
Abstract
Background:
The World Health Organization has estimated that worldwide around 50 million people have dementia. The World Alzheimer Report estimated that between 2 and 10% of all cases of dementia begin before the age of 65. Early and young onset dementias (EYOD) provoke more working, social, family, and economic consequences than late onset dementias. All general studies about costs of dementias show that most of them are indirect or social costs. Despite that, very few studies have been performed in EYOD.
Objective:
To do a systematic review of literature about indirect or social costs in EYOD to know the state of knowledge and to discover gaps that should be filled.
Methods:
A systematic review was performed in the main database: Scopus, PsychInfo, Web of Science (Web of Science Core Collection, Medline and SciELO), and CINAHL. Additionally, we looked for reviews in Cochrane and in the International Prospective Register Of Systematic Reviews (PROSPERO).
Results:
Most of the studies are about costs of dementias in general, but they do no differentiate costs for the case of EYOD. Many studies highlight the increased costs for EYOD but very little included evidence of that. 135 papers were selected. Finally, only two were studies providing data. EYOD reduce the odds to get or maintain a job. Most of the care is provided by informal caregivers. The costs in EYOD are 39.26% higher among EYOD than in late onset.
Conclusion:
There is a lack of studies about social and indirect costs in EYOD. More evidence is needed.
INTRODUCTION
Early onset dementia (EOD), arbitrarily defined by age at onset and previously designated “presenile” [1], refers to dementia becoming clinically manifested before age 65 [2, 3]. Young onset dementia (YOD) has been use for onset before 45 [4], but there is no consensus at this point; some authors define YOD dementia and EOD with the same definition [5–7]. In this paper, the terms will be used interchangeably, as was done by Rossor [8] and Massellis [2].
The World Health Organization (WHO) has estimated that worldwide around 50 million people have dementia, with nearly 60% living in low- and middle-income countries. This figure is expected to reach 82 million in 2030 and 152 in 2050. The estimated proportion of the general population aged 60 and over with dementia at a given time is between 5–8% [9]. As Davis et al. (2011) mentioned [1], the World Alzheimer Report estimated that between 2 and 10% of all cases of dementia begin before the age of 65.
Early and young onset dementias (EYOD) are frequently underdiagnosed, misunderstood, and inadequately treated, with limited services and resources in many countries [10]. EYOD are a very heterogeneous group of syndromes that include dementias due to: Alzheimer’s disease (AD), vascular dementia, cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy, frontotemporal dementia, Parkinson’s disease, dementia with Lewy bodies, Huntington’s disease, Creutzfeldt-Jakob disease, Down’s syndrome, HIV, chronic alcoholism, as part of the evolution in certain cases of mild cognitive impairment, and mixed dementia, among others. It is very interesting to note the paper of Jefferies and Agrawal (2009) [3] which covers these issues. AD has been described as the most common dementia diagnosis even among young adults [10]. EYOD are more likely to run in families and be inherited in a Mendelian fashion [2].
In a recent study, authors found that people with EYOD are more likely to exhibit behavioral disturbances and neuropsychiatric symptoms but were less frail and less dependent for activities of daily living [11]. There are no specific symptoms for EYOD but in a report published in 2005 in Ireland, they found that 56% experienced depression and 71% suffered from anxiety [12]. Additionally, to suffer from EYOD implies specific consequences different to those of late onset dementias (LOD). More people are of working age (versus retired in late onset), as are their partners, they have dependent children, and they struggle to access to social and medical services designed for dementias (that usually debut at old ages).
In a study with the UK population [13], it was estimated that by 2040, over one million people living with dementia will receive some level of unpaid and/or paid care. Kriit et al. (2021) [14] stated that “in Europe, the annual dementia-related societal costs including all costs occurring due to dementia, regardless of the funding source, have been estimated to be € 10.3 billion, where informal care contributes about one third of the total costs”.
Direct costs usually includes all the medical care costs (e.g., hospitalization, medical visits, assessment technologies, drugs, etc.) and social service costs (e.g., day care centers, nursing homes, home-care services, etc.) that are financed totally or partially by the State or an insurance institution, and all the out-of-pocket costs assumed by informal caregivers (e.g., home adaptations). Meanwhile indirect costs, sometime also named as social costs, reflect the average productivity losses (e.g., early retirement, loss of jobs) and time of dedication by informal caregivers. It means that these costs usually include those types of costs that do not imply a payment but can be estimated by revealed preference methods such as: the opportunity costs, the estimation of a substitution costs by a formal caregiver, or a loss of quality of life, frequently measure as quality-adjusted life-year (QALY) [14–16]. And they can also be estimated by stated preference methods, such as: contingent valuation (e.g., willingness to pay and willingness to accept) [17–20] or by discrete choice experiments [21–24]. Additionally, some authors have highlighted that caregiving can also derive positive utility such as satisfaction or self-fulfillment for taking care of a loved one [19, 25].
Most of the papers about EYOD highlight the relevance of the cost associated to this condition [26–30]. Some studies have measured the direct and indirect costs for dementias [13, 31–35], but very few performed an empirical evaluation of these costs [6, 36].
The clinical characteristics of the syndrome in the LOD and the EYOD are similar, even age is no longer used to discern dementia subtypes [37] but, costs for EYOD are different. The aim of this systematic review is to show what do we know about indirect or social costs in EYOD and to highlight the gaps of knowledge that can encourage research teams to fill them.
MATERIALS AND METHODS
A review of the literature was performed in the main databases in order to have a comprehensive view of the state of knowledge about indirect and social costs in EYOD.
The research was conducted on 20 July 2021 through: Scopus, PsychInfo, Web of Science (WOS), and CINAHL. We looked for papers published from 1990 to 2021. In CINAHL, we only could look for papers between 2005 to 2021. In the WOS, we used three databases: 1) Web of Science Core Collection, 2) Medline, and 3) SciELO. Additionally we looked in Cochrane and in the International Prospective Register Of Systematic Reviews (PROSPERO) [38] to find similar reviews. No one was found. The review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [39].
Only articles or reviews written in English or in Spanish were included. To be selected, a paper should contain at least a combination of keywords as seen in Table 1. The keywords and Boolean operators used were: (Early OR Young) AND Onset AND Dementia AND (Social OR Indirect) AND Cost*. These terms should be in the title, abstract, or keywords.
Key words and results obtained in the different databases
An iterative and hierarchical research process of selection was followed as shown in Fig. 1. 135 papers were found in the first step in all the databases. In the second phase, we eliminated duplicates in the different search sequences. To do that we used the Endnote app for papers obtained from WOS and Mendeley for the following steps. After that, 68 papers were chosen to be reviewed in the third phase (See Fig. 1).
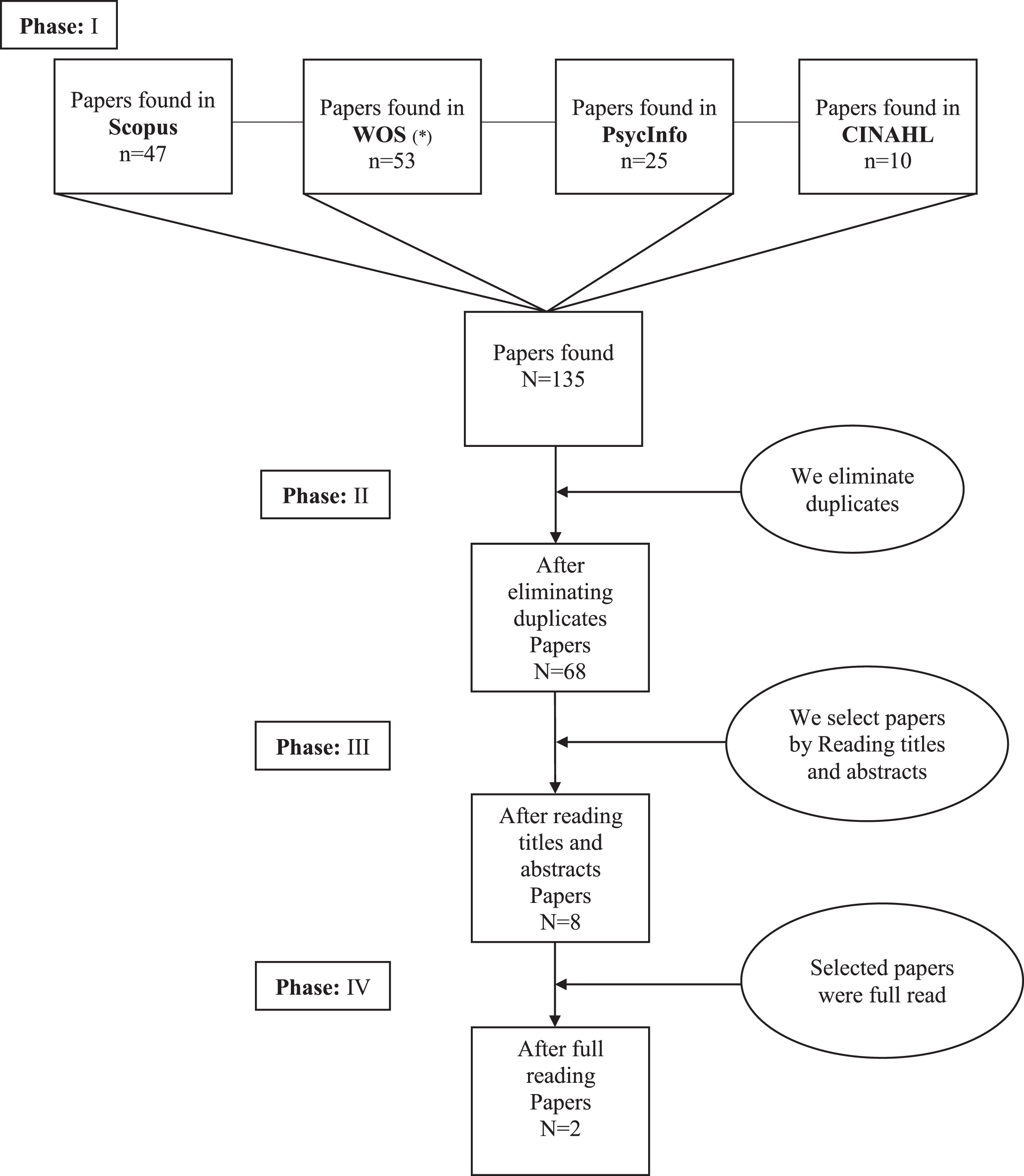
Hierarchical research process. Papers found and selected. (*)In the WOS we used three databases: 1) Web of Science Core Collection, 2) Medline, and 3) SciELO.
In the third phase, papers were screened one by one by title and by abstract. Those that did not have to do with the aim of this study were discarded, such as papers that mainly focus on: other neurological disorders that do not cause dementias, papers not focused in indirect or social cost, such as those only about direct costs, or about drugs or treatment costs. We also discarded papers about psychological, biochemical, and physiological factors, papers that only were about caregivers’ burden, papers about the questionnaire’s assessment and validation of them, and in general all the papers that do not have to do with the indirect or social costs of EYOD. Eight papers were selected for a full reading.
In the fourth phase, after the full reading, we discarded papers that even though they included in their abstracts or in their titles concepts about the indirect or social costs of EYOD, they did not perform this kind of analysis nor did they include an evaluation from the literature of this type.
Finally, only two papers were considered as papers that were relevant to the aim of this systematic review.
RESULTS
Very little is known about EYOD in comparison with LOD cases. These syndromes currently present atypical symptoms, and this delays the correct diagnosis for more than four years as some authors stated [40, 41]. The confusion is higher when the person has depression or when the syndrome debuts with mild cognitive impairment [42, 43].
These special circumstances are even more evident when we analyze the social and economic face of these types of syndromes. Some authors state that these people face inequity across the dementia pathway compared to those with late onset dementia [44]. In this sense, some caregivers of young onset cases complain about the delay in receiving funding for continuing healthcare or even about the availability of services when the person with dementia is young [45]. This is because these people are below the age at which geriatric services are available. Additionally, the psychological disturbance for caregivers is higher among EYOD cases because these syndromes are associated with late stages of life [46], and frequently in young onset cases the syndrome implies behavioral symptoms [47]. This experience of increased difficulty in coping with dementia in EYOD is common among different cultures [48].
The first noteworthy output is that there is a clear lack of studies about social and indirect costs in EYOD. Despite the relevance of the profile of people with EYOD (e.g., employment situation, diagnosis delay, lack of specific social services, etc.), in our systematic research about the indirect and social costs in EYOD cases, very few studies have been found. There are studies in different countries [15, 49–51] that evaluate these types of costs for the general profile of people with dementia, mainly for AD cases but, the economic studies for the specific group of EYOD is very infrequent.
In most of the literature discarded, even though they mention the relevant socio-economic consequences of EYOD cases in general terms, they did not perform an economic study or even mention data from other research that support their statements. Consequently, we had to dismiss many papers that were selected by title, abstracts, and even a number of the papers that were selected for a full reading [29, 53].
Between the two papers that after a full reading deserved to be included as papers with an evaluation of indirect or social costs in EYOD, one of them was about several types of dementia [6], and the other was focused on AD [36]. However, at the end of this section, we also analyzed some interesting issues of some of the discarded papers.
Selected papers
The study of Stamou et al. (2021) [6] found that people with EYOD reported receiving the diagnosis at the average age of 58 years old (range 37–65). The most common diagnosis was AD (around 50%) and the next most common diagnosis was a variant of frontotemporal dementia (12.9%); the rest reported a variety of diagnoses, with a small proportion (7.7%) not knowing nor reporting the dementia type. Most of the people with EYOD live in their own home (only 6.6% lived in a care home). The condition of being a young person with dementia seems to have an effect on the working situation. In their data, those in employment were, on average, younger and with a closer diagnosis at the moment of data collecting (2.7 versus 4.5 years for young onset versus late onset cases).
In this study [6], with a sample size of 233 people from UK, they calculated the costs of care (British pounds 2018) over a 3-month period, based on reported service use, in five groups: nurses and allied health professionals, medical, hospital inpatient, social care, and family care. The mean cost of formal care was 749.57 pounds. The informal care cost was about 9,727.36 pounds. Authors highlight that in the case of family care, the distribution was highly skewed.
Taking care of a person with EYOD is very time-consuming task. Most of the caregivers in this study (60%) reported spending more than 5 h per day supervising/helping the person with dementia and over 40% reported spending an additional 15 h per week or more on household tasks since the diagnosis.
In the study of Kandiah et al. (2015) [36] performed on a sample of 255 people from Singapore, they stated that EYOD have direct consequences on employment thus, authors reported that more patients reported loss of employment compared to those with LOD (43.2% versus 2.4%). This was also pointed out by Mayrhofer et al. (2021) [54]. EYOD patients who lost their jobs considered that it was because of the symptoms directly related to dementia. Among EYOD patients who lost their jobs, 40% were in the mild stage of dementia.
The median annual costs among community dwelling patients with EYOD were 39.26% higher among EYOD versus LOD cases. For EYOD, the median annual costs were in Singapore dollars (SGD) 21,391 (approximately US dollars (USD) 15,815 as of 31 January 2015) and that for LOD were SGD 11,356 (approximately USD 8,396). Of these costs, the indirect costs accounted for 82.6% of the total annual costs. Meanwhile in the case of LOD, the indirect costs were 68.0%. The bulk of costs in EYOD were indirect costs related to the loss of employment of the patients.
The top three cost contributors were productivity loss (68.5% of the total annual costs), informal care (14.3%), and home care (6.5%) for patients with EYOD. In contrast they did not find significant differences in terms of direct costs between YOD and LOD, except for a higher utilization of home care services among patients with LOD (37.1% versus 26.1%).
Discarded studies
Among some of the studies discarded after a full reading, we found some interesting guidelines to bear in mind. Thus, for example in the case of Huntington’s disease, a rare neurodegenerative disease that provokes YOD, a study [55] in a comparison between UK and US social services, stated that people who suffer from this condition have more difficulties with obtaining financial benefits from disability services (UK = 59.3%, US = 34.2%). Additionally, this kind of disease has a special economic burden due to the fact that they are not included in the lists of chronic diseases. The results of this are that the people with Huntington’s disease cannot use the preference prices for medications [56].
The study of Maresova et al. (2016) [49] was discarded because it was not a paper about EYOD, but in contrast they provided an interesting comparison among different strategies of measuring indirect costs in studies performed in Europe (France [57], Germany [34], and England [32]), South America [58], and the US. These studies could also not be selected due to the fact that they are not studies about EYOD.
For the case of France, indirect costs were measured by the loss of productivity, as an effect of the illness on the patient or caregiver’s abilities to work. In the German [34] and English [32] studies, they valued the indirect costs in terms of the time that informal caregivers dedicated to patients for care and supervision. In the case of South America [58], they pointed out that indirect costs should also be measured in terms of time, but they added that caregivers’ health should also be bear in mind. Finally, in the case of the US, the paper of Maresova et al. (2016) [49] mentioned different studies but all of them were about the general costs of dementia.
Differences due to the cultural and social services that are available must be considered. In a study performed in Holland in EYOD, the authors [52] stated that formal care was provided in 79.9% of the cases with an average amount of 79.6 h per month. In general, informal care is usually much higher than formal care. In this case, it seems that even the amount of formal care was higher, so the general rule was fulfilled. The amount of informal care was more than three times the amount of formal care at 259.6 hs/month. As it also happens with LOD, the amount of informal care was associated with disease severity.
Other papers [29, 53] were interesting contributions to knowledge and were included for a full reading because in a previous step, they seemed as if they could include relevant data about the issue of this research. However, these papers did not perform any evaluations of the economic costs in EYOD.
Type of publication analyzed
Finally, as it can be seen in Table 2, the topics about EYOD are of interest to the higher impact journals. Among the selected papers for a full reading, five out of eight are currently Q1 ranked journals. Most of the papers offer a description of the main cost drivers, and they frequently include an intuitive estimation of the importance of these costs but, they did not perform an analysis of the indirect or social costs in EYOD cases, with the exception of the two selected cases.
Characteristics of selected and discarded papers for a full reading and current ranking of the classification of the journals
AD, Alzheimer’s disease
DISCUSSION
EYOD comprise of a great variety of neurodegenerative diseases from different etiologies that share the common characteristic of the early age of onset, but they differ in the typologies of sign and symptoms. The fact that these syndromes debut early in life implies different social, family, and economic consequences to those that debut in old ages. It has been a striking finding, the very little studies that we have found that cover these topics.
Most of the papers selected to be considered only include statements without empirical support about the importance of the socioeconomic consequences of early onset versus late onset, but there are a dramatically small number of studies that measure the indirect and social costs in EYOD. Additionally, the empirical studies that we have found have very small samples [6, 36] (see Table 2). It is difficult to state robust conclusions about indirect or social costs with so few studies. In either case, the economic consequences are different in late and in young onset. The fact that the person with dementia in these cases is younger means that the productivity losses are greater. The study of Kandiah et al. (2015) [36] has shown that EYOD patients who lost their job considered it was because of symptoms directly related to dementia. The bulk of cost in YOD were indirect cost related to loss of employment of patients. Again, in these cases, as in other studies about the indirect or social costs independently of the moment of onset [51, 59], the biggest proportion of costs are assumed by informal (family basically) caregivers [15, 61], as shown by Stamou et al. (2021) [6] in their study for early onset cases (mean cost of formal care was 749.57 pounds. Informal care cost was about 9,727.36 pounds).
Another relevant discovery after the literature review was the fact that there is a lack of knowledge about EYOD cases in many relevant factors such as what the costs are in the cases of non-ADs (e.g., Huntington’s disease, frontotemporal dementia, dementia in Parkinson’s disease, dementia with Lewy bodies, vascular dementia, etc.). Many of them for their particular characteristics of their early symptoms such as behavioral disturbances, hallucinations, or mood disorders have serious consequences limiting social (e.g., isolation), family (e.g., divorces, altered relation with their children) and working life (e.g., unemployment and loss of jobs) [62], and consequently can reduce personal incomes.
The caregiver’s role is essential to assess the indirect and social costs in long time care, and obviously in the case of dementias. In young or early onset dementias the availability in hours is reduced due to their higher proportion of caregivers in active working situations, it means that the necessity of formal caregivers is greater, and consequently the costs. It can explain the enormous differences in the indirect costs found by Kandiah et al. (2015) [36]. Some studies [55] read in this review have pointed out additionally the difficulty of access to social services or even to social medical benefits for early onset cases due to their young age. In this circumstance, we must add that the decline in EYOD is frequently faster than in LOD [63–65]; it means that the need of support is greater in a shorter period of time.
There are a lot of questions and areas in which further studies can fill the gaps of knowledge, for instance: how the type of dementia affects the indirect costs, the differences in costs between EYOD and LOD due to comorbidities, what kind of differences are present due to sociodemographic characteristics, the effect of education [53], how the delay in diagnosis affects the costs. In reference to the last question, many papers have been alerted about this common issue [7, 66–68].
It is not usual to find published negative results in journals. To find so few studies in a systematic review could be considered a negative result but it also could be read as a very positive discovery. In our opinion the biggest strength of this paper is in line with its biggest limitation. We have found very few studies that had to do with our topic of research, indirect or social cost in EYOD. Obviously, this is a clear limitation to get conclusions about the state of knowledge in this topic. But, at the same time, this review shows opportunity windows for further work.
DISCLOSURE STATEMENT
The author’s disclosure is available online (https://www.j-alz.com/manuscript-disclosures/21-5204r1).