
Abstract
Background:
Studies on plasma orexin-A levels in prodromal dementia with Lewy bodies (DLB) and the relationship with clinical manifestations are rare.
Objective:
To assess plasma orexin-A levels and evaluate the correlation with clinical features in patients with mild cognitive impairment with Lewy bodies (MCI-LB) and DLB.
Methods:
Plasma orexin-A levels were measured in 41 patients with MCI-LB, 53 with DLB, and 48 healthy controls (HCs). Informant-based history, neurological examinations, neuropsychological assessments, laboratory tests, and neuroimaging were collected and the correlation between orexin-A and various indicators evaluated.
Results:
Plasma orexin-A levels in patients with MCI-LB (1.18±0.33 ng/mL, p = 0.014) or DLB (1.20±0.44 ng/mL, p = 0.011) were significantly higher than in HCs (1.02±0.32 ng/mL) and associated with gender and age. DLB patients with fluctuating cognition (FC) (1.01±0.23 versus 1.31±0.50, p = 0.007) or parkinsonism (PARK) (0.98±0.19 versus 1.25±0.47, p = 0.030) had significantly lower plasma orexin-A levels than subjects without FC or PARK. Plasma orexin-A levels were significantly negatively correlated with irritability and UPDRS-III scores and significantly positively correlated with disinhibition scores.
Conclusion:
This is the first report in which elevated plasma orexin-A levels were observed in patients with MCI-LB or DLB. In addition, lower orexin-A levels were found in patients with DLB and FC or PARK compared with HCs. The plasma orexin-A levels were associated with the presence of core features and motor and neuropsychiatric symptoms in patients with MCI-LB and DLB.
Keywords
INTRODUCTION
Dementia with Lewy bodies (DLB) is the second most common type of neurodegenerative dementia, characterized by fluctuating cognition (FC), visual hallucinations (VHs), rapid eye movement sleep behavior disorder (RBD), and parkinsonism (PARK) symptoms [1]. Because the mechanism of DLB is controversial, the initial clinical manifestations can occur 15 years or more before the onset of dementia and the manifestations overlap with Alzheimer’s disease (AD), Parkinson’s disease (PD), and other α-synuclein-related syndromes, identification of core clinical features and early diagnosis of DLB present particular challenges [2].
argethispage2pt Orexin, consisting of orexin-A and orexin-B, is a neuropeptide synthesized by orexin neurons in the lateral hypothalamic area (LHA). In previous studies, a 25% reduction was reported in hypothalamic hypocretin neurons and Lewy bodies (LB) at early stage I in patients with PD, and over 60% reduction at advanced stage [3]. The neuropathological or cerebrospinal fluid (CSF) evidence indicated that orexin-A levels in DLB (mean level range: 240.3–521 pg/mL) were lower than in AD (mean level range: 256.8–474 pg/mL), higher than in frontotemporal lobar degeneration (FTLD) (mean level range: 245–258 pg/mL), and equal or lower than in normal elderly individuals (mean level range: 248.1–497 pg/mL) [4, 5]. Although significant positive correlation was observed between the severity of RBD and CSF orexin-A levels in patients with DLB in Inagawa’s cohort [6], which attempted to explore the potential relationships between orexin-A and the clinical symptoms of DLB, the results remain controversial and limited [7, 8]. Furthermore, the effects of orexin-A levels on mild cognitive impairment with Lewy bodies (MCI-LB) have not yet been investigated. The collection of CSF by lumbar puncture is more invasive and injurious than that of peripheral blood; collecting peripheral blood by venipuncture is more acceptable in routine clinical practice to evaluate the orexin-A levels. Currently, the relationship between plasma orexin-A and clinical symptoms has been preliminarily-explored in PD [7], sharing the same α-synuclein neuropathological with DLB, suggesting that plasma orexin-A levels were increased in early- and medium-stage PD, and were correlated with the non-motor symptoms of PD, whereases studies on plasma orexin-A in DLB and MCI-LB are blank.
Therefore, in the present study, the plasma orexin-A levels in patients with prodromal DLB were investigated for the first time. In addition, the correlation between plasma orexin-A levels and clinical manifestations was evaluated to determine the effects of orexin-A in patients with early stage DLB and identify new evidence of the potential mechanisms underlying DLB pathophysiology.
MATERIALS AND METHODS
Study participants
The present study included 41 patients with MCI-LB, 53 with DLB, and 48 healthy controls (HCs) recruited from December 2020 to December 2021 at the cognitive impairment clinics, Beijing Tiantan Hospital, Beijing, China, a center in the China Lewy Body Disease Collaborative Alliance.
Diagnoses were confirmed by two specialists and if there was disagreement, the subject was excluded. A probable DLB diagnosis can be made with two or more core symptoms with or without indicative biomarkers, or only one core symptom with one or more indicative biomarker, according to the 2017 criteria by McKeith et al. [1]. Probable MCI-LB was diagnosed if a patient had two or more core LB symptoms with or without the presence of a proposed biomarker [positive FP-CIT SPECT or dopamine transporter (DAT) PET, and/or meta-iodobenzylguanidine (MIBG) scan, and/or polysomnographic confirmation of REM sleep without atonia], or only one core clinical feature plus one or more proposed biomarkers [9]. Both MCI-LB and DLB showed relative preservation of medial temporal lobe structures on MRI/CT, while patients with MCI-LB preferred to have insular thinning and gray matter volume loss on MRI. Additionally, 37 patients (29 patients with MCI-LB, eight patients with DLB) underwent FP-CIT SPECT or DAT PET, 14 patients (nine patients with MCI-LB, five patients with DLB) underwent MIBG scan, and 54 patients (30 patients with MCI-LB, 24 patients with DLB) underwent polysomnography. Totally, 23 patients (17 patients with MCI-LB, six patients with DLB) showed reduced dopamine transporter uptake in basal ganglia, nine patients (five with MCI-LB, four patients with DLB) demonstrated reduced MIBG uptake on myocardial scintigraphy, and 46 patients (24 patients with MCI-LB, 22 patients with DLB) with RBD were confirmed by polysomnography. Objective cognitive impairment is based on the scores from neuropsychological measures that are typically 1 to 1.5 standard deviations (SDs) below the mean for their age- and education-matched peers on culturally appropriate normative data. A global Clinical Dementia Rating (CDR) score≤0.5 points indicates preserved daily and social functioning [9]. Exclusion criteria were as follows: diagnosis of any neurological disease except MCI-LB or DLB; currently using orexin receptor antagonists; patients with hearing loss, aphasia, or an inability to complete a clinical examination or scale assessment; history of mental disorders and illicit drug abuse; patients with acute or chronic liver and kidney dysfunction, malignant tumors, or other serious underlying diseases. HCs were recruited from friends and relatives of the patients and had no history of psychiatric or neurological illness or evidence of cognitive decline.
The study was designed and conducted in accordance with the Declaration of Helsinki, received ethical approval from the Beijing Tiantan Research Ethics Committee, and written informed consent was obtained from all participants.
Clinical assessment
All participants underwent a standardized diagnostic workup that included a semi-structured medical history interview, collection of an informant-based history (including demographic characteristics, lifestyles, comorbidities, family history of cognitive impairment, course of memory loss, and body mass index (BMI, kg/m2)), clinical and neurological examinations, neuropsychological assessments, laboratory tests (blood and/or CSF samples), and neuroimaging tests (structural imaging of MRI/CT, and/or PET CT, SPECT), as previously described [10, 11]. Neuropsychological assessments included the Mini-Mental State Examination-Chinese version (C-MMSE), the Montreal Cognitive Assessment (MoCA), and CDR used to evaluate global cognitive function and severity of cognitive impairment. The Activities of Daily Living (ADL) was used to measure the functional status. Neuropsychiatric features were assessed with the 12-item Neuropsychiatric Inventory (NPI) using the information provided by the caregiver.
The core clinical features of DLB were assessed using the questionnaire and physical examinations based on consensus [1, 12]. VHs were systematically assessed using a sub-scale of the NPI, with specific reference to the occurrence of VHs to exclude hallucinations in other modalities (e.g., auditory hallucinations) [13]. PARK was considered present when the neurological examination showed extrapyramidal signs (tremor, bradykinesia, and/or rigidity) and measured using UPDRS-III [14]. All patients with PARK underwent clinical evaluation during the off-medication phase. RBD was rated as present according to caregiver reports stating the patient appeared to “act out” their dreams and were moving extensively during sleep and measured using the RBD screening questionnaire (RBD-SQ) or polysomnography [15]. Fluctuations including spontaneous alterations in cognition, attention, and arousal were rated positive according to the patient or caregiver complaints of changing during the day and over weeks, then assessed using the One Day Fluctuation Scale (ODFAS) and the Clinical Assessment of Fluctuation (CAF) scale, respectively [16].
Sample collection
After a 12–14 h overnight fast and between 07 : 30 and 08 : 30 am before breakfast, peripheral blood from each participant was collected by venipuncture into 6 mL EDTA-containing test tubes. Immediately (within 2 h) after collection, blood was centrifuged (2,200 rpm, 10 min) and stored at –80°C until measurement. Smoking, alcohol consumption, and vigorous activity were prohibited 24 h before the study.
Measurement of plasma orexin-A levels
Plasma orexin-A levels were measured using an enzyme-linked immunosorbent assay (ELISA) kit (EK-003-30; Phoenix Pharmaceuticals, Burlingame, CA, USA). The detection range of this kit is 0–100 ng/mL, with a sensitivity of 0.2 ng/mL, and the intra- and inter-assay variability were < 10% and < 15%, respectively. Samples were analyzed twice on the same plate and the concentration values obtained from all samples were within the detection linearity range (0.12–2.0 ng/mL) of the kit.
APOE genotyping
Genomic DNA was extracted from peripheral blood stored at –80°C and the APOE gene was amplified using polymerase chain reaction (PCR). The following PCR primers were used: 5′-AGGAACAACTGACCCCGGT-3′ (upstream) and 5′-TGCTCCTTCACCTCGTCCA-3′ (downstream). Each amplification reaction contained 1μL DNA, 1μL primers, 1μL 10% dNTP, 5μL Taq Buffer, 5μL 25 mM MgCl2, 0.5μL Taq DNA polymerase (5 U/μL), and 35.5μL double-distilled water. The thermal reactor was programmed as follows: initial denaturation at 94°C for 3 min, 35 cycles at 94°C for 30 s, annealing at 57°C for 35 s, extension at 72°C for 40 s, and final extension at 72°C for 10 min. The amplification product (50μL) was purified using a product purification kit (SK 1141). The purified product was sequenced using ABI 3730xl DNA analyzer. All genotypes were determined without knowledge of the patient status.
Statistical analyses
Descriptive analyses were conducted using frequency for qualitative variables and mean (±SD) or median (Q25, Q75) for quantitative variables. To assess differences among the HCs, MCI-LB, and DLB groups, Student’s t-test was performed to compare two independent groups for normally distributed data and Mann-Whitney U test was used for nonparametric data. Qualitative variables were assessed using a chi-squared test. Because the cut-off value of plasma orexin-A has not been determined, in the present study, the median point of the HCs (i.e., median split, median = 0.92 ng/mL) was used as the cut-off point and the values above the cut-off point were considered elevated. The proportion of elevated plasma orexin-A level was recorded by number (%). Logistic regression (odds ratio, OR) with 95% confidence intervals, CIs) was used to analyze the associations between elevated plasma orexin-A levels and related factors as shown in Table 2. The Spearman’s correlation was used to evaluate the correlation between the plasma orexin-A level and neuropsychological assessments. In the partial correlation analysis, gender and age were entered as covariates in three adjusted models.
Associations between elevated plasma orexin-A levels and related factors in variable modes by logistic regressions (OR, 95% CI)
BMI, body mass index; APOE, Apolipoprotein E; OR, odd ratios; 95% CI, 95% confidential interval. *p < 0.05, **p < 0.01, ***p < 0.001.
For statistical analyses, the IBM Statistical Package for the Social Sciences (SPSS) for Windows (version 25.0; IBM Corporation, Armonk, NY, USA) was used. A p-value < 0.05 was considered statistically significant. All tests were performed bilaterally.
RESULTS
Demographic data and clinical assessments in HCs, MCI-LB, and DLB groups
Group demographics and clinical assessments are summarized in Table 1. The three groups did not differ in terms of age, years of education, BMI, or comorbidities (including stroke, diabetes mellitus, heart disease, and hypertension). In the MCI-LB group, more participants were females than in HC (87.8% versus 50.0%) and DLB groups (87.8% versus 66.0%). In the DLB group, more patients were APOE ɛ4 carriers (41.5% versus 7.7%) and showed a longer course of memory loss (p = 0.001), lower C-MMSE (p < 0.001) and MoCA (p < 0.001) scores, higher ADL (p < 0.001), UPDRS-III (p = 0.109), and CDR (p < 0.001) scores as well as higher frequency of neuropsychiatric symptoms than participants in the MCI-LB group.
Sample characteristics
HC, healthy controls; MCI-LB, mild cognitive impairment with Lewy bodies; DLB, dementia with Lewy bodies; SD, standard deviation; BMI, body mass index; CI family history, cognitive impairment family history; APOE, Apolipoprotein E; C-MMSE, the Mini-Mental State Examination (Chinese version); MoCA, the Montreal Cognitive Assessment; ADL, the Activity of Daily Living Scale; CDR, the clinical dementia rating; NPI, the Neuropsychiatric Inventory; RBD, rapid eye movement sleep behavior disorder. a There were 41 participants in HC group, 39 patients with MCI-LB, and 41 patients with DLB having APOE genotype test. P1 means HC versus LB-MCI; P2 means NC versus DLB; P3 means LB-MCI versus DLB.
Plasma orexin-A levels in HCs, MCI-LB, and DLB groups
As shown in Fig. 1, plasma orexin-A levels in patients with MCI-LB (1.18±0.33 ng/mL, p = 0.014) or DLB (1.20±0.44 ng/mL, p = 0.011) were significantly higher than in HCs (1.02±0.32 ng/mL; Fig. 1a). The same findings were found after adjusting for gender and age based on linear regression models (MCI-LB versus HCs: coefficient β= 0.089, 95% CI: 0.019–0.159, p = 0.013; DLB versus HCs: coefficient β= 0.054, 95% CI: 0.002–0.107, p = 0.043). Overall, females had significantly higher plasma orexin-A levels than males (1.17±0.40 versus 1.05±0.30, p = 0.038; Fig. 1b) and overweight participants had significantly lower plasma orexin-A levels than subjects with healthy weight (1.05±0.39 versus 1.16±0.38, p = 0.041; Fig. 1d). Significant differences in age (Fig. 1c) and night-time sleep duration (Fig. 1e) were not observed among participants.
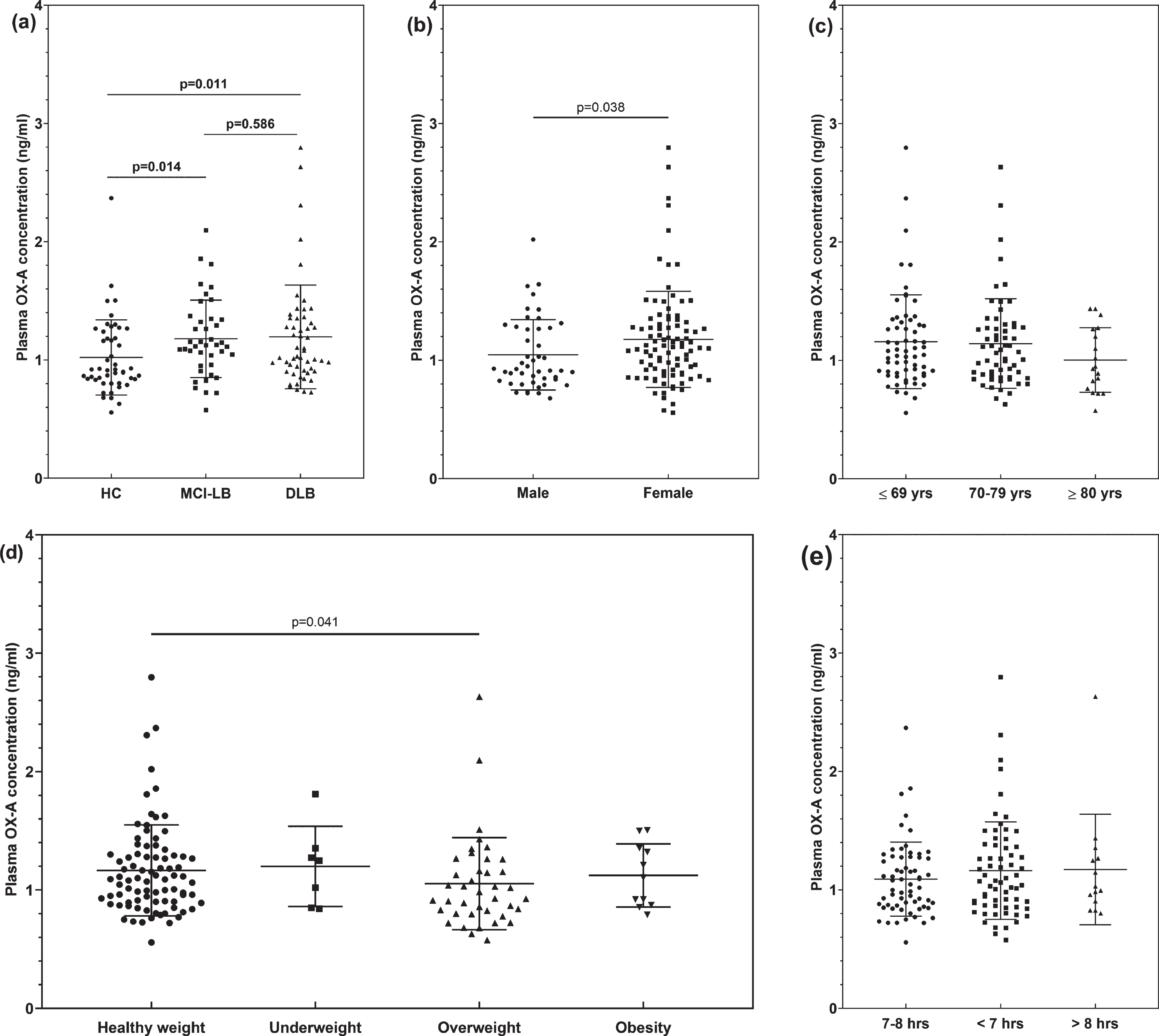
Differences in plasma orexin-A concentrations between HCs, MCI-LB, and DLB. (a) Plasma orexin-A levels in patients with MCI-LB and DLB were significantly higher than healthy controls. Participants were grouped according to gender (b), age (c), BMI (d), and night-time sleep duration (e), and each of these groups was compared each other by Mann-Whitney U test. All data are presented as the means±standard deviations. p-values are also showed in the figures. HC, healthy controls; MCI-LB, mild cognitive impairment with Lewy bodies; DLB, dementia with Lewy bodies; BMI, body mass index; OX-A, Orexin-A.
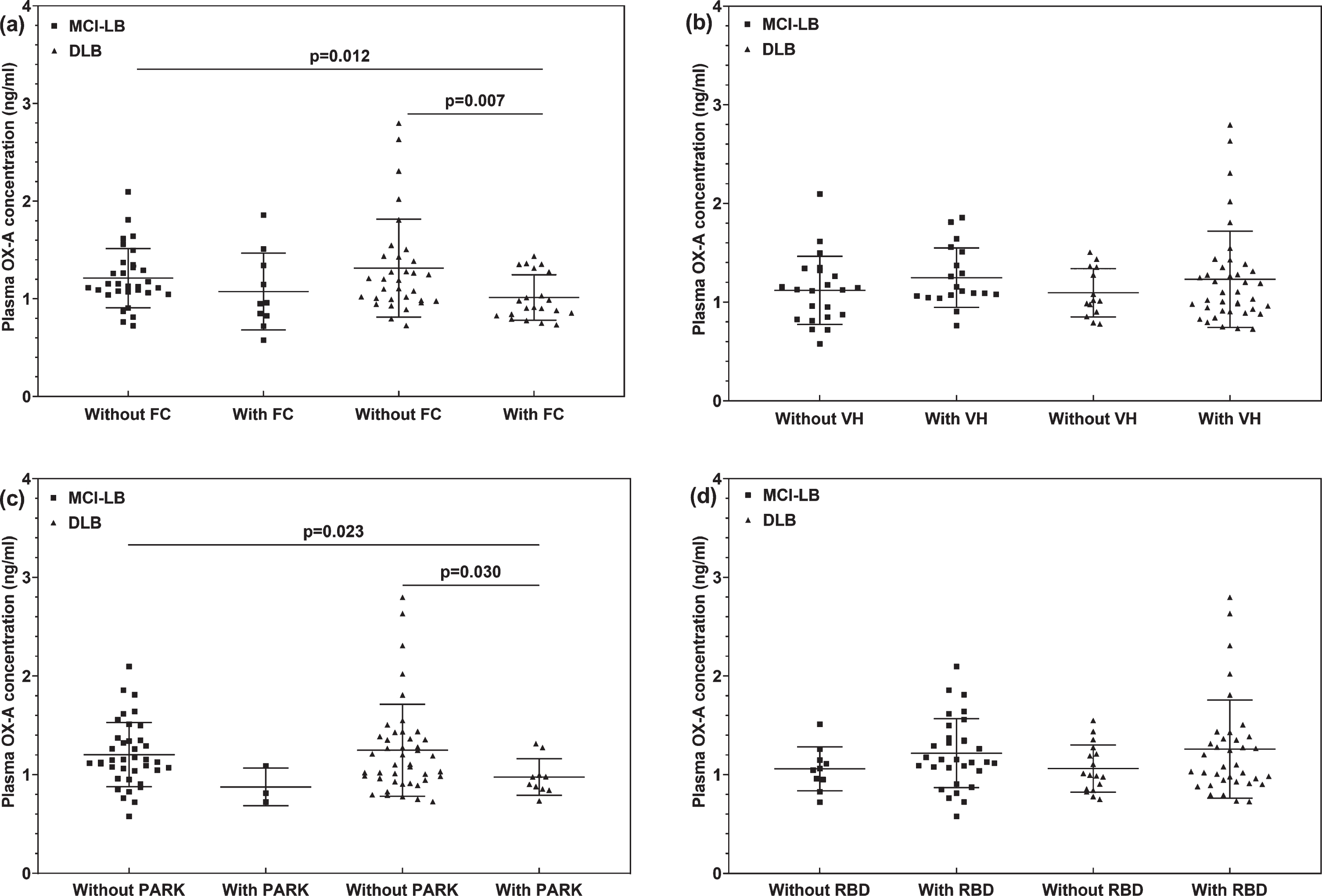
Associations between plasma orexin-A levels (ng/ml) and core clinical features of MCI-LB and DLB patients. MCI-LB, mild cognitive impairment with Lewy bodies; DLB, dementia with Lewy bodies; FC, fluctuating cognition; VH, visual hallucination; PARK, parkinsonism; RBD, rapid eye movement sleep behavior disorder; OX-A, Orexin-A.
When a cut-off point of plasma orexin-A level was set at 0.92 ng/mL based on the median value in the HCs (i.e., median split), the proportion of participants above the cut-off was 78.0% (32/41) in patients with MCI-LB (χ 2 = 7.46, p = 0.006) and 73.6% (39/53) in patients with DLB (χ 2 = 5.970, p = 0.015). Female gender (OR = 2.44, 95% CI: 1.11–5.38 in Model 1) and younger age (OR = 0.91, 95% CI: 0.84–0.99 in Model 4) were associated with elevated plasma orexin-A levels and significant association was not found between plasma orexin-A levels and BMI, night-time sleep duration, course of memory loss, and other clinical variables in Table 2.
Correlation between plasma orexin-A levels and clinical features of patients with MCI-LB or DLB
The frequency and combination of core features in patients with MCI-LB or DLB are shown in Table 3. Among the 41 patients with MCI-LB, 21 (51.2%) patients had one core feature, 18 (43.9%) had two core features, and 2 (4.9%) had three core features. Among the 53 patients with DLB, 13 (24.5%) patients had one core feature, 31 (58.5%) had two core features, 5 (9.4%) had three core features, and 4 (7.5%) had three core features. The plasma orexin-A levels decreased as the number of core features increased in patients with DLB, although without statistically significant difference.
Frequency and combination of core features in the patients with MCI-LB and DLB
MCI-LB, mild cognitive impairment with Lewy bodies; DLB, dementia with Lewy bodies; OX-A, Orexin-A; FC, fluctuating cognition; PARK, parkinsonism; RBD, rapid eye movement sleep behavior disorder; VH, visual hallucinations.
In addition, patients with MCI-LB or DLB and FC (Fig. 3a) or PARK (Fig. 3c) had lower plasma orexin-A levels, and subjects with VHs (Fig. 3b) or RBD (Fig. 3d) had higher plasma orexin-A levels than subjects without, especially among patients with DLB (FC: 1.01±0.23 versus 1.31±0.50, p = 0.007; PARK: 0.98±0.19 versus 1.25±0.47, p = 0.030).
A significant negative correlation was found between plasma orexin-A levels and UPDRS-III scores among patients (crude r = –0.294, p = 0.004 in all patients; adjusted r = –0.392, p = 0.013 in patients with MCI-LB; crude r = –0.286, p = 0.038 in patients with DLB) as shown in Table 4. Plasma orexin-A levels also significantly correlated with scores of disinhibition (adjusted r = 0.242, p = 0.020) and irritability (crude r = –0.255, p = 0.013). Particularly, plasma orexin-A levels negatively correlated with scores of irritability in patients with MCI-LB (crude r = –0.345, p = 0.027; adjusted r = –0.346, p = 0.029) and positively correlated with scores of disinhibition (crude r = 0.193, p = 0.165; adjusted r = 0.444, p = 0.001) in patients with DLB. Correlations were not observed between plasma orexin-A levels and total scores of C-MMSE, MoCA, ADL, CDR, and NPI for all patients with MCI-LB or DLB.
Associations between neuropsychological assessments with plasma orexin-A levels (ng/mL): Spearman’s rho
MCI-LB, mild cognitive impairment with Lewy bodies; DLB, dementia with Lewy bodies; C-MMSE, the Mini-Mental State Examination (Chinese version); MoCA, the Montreal Cognitive Assessment; ADL, the Activity of Daily Living Scale; CDR, the clinical dementia rating; NPI, the Neuropsychiatric Inventory. Crude models were analyzed by Bivariate Correlations with Spearman’s rho; Model 1 (adjusted by gender), Model 2 (adjusted by age), and Model 3 (adjusted by both gender and age) were analyzed by Partial correlations. *p < 0.05, **p < 0.01, ***p < 0.001.
DISCUSSION
In the present study, the plasma orexin-A levels and the correlation with clinical features in patients with prodromal DLB was investigated. The main findings indicated that plasma orexin-A levels were elevated in patients with MCI-LB or DLB compared with HCs. Plasma orexin-A levels were associated with the presence of core features; patients with MCI-LB or DLB and FC or PARK had significantly lower plasma orexin-A levels than subjects without. In addition, plasma orexin-A levels were associated with motor and neuropsychiatric symptoms; negative correlation with UPDRS-III scores and irritability and positive correlation with scores of disinhibition in patients with MCI-LB or DLB.
Interpretation of results
In the present study on prodromal DLB, plasma orexin-A levels were elevated which was different from some studies based on neuropathology and CSF. Kasanuki et al. demonstrated a reduced neocortical hypocretin immunoreactivity in patients with DLB [17]. In several studies, CSF orexin-A levels were shown reduced or statistically similar to levels in the HCs, although the mean orexin-A levels in the DLB group were higher in some subjects in the study cohort [4, 19]. In a study by Huang et al., plasma orexin-A levels were significantly higher in PD subjects than in HCs, which is similar to the present study results reflecting elevated plasma orexin levels in α-synuclein-related syndromes [7].
Because the origin of plasma orexin-A has not yet been determined, statements regarding the consistency of orexin-A levels in plasma and CSF are controversial. In a recent study, peripheral orexin-A was hypothetically “intact”, independent, and not associated with reduced central orexin-A level in narcolepsy type-1, a sleep disorder characterized by loss of orexin production in the brain and diagnosed based on low orexin-A levels in the CSF [20]. A possible explanation for this “intact” finding could be that orexin-A-producing neurons in the hypothalamus are more sensitive and prone to death during onset, resulting in low central orexin-A levels. Peripheral orexin-A-producing cells might recover more easily by the active autoimmune process, resulting in recovery and possibly a higher number of cells as the disease progresses. However, the effect of peripheral orexin-A is minimal and a significant relationship between orexin-A and disease progress was not found in the present study. Thus, more studies are needed to confirm this hypothesis. Because orexin-A neurons are mostly restricted to the LHA, and highly lipophilic orexin-A rapidly crosses the BBB via a nonsaturable mechanism [21], we postulated that circulating orexin-A could originate from the hypothalamus through the BBB, in which case plasma orexin-A levels may at least partially reflect the production of orexin-A in the hypothalamus. Our results indicate the observed increase in plasma orexin-A levels reflects increased orexin-A in patients with MCI-LB or DLB.
Furthermore, plasma orexin-A levels in patients with MCI-LB or DLB and FC or PARK were significantly lower than in subjects without. FC is considered the most characteristic and frequent core feature of DLB and observed in up to 90% of patients [1, 22]. In previous studies, fluctuation was considered to arise from the disordered switching of the brain states, which were defined by specific changes in local and global patterns of cortical states. Disruption of thalamocortical or corticocortical connections, or dysregulation of neurotransmitter/neuromodulatory pathways, may be candidate mechanisms for FC. Ascending projections from prefrontal cortex to brainstem and basal forebrain, and the dysregulation of monoaminergic signaling, cholinergic signaling, or orexinergic signaling in the lateral hypothalamus play important roles in the regulation of cortical states (reviewed in [23, 24]). Fluctuations can occur in the early stage of DLB, and although not easily recognized clinically, are actually abnormal at the biological level, with decreased orexin levels, consistent with the findings of the present study.
The associations between orexin-A and PARK in this study are consistent with previous reports in PD and PD with dementia cases [4, 25], and similar findings in experimental animal models [26, 27]. Striatal dopamine deficiency and metabolic changes are well-known phenomena in DLB. In addition, orexin-A has a protective effect on dopamine neurons. During the course of disease, when orexin neurons and orexin levels decrease, the protective effect on dopamine weakens, causing or aggravating PARK symptoms [28–30]. In the present study, an inverse correlation was observed between orexin levels and UPDRS-III score (i.e., the severity of dyskinesia and orexin). To some extent, these pathological mechanisms are responsible for this finding.
Notably, plasma orexin-A levels positively correlated with the score of the disinhibition items on NPI in patients with DLB. Disinhibition in dementia patients presents as increased impulsivity and loss of control. Studies in which orexin and disinhibition in dementia patients was investigated have not yet been performed. We hypothesized disinhibition may be associated with increased orexin levels and activation of the reward system, a circuit closely related to the orexin system. In addition, this result may be associated with decreased dopamine. In previous studies, an inverse relationship was shown between reduced striatum uptake on DAT-scan and the score of positive neuropsychiatric symptoms (e.g., delusions and hallucinations) due to impairment of the LHA/ventral tegmental area, hypothalamus/basolateral amygdala/nucleus accumbens, and hypothalamus/prefrontal cortex/hippocampus pathways [31, 32]. However, objective evidence is lacking to confirm the above finding, which needs further investigation and verification.
Strengths and limitations
To the best of our knowledge, this is the first report in which the plasma orexin-A levels and the relationship with clinical core symptoms were investigated in patients with prodromal DLB. However, the study sample was relatively small and orexin-A levels varied with values overlapping in individuals among the groups. Since this study was conducted in the cognitive impairment clinic, the patients had fewer PARK symptoms (most of them preferred to visit movement disorder clinics) and were relatively with poor cognitive performance even belonging to the prodromal stage, leading to selection bias and limiting the diversity of clinical symptoms of the target patients. A multidisciplinary approach to recruit more patients at prodromal stage is necessary. In addition, all diagnoses were based on the standardized clinical assessment rather than pathological confirmation because these methods have been shown to have high specificity when validated against autopsy findings [1]. Another possible limitation is that orexin-A level in peripheral blood is likely affected by the circadian rhythm; however, the time of blood collection was restricted to a specific time in the morning to minimize bias. Meanwhile, due to the incomplete medication information of all the participants, we could not determine the effect of other types of drugs (such as drugs for hypertension, diabetes mellitus, dementia, or PD) on plasma orexin-A levels, even though we excluded participants using orexin receptor antagonists. Finally, because whether plasma orexin-A levels reflect central orexin-A activity remains controversial, further investigation is needed regarding the correlation of orexin-A in plasma and CSF using a longitudinal cohort.
Conclusion
Plasma orexin-A levels are elevated in patients with MCI-LB or DLB and associated with the presence of core features such as motor and neuropsychiatric symptoms. These findings indicate that orexin system changes may underly the mechanisms of DLB, and monitoring orexin-A levels may be a potential treatment or prevention strategy for DLB. In addition, in the clinical treatment of sleep disorders, PARK, and neuropsychiatric symptoms, attention should be given to how the interaction between orexin and drugs affects the disease, and drug prescriptions should be carefully selected.
Footnotes
ACKNOWLEDGMENTS
The authors are grateful to all those who participated in this study and wish to acknowledge the valuable assistance obtained from all specialized physicians. We sincerely gratitude Jing Li (Tianjin Huanhu Hospital, Tianjin, China) for the data collection and input. The ELISA tests were sponsored by Dr. Sen Liu and his research team at Beijing Pason Pharmaceuticals Inc., including the experimental methods, purchase for diagnostic reagents, and technical support. We would like to express our sincere gratitude to Dr. Sen Liu and his team. All these authors accept responsibility for all aspects of the manuscript and approved the final version of the manuscript.
This work was supported by the National Natural Science Foundation of China [grant number 82171182], Science and Technology Project of Tianjin Municipal Health Committee [grant number ZC20121 and KJ20048].