a cross-sectional, door-to-door, population-based survey conducted across 92 communities, aimed at investigating the prevalence of all-cause dementia and LBD in rural Ji County, China, from April to December 2019.
All eligible subjects included in the study were ≥65 years old, listed in the census of the community registry office, and had lived in the community for at least one year prior to the survey date. Those listed in the census but who were institutionalized were not included in the study. Excluding subjects who refused to participate (n = 114), were untraceable (n = 9), had mental disorders (n = 12), were deceased (n = 7), or did not complete the full questionnaire because of inadequate hearing, speaking, or vision (n = 232), a total of 5,958 participants were finally analyzed in this research.
The protocol for the current study was reviewed and approved by the ethics committee at Tianjin Huanhu Hospital (2019–40). Informed consent was obtained from each subject either directly or from his or her guardian.
Measurement
Figure 1 illustrates the processes of the door-to-door, two-phase survey, as well as the number of participants involved at each step.
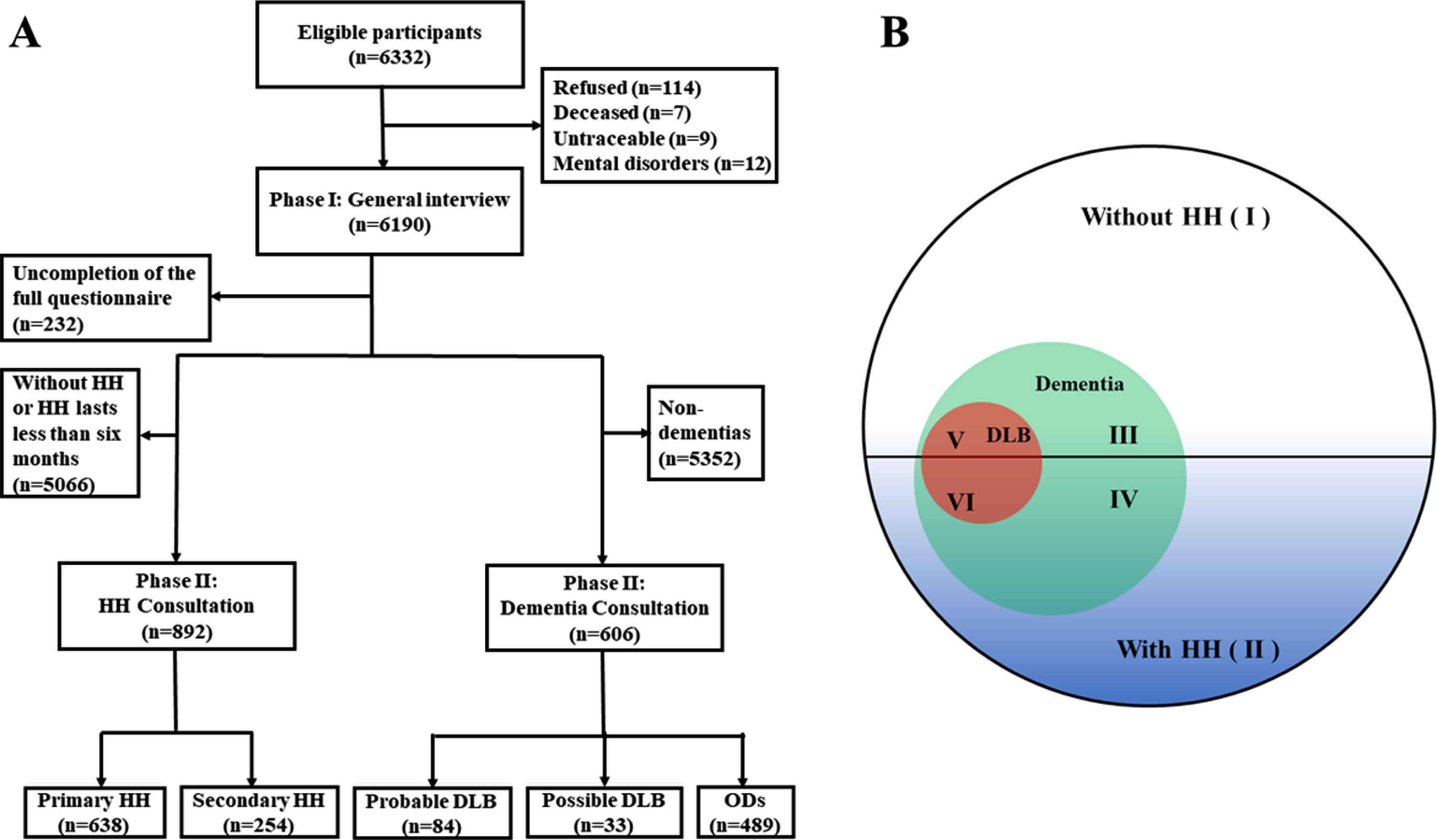
Flowchart (A) and the distributions of participants (B). In A, the flowchart of the survey with two phases was showed, to investigate the prevalences of dementia, dementia with Lewy bodies, and hyperhidrosis. The distributions of participants were shown in B: (I) 5,066 participants without HH; (II) 892 participants with HH; (III) 482 participants with dementia but without HH; (IV) 124 participants with dementia and HH; (V) 35 participants with DLB and HH; (VI) 49 participants with DLB but without HH. HH, hyperhidrosis; DLB, dementia with Lewy bodies; ODs, other dementias.
Phase I: General interview
A centralized medical examination at the health station and an in-person survey were conducted. Basic demographic characteristics such as gender, age, education, marriage status, and comorbidities, such as stroke, diabetes mellitus (DM), hypertension, as well HH symptoms and severity, were collected. The evaluations, including Scales for Outcomes in Parkinson’s Disease-Autonomic questionnaire (SCOPA-AUT) [8], the Chinese Mini-Mental State Examination (C-MMSE) [9], the Clinical Dementia Rating (CDR) scale [10], and the Activities of Daily Living (ADL) scale [11], were administered by qualified and experienced specialists in neurology, all of whom experienced the same training at Tianjin Huanhu Hospital in Tianjin, China.
Participants with C-MMSE score below the cutoff points 17, 20, and 24 points for participants who were illiterate, or had only undergone primary school or higher education, respectively) [12] and/or a CDR of 0.5 or higher, as well as any participants who responded “Yes” to items 17 or 18 on the SCOPA-AUT (referred to as the “with hyperhidrosis” group), were deemed eligible for phase II of the study.
Phase II: Consultation
For dementia. Participants who were eligible for phase II of the study were examined for the presence of all-cause dementia and/or probable DLB. Physical examination, blood tests (thyroid function, syphilis, HIV, and vitamin B12 level), and a neuroimaging examination [magnetic resonance imaging (MRI) or computed tomography (CT), if the participant could not undergo MRI] were arranged to obtain or rule out a diagnosis of dementia. Then, the records of all examinations above were evaluated again and, if the situation of the patient was complicated or the diagnosis of probable DLB was difficult to make, the patient underwent an 11C-PIB PET scan and an 18F-FDG PET scan. Diagnoses of probable DLB were confirmed blindly by two board-certified neurologists and, if there was disagreement between them, the subject was excluded.
For hyperhidrosis. All participants were asked about issues including the pattern of sweating, age of onset, possible initiating causes, duration (the course of HH), frequency, amount, distribution, night sweating, family history, and any symptoms pointing to a secondary cause. The Hyperhidrosis Disease Severity Scale (HDSS) [13] was used to rank the influence of sweating on everyday activities on a four-point scale. Participants who responded with a score of three or four were considered to have severe HH, while those who responded with a score of one or two were considered to have mild or moderate HH (see Table 1).
Severity of hyperhidrosis (HDSS)
Criteria for dementia, DLB, and HH
In the current study, dementia was diagnosed based on the Diagnostic and Statistical Manual of Mental Disorders IV criteria (DSM-IV) [14]. The diagnosis of probable DLB was conducted by using consensus criteria for DLB established in 2017 by McKeith et al. [15] with two or more core clinical features of DLB present, with or without the presence of indicative biomarkers.
Specific diagnostic criteria for primary HH consist of 6 months of visible focal sweating that exceeds thermoregulatory needs and at least two of the following: HH with a symmetrical bilateral distribution, disturbing daily activities, occurring more than once a week, having an onset before 25 years of age, having a positive family history, and lacking nocturnal symptoms. The diagnosis of secondary HH mainly includes an asymmetric, unilateral, or generalized distribution, nocturnal symptoms, onset after 25 years of age, and a negative family history. The underlying causes of excessive sweating are sufficient to differentiate between primary and secondary HH [16, 17].
Statistical analysis
All analyses were performed with SPSS version 25.0 (SPSS, Inc., Chicago, IL, USA). The prevalences of all-cause dementia, DLB, and HH were estimated for the entire study population. The prevalences and respective 95% confidence intervals (CI) according to five-year age groups and gender were also calculated. The age was classified as 65–69, 70–74, 75–79, 80–84, and≥85 years of age. Educational attainment was divided into five levels: 0, 1–6, 7–9, 10–12, and more than 12 years of education.
Continuous variables are expressed as mean [±standard diversion (SD)]. Frequency distributions were used to analyze the qualitative variables. The Chi-square and Mann-Whitney U tests were used to assess the clinical factors associated with the presence of dementia. Goodness-of-fit tests (Pearson and deviance) were used to estimate dispersion parameter and examine the adequacy of the models. Logistic regression was used to analyze the association between HH and dementias. And the linear regression (along with its 95% CI), and Durbin-Watson (DW) test were used to describe the association between HH duration and C-MMSE scores. Statistical significance, determined with 2-tailed, unpaired testing, was evaluated at p < 0.05.
RESULTS
Characteristics of samples
A total of 5,958 participants [3,385 (56.8%) females and 2,573 (43.2%)] males, with a mean age of 72.2±6.0 years old) were examined. Participants in groups with and without HH were significantly different from each other in terms of various variables (Table 2).
Demographic and Clinical variables of 5,958 samples
Num, number; HH, hyperhidrosis; Pro., proportions; DM, diabetes mellitus. †p-value means the comparation between “with HH” and “without HH”.
Prevalences of the all-cause dementia, DLB, and HH
Table 3 shows the prevalence rates of all-cause dementia, DLB, and HH according to age level. The overall prevalence of all-cause dementia was 10.17% (95% CI: 9.40%–10.94%), and the prevalence was much higher in females (14.89%, 95% CI: 13.69%–16.09%) and increased with advancing age. The prevalence of DLB in the total population was 1.41% (95% CI: 1.11%–1.71%) and that in the dementia population was 13.86% (95% CI: 11.10%–16.62%). Both of these prevalence rates were higher in females [2.07% (95% CI: 1.59%–2.55%) in total females, 13.89% (95% CI: 10.86%–16.92%) in dementia-affected females] and the age group of 80–84 [2.96% (95% CI: 1.57%–4.35%) in total females, 20.00% (95% CI: 11.32%–28.68%) in dementia-affected females]. The overall prevalence of HH in the total population was 14.97% (95% CI: 14.07%–15.88%), while it was 20.46% (95% CI: 17.24%–23.68%) in the dementia-affected population. The DLB-affected population had the highest prevalence of HH, at 41.67% (95% CI: 30.90%–52.43%). The prevalence of HH continuously decreased with age among the patients with dementia and DLB.
Prevalences of all-cause dementia, DLB and HH according to gender and age level
DLB, dementia with Lewy bodies; Pre., prevalence; CI, Confidence Interval; HH, hyperhidrosis.
HH characteristics in participants with dementia
As shown in Table 4, the 892 participants with HH reported that they had suffered from it for an average of 8.27 (±10.41) years, with a range from one to sixty years. In addition, 638 (71.5%) participants had primary HH and 254 (28.5%) secondary HH. Five hundred and eight (57.0%) participants with HH thought that their HH was noticeable, but that it did not interfere with their daily activities. Participants with HH and dementia (n = 124) had shorter HH duration (6.39±7.58 years) than those with HH without dementia (n = 768, 8.57±10.77 years, p = 0.002). Secondary HH was more common in participants with HH and dementia (n = 50, 40.3%), and participants with HH and DLB (n = 14, 40.0%).
HH characteristics in population with dementia
“Duration” means the course of HH by asking “How long do you have over sweating?” during the investigation. P1 means the comparation between “all HH samples” and “HH with dementia”; P2 means the comparation between “all HH samples” and “HH with DLB”; P3 means the comparation between “HH without dementia” and “HH with dementia”; P4 means the comparation between “HH without dementia” and “HH with DLB”; P5 means the comparation between “HH with dementia” and “HH with DLB”. Num., number; HH, hyperhidrosis; Pro., proportions; SD, standard deviation; HDSS, Hyperhidrosis Disease Severity Scale.
Associations between HH and cognitive performance
The associations between HH duration and cognitive performance are shown in Fig. 2. In all participants with HH, there was a significant positive relationship between HH duration and MMSE score (r = 0.207, p < 0.001, DW test = 1.806). However, in subgroups of HH subjects with dementia or DLB, these variables were negatively correlated, albeit not significantly.

The linear regression and 95% CI between HH duration and cognitive performance. The linear regressions and its 95% CI between the course of HH and MMSE scores were described in A–C by the dementia types, HH types and HDSS degrees, respectively. HH duration means the course of HH by asking “How long do you have over sweating?” during the investigation. HH, hyperhidrosis; 95% CI, 95% confidence interval; DLB, dementia with Lewy bodies; MMSE, the Mini-Mental State Examination; HDSS, Hyperhidrosis Disease Severity Scale.
It was also demonstrated that participants with HH were 1.536 (95% CI: 1.243–1.897) times more likely to have all-cause dementia than those without it (p < 0.001) and also had a higher risk after adjusting for covariance in different models (p < 0.05) in Table 5. In particular, HH had a large influence on the occurrence of DLB (OR = 4.263, 95% CI: 2.745–6.623, p < 0.001). Participants with HH were 3.616 (95% CI: 2.267–5.767, p < 0.001) times more likely to suffer from DLB than those without it, after adjusting for all covariance mentioned in Model IV. What’s more, we didn’t find overdispersion (p > 0.05 in the logistic regression models) by Pearson and deviance chi square tests (Supplementary Table 1).
Associations between hyperhidrosis and dementias in variable models
DLB, dementia with Lewy bodies; ORs, odd ratios; CI, Confidence Interval. *p < 0.05; **p < 0.001.
DISCUSSION
This is the first population-based study focusing on an elderly population in China to provide a reliable estimate of the prevalence of HH and its association with the risk of dementia. In the cross-sectional survey (n = 5,958) of elderly Chinese, the prevalence of HH was 14.97% (95% CI: 14.07%–15.88%), with a mean duration of 8.27 (±10.41) years. Those with dementia or DLB, particularly females, had a significantly higher prevalence of HH.
In this study, we found higher overall prevalence rates of all-cause dementia and DLB of 10.17% (95% CI: 9.40%–10.94%) and 1.41% (95% CI: 1.11%–1.71%), respectively, in the population aged ≥65 years, which are slightly higher rates than in our previous research [9, 18] and in a study in rural western Japan [19]. This could be explained by the older age of the target population in the current survey. We also found that the prevalence of DLB was 13.86% (95% CI: 11.10%–16.62%) among the dementia-affected population, and females showed almost the same proportion as males, which is consistent with previous reports [20, 21].
The prevalence of HH in elderly Chinese was much higher than previously reported among the Americans and Poles [4, 23]. In a study of 5,807 subjects between 5–64 years old conducted in Japan, Fujimoto et al. [24] provided questionnaires to companies and in schools and reported a prevalence of 12.76%. These different rates may be due to the various age ranges of the respondents, diagnostic criteria, investigating methods, and geographic disparities. However, a population-based survey in German adults reported a similar prevalence rate of 16.3% [25]. The study of HH worldwide primarily focuses on younger individuals, ignoring the needs of and emergence of HH in the elderly population [26]. An epidemiological study of HH in China, using 10,000 college students, showed a prevalence rate of 2.08% [27], with females and a positive family history demonstrating an increased risk for HH.
Generally, primary HH is reported more than secondary HH. The population with dementia or DLB had a higher proportion of secondary HH than those without dementia (with dementia: 40.3% versus 26.6%, p = 0.002; with DLB: 40.0% versus 26.6%, p = 0.080). Secondary HH is usually related to many diseases and the administration of numerous drugs. The population with HH and dementia was older than that with HH but without dementia, as well as having more comorbidities, which could increase the possibility of developing secondary HH and having it for a shorter duration. Moreover, the HH duration was significantly positive correlated with the MMSE score among the total HH population, while in the population with HH and dementia, these variables showed a negative correlation, although it did not reach significance. The subjects with dementia had older age, lower education level, and more comorbidities, which could cause secondary HH later in life. The severity of HH among the different groups was also investigated. The proportions decreased as the severity increased and showed no significant difference between the populations with or without dementia. Although more than half of the population with HH presented a mild or moderate form of the condition, there were numerous individuals with a severe condition, which requires medical attention.
HH was more prevalent in females than in males and the distribution of the population included in the current study was quite consistent with other studies. A recent study with 4,133 participants in Brazil reported prevalence of HH of 2.07%, with 60% of those affected being female [28]. Females may more frequently be accompanied by excessive stress [29], anxiety/depression [30], sleep disturbances [31], or complications of endocrine and metabolic disorders [32]. Moreover, females more frequently [33] seek treatment than males and are more inclined to complain about HH. In this study, elderly females, particularly those with dementia or DLB, had a significantly high prevalence rate of HH, although the potential mechanism linking HH and dementia remains unknown.
The involvement of central and peripheral neurons controlling autonomic function may manifest as orthostatic hypotension, thermoregulatory dysfunction, gastrointestinal dysmotility, and urogenital dysfunction with neurogenic bladder and sexual dysfunction [34]. Hyperactivity of the sympathetic nervous system is largely thought to be responsible for HH [35]. Indeed, de Oliveira et al. [36] identified a significantly higher number and apoptosis of ganglion cells in the ganglia of individuals with HH.
Alpha-synuclein accumulation in the form of Lewy bodies has been demonstrated in the brainstem (substantia nigra, locus ceruleus, etc.), limbic system (amygdala, transentorhinal cortex, and cingulate) and neocortex (frontal, temporal, and parietal) of patients with LBD [34]. There are extensive fibrous connections among the temporal lobe, frontal lobe, amygdala, and brain stem, which are involved in in regulating cognition, emotion, sleep, autonomic nervous system and other functions. The anterior cingulate projects to the anterior insula and subcortical autonomic nuclei and participates in different autonomic responses, while the amygdala projects to downstream effectors, including the hypothalamus and brain stem, for autonomic responses. The preoptic/anterior hypothalamic region is critical for thermoregulation. It contains heat-sensitive neurons that initiate responses for heat loss (sweating and skin vasodilation) and inhibits cold-sensitive neurons in the dorsomedial nucleus, which projects to the nucleus raphe pallidus to initiate responses for heat gain (skin vasoconstriction and metabolic thermogenesis). A cross-sectional analysis of PD subjects suggested that those with HH resembled the autonomic phenotype [31]. Lewy bodies have been shown in the hypothalamus of patients with PD. Clinically, patients with PD manifest thermoregulatory dysfunction with alterations in maintaining core temperature, as well as hyperhidrosis and hypohidrosis. Consistent with our previous hypothesis, HH was more common in elderly and increased the risk of dementia, particularly DLB, after adjusting for covariates. Few previous studies focused on the effects of HH (or the ANS) on dementia. In this study, participants with HH were found to be 1.536 (95% CI: 1.243–1.897) times more likely to have all-cause dementia than those without it (p < 0.001) and had greater influence on the occurrence of DLB (OR = 4.263, 95% CI: 2.745–6.623, p < 0.001).
Several studies have examined ANS dysfunction in subjects with dementia. The results in those with AD were controversial, while ANS dysfunction frequently occurred in alpha-synucleinopathies comprised cardiovascular, gastrointestinal, urogenital, and thermoregulatory disturbances [37]. ANS dysfunction supports the diagnosis of DLB [15] and is a prodromal feature in the diagnosis. In a study including 90 patients with probable DLB, 87.8% showed ANS dysfunction (particularly orthostatic hypotension) before or at the time of memory loss, with a duration of 1–9 years [38]. The pattern of dysfunction in DLB is similar to that in PD but generally more severe, placing the degree of autonomic failure in DLB on a spectrum between PD and MSA. In terms of the topographic sequence of the development of Lewy bodies, they first involve the amygdala, where they cause neuron loss. Deterioration of the structure of the amygdala may then lead to impaired connections with other brain regions, which can in turn affect autonomic nervous function. Hyperhidrosis may be a result of compensatory HH or dopaminergic medications in LBD [39]. Moreover, in the population with HH, anxiety/depression are common. Anxiety/depression is known to increase the risk of dementia by affecting the sympathetic and parasympathetic nervous systems, as well as the endocrine and metabolic systems. Increased sleep disturbances, which also happen to be responsible for HH, can also increase the risk of dementia. Further studies are needed to investigate whether HH and anxiety/depression share the same pathogenic pathway. DLB patients have more behavioral and psychiatric symptoms, along with a higher risk of anxiety and depression, than those with AD. They also suffer more from sleep disorders, including rapid eye movement sleep behavior disorder and excessive daytime sleepiness, which can increase the production of excessive sweat. HH is also more affected by other morbidities. Therefore, it is unclear if HH has an independent effect on dementia or if it increases the risk of dementia through other morbidities; this mechanism needs to be further explored.
The current study provides original information on HH and is the first to describe the association between HH and dementia in an elderly Chinese population. There are some limitations to this study. For example, the subjects are confined to the elderly in rural China, and the small sample size limits our further analysis, so we should expand the population to obtain more generalizable findings. Second, the study involved a cross-sectional design, limiting our ability to infer causality, which needs a prospective cohort. In addition, although we have information on the symptoms, we lack detailed data on medical examinations related to HH, so we cannot describe the etiology of HH. Finally, in this study, there is the possibility of recall bias on the duration of HH, although we obtained information on this from both the participants and their caregivers. Future studies more specifically and objectively evaluating the relationship between HH and dementia are warranted.
CONCLUSION
Elderly people presenting with HH are at high risk of dementia, particularly in DLB. HH might be a distinctive clinical feature to predict a future diagnosis of dementia. It is important to improve awareness of HH both in dermatologists and neurologists.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the National Natural Science Foundation [grant number 82171182], the National Key Research and Development Program of China [grant number 2016YFC1306305], Research Project of Tianjin Nursing Association [grant number tjh513lky2020YB05], Science and Technology Project of Tianjin Municipal Health and Health Committee [grant number ZC20121 and KJ20048].