
Abstract
Background:
The effect of weight modification on future dementia risk is currently a subject of debate and may be modified by age.
Objective:
The aim of the present study was to investigate the association between body mass index (BMI) status with mild cognitive impairment (MCI) (a preclinical stage of dementia) in middle-aged and older adults residing in six low- and middle-income countries using nationally representative data.
Methods:
Cross-sectional data from the Study on Global Ageing and Adult Health (SAGE) were analyzed. MCI was defined using the National Institute on Aging-Alzheimer’s Association criteria. BMI (kg/m2) was based on measured weight and height and categorized as: underweight (<18.5), normal (18.5–24.9), overweight (25.0–29.9), and obese (≥30.0). Multivariable logistic regression analysis and meta-analysis were conducted to assess associations.
Results:
Data on 32,715 individuals aged ≥50 years with preservation in functional abilities were analyzed [mean (SD) age 62.1 (15.6) years; 51.7% females]. Among those aged 50–64 years, compared to normal weight, underweight (OR = 1.44; 95% CI = 1.14–1.81), overweight (OR = 1.17; 95% CI = 1.002–1.37), and obesity (OR = 1.46; 95% CI = 1.09–1.94) were all significantly associated with higher odds for MCI. In those aged ≥65 years, underweight (OR = 0.71; 95% CI = 0.54–0.95) and overweight (OR = 0.72; 95% CI = 0.55–0.94) were associated with significantly lower odds for MCI, while obesity was not significantly associated with MCI.
Conclusion:
The results of the study suggest that the association between BMI and MCI is likely moderated by age. Future longitudinal studies are required to confirm or refute the present findings before recommendations for policy and practice can be made.
INTRODUCTION
Dementia is an umbrella term used to describe a collection of syndromes that result in impaired ability to remember, think, or make decisions that interferes with performing everyday activities [1]. Globally, approximately 50 million people have dementia and approximately 60% of those with dementia reside in low- and middle-income countries (LMICs) [2]. Dementia is a significant global problem as it is a major cause of disability and dependency among older people worldwide. For example, in 2015, the total global societal cost of dementia was estimated to be US$ 818 billion, equivalent to 1.1% of global gross domestic product [2]. Since there are currently no disease modifying treatments for dementia [3] there is the need to identify modifiable risk factors for the preclinical transitional stages of dementia such as mild cognitive impairment (MCI).
MCI is an early stage of memory loss or other cognitive ability loss (such as language or visual/spatial perception) in individuals who maintain the ability to independently perform most activities of daily living [4]. It is important to note that there is no specific test for the diagnosis of MCI and a judgement is usually made based on the following criteria: 1) problems with memory or another mental function; 2) mental function has declined over time; 3) daily activities are generally not impaired; 4) mental status testing shows a mild level of impairment for age and education level; and 5) diagnosis is not dementia [5]. MCI has a high progression rate to dementia (12%, 20%, and 50% at 1, 3, and 5 years, respectively) [6], and is increasingly being considered an important stage for intervention to prevent or delay the onset of dementia.
There is currently growing interest in body mass index (BMI; particularly overweight and obesity) as a risk factor for MCI or dementia. A recent meta-analysis including longitudinal studies from high-income countries found that high BMI in mid-life is associated with greater risk for dementia onset, but that the opposite is true in late life [7]. This suggests that weight reduction, only in mid-life, may lead to lower dementia risk. In a more recent large epidemiological study including 1,349,857 dementia-free middle-aged participants from 39 cohort studies, it was concluded that the association between BMI and dementia is likely to be attributable to two different processes:(1) a harmful effect of higher BMI, which is observable in long follow-up, and 2) a reverse-causation effect that makes a higher BMI to appear protective when the follow-up is short [8]. In another recent study of 3632 US participants aged 20 to 60 years, it was found that each 1 kg/m2 increase in BMI at 40–49 years was associated with higher risk of dementia, but lower risk after 70 years [9].
It is possible that high adiposity leads to cog-nitive impairment via a range of potential mechanisms including impaired cerebral metabolism [10], elevated leptin [11], inflammation, and neuronal degradation [12]. On the other hand, being underweight may also be a risk factor for MCI or dementia via frailty and undernutrition [13, 14].
However, there are only a small number of studies on the association between BMI and MCI (a critical stage to intervene to prevent dementia), with most studies being of small sample size and from high-income settings, despite the fact that dementia is expected to increase rapidly in low-economic regions [2]. Moreover, current data suggests that the prevalence of MCI in LMICs is high. For example, a recent systematic review found that in LMICs, the prevalence of amnesic MCI using the Petersen criteria ranged from 0.6% to 22.3%. Similar variability existed across studies using the International Working Group Criteria for amnestic MCI (range 4.5% to 18.3%) and all-MCI (range 6.1% to 30.4%) [15]. In addition, the number of people with overweight and obesity is increasing in LMICs [16] and the prevalence of undernutrition is high [17]. Thus, data that can shed light on the potential role of weight modification on MCI/dementia prevention in this setting is of substantial importance. Given this background, the aim of the present study was to investigate the association between BMI status (i.e., underweight, overweight, obesity) with MCI in 32,715 middle-aged and older adults residing in six LMICs.
METHODS
The survey
Data from the Study on Global Ageing and Adult Health (SAGE) were analyzed. These data are publicly available through: http://www.who.int/healthinfo/sage/en/. This survey was undertaken in China, Ghana, India, Mexico, Russia, and South Africa between 2007 and 2010. These countries broadly represent different geographical locations and levels of socio-economic and demographic transition. Based on the World Bank classification at the time of the survey, Ghana was the only low-income country, and China and India were lower middle-income countries although China became an upper middle-income country in 2010. The remaining countries were upper middle-income countries.
Details of the survey methodology have been published elsewhere [18]. Briefly, in order to obtain nationally representative samples, a multistage clustered sampling design method was used. The sample consisted of adults aged ≥18 years with oversampling of those aged ≥50 years. Trained interviewers conducted face-to-face interviews using a standard questionnaire. Standard translation procedures were undertaken to ensure comparability between countries. The survey response rates were: China 93%; Ghana 81%; India 68%; Mexico 53%; Russia 83%; and South Africa 75%. Sampling weights were constructed to adjust for the population structure as reported by the United Nations Statistical Division [19]. Ethical approval was obtained from the WHO Ethical Review Committee and local ethics research review boards. Written informed consent was obtained from all participants.
Mild cognitive impairment
MCI was ascertained based on the recommendations of the National Institute on Aging-Alzheimer’s Association [20]. We applied the identical algorithms used in previous SAGE publications using the same survey questions to identify MCI [21, 22]. Briefly, individuals fulfilling all of the following conditions were considered to have MCI: Concern about a change in cognition: Individuals who replied ‘bad’ or ‘very bad’ to the question “How would you best describe your memory at present?” and/or those who answered ‘worse’ to the question “Compared to 12 months ago, would you say your memory is now better, the same or worse than it was then?” were considered to have this condition. Objective evidence of impairment in one or more cognitive domains: was based on a < –1 SD cut-off after adjustment for level of education, age, and country. Cognitive function was assessed through the following performance tests: word list immediate and delayed verbal recall from the Consortium to Establish a Registry for Alzheimer’s Disease [23], which assessed learning and episodic memory; digit span forward and backwards from the Weschler Adult Intelligence Scale [24], that evaluated attention and working memory; and the animal naming task [23], which assessed verbal fluency. Preservation of independence in functional abilities: was assessed by questions on self-reported difficulties with basic activities of daily living (ADL) in the past 30 days [25]]. Specific questions were: “How much difficulty did you have in getting dressed?” and “How much difficulty did you have with eating (including cutting up your food)?” The answer options were none, mild, moderate, severe, and extreme (cannot do). Those who answered either none, mild, or moderate to both of these questions were considered to have preservation of independence in functional activities. All other individuals were deleted from the analysis (935 individuals aged ≥50 years). No dementia: Individuals with a level of cognitive impairment severe enough to preclude the possibility to undertake the survey were not included in the current study.
Body mass index
Height was measured using a stadiometer, and weight was measured using an electronic weighing scale that was periodically calibrated. Weight and height measurements were taken with participants wearing only one layer of clothes and with their shoes off; height was recorded to the nearest 0.1 cm with a stadiometer, while weight was measured to the nearest 0.1 kg with a weighting scale. BMI was calculated as weight in kilograms divided by height in meters squared based on measured weight and height and classified as underweight (BMI < 18.5 kg/m2), normal weight (BMI 18.5–24.9 kg/m2), overweight (BMI 25.0–29.9 kg/m2), and obesity (BMI ≥30 kg/m2) in line with WHO guidelines [26].
Control variables
The control variables were selected based on past literature [27] and included age, sex, wealth quintiles based on income, years of education received, physical activity, alcohol use, smoking (never, current, former), depression, anxiety, sleep problems, diabetes, hypertension, and stroke. Levels of physical activity were assessed with the Global Physical Activity Questionnaire and were classified as low, moderate, and high based on conventional cut-offs [28]. Consumers of at least four (females) or five drinks (males) of any alcoholic beverage per day on at least one day in the past week were considered to be ‘heavy’ drinkers. Those who had ever consumed alcohol but were not heavy drinkers were categorized as ‘non-heavy’ drinkers [29]. Questions based on the World Mental Health Survey version of the Composite International Diagnostic Interview [30] were used for the endorsement of past 12-month DSM-IV depression [31]. Those who claimed to have severe/extreme problems with worry or anxiety in the past 30 days were considered to have anxiety [32]. Sleep problems were assessed by the question “Overall in the last 30 days, how much of a problem did you have with sleeping, such as falling asleep, waking up frequently during the night or waking up too early in the morning?” and those answering severe or extreme were considered to have sleep problems [33]. Stroke and diabetes were based solely on self-reported lifetime diagnosis. Hypertension was defined as having at least one of: systolic blood pressure ≥140 mmHg; diastolic blood pressure ≥90 mmHg; or self-reported diagnosis.
Statistical analysis
The statistical analysis was performed with Stata 14.1 (Stata Corp LP, College station, Texas). The analysis was restricted to those aged ≥50 years. The middle-aged were also included in our study as from the point of prevention of dementia, intervening in middle-age is now considered important [34], especially that cognitive dysfunction can manifest up to 10 years before a dementia diagnosis [35]. The analysis was stratified by age (i.e., middle-aged 50–64 years and older adults ≥65 years) as a previous study showed that the association between BMI and MCI may differ between these age groups [27]. Multivariable logistic regression analysis was conducted to assess the association between BMI (independent variable with normal weight as the reference category) and MCI (dependent variable) using country-wise samples while simultaneously adjusting for age, sex, wealth, education, physical activity, alcohol use, smoking, depression, anxiety, sleep problems, diabetes, hypertension, and stroke. The Higgins’s I2 based on estimates from each country was also calculated in order to assess between-country heterogeneity. The Higgins’s I2 represents the degree of heterogeneity that is not explained by sampling error with a value of < 40% often considered as negligible and 40–60% as moderate heterogeneity [36]. A pooled estimate was obtained by random-effects meta-analysis.
The sample weighting and the complex study design were taken into account in the analyses. Results from the regression analyses are presented as odds ratios (ORs) with 95% confidence intervals (CIs). The level of statistical significance was set at p < 0.05.
RESULTS
The final sample included 32,715 individuals (China n = 12,815; Ghana n = 4,201; India n = 6,191; Mexico n = 2,070; Russia n = 3,766; South Africa n = 3,672) aged ≥50 years with preservation in functional abilities. There were 19,092 individuals between the ages of 50 and 64 (63.3%), and 13,623 aged≥65 years (36.7%). Overall, the mean (SD) age was 62.1 (15.6) years while 51.7% were females. The overall prevalence of MCI was 15.3%, while that of underweight, normal weight, overweight, and obesity was 16.2%, 47.8%, 24.5%, and 11.5%, respectively. The sample characteristics by country are provided in Table 1. The prevalence of MCI ranged from 7.4% in Ghana to 24.3% in China, while the prevalence of underweight and obesity were particularly high in India (38.4%) and South Africa (46.6%), respectively.
Sample characteristics by country
SD, Standard deviation; Data are % unless otherwise stated.
The association between underweight (versus normal weight) weight is shown in Fig. 1. Among those aged 50–64 years, overall, underweight was associated with a significant 1.44 (95% CI = 1.14–1.81; I2 = 0.0%) times higher odds for MCI, while for those aged ≥65 years, underweight was significantly associated with lower odds for MCI [0.71 (95% CI = 0.54–0.95; I2 = 19.5%)]. In terms of overweight (versus normal weight), among the middle-aged, overweight was significantly associated with higher odds for MCI [OR = 1.17 (95% CI = 1.002–1.37; I2 = 0.0%)], and among older adults, overweight was significantly associated with lower odds for MCI [0.72 (95% CI = 0.55–0.94; I2 = 26.8%)] (Fig. 2). As for obesity (versus normal weight), this was associated with a significantly higher odds for MCI among the middle-aged (OR = 1.46; 95% CI = 1.09–1.94; I2 = 5.5%), but this was not significantly associated with MCI among older adults (Fig. 3).
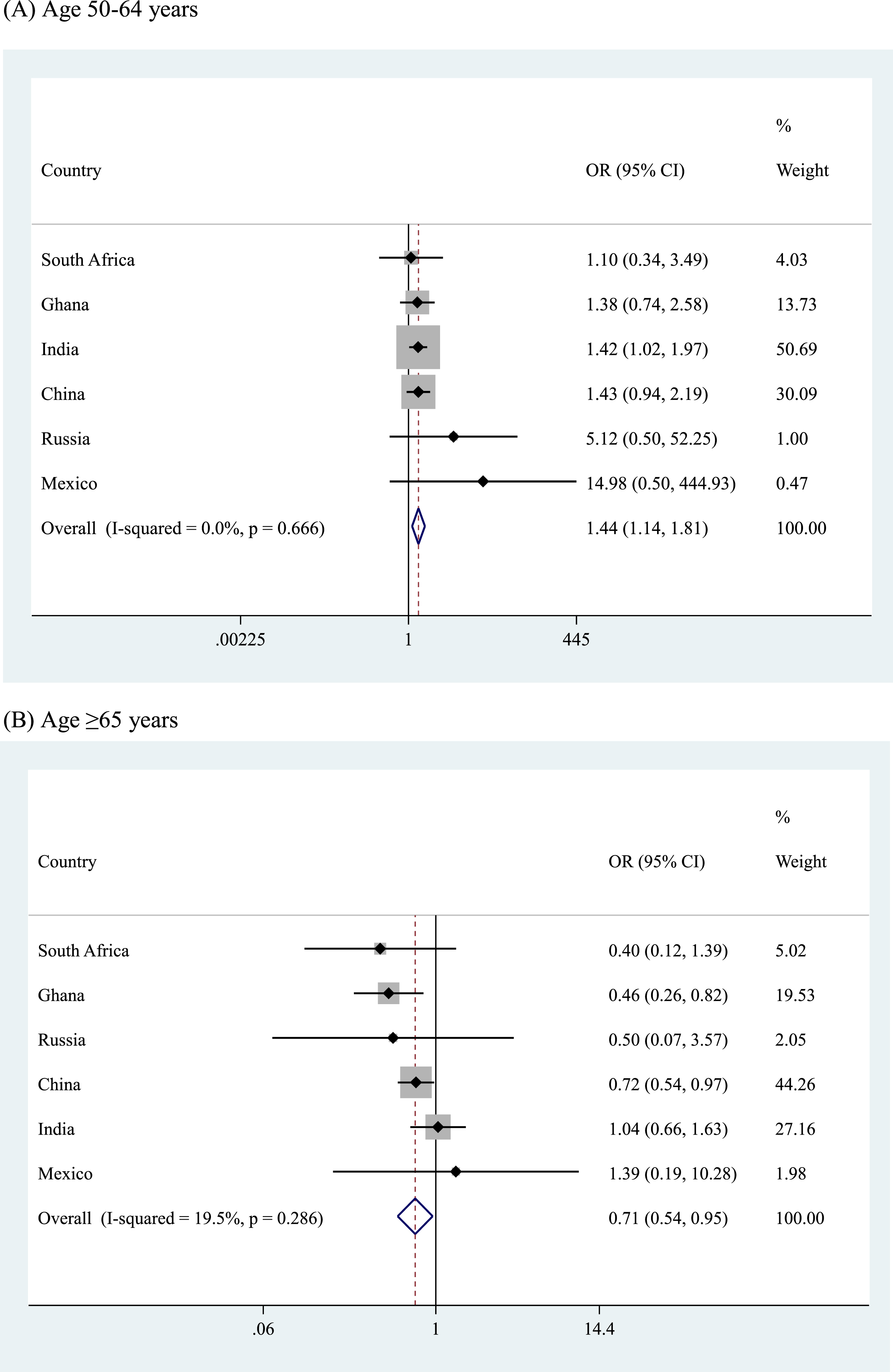
Country-wise association between underweight (versus normal weight) among people aged (A) 50–64 years and (B) ≥65 years estimated by multivariable logistic regression. OR, Odds ratio; CI, Confidence interval. Models are adjusted for age, sex, wealth, education, physical activity, alcohol use, smoking, depression, anxiety, sleep problems, diabetes, hypertension, and stroke. Overall estimate was obtained by meta-analysis with random effects.

Country-wise association between overweight (versus normal weight) among people aged (A) 50–64 years and (B)≥65 years estimated by multivariable logistic regression. OR, Odds ratio; CI, Confidence interval. Models are adjusted for age, sex, wealth, education, physical activity, alcohol use, smoking, depression, anxiety, sleep problems, diabetes, hypertension, and stroke. Overall estimate was obtained by meta-analysis with random effects.

Country-wise association between obesity (versus normal weight) among people aged ≥65 years estimated by multivariable logistic regression. OR, Odds ratio; CI, Confidence interval. Models are adjusted for age, sex, wealth, education, physical activity, alcohol use, smoking, depression, anxiety, sleep problems, diabetes, hypertension, and stroke. Overall estimate was obtained by meta-analysis with random effects.
DISCUSSION
Main findings
Results from this large multi-country sample of middle-aged and older age adults showed that in middle-aged adults, underweight, overweight, and obesity are significantly associated with higher odds for MCI when compared to normal weight. In contrast, in older adults, underweight and overweight were associated with significantly lower odds for MCI. Although obesity was associated with 0.74 (95% CI = 0.49–1.14) times lower odds for MCI in older adults, this was not statistically significant. The level of between-country heterogeneity in these associations was in general low.
Interpretation of the findings
One meta-analysis including longitudinal data found that overweight and obesity in middle-age was associated with a non-significant 1.10 (95% CI =0.99–1.22) and a significant 1.41 (95% CI = 1.20–1.60) times higher risk for dementia onset, respectively. In older adults, overweight was non-sig-nificantly (RR = 0.88; 95% CI = 0.74–1.02) and obesity significantly (RR = 0.83; 95% CI = 0.74–0.94) associated with lower odds for dementia onset [5]. Our results are somewhat similar to the results of this meta-analysis and add to this previous literature by suggesting that weight reduction in middle-aged adults who are overweight may potentially lead to a reduced dementia risk in LMICs. In addition, our finding that underweight was associated with higher odds for MCI in middle-aged adults supports one previous longitudinal study that identified that underweight in mid-life is positively associated with dementia [37]. More research is needed to test whether addressing overweight and obesity may lead to decreased risk for future MCI/dementia onset, and whether maintenance of normal weight in middle-aged adults may be particularly important in LMICs.
The finding that overweight/obesity was associated with higher odds for MCI in the middle-aged may be explained by mechanisms that cause brain volume reduction such as inflammation, cardiovascular risk factors, and low physical activity [7]. As for the lower odds for MCI in older individuals with overweight observed in our study, there are several hypotheses that may explain this. First, overweight that occurs in older adulthood (following periods of relatively normal weight throughout middle-age) may impact cognition less than being overweight starting in middle age or earlier in the life course [38]. Second, older adults who have a higher BMI are often less likely to have frailty or other comorbidities, and this may have a protective effect on cognitive impairment [39].
The higher odds for MCI among underweight middle-aged individuals may be explained by several factors. First, underweight in middle-age may be associated with eating disorders, and these have been found to affect memory function. For example, anorexia nervosa is associated with disruption of functioning of the visuo-spatial sketch pad and central executive components of working memory [40]. Next, underweight may be associated with undernutrition, which is associated with cognitive impairment via micronutrient and macronutrient deficiency [41, 42]. Finally, underweight may be a sign of the presence of other comorbidities or frailty, which can increase risk for cognitive decline, but were not assessed in the present study [43]. As for the finding that underweight was associated with lower odds for MCI in older adults, mechanistic and epidemiologic evidence suggests that MCI or dementia may cause involuntary weight loss well before its clinical onset [37], and low BMI may spuriously appear to be protective against MCI or dementia.
Public health implications and areas for future research
Findings from the present study suggest that maintenance of normal weight only in mid-life may possibly lead to lower MCI and dementia risk in LMICs. In the context of LMICs and to achieve weight reduction in mid-life for people with overweight/obesity, lifestyle interventions that includes both diet and physical activity components may be most effective [44]. Moreover, action planning and self-monitoring of outcomes of behavior have been found to achieve best results, and thus any lifestyle intervention to achieve weight loss in this setting should consider embedding such techniques [45]. The Exercise is Medicine Global Initiative is designed to support health care professionals in prescribing exercise for patients by training providers to assess patient physical activity levels, imparting behavioral counseling to increase activity using change models, and referring patients to resources to facilitate physical activity [46]. Importantly, this initiative already exists in LMICs, and evaluation of its impact will provide important data on how to adapt and scale up this program to encourage healthy activity levels and weight status [47].
Strength and limitations
The large sample of middle-aged and older adults across six LMICs is a clear strength of the present study. However, findings from this study must be interpreted in light of the study limitations. First, the study was cross-sectional in nature, and therefore, temporal associations or causality cannot be established. Clearly, future longitudinal and intervention studies are necessary to understand the mechanisms that underlie the associations observed and to clarify the effect of weight modification on future risk of MCI or dementia.
Second, we did not have information on weight trajectories over the life course, despite the fact that this has also been reported to be important in determining risk for MCI/dementia. Third, participants with mild forms of dementia could have been included in our study sample as the study did not include a clinical assessment of dementia. Fourth, we did not have information on nutritional factors, while the data on physical activity used in our study was only on current levels of physical activity. Physical activity during the life course and nutritional factors are known to influence BMI, and also risk for MCI or dementia [48, 49] and thus, residual confounding is possible. Fifth, the use of BMI as an exposure may be a further limitation as BMI does not measure adiposity (although heavily correlated) or fat free mass [50]. Indeed, this may lead to some data distortion in older adults as more fat free muscle mass is associated with less cognitive issues [51]. Finally, the countries included in the study were not randomly selected. Thus, the results are not generalizable to all LMICs or high-income countries
Conclusions
In this large sample of middle-aged and older adults from six LMICs, it was found that underweight, overweight, and obesity are significantly associated with higher odds for MCI in the middle-aged, but that underweight and overweight are associated with significantly lower odds for MCI in older adults. These findings add to the current debate on whether weight modification has a role in the prevention of dementia.
Footnotes
ACKNOWLEDGMENTS
This paper uses data from WHO’s Study on Global Ageing and Adult Health (SAGE). SAGE is supported by the U.S. National Institute on Aging through Interagency Agreements OGHA 04034785, YA1323–08-CN-0020, Y1-AG-1005–01 and through research grants R01-AG034479 and R21-AG034263.