
Abstract
Background:
Life-course approaches to identify and help improve modifiable risk factors, particularly in midlife, may mitigate cognitive aging.
Objective:
We examined how midlife self-rated physical functioning and health may predict cognitive health in older age.
Methods:
We used data from the Health and Retirement Study (1998–2016; unweighted-N = 4,685). We used survey multinomial logistic regression and latent growth curve models to examine how midlife (age 50–64 years) activities of daily living (ADL), physical function, and self-reported health affect cognitive trajectories and cognitive impairment not dementia (CIND) and dementia status 18 years later. Then, we tested for sex and racial/ethnic modifications.
Results:
After covariates-adjustment, worse instrumental ADL (IADL) functioning, mobility, and self-reported health were associated with both CIND and dementia. Hispanics were more likely to meet criteria for dementia than non-Hispanic Whites given increasing IADL impairment.
Conclusion:
Midlife health, activities limitations, and difficulties with mobility are predictive of dementia in later life. Hispanics may be more susceptible to dementia in the presence of midlife IADLs. Assessing midlife physical function and general health with brief questionnaires may be useful for predicting cognitive impairment and dementia in later life.
INTRODUCTION
As global populations age, Alzheimer’s disease and related dementias (ADRD) burdens are expected to grow, and disproportionately so among racial/ethnic minorities [1]. Older adults, ages 65 years and older, in the US will count close to 95 million by 2060 [2], and 2 in 5 will be Black or Hispanic. Currently, more than 1 in 9 individuals (11.3%) ages 65 years and older meet criteria for ADRD [3]. A growing body of research underscores the need for using life-course approaches to identify and help improve modifiable risk factors, particularly in midlife, to mitigate later life health conditions [4], including unhealthy cognitive aging and dementia [5]. The availability of accessible, affordable, non-invasive, and early midlife measures that could predict ADRD in later life could be especially valuable. Self-reported measures of function and health have been linked to accelerated aging and diminished life expectancy [6–10]. These midlife risks have yet to be thoroughly investigated for their utility in predicting cognitive impairment in older adulthood. This is particularly important in diverse racial/ethnic minorities given known group differences and variabilities in health status and risks for age of onset and prevalence of disability and other functional impairments [11–13].
To date most work has, understandably, focused on studying either earlier life and childhood health or, particularly relevant to gerontology, older adulthood which is commonly defined as 65 years and older. Midlife ushers important physiological transformations and accelerates disease risks accumulation [4]. Examining midlife health offers an opportunity for understanding how risk modification during this critical period in the life-course influences later life outcomes [14]. The few available studies of midlife risks for older age cognitive health have identified a number of biopsychosocial factors including socioeconomic characteristics (e.g. occupation [15]), health behaviors (e.g., tobacco [16]), and cardiovascular disease risk (e.g., diabetes [17]). This study builds on the growing evidence base investigating the contributions of midlife health conditions to later life cognitive dysfunctions [18] by examining the impact of a series of health exposures that might contribute to unhealthy aging, namely suboptimal self-reported health, and disability in the form of activities of daily living (ADL) and instrumental activities of daily living (IADL) [19, 20]. Poor self-reported physical health and functional abilities among older adults have been linked to cognitive decline and increased risk of dementia in later life [21–23]. IADL tasks in particular (e.g., handling money) are sensitive to cognitive performance and can detect early deficits in cognitive function [24]. Published studies have linked both total IADL scores as well as specific IADL items to dementia outcomes [25]. Some, but not all, diagnostic criteria for dementia and neurocognitive disorders require impairments in IADLs due to cognitive impairments [26]. Additionally, emerging population level research distinguishes between different measures of functional status/limitations as potential markers for cognitive function and decline. Recently, McGrath and colleagues, using longitudinal data on adults 50 years and older have shown that every 5 kg higher handgrip strength was associated with a 3% decrease in the odds of both cognitive impairment and severity of impairment [27], and suggested that loss in gross motor skills such as handgrip strength can forecast potential loss in cognitive function. Curreri et al. [28] linked two basic measures of fine motor skills (putting a shirt on and manual dexterity, as well as change in these measures) to development of cognitive impairment in a sample of cognitively intact older adults 65 years and older, and argued for using subtle changes in these skills as early markers of cognitive risk and for specialist referrals. Most work on functional status and activity limitations have focused on older adults. Yet, recent work on longitudinal changes in fine and gross motor skills show consistent linear decline in middle age, between the ages of 45 and 65, that precedes steeper change in older adulthood [29]. Interestingly, this work also points to high variability in rates of change over age that differ by functional domains. Indeed, results from this work suggest that the earliest reported changes are found in “motor domains that depend on white matter integrity [...whereas] measures related to alteration in gray matter volume [. . .] showed a later decline” [29]. Notably, rates of decline in motor skills, while concomitant with decline in test-based cognitive function, were less sensitive to educational attainment, potentially offering a less biased approach (not subject to education enhanced cognitive reserve) to earlier risk detection. However, investigations seldom examine links between multiple midlife characteristics (i.e., self-reported health, physical limitations, and difficulties in performing activities of daily living) and dementia. Furthermore, we do not know if higher rates of ADRD prevalence among Blacks and Hispanics relative to Whites are attributable to increased ADRD susceptibility in the presence of midlife risk factors [30].
To conceptually frame our hypothesis relating to modification by race/ethnicity, we draw from Glymour and Manly’s conceptual model on life-course correlates of racial/ethnic cognitive aging [31]. Glymour and Manly offer four modeling schemes: (a) immediate risk; (b) biological accumulation; (c) latency; and (d) social trajectories [31]. In line with these modeling schemes, our motivating argument for testing racial/ethnic differences stems from empirical evidence highlighting how accumulated life-long exposure to social, economic, and psychological burdens lead to differential accumulation of biological risks and shape racial/ethnic variations in physical and cognitive health outcomes. Stated differently, and following on arguments presented in Ortiz et al. [32], we argue that neurodegenerative pathways can be predicted from proximal dynamics (e.g., physical health dimensions and comorbidities) emerging in midlife, a crucial health transition period for older age outcomes, and shaped by distal social dynamics (e.g., risk exposures) and their individual-level sequelae (e.g., mental health). In this study, measures of disability and functional limitations represent these proximal factors that can potentially differentially shape racial/ethnic cognitive outcomes, holding distal and individual-level factors constant. Understanding how these measures vary in their associations with cognitive function by race/ethnicity can potentially help reduce disparities in cognitive outcomes and could enhance the development of more targeted interventions in underserved groups of older adults.
The purpose of this work was to examine a set of self-reported measures of function and health, assessed in midlife, that could influence cognitive status and mortality in older age. We first examined how disability in daily functioning, mobility limitations, motor skill limitations, and self-reported health among adults 50–64 years of age influenced cognitive status and mortality 18 years later. Second, we tested for modifications in the effects of disability in daily functioning, mobility limitations, motor skill limitations, and self-reported health on cognitive status and mortality by race/ethnic groups. First, we expect that all functional limitations measures considered in this study will be associated with lower baseline cognitive function (based on the modified Telephone Interview of Cognitive Status; TICS-m), steeper cognitive decline (TICS-m), and higher risk for cognitive status impairment in later life (on average 18 years later), including cognitive impairment not dementia (CIND) and dementia. Second, given the study’s focus on middle age and the relatively crude nature of the motor skills specific measures of functional limitations, we expect varying levels in the magnitudes of associations relative to the more established measure of disability. Additionally, we expect self-reported health, which is a more complex construct, to be associated with baseline cognitive function but to be more-weakly associated with longitudinal cognitive outcomes. Finally, given the higher risk for disability and earlier onset of these limitations in minority populations, we expect that race/ethnic groups will have increased risk for worse cognitive status including CIND and dementia through worse disability relative to their non-Hispanic White counterparts.
METHODS
Data
We used data from the Health and Retirement Study (HRS), which is a nationally representative sample of US adults over age 50 years [33]. The HRS collects data on functional limitations, disability (IADLs and ADLs) and cognitive performance using a series of survey questionnaires. Detailed descriptions of the HRS and its sampling framework can be found elsewhere [34]. For this analysis, we used 10 waves of biennial data with 1998 as the baseline year to examine cognitive status 18 years later in 2016. All self-reported health, physical limitations, disability, and cognitive data were taken from the RAND HRS Data file [35].
Analytical subpopulation
The HRS enrolled 42,053 participants from 1992 to 2016 including individuals from multiple age cohorts [34, 36]. For the current study, we only included participants enrolled in the original HRS or Warbabies cohort (n = 16,422) in order to maximize the number of individuals who consistently remained in the sample during our analytical time period (1998–2016). From individuals in these two cohorts, given our aims, we only included individuals ages 50 to 64 at the 1998 baseline (n = 9,712). Additionally, we excluded n = 1,258 participants who had missing observations on any of our covariates of interest. We also excluded n = 125 participants who met criteria for dementia at the baseline year (1998). We did not exclude individuals with CIND at baseline as this classification is relatively unstable. For example, in the wave following the baseline year, close to a third of individuals with CIND at baseline reverted to normal cognitive function. In the primary analyses we also excluded n = 2,332 participants who died by 2016 (however, see sensitivity analyses below). Finally, we excluded n = 1,312 participants who were lost to follow up in 2016. The unweighted analytical sample size was n = 4,685 individuals.
Outcomes
We measured cognitive status in 2016 as a three-category indicator, using the Langa-Weir (LW) classification, which included: 1) normal cognition, 2) cognitive impairment but no dementia (CIND), and 3) dementia. The cut points for the LW classification were derived through extrapolations from more comprehensive adjudication processes using data from the Aging, Demographics, and Memory Study (ADAMS; a subsample of the HRS) and validated against prevalent CIND and dementia in ADAMS. The LW classification (see details in the Supplementary Material) is used extensively in published work and the construction and rationale for its underlying algorithm are published elsewhere [37, 38].
We also used the continuous TICS-M as a measure of cognitive function and to assess cognitive decline in latent growth curve modeling. The HRS uses a reduced version of the TICS developed by Breitner and colleagues in a clinical study of dementia. The TICS-M score has a range of 0–27 with higher scores indicating better cognitive function. Details on the modifications are published in published documentation [39].
For the first set of sensitivity analyses, we created a four-category outcome by combining cognitive status in 2016 with death status in 2016 to account for attrition due to morality by including participants who were alive at baseline (1998) but died by the 2016 wave. Using this combined cognitive status and death outcome, we repeated the primary analysis. Additionally, among those classified as dementia in 2016, 39.2% satisfied criteria based on proxy reports. As such, we conducted a second set of sensitivity models using a 4-cateogry classification to distinguish between individuals meeting criteria for dementia based on self versus proxy reported assessment (Normal, CIND, Dementia, and Proxy Dementia).
Exposures
We examined a set of midlife health exposures at baseline including functional limitations and self-reported health. The RAND HRS contains 6 functional limitations indices gauging a respondent’s ability to perform specific tasks. The 6 indices, along with their component questions, are: 1) Activities of Daily Living (ADL; range 0–5) regarding bathing, eating, dressing, walking across a room, and getting in or out of bed; 2) Instrumental Activities of Daily Living (IADL; 0–5) probing independent ability to use a telephone, take medication, handle money, shop and prepare meals; 3) Mobility question on ability for walking several blocks, walking one block, walking across the room, climbing several flights of stairs, and climbing one flight of stairs; 4) Large Muscle (0–4) questions on sitting for two hours, getting up from a chair, stooping or kneeling or crouching, and pushing or pulling a large object; 5) Gross Motor Skills (0–5) evaluating walking one block, walking across the room, climbing one flight of stairs, and bathing; and 6) Fine Motor Skills (0–3) probing ability to pick up a dime, eat, and dress. The criteria for each measure are summarized in Supplementary Table 1 for reference. Finally, a self-reported health status measure evaluated general health status and had a range of 1 to 5 where “1” is excellent and “5” is poor.
Covariates
All covariates used in this analysis were from the baseline year (1998). The guiding principle for covariates choice was to control for known socioeconomic, demographic, and health behavior drivers of health outcomes and to adjust for the effects of the unequal distributions of these characteristics across racial ethnic groups in our modification analyses. Similar adjustments have been used in previous work examining biological and social exposures to cognitive function and cognitive status impairment [32, 40]. Future work, however, should include additional measures intended to test more specific pathways offered by the biopsychosocial framework (including genetic predisposition, early life risks, as well as other individual characteristics and distal level factors). For this study, we adjusted for sex, continuous age (years), race/ethnicity (White, Black, Hispanic, other; specifically, we coded this variable so that individuals were classified as White, Black, or Other first. Subsequently, we created a new category isolating Hispanic ethnicity based on whether respondents in any of the three racial groups responded “Yes” to being Hispanic. We included education as a continuous measure, health insurance status measured using a four-category indicator (government only, government and private, private only, no insurance), employment status (working fulltime/part-time, not working), income (using quintiles to adjust for the effects of right skew), smoking status (current, former, never), vigorous activity status (≥3 days of vigorous activity per week), continuous body mass index (BMI; kg/m2), and depressive symptoms (using a continuous measure of the CESD-8). We also accounted for cohort and census region (Northeast, Midwest, South, West).
Statistical analyses
First, we generated descriptive statistics to characterize the study sample overall and by cognitive status. We reported survey adjusted percentages, standard errors, and chi-square derived p-values for categorical variables and survey adjusted means, standard deviations, and t-test derived p-values for continuous variables in Table 1.
Baseline descriptive characteristics of Health and Retirement Study target sample by Langa-Weir cognitive status in 2016
CIND, cognitively impaired but not dementia; BMI, body mass index; p, Pearson’s chi square test for continuous variables; Regression based F test for categorical variables. a % and standard errors (SEs) are presented; b means and standard deviations are presented.
Second, we fit survey multinomial logistic regression models to estimate relative risk ratios (RRR) and 95% confidence intervals (CIs) of each of the midlife health exposures (6 functional limitations and self-reported health) on cognitive status (normal, CIND, and dementia) in 2016. We fit four regression models: 1) crude (without covariate adjustments); 2) age and sex adjusted; 3) additional adjustment for continuous education; and 4) full adjustment to include all the covariates specified above (see covariates section). We reported the RRRs with 95% CIs in Table 2 and visualized the crude and adjusted RRRs to facilitate interpretation and comparisons in Fig. 1. We calculated marginal probabilities from the covariate adjusted models along with 95% CIs and plotted them in Fig. 2 and Supplementary Figure 1 to translate the risk ratios into probability predictions for how worse midlife functional limitations affect cognitive status classification. Subsequently, we tested for differential associations (modification effects) by race/ethnicity (interaction with the midlife health exposures) and reported joint p-values in Supplementary Tables 3 and 4 to highlight significant overall effects of the modification variables.
Associations between midlife health exposures at baseline (1998) and Langa-Weir cognitive status in 2016
RRR, relative risk ratios; CI, confidence intervals; CIND, cognitively impaired but not dementia. M1: Crude. M2: M1 + Age, Sex. M3: M2 + Years of school (Centered at 12). M4: M3 + Region, labor status, smoking status, physical activity status, body mass index, insurance status, marital status, income (quintile), CESD. *p < 0.05, **p < 0.01, ***p < 0.001.
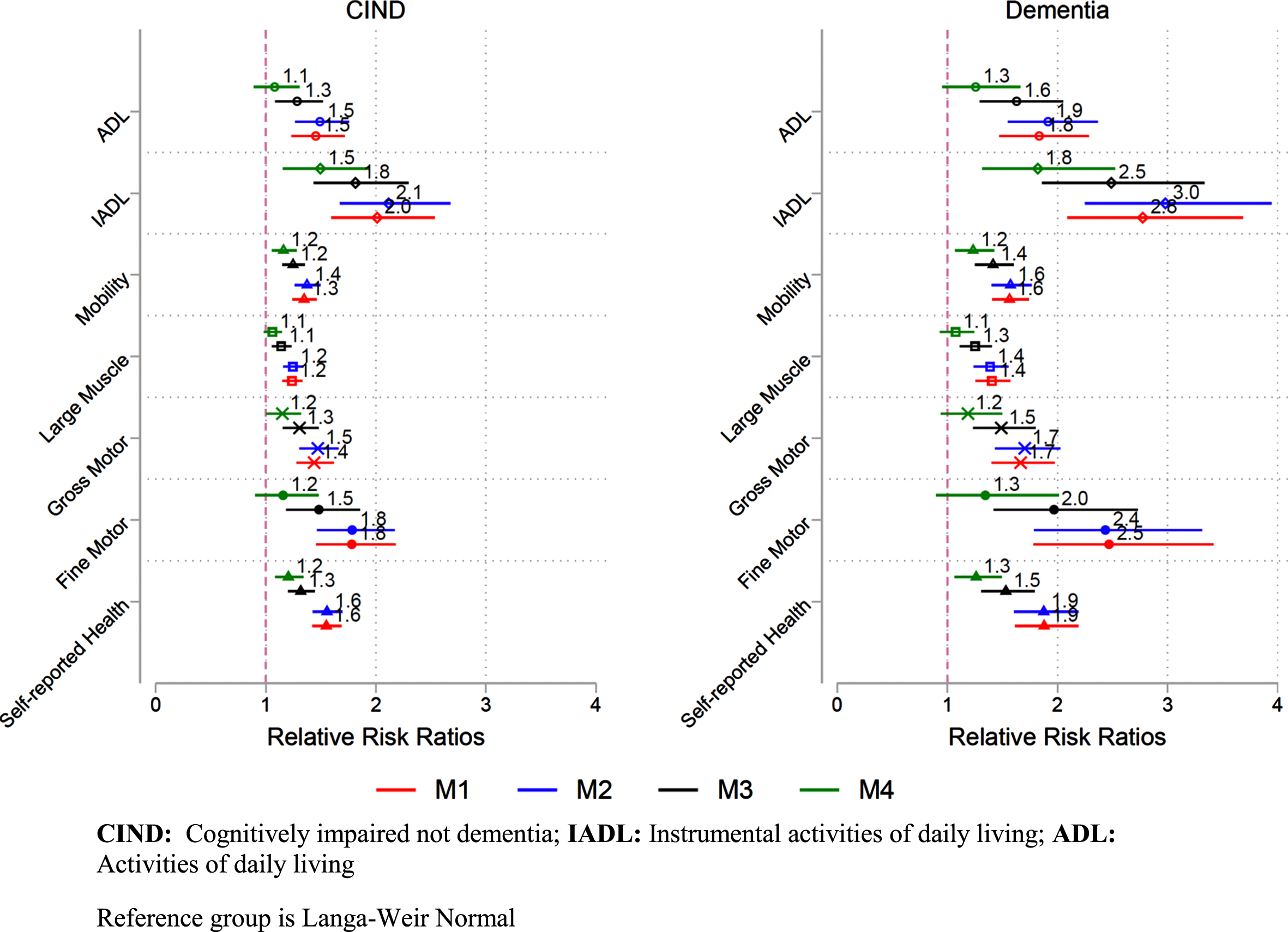
Relative risk ratios of the associations between midlife health exposures in 1998 and Langa-Weir CIND and Dementia outcomes in 2016.

Multinomial logistic regression marginal estimates with 95% confidence intervals. Primary midlife health exposures. Higher values indicate more limitations.
Third, we used latent growth curve models (LGCM) to test longitudinal associations between each midlife health exposure and the trajectory of cognitive function (using the continuous TICS-M) over ten time points. Compared to the analytical models described above, LGCM can clarify whether and to what extent midlife health exposures influence baseline cognitive function and longitudinal cognitive change. Detailed theoretical and applied treatments of latent growth models are provided elsewhere [41, 42]. A brief description of these models as used in this study is provided in the Supplemental Material. A linear function provided good fit to the data, and all models were estimated as such. In sensitivity analyses, we re-estimated the LCGM without imposing a parametric functional form on time (e.g., linear). Results were qualitatively unchanged. We used years since baseline wave as the time metric and estimated the models using full information maximum likelihood (FIML) to account for all available data. All LGCM models were fit using Mplus 8.3. Table 3 includes the estimated fixed and random effects (variance estimates of growth parameters) and inferential statistics (SEs, and p-values). Evaluation of changes in the estimated variances/residual variances of the intercept and slope allowed us to assess the contribution of the covariates to explaining between individual differences in growth trajectories.
Latent growth curve models examining the associations between midlife health exposures at baseline and change in TICS-M cognition from 1998–2016
TICS-M, modified Telephone Interview for Cognitive Status; IADL, Instrumental activities of daily living; ADL, Activities of daily living. M0: Unconditional linear growth model. M1: Crude. M2: M1 + Age, Sex. M3: M2 + years of school. M4: M3 + Region, labor status, smoking status, physical activity status, body mass index, insurance status, marital status, income (quintile), CESD. *p < 0.05, **p < 0.01, ***p < 0.001.
The estimated mean of the intercept denoted the average TICS-M score for the analytical subpopulation at baseline and the estimated slope mean quantified the average decline in TICS-M score over time. First, we fit a model without an imposed parametric functional form on time. Then we used years since the baseline (1998) period as a linear time metric to estimate the next series of models: 1) no covariates adjustment, 2) age and sex adjustment, 3) age, sex, and education adjustment, and 4) full covariates adjustment (age, sex, education, cohort, occupational status, smoking status, physical activity status, BMI, and insurance status).
We conducted two sensitivity analyses. In the first set, we combined the cognitive status outcome with death status in 2016. The descriptive statistics over the combined measure are included in Supplementary Table 5. Additionally, the survey multinomial logistic regressions from the primary analysis were repeated using the combined measure and presented in Supplementary Table 6. In the second set, we distinguished dementia classification based on whether cognitive information was provided by the respondents versus their proxy. The descriptive statistics over these cognitive classifications are provided in Supplementary Table 7. Additionally, the survey multinomial logistic regressions replicating the primary analysis are presented in Supplementary Table 8.
All analyses accounted for the complex survey design of the HRS including sampling probability weights (using the baseline 1998 wave), clustering and stratification. Analyses were conducted using Stata version 16 and Mplus 8.3.
RESULTS
Descriptive statistics (Table 1)
Weighted estimates indicated that by 2016 79.3% (unweighted n = 3,518) satisfied criteria for normal cognition, 15.6% (unweighted n = 848) were CIND and 5.0% (unweighted n = 319) met criteria for dementia. Mean baseline age was 56.0 years, 42.1% were males, mean education was 13.1 years and almost half reported more than 12 years of education. The majority were non-Hispanic Whites (81.5%), 8.9% were non-Hispanic Black, and 7.1% were Hispanic. Almost two-thirds of the target population (67.6%) reported working full time or part time, 75.8% were married, and 8.7% had no insurance. The mean BMI was 27.5, more than two-fifths never smoked (42.6%), and over half performed vigorous physical activity (53.3%). When comparing all three categories of cognitive status, the group with dementia was more likely to be older, female, less educated, had a higher proportion of non-Hispanic Blacks and Hispanics, and had a higher proportion of current smokers.
Functional limitations, self-reported health, and cognitive status (Table 2)
In all the multinomial logistic regression models, we set the normal category for cognitive status as the reference. Worse levels for all 6 functional limitations and self-reported health were significantly associated with higher CIND risk. However, after adjusting for covariates, only limitations in IADL (RRR = 1.50 [1.16, 1.94], p < 0.01), mobility (RRR = 1.16 [1.05, 1.28], p < 0.01), gross motor skills (RRR = 1.15 [1.01, 1.32], p < 0.05), and also worse self-reported health (RRR = 1.21 [1.09, 1.34], p < 0.001) were significantly associated with CIND. The magnitudes of the reported associations with these midlife health exposures were partially attenuated through covariates adjustment; by 25.4%, 14.1%, 20.1%, and 21.9%, respectively. Similarly, in the crude models, worse functional limitations on all 6-measures and self-reported health were significantly associated with higher likelihood of dementia. After adjusting for covariates, dementia was only significantly linked to higher IADLs (RRR = 1.82 [1.32, 2.52], p < 0.001), worse mobility (RRR = 1.23 [1.07, 1.43], p < 0.01), and worse self-reported health (RRR = 1.26 [1.06, 1.49], p < 0.01). The magnitudes of the reported associations with these exposures were partially attenuated through covariates adjustment; by 34.3%, 21.2%, and 33.0%, respectively. To facilitate the interpretation of these results the RRRs from Table 2 were plotted in Fig. 1, and the marginal probability estimates for classification into each of the cognitive status categories in Fig. 2 (for the exposures that remained significant after covariates adjustments) and Supplementary Figure 1 (for all remaining exposures). We used post-hoc testing through seemingly unrelated estimation techniques to examine equality of RRRs (k = 14 estimators) derived for the individual functional limitations and self-reported health models (k = 7 multinomial models) as described above. The technical aspects for deriving simultaneous distributions of estimators and for generating simultaneous variance/covariance estimates from k different models to allow stacked cross model comparisons and testing, through Hausman tests, are detailed elsewhere [43]. Our post-hoc tests indicated significant differences in the magnitudes of the derived RRRs from the estimated exposures for both CIND and Dementia. These results are presented in Supplementary Table 2.
Functional limitations, self-reported health, and cognitive function and decline (Table 3)
The mean TICS-M scores at baseline (mean intercept) was 17.7 (SE = 0.089, p < 0.001), and the average biennial decline (slope) was –0.24 (SE = 0.007, p < 0.001). The variances for the intercept and slope were 8.8 (SE = 0.311, p < 0.001) and 0.042 (SE = 0.003, p < 0.001), respectively. We found that worse self-reported health was associated with poorer cognitive function (mean TICS-M score) at baseline [–0.846 (SE = 0.054, p < 0.001)] and with more pronounced decline per biennial wave [–0.013 (SE = 0.005, p < 0.05)]. However, these associations were explained by adjustment for age and sex. Similarly, in crude models we found significant associations between worse mobility and lower baseline cognitive function as well as slope of decline [(–0.012 (SE = 0.005, p < 0.05)]. These associations were also explained by adjustment for age and sex.
Additionally, we found that worse IADLs and gross motor skills were associated with lower cognitive function (mean TICS-M score) at baseline after adjusting for covariates. In particular, each additional unit of IADL, and gross motor skills limitation was associated with –0.473 (SE = 0.122, p < 0.001) and –0.185 (SE = 0.078, p < 0.05) lower mean TICS-M score at baseline, respectively.
Race/ethnicity modifications
The results for race/ethnicity interactions are summarized in Supplementary Tables 3 and 4. Race/ethnicity modified the associations between ADL (p = 0.039) and IADL (p = 0.011) and cognitive status in 2016. Specifically, Hispanics were more likely to satisfy criteria for dementia compared to non-Hispanic Whites given higher ADL (Δ= 0.041 [0.014, 0.068], p < 0.01) and IADL (Δ= 0.08 [0.033, 0.127], p < 0.01) limitations. However, these differences were explained by adjusting for covariates. We found no consistent statistical evidence to support race/ethnicity modifications in associations between the other functional limitations measures or self-reported health and cognitive status.
Sensitivity Analysis 1 (Supplementary Tables 5 and 6)
All associations described in the primary analysis remained consistent when we considered death as a competing risk category in our models. The results for the sample descriptive characteristics and survey multinomial logistic regressions are summarized in Supplementary Tables 5 and 6, respectively.
Sensitivity Analysis 2 (Supplementary Tables 7 and 8)
All associations described in the primary analysis remained consistent when we distinguished between self and proxy assessed dementia groupings in our models. The results for the sample descriptive characteristics and survey multinomial logistic regressions are summarized in Supplementary Tables 7 and 8, respectively.
DISCUSSION
Our study examined longitudinal associations between midlife functional limitations and self-reported health and later life cognitive outcomes (including cognitive status and change in function) using nationally representative US data. First, we showed that individuals who reported higher levels of functional limitations and worse self-reported health between ages 50–64 years were more likely to meet CIND and dementia criteria 18 years later. Our findings pointed to IADLs and mobility limitations and worse self-reported health in midlife as specific factors for higher relative risks for both CIND and dementia in later life. Investing in resources that prevent or help ameliorate midlife limitations in daily function, enhance mobility, and foster improvements in subjective health may help partially mitigate the expected growth in dementia in the US. Second, our results suggested that middle-aged Hispanics with disability are more likely to meet criteria for dementia 18 years later compared to non-Hispanic Whites, but the higher likelihood was explained by adjustment for race/ethnicity differences in covariates. The mechanisms and pathways of disablement among Hispanics require closer scrutiny particularly the role of socioeconomic and other health enabling resources. Earlier interventions to modify or reduce the potential for disability in Hispanics can influence the course of cognitive health in this group and yield important population health benefits.
Our first finding highlighted limitations in IADLs in midlife as specific factors for higher relative risks for both CIND and dementia in later life. Our results were in line with previously published studies linking midlife IADL limitations and diagnosis of CIND and dementia [20, 44–46]. A recent study by Edwards and colleagues examining US individuals ages 55 years and older found that 50% of females and 40% of males with CIND or dementia reported having some disability [47]. A prospective study using the Framingham cohort suggested that the preclinical phase of dementia could begin 10 years before diagnosis [44]. Pérès et al., using data from the Personnes Agées QUID cohort, a French epidemiological survey on cerebral and functional aging, also showed that subjects who later developed dementia performed worse in complex activities of daily living 10 years prior to diagnosis [20]. Previous work also suggested that IADL limitations have an important predictive power for incident dementia, and there is evidence for including IADL limitations in mild cognitive impairment (MCI) criteria to improve the prediction of dementia as well [45, 46]. More attention to IADLs during midlife may allow for uncovering early markers of cognitive problems and creating corrective courses that might modify and delay disease course.
Recent evidence suggests that disabilities are increasingly prevalent in midlife [48]. With the expected aging of the US population a continuous surge in rates of disability is a warning sign for downstream development of burdensome diseases, including dementia. There are numerous potential causes underlying disability development. To list a few, the epidemic growth in obesity rates in the United States starting in childhood and extending into older age, particularly among race/ethnic groups [49]. As important, the continuous breakdown in the safety net [50], and the increased physical and psychological demands and burdens required to sustain individual and household economic viability, particularly among the fraying middle class, and several historically underprivileged groups, and the influence of life-course exposures to such contexts to the disablement process. Advances in technology and entertainment offerings that promote sedentary lifestyles, hinder participation in traditionally protective measures of mobility, physical activity and social engagement and increase the risk of chronic disease and functional impairment [51–54].
While in the aggregate our findings emphasize the importance of midlife functional limitations to later life outcomes, our results offer a more nuanced view of how different measures of limitations are linked to these outcomes. We found that IADLs were associated with both CIND and dementia in later life in unadjusted and adjusted models, whereas midlife ADLs were only linked to later life dementia in the unadjusted models. This may be attributed to IADLs’ susceptibility to cognitive difficulties and ADLs sensitivity to physical impairment [55]. Our findings were consistent with evidence on the importance of task complexities in the criterion to define the syndrome of MCI: that is, impairments in IADLs, and not ADLs, are sometimes used to distinguish MCI from dementia [24]. Thus, IADL limitations can be used to statistically predict future cognitive status outcomes. Clinically, earlier onset of IADLs, in middle age, can also be used as an early marker or warning when constructing patient risk profiles for cognitive impairment.
We also reported that mobility limitations in midlife were associated with cognitive decline and dementia in later life. Several studies have used more specific measures of mobility, such as gait speed and dual-task gait, to assess mobility functioning, and showed robust links between these measures and various health outcomes (e.g., cognitive status, motor declines, falls) and endpoints (e.g., mortality) [56]. The measures of mobility in our study primarily consisted of walking on level ground and vertical climbing distance. Few studies have examined how these specific measures assessed in midlife are related to longitudinal cognitive outcomes [57, 58]. Despite being relatively crude physical measures, our results suggest that they are sufficient indicators of risk for cognitive dysfunction. While gait speed is a more sensitive measure of functional mobility for older adults [59], interventions that target physical activity including light activities that facilitate walking and climbing small distances may be additional avenues to modify an individual’s risk for cognitive decline and dementia. Research has shown that self-reported health is another strong predictor of cognitive decline, impairment, dementia and mortality among older adults [23, 60]. Though the associations of midlife self-reported health on later life cognitive status has not been well studied, literature supports the validity of self-reported health as a robust health measure in middle-aged populations [61]. Our findings warrant further exploration of whether and how components of self-reported health in midlife, including subjectively and objectively measured criteria, act independently or synergistically to influence trajectories of aging and cognitive outcomes.
Regarding cognitive trajectories, we found that lower self-reported health and mobility limitations resulted in worse cognitive function at baseline as well as more pronounced rates of decline in cognitive function, but these associations were explained by adjustment to covariates. Prior studies also suggest that decline in mobility and cognitive function interact and increase risk of adverse event and conditions, such as falls and fractures, that may lead to further cognitive decline [62, 63]. Mobility has been more strongly linked to fluid aspects of cognition, such as attention, learning, and sensory integration [21]. Thus, mobility limitations in midlife may expedite the rate of cognitive decline as an individual approaches later life. Overall, we did not find robust results in the effects of mobility limitations on decline in cognitive function like Tolea et al. did [62]. This may be attributed to differences in the cognitive measures used. Whereas Tolea et al. used a clinical assessment for dementia, our study relied on threshold values from a relatively short research index for determining cognitive function and status. Additionally, participants in Tolea’s et al. study were much older at baseline (76.8±8.5 years) when compared to the present study’s average age at baseline.
We did not find evidence to link midlife disability and limitations measures to the rate (slope) of cognitive decline [64]. Rajan et al., using data from the Chicago Health and Aging Project, an ongoing longitudinal study of Alzheimer’s disease, have shown that disability was associated with a faster rate of decline in cognitive function in older adults [64]. Similar findings linking IADL limitations to worse cognitive trajectories, cognitive impairment and dementia have been published [45, 65]. Most of these studies, however, focused on older individuals which could explain differences in reported associations relative to our study. Our results suggest that the presence limitations in midlife may predispose one to have worse baseline cognition which carries over time. Future work should examine and contrast the trajectories of cognitive decline among those that switch to CIND and dementia compared to the cognitively resilient. Identifying how limitations and disabilities influence the course of cognitive decline over time and determining potential midlife factors that contribute to attenuating or explaining these associations can aid in developing more targeted interventions within these higher risk groups.
No studies to date, to our knowledge, have examined whether and how race/ethnicity modifies the relationships between midlife functional limitations and self-reported health and cognition. Previous studies reported that Hispanics and Blacks have higher levels and earlier onsets of functional limitations [66–70]. Given the higher prevalence of functional limitations and disabilities in minority populations at younger ages, studies that aim to provide a clear understanding of the disablement process and to identify primary targets for modification interventions can yield important public health gains and alleviate downstream burdens of cognitive disease in these groups. Our findings showed that Hispanics with higher baseline IADLs were more likely to meet dementia criteria than Whites 18 years later. The Hispanic Health Paradox suggests that Hispanics have longer life-expectancy at birth compared to non-Hispanic Whites [71]. While the Hispanic Paradox continues to be widely debated [72], several recent studies have shown that despite this longevity Hispanics are likely to live longer periods of their lives with elevated levels of disabilities and morbidity, relative to non-Hispanic Whites [73]. The increased disease burden that Hispanics face, including higher likelihood of cognitive disease, has critical implications for quality of life and for personal, familial, and systemic resource allocations [30]. The older Hispanic population is projected to increase by four-fold over the next three decades, which is more than any other major ethnic/racial group [74]. Additionally, Hispanics may be disproportionately affected by ADRD compared to non-Hispanic Whites [75]. The reported modifications in associations were explained by adjustment to covariates, including for enabling factors, thus highlighting the contributions of sociodemographic and economic contexts to health differentials between Hispanics and non-Hispanic Whites. Targeted risk modification for socioeconomically vulnerable subgroups within Hispanics can be particularly useful, though the nature of these modification and interventions is hard to pinpoint.
Our findings, overall, point to the importance of physical health and function in midlife as antecedents to older age cognitive health. Given the higher prevalence and earlier onset of functional limitations and disabilities in race/ethnic groups and the critical role of life-course exposures to increasing the incidence of these outcomes, our results highlight the need to better understand and address the disablements pathways in light of the forecasted aging of the US population. From this perspective, our study points to critical public health issues to anticipate and attempt to address among today’s young and middle-aged adults who will form the majority of the 1 in 4 older adults expected by 2050. However, our results also offer evidence for differential associations between alternative measures of functional limitations and cognitive outcomes. On one hand, in line with published evidence, we point to a potentially common neurological pathways for adverse functional health, ushered starting midlife, and later life cognitive dysfunctions, mainly as a result of baseline cognitive deficits. Yet, the fact that we detected differences in associations with population level data and at the crude level of distinction that our measures permit also suggests the possibility for differing mechanisms at work. Exploring these mechanisms goes beyond the scope of this manuscript and our limited data. More precise clinical measures are needed to validate our findings and to clarify the nature of these mechanisms. Still, our results add to the evidence base and discussion around the need to find and address earlier markers of cognitive dysfunctions given the current absence of successful pharmacological treatment options.
Our study has several strengths. The HRS is a national longitudinally representative dataset of individual older than 50 years of age. The HRS has a well characterized sample of Black, White, and Hispanic participants with 1) self-reported measures of functional (physical and disability) limitations and self-reported health at midlife (ages 50–64), 2) availability of cognitive/mortality status after a long follow up period, and 3) relatively low rates of attrition over the 18-year time period. Currently, the evidence base on the associations between midlife functional limitations and health and later life cognitive outcomes are under-developed. Our results are a first step to help establish and better understand how midlife context shapes later life outcomes, and whether midlife health contexts influence race/ethnicity outcomes differentially.
Our results should be considered in the context of several limitations that should be addressed in follow-up studies. First, we focused on global cognition and used a threshold-based measure (the LW research criteria for CIND and dementia) of cognitive impairment for classification. Examining specific cognitive domains would help to better understand and clarify the effects of our risk factors on cognitive functioning. Previous studies have shown that functional limitations could have a differential effect on specific domains of cognition [76]. Second, we did not exclude individuals with baseline CIND from our analyses, despite elevated impairment and higher risk for transition to dementia in this group. We opted not to do so given the relatively high instability in classification for this group (close to a third reverted to normal within 2 years). However, focusing on CIND individuals, particularly those that maintain that status or transition to more severe impairment status, requires further examination, particularly given the increased interest in pre-clinical stages of diseases and monitoring and potential intervention before onset of more severe symptoms. Future work should examine the role of the risk factors/exposures considered in this study in accelerating how individuals with CIND switch to dementia. Third, we did not examine longitudinal change in functional limitations and their potential effects on later life cognitive outcomes. Future work should clarify whether and how longitudinal variability in daily functioning and physical and motor functioning can potentially affect change in later life cognitive status. Finally, while we modeled death as a competing risk in sensitivity analyses and reported consistent findings from these models we did not account for attrition due to selective non-response or non-death related attrition [77]. Older age adults and those with health and functional limitations are more likely to drop out from follow-up studies, and this may more so apply to Blacks and Hispanics. Non-death specific attrition over the 18 years of study, given the younger age considered, was relatively low. Differences in baseline characteristics for 2016 respondents, those that died, and non-deceased attritors are presented in Supplementary Table 9. Future work should consider incorporating missing data schemes (through imputations or direct modeling of missingness patterns) particularly for modeling the effects of longitudinal change in disability and functional limitations on cognitive status.
Conclusion
Using data covering 18 years of follow-up, we found that worse midlife functional limitations were associated with an increased likelihood of impaired cognitive status. Our findings suggest that midlife years play an important role in healthy cognitive aging and may be a critical period for interventions. In light of the forecasted increase in dementia rates over the next few decades, modifying the midlife health profiles of US adults—though the mechanisms for how to do so remain largely unknown—can potentially yield important public health savings and reductions in structural and social health burdens.