
Abstract
Background:
In recent years, scientific research on the gut microbiota and their relationship with some diseases, including neurological ones, has notably increased. As a result of these investigations, the so-called gut-brain axis arises. Despite its influence on the evolution and development of cognitive impairment, the gut-brain axis is little defined and demonstrated.
Objective:
To provide the best scientific evidence available on the relationship between the gut microbiota and Alzheimer’s disease.
Method:
Systematic and narrative review of the information generated in the last 5 years in national and international databases, in English and Spanish.
Results:
Eight observational studies were selected, carried out in humans and, therefore, suitable for inclusion in this review.
Conclusion:
The results of these studies support the hypothesis that there is a relationship between the gut microbiota and cognitive disorders through the gut-brain axis. However, today, there is a substantial lack of human studies, especially clinical trials, which makes it difficult to formulate clinical recommendations on this topic.
INTRODUCTION
Neurological diseases
The increase in life expectancy and the constant aging of the population carries the risk of developing some conditions, in particular, neurodegenerative diseases such as dementia. In this regard, the United Nations in 2019 reported that there were 703 million people over 65 years of age and projected that by 2050 there will be around 1.5 billion. In high-income countries, there will be an increase from 226 to more than 285 million people (MP) between 2019 and 2030, respectively [1]. This fact shows that the elderly represent an increasingly significant percentage, compared to the general population.
Aging constitutes a greater risk of contracting diseases related to some type of dementia, which affects more than 55 MP; however, it is expected to increase, by 2030, to more than 78 MP [2, 3]. The global cost of dementia is estimated to be “$817.9 billion USD” [4]. Likewise, Alzheimer’s disease (AD) is reported as the sixth cause of death and the fifth in people over 65 in the US [5].
In this sense, AD is the most common type of dementia, representing between 60% and 80% of cases [6]. Derived from neuronal degeneration, and learning and memory impairment, people living with the disease are affected in their activities of daily living, causing dependency, disability, and even mortality [7].
It has been reported that AD is characterized by an accumulation of amyloid-β (Aβ) peptides, followed by the formation of the hyperphosphorylated tau protein, accumulations of which cause neuroinflammation, which in turn triggers failure in synaptic activity and neuronal death [8, 9]. In the same vein, it has been noted that the intestinal and blood-brain barrier, having greater permeability as a consequence of aging or disease, are related to the pathogenesis of AD and other neurodegenerative disorders, because dysbiosis allows the passage of cytokines induced by lipopolysaccharides/amyloids or other small pro-inflammatory molecules [8, 9].
Microbiota
The intestinal microbiota, located in the human digestive tract, is made up of an ecosystem of around 100 billion microorganisms such as bacteria, archaea, fungi, and viruses [10]. Its composition depends on various factors, such as age, sex, diet, and race. Likewise, it is conditioned by exogenous factors such as the geographical environment, physical exercise, the consumption of medications, mainly antibiotics, smoking, alcohol consumption, and a lifestyle that causes disorders such as stress, among others [10, 11].
These last three factors are increasingly present, from an early age, in the daily routine of many people, as well as in the consumption of conventional medicines, which are abused on numerous occasions [12, 13]. As the body ages, the regenerative capacity of tissues decreases, affecting the structure of the microbiota. The transition between the adult and elderly microbiota is also characterized by a reduction in bacterial diversity, mainly of Bifidobacteria, Bacteroidetes, and Lactobacillus [14].
All these factors lead to dysbiosis, a phenomenon that consists of “qualitative or quantitative alterations of the microbiota of the digestive tract, which produce overgrowth or reduction of the microbiota” [15]. However, it is not yet clear to what extent each of these factors influences the quality of the microbiota, since it constantly changes, varying its composition throughout the day.
The fact that the intestinal microbiota is dynamic and dependent on each individual [13] makes its study particularly complex. Various studies have confirmed the importance of the microbiota in metabolic, endocrine, and protective functions against infectious and inflammatory processes.
Microbiota-gut-brain axis and neurological diseases
In addition, it collaborates in neurological function, which establishes the so-called microbiota-gut-brain axis [9, 16]. In contrast, a deficient microbiota is associated with the development of inflammatory bowel diseases, type 2 diabetes mellitus, obesity, and neurodegenerative diseases [8, 13]. In turn, although it has not yet been systematically verified, it has been suggested that a gut with poor microbiota could lead to an “unhealthy brain” [17, 18].
The microbiota-gut-brain axis is a two-way communication system that allows intestinal microorganisms to communicate with the brain, and vice versa. However, the factors of intestinal dysbiosis lead to a lower proportion of bacteria that synthesize butyrate, which generates inflammatory activity. This, in turn, triggers a compromise of the blood-brain barrier, which directly influences the accumulation of Aβ or other pro-inflammatory molecules that promote neuroinflammation and the development of AD [8, 9].
Factors affecting microbiota-gut-brain axis
Diet is recognized as the superlative modulator of the gut microbiota, so much so that cognitive health related to AD can benefit from modulating a diet focused on unsaturated fats, fruits, vegetables, and whole grains [19].
In this sense, it is known that a high fat diet can alter the composition of the intestinal microbiota by reducing several bacterial groups, such as Bifidobacterium spp., Eubacterium rectal, the group of Clostridium coccoides, and bacteria related to Bacteroides. This, in addition to promoting “metabolic endotoxemia”, a consequence of the increase in lipopolysaccharide, which causes chronic inflammation, insulin resistance, and diabetes mellitus. The intestinal microbiota participate in the conversion of plant polysaccharides to short chain fatty acids (SCFA), predominantly acetate, propionate, and butyrate [18].
It is possible that alteration of the intestinal microbiota is related to a decrease in the levels of SCFA such as butyrate, since it facilitates the microglial activation induced by the increase in the levels of lipopolysaccharide or bacterial amyloids in the CNS, which may be involved in the development of AD, suggesting another mechanism for the development of AD [19].
Currently, there have been several studies on the use of supplements that directly target gut bacteria in AD. These have shown in clinical trials that a 12-week consumption of a probiotic combination of Lactobacillus acidophilus, Lactobacillus casei, Bifidobacterium bifidum, and Lactobacillus fermentum, has significant positive effects on cognitive functioning, although no effects on oxidative stress or inflammation were observed [20].
This work aims to provide the best scientific evidence available on the relationship between gut microbiota and cognitive disorders, through the microbiota-gut-brain axis, in addition to identifying whether this relationship could be used for the prevention and treatment of dementia, specifically AD, which affects the cognitive process.
METHODS
Design
This systematic review focuses on a comprehensive search for available scientific information about the relationship between the gut microbiota and AD. For this, a systematic method was used to guide the identification, data collection, evaluation, and identification of available scientific evidence.
Search strategy
To search for information, only observational scientific articles were included, whether transversal or longitudinal, published from January 2016 to May 2020, available in open access, published in English, Spanish, and Portuguese. In addition, articles exclusively carried out in humans were searched, due to the lack of practical information in a first screening.
For information search, the DeCS and MeSH thesauri were used, for an adequate exploration of the databases. The following Boolean operators were used: AND, to establish the logical operations between concepts, OR, to retrieve documents where at least one of the specified arguments appears, and NOT to indicate that the keyword before the operator should not appear in our search.
The databases consulted were Pubmed, Scielo, Scopus, Web of Science, and BVS, making different combinations with the following keywords: “gastrointestinal microbiome”, “microbiota”, “Alzhei-mer’s disease”, “Parkinson’s disease”, and “gut microbiota”.
Study selection
The results of each search were individually checked for relevance within the scope of this systematic review; the title and full abstract were read. Documents were excluded by screening title and abstract, and those articles that did not adhere to the subject of the composition of the microbiota and the relationship with the gut-brain axis or because they were carried out in animals, as well as because they did not comply with any of the established goals, were excluded.
Evaluation of methodological quality
To assess quality, the Newcastle-Ottawa scale tool [21] was used, which consists of eight items collected in three groups that were evaluated: selection of study groups, comparability of groups and determination of exposure or outcome of interest, which assesses the quality of cohort, cross-sectional or case-control studies. The Newcastle-Ottawa scale [22] is rated by several stars according to the items evaluated; an article of high quality was considered one that has between 7 and 9 stars, moderate between 4 and 6 stars and poor between 1 and 3 stars.
RESULTS
In a first search, 599 articles were obtained, of which, after eliminating duplicates and filtering by inclusion criteria and relevance of the study, 283 articles remained. Later, after reading the abstract, 172 articles were eliminated, leaving 14 documents to evaluate the methodological quality. In the end, eight documents were included after removing the low-quality documents (Fig. 1).
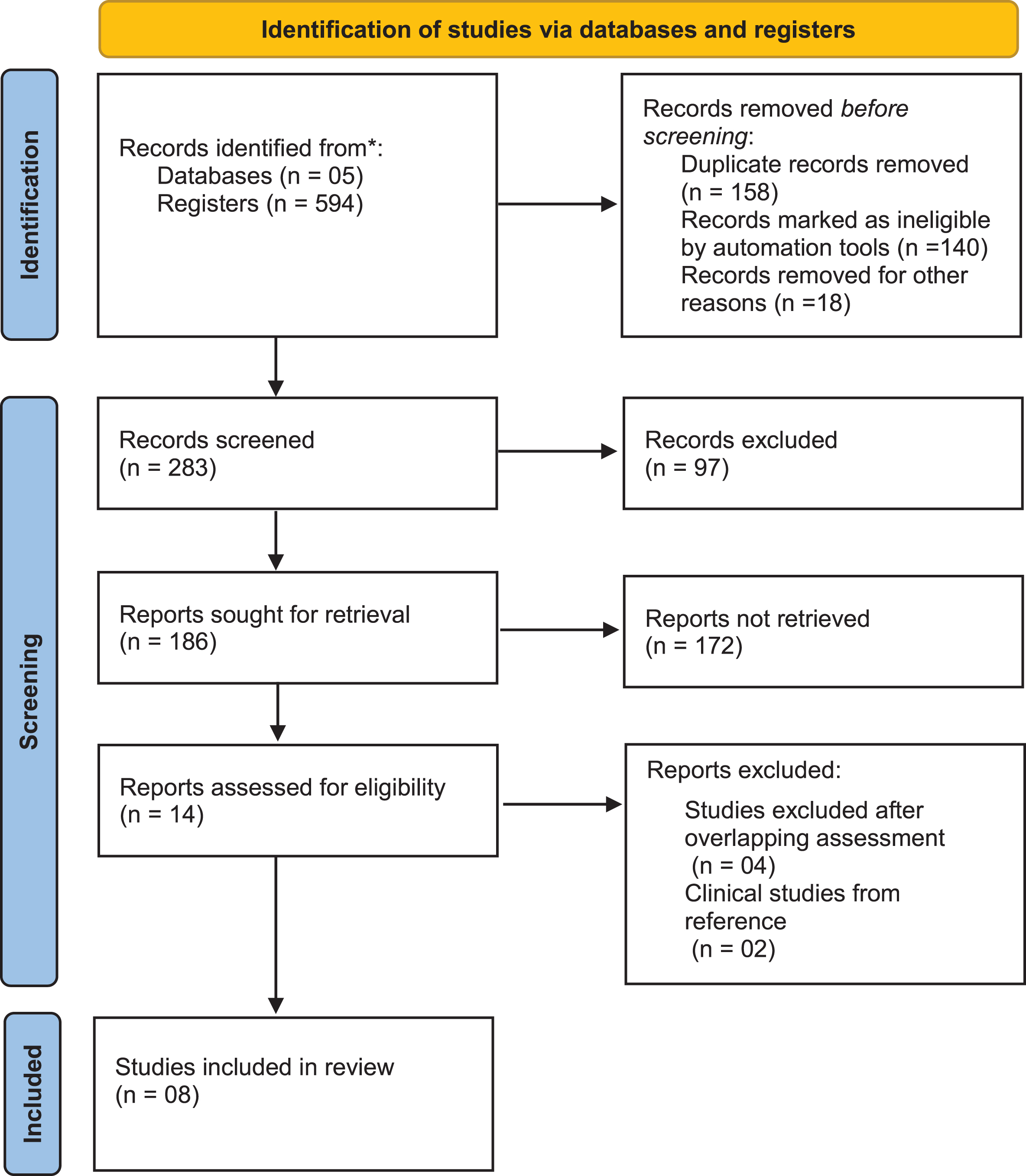
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only. *Pubmed, Scielo, Scopus, Web of Science and BVS.
In the selected studies, the US [23–27] was found as the country with the highest production in this context (5), followed by China (1) [28], Taiwan (1) [29], and Japan (1) [30].
Regarding the design of the studies carried out, both cross-sectional [23, 30] and longitudinal studies have been used alike, with 50% of the selected studies being of a cross-sectional type and the remaining 50% of a longitudinal type [24, 27, 29].
Concerning the sampling and sample size, three of them used a stratified sampling [25, 28–30], two used an intentional sampling [24, 26], one with simple random sampling [23], and another that did not specify the type of sampling [27]. The type of sample was also varied, the most common being the selection of participants with dementia, participants with mild cognitive impairment, and healthy participants. In terms of size, these samples range from 95 to 161,490 participants.
The age ranges of the frequent variations were fundamentally from 40 years onwards, although the greatest specific weight was made up of people over 60 years of age, because they are the patients with the highest incidence of mental illnesses and cognitive disorders.
Regarding the gender of the participants, in the studies there was a higher prevalence of women compared to men, although in some studies, the proportion was quite equal (Table 1).
Characteristics of included studies
AD, Alzheimer’s disease; BA, bile acids; CSF, cerebrospinal fluid; IBS, irritable bowel syndrome; IM, intestinal microbiota; MCI, mild cognitive impairment; P-gp, P-glycoprotein; SCFAs, short chain fatty acids; TMANO, Trimethylamine N-oxide.
The samples of the eight studies selected had been obtained from various fields such as research centers (25%), clinics (25%), and databases (25%), but it should be noted that the significantly larger samples were collected from the databases.
According to the results of the different studies carried out, it can be deduced that there is a relationship between the variable “deficient and not very diverse microbiota in bacteria” and the “person with Alzheimer’s disease”. On the contrary, there is a relationship between the “microbiota rich and very diverse in bacteria” and the “mentally healthy person”. This relationship is statistically significant, with p < 0.05, and clinically relevant in light of the results obtained [23–26, 28–30].
Regarding the evaluation of methodological quality, the eight documents have a good methodological implementation according to the Newcastle-Ottawa scale [21, 31], the highest percentage of quality (62.5%) is within an optimal range; therefore, they can infer a good methodology in studies.
On the other hand, some of the selected studies may have some type of bias, due to factors such as lifestyle and the diet, and their small sample size.
DISCUSSION
All the studies show that dementia and other cognitive disorders are associated with a deficient intestinal microbiota, without prejudice to the fact that, as expressly indicated in some of the studies, it would be convenient to carry out other complementary investigations that confirm and enrich the conclusions reached in these studies.
Thus, Vogt (US), in his study “Alterations of the intestinal microbiome in Alzheimer’s disease” [23], shows that the intestinal microbiome of participants with AD presents a decrease in microbial diversity, in addition to being different in its composition from that of the individuals in the control group. Likewise, he added that intestinal bacterial communities may be a therapeutic target for AD patients. The latter is very relevant, since he talks about the possibility of treating and curing diseases through the intestinal microbiota.
Chen [29] mentioned that irritable bowel syndrome is associated with an increased risk of dementia. Furthermore, he noted that this effect is obvious only in patients≥50 years of age. This indicates that having a good microbiota is especially important in the elderly.
On this point, he agrees with Saji [30], who shows that components of the gut microbiome, particularly Bacteroides and “other” bacteria, are independently associated with dementia. These associations are stronger than those of traditional dementia biomarkers. However, more studies are needed to reinforce and complement this line of work.
In this sense, knowledge about the bi-directional biochemical communication between brain and intestine and the influence of a microbiota which is bacteriologically poor and not very varied on AD is still scarce in the scientific literature, especially regarding the complete process of AD.
This lack of knowledge about mental disorders is especially serious if we consider that, worldwide, more than forty-seven million people suffered from some type of dementia in 2015, and it is estimated that this number will have tripled by the year 2050.
The concept of the microbiota-gut-brain axis originated from studies carried out in mice. This axis is a bidirectional communication system of which, due to the small number of studies carried out in humans so far, there is still little and limited knowledge of its operation and implications in brain functions. However, research supports the hypothesis that the microbiota may be the cause of some of the most serious neurodegenerative and psychiatric disorders, including AD.
The latest human research has demonstrated a novel association between the gut microbiota and dementia, suggesting that the gut microbiota can modulate host brain function through the microbiota-gut-brain axis. Thus, this review shows how the gut microbiota of people suffering from AD differs from that of subjects without dementia.
In this way, it has been possible to verify that alterations in the intestinal microbiota are associated with a wide spectrum of degenerative and psychiatric neurological pathologies that range from autism, multiple sclerosis, and Parkinson’s disease, to the most widespread dementias, such as AD [24, 27, 29].
Although it is still not entirely clear how the gut influences the development of neuropathologies, substantial research evidence supports the existence of a gut-brain axis that allows two-way communication between the gut and the brain through various pathways, including immune, endocrine, and neuronal mechanisms [32].
However, studies have shown that alterations in the intestinal microbial communities in AD patients can produce pathophysiological changes in the brain [23, 28].
As mentioned by Vogt et al. [25, 33], MahmoudianDehkordi et al. [26], and Chen et al. [29], these findings provide more information on gut microbial involvement in AD and help to understand the gut-brain axis. However, more research, including experimental work, is needed to determine the precision of the causal relationship between gut microbiota and pathogenesis of AD.
On the one hand, an interesting fact that the studies reveal is that the incidence of dementia increases with age, is higher among men than among women, and usually coincides with a higher incidence of comorbidity. In this sense, people over fifty years of age showed a greater risk of suffering from dementia, a risk that progressively increased with age [24, 27, 29].
On the other hand, it should be noted that some of the studies analyzed in this work could have some type of bias, mainly due to the size of the sample and because diet, lifestyle, exposure, and other factors may contribute to the differences in the microbiota of the groups.
However, in late 2021, from a double-blind multicenter randomized clinical trial, Kim et al. [34] found that the relative abundance of inflammatory-causing gut bacteria was significantly reduced at week 12 in a probiotic group (p < 0.05). Furthermore, the probiotic group showed greater improvement in the mental flexibility test and stress score than the placebo group (p < 0.05). Unlike placebo, probiotics significantly increased the serum level of brain-derived neurotrophic factor (BDNF) (p < 0.05). Notably, gut microbes displaced by probiotics (Eubacterium and Clostridiales) showed a significant negative correlation with serum BDNF level only in the probiotic group (RS = –0.37, RS = –0.39, p < 0.05).
With this, they showed the benefits of supplementation with probiotics, since they promote mental flexibility and relieve stress in healthy older adults, in addition to causing changes in the intestinal microbiota.
Furthermore, these results can be supported by the findings of Tran et al. [35], in which the influence on the structure and function of the intestinal microbiome in humans and mice was explored, where there was evidence of a link between the genotypes of apolipoprotein E (APOE) and the composition of the intestinal microbiome. In this study, they point out that the loss of butyrate- and SCFA-producing bacteria in APOE4 carriers could drive the impact of the APOE4 allele on neuropathology. This suggests a possible role of the buryate-producing bacteria of the intestinal microbiota as a point of intervention to mitigate the impact of the APOE genotype in the development of AD.
Nevertheless, additional studies with larger samples are needed to corroborate and expand what has been discovered so far. But above all, more longitudinal studies are required that cover the pre-symptomatic stages of the disease. Also, studies are needed to establish the influence of changes, composition, and activity of the intestinal microbiota in patients with AD, so that it can be studied in different periods, in addition to carrying out follow-up investigations in the patient to define the cause-effect relationship begun by Vogt et al. [25, 33], MahmoudianDehkordi et al. [26], and Chen et al. [29].
Study limitations
The fact that the intestinal microbiota is unique, dynamic, changing, and easily adjustable by external factors, such as diet and lifestyle, makes studying it difficult. However, evidence is being generated that highlights the effect of inflammation on intestinal homeostasis. A route of action for research is outlined in the search for strategies that preserve the proportion and prevalence of gut microbiota by modulating inflammation.
Furthermore, despite these findings, the information available comes primarily from animal studies. Therefore, many clinical trials in humans are necessary, providing us with better and more precise knowledge of the intestinal microbiota before making the appropriate recommendations for clinical practice.
Conclusion
There is a high association between the decrease in the richness of the microbiota and the incidence of AD. According to the evidence found, the existence of a gut-brain axis and its relationship with the gut microbiota in dementia is highly probable. In addition, the composition of gut microbiota, such as Bacteroides or bacteria such as Clostridium difficile, is a factor that is specifically associated with dementia and AD.
The ability to modulate the intestinal microbiota reveals a relevant field to conduct research and develop new strategies to prevent cognitive and other disorders.