
Abstract
Background:
The relationship between body mass index (BMI) and dementia is inconclusive. Undesirable loss of fat-free mass is a risk factor for cognitive decline while obesity is also a risk factor for cardio-metabolic disorders among the older adults.
Objective:
This study aimed to examine the association between BMI and incident all-cause dementia among Chinese older adults using a prospective study.
Methods:
Participants were 1,627 community residents aged 60 or older without dementia from the Shanghai Aging Study. Cox regression models, incorporated with restricted cubic splines, were used to explore a nonlinear association between baseline BMI and risk of all-cause dementia as measured by hazard ratio (HR) using both frequentist and Bayesian approach.
Results:
We diagnosed 136 incident dementia cases during the mean follow-up of 5.3 years. Compared with moderate BMI (18.5–24.0 kg/m2), low BMI (< 18.5 kg/m2) were related to an increased risk of dementia with the HR as 3.38 (95% CI 1.50–7.63), while high BMI (≥24.0 kg/m2) showed a decreased risk of dementia without statistical significance (HR = 0.91, 95% CI 0.60 to 1.39). Sensitivity analysis in participants without central obesity indicated that the association was still significant with even higher HR. Bayesian approach presented the similar results.
Conclusion:
Our result indicates that low BMI may contribute to high risk of incident dementia, even in individuals without central obesity.
INTRODUCTION
Dementia is a progressive brain disorder accompanied by a deterioration of memory and thinking, as well as a decrease in motivation and emotional and language problems [1]. Dementia is a global public health problem, and its impact is bound to increase in the future, with a rapidly aging world population [2]. Dementia has nonreversible physical, mental, economic, and social damage on patients and their caregivers [3]. Without effective treatment, prevention against cognition impairment is more vital to slow down the development of dementia.
Body mass index (BMI) is a widely-accepted, con-venient measurement showing stable and valid asse-ssment on body fat and health status [4]. Although this indicator leaves a lot to be desired on its accuracy, its widespread use in population and medical research shows no sign of abating [4]. BMI-cognition association in previous community-based studies was not consistent [5–10]. Some demonstrated that low BMI increased the risk of cognitive decline while higher BMI might be a protective factor [10–14]. However, a few studies raised the opinion that weight status is unlikely to be a plausible intervention target for dementia [15, 16]. Categorizing BMI or assuming a linear relationship between BMI and dementia may lead to biases. Thus, smoothing techniques were expected to use to avoid bias. Some observational studies reported inconsistent results of the relationship between BMI and cognitive impairment when taking waist-hip ratio (WHR) into consideration [17, 18]. We therefore hypothesized that there may be an association between BMI and risk of cognitive impairment, and central obesity may alter the effects of BMI on cognitive impairment to some extent.
The Shanghai Aging Study is a population-based cohort study with a design, operational procedures, and diagnostic criteria similar to most cohort studies in western countries. Our previous cross-sectional study found a significant correlation between lower BMI and prevalent mild cognitive impairment (MCI) at the baseline [19]. The current prospective study further examined the association between BMI and risk of dementia among older adults in urban Shanghai.
METHODS
Study participants
Between January 2010 and December 2012, 2,985 permanent residents aged ≥60 years were recruited for the Shanghai Aging Study from the Jing’ansi community in Shanghai, China. Participants were excluded if they were 1) living in nursing homes or other institutions; 2) experiencing mental deficiency or severe schizophrenia, according to their medical records; or 3) having severe impairment of hearing, vision, or verbal function that could not accomplish the neuropsychological evaluation. Detailed recruitment procedures were published previously [20].
This study was approved by the Medical Ethics Committee of Huashan Hospital, Fudan University, Shanghai, China (No. 2009-195). Written informed consent was obtained from all participants and/or their legal guardians.
Characteristics and apolipoprotein E genotype
At baseline, the demographics characteristics of the participants were collected via an interviewer administered questionnaire, including age, gender, years of formal education, smoking, and drinking behaviors. Smoking status was defined if the participant had smoked in the past one month. Alcohol consumption was defined if the participants had at least one serving of alcohol weekly during the past year [21]. Medical histories, such as hypertension and type 2 diabetes, were recorded and further confirmed based on the participants’ medical records.
The apolipoprotein E (APOE) ɛ4 allele is recognized as a major generic risk factor for sporadic late-onset Alzheimer’s disease (AD). DNA was extracted from the blood or saliva samples of each participant to conduct APOE genotyping using the TaqMan SNP method [22]. The presence of at least one ɛ4 allele designated the participant as APOE ɛ4 positive.
Anthropometric measurements
Anthropometric measurements included measu-rements of height, weight, and waist and hip circumferences, and were measured by research nurses. Body mass index (BMI) was then calculated as weight in kilograms (kg) divided by height in meters (m) squared. To calculate waist to hip circumference (WHR), the waist circumference was divided by the hip circumference. Central obesity was defined as WHR > 0.85 in females, > 0.90 in males [23].
Neurological and neuropsychological assessments and diagnosis
At baseline, neurologists examined each participant’s motor responses and reflexes. Each participant was administered a battery of neuropsychological tests for global cognition, executive function, special construction function, memory, language, and attention. The battery of tests contained the following: 1) the Mini-Mental State Examination [24]; 2) the Conflicting Instructions Task (Go/ No Go Task) [25]; 3) the Stick Test [26]; 4) the Modified Common Objects Sorting Test [26]; 5) the Auditory Verbal Learning Test [26]; 6) the Modified Fuld Object Memory Evaluation [27]; 7) the Trail-making tests A and B [28]; 8) the RMB (Chinese currency) test [29]]. Participants with < 6 years of education were given tests 1 to 4, 6, and 8. Participants with ≥6 years of education were given test 1 to 5, and 7. Normative data and more details of these tests were reported elsewhere [20]. All tests were conducted in Chinese by study psychometrists within 90 minutes. Neurologists also administered the clinical dementia rating (CDR) [30] and the Lawton and Brody Activity of Daily Living (ADL) [31] to elicit memory complaints and the ability to perform activities of daily living.
After each clinical assessment, a panel of neurologists, neuropsychologists, and research coordinators reviewed the physical examinations, neuropsychological tests, and functional ability, respectively for each participant and reached a consensus diagnosis for dementia using the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) [32]. We used NINCDS-ADRDA criteria to diagnose AD [33]. We diagnosed vascular dementia based on the clinical and radiological evidence of vascular diseases according to the NINDS-AIREN criteria [34]. Detailed diagnostic procedures have been reported before [35].
Follow-up procedure
From April 1, 2014, to December 31, 2016, dem-entia-free participants with valid anthropometric measurements at baseline were scheduled to follow-up. Research coordinators contacted participants using their contact information provided at the beginning of the study. Cognitive function was evaluated again, using the same neuropsychological battery that was previously used at the baseline. A consensus diagnosis of incidence dementia was concluded by the same panel of experts, using the same diagnostic criteria at the baseline.
Statistical analysis
We only included participants followed more than 2 years as our full data set. We excluded participants without diagnosis in the follow up and filled the missing values with mean/median values for baseline variables [36]. The mean with the standard deviation (SD) and numbers with frequencies (%) were used to describe continuous and categorical variables respectively. The analysis of variance (ANOVA) test was used to analyze the differences between continuous variables. The Pearson’s chi-squared test was used to tell the differences among categorical variables. For individuals with incident dementia, the follow-up time was defined as the duration from base-line investigation to the diagnosis of dementia. For those who did not develop dementia, the follow-up time was defined as the duration from baseline assessment to the follow-up interview. The incidence of dementia was calculated as the number of new-onset cases divided by the cumulative person-years of follow-up. Cox regressions combined with spline BMI were used to determine the nodes. Considering current clinical applications of BMI categories, the variable BMI was then categorized into low (BMI < 18.5 kg/m2), moderate (18.5≤BMI < 24.0 kg/m2), and high (BMI≥24.0 kg/m2) to estimate the hazard ratio (HR) with 95% confidence intervals (CIs) for dementia. Model 1 adjusted for restricted cubic spline (RCS) on BMI. Model 2 additionally adjusted for gender, age, and years of education. Model 3 added variables of APOE ɛ4, smoking, alcohol drinking, depression mood, diabetes, hypertension, hyperlipidemia, and stroke. Sensitivity analysis was used for the assessment of a model’s overall uncertainty by excluding participants with central obesity in Model 4. Proportional hazards (PH) hypothesis testing for models were performed. Stratified subgroup analyses were performed according to sex, stroke, hypertension, and APOE ɛ4 allele. Significance tests of each stratum were using the Wald test.
Bayesian version of cox model was used to report 95% HPD credible interval (CrI) [37]. The following parameters were specified: number of iterations (= 20,000), thinning interval (= 1), burn-in (= 2,000). Estimated hazard ratios and 95% credible intervals were then derived from 20,000 simulated draws from the approximate posterior distribution using the mean along with 2.5 and 97.5 percentiles. Given the small number of participants in low BMI subgroup, all results should be interpreted with caution, and we recommend to focus on effect estimates rather than statistical significance [38]. Since noninformative prior distributions for the regression coefficients were used, the mean and standard deviations of the posterior distributions for the model parameters are close to the maximum likelihood estimates and standard errors. Data analysis was conducted using R, version 4.1.0, and SAS, version 9.4 (SAS Institute Inc).
RESULTS
Demographic characteristics of study population
The dataset of this study covered 1,627 individuals who had completed baseline anthropometric measurements and diagnosis of cognition at follow-up. As shown in Table 1, the baseline average age of analyzed participants was 71.3 (SD = 7.3) years, and average education was 11.9 (SD = 4.0) years. Women accounted for 54.1% of the study participants. The average BMI was 24.6 (SD = 3.5) kg/m2. The characteristics of education years, hip circumference, waist circumference, WHR, proportion of central obesity, LDL-C, HDL-C, fast glucose, prevalence of type 2 diabetes, stroke, and hypertension were significantly different among three BMI partitions (Table 1).
Demographics of study participants at baseline and follow-up
#Comparison among groups with different BMI categories. *p < 0.05, **p < 0.01. MMSE, Mini-Mental State Examination; APOE ɛ4(+); TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol.
Incidence rate of dementia
After an average follow-up year of 5.3, 136 participants were diagnosed as dementia. Overall dementia incidence was 1.59 (95% CI 1.33–1.87)/100 person-years. And dementia incidences in groups of low, moderate, and high BMI were 3.56 (95% CI 1.71–6.41)/100 person-years, 1.68 (95% CI 1.29–2.14)/100 person-years, and 1.41 (95% CI 1.10–1.78)/100 person-years respectively, which were significantly different (p < 0.05). The higher incidence of dementia was found in participants with low BMI. PH hypothesis testing showed that all models satisfied the PH test (p = 0.33 for Model 1; p = 0.256 for Model 2; p = 0.184 for Model 3; p = 0.171 for Model 4). Cumulative incidence rate of dementia in participants with low BMI was significantly higher than those with moderate and high BMI (log-rank test, p = 0.0051) (Fig. 1).
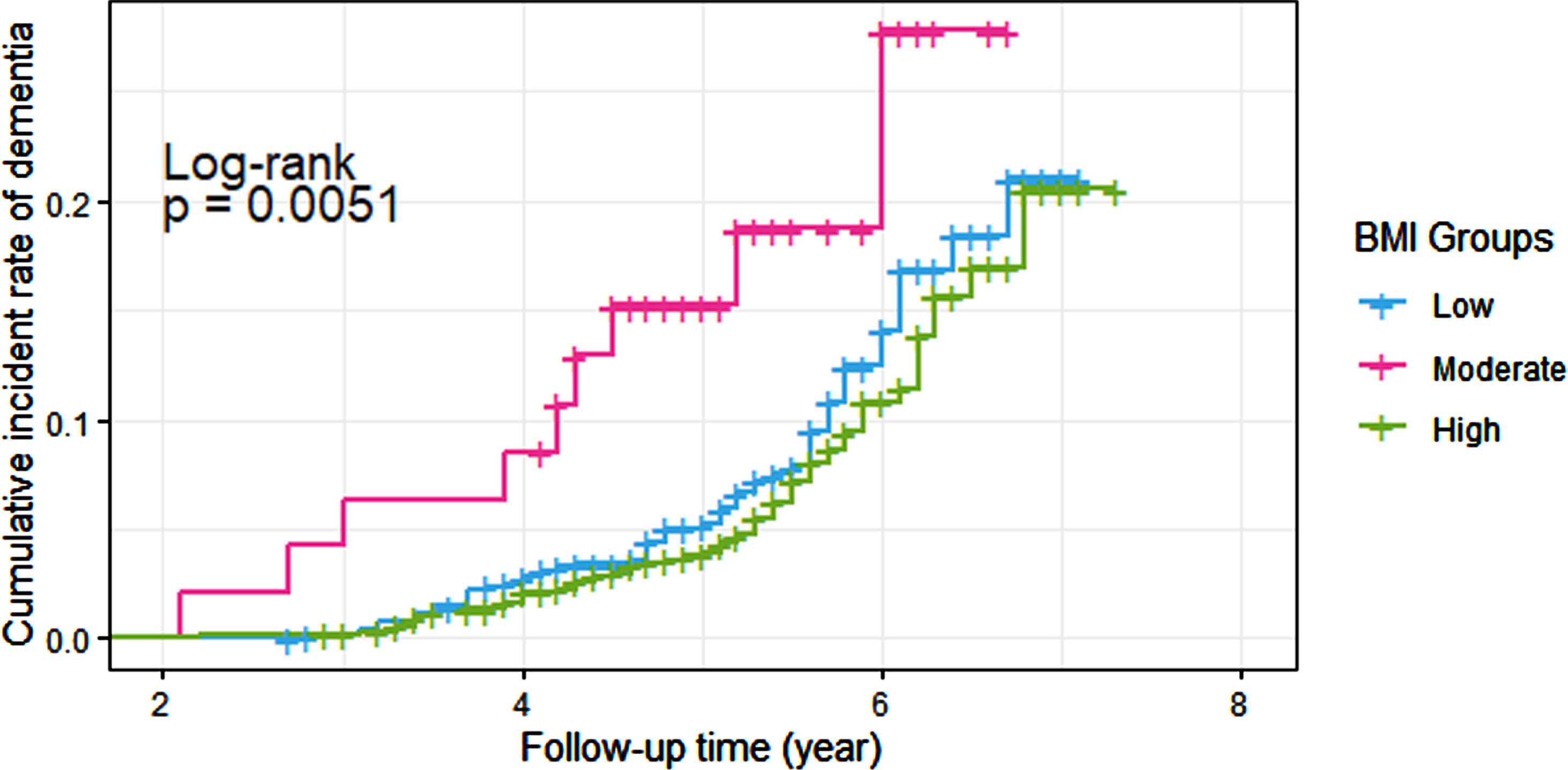
Kaplan-Meier failure curve for incident dementia in three BMI partitions.
Association between BMI and incident dementia
An L-shaped relationship between splined BMI and hazard ratios of dementia was found (Fig. 2). Model 1–3 all showed the same trend of dementia incidence on BMI. As shown in Table 2, Participants with low BMI had increased risk of incident dementia (HR = 2.29 [95% CI 1.13–4.61]) compared with moderate BMI in the unadjusted model (Model 1). The association remained significant (HR = 2.38 [95% CI 1.17–4.85]) after adjusted for age, gender, and years of education (Model 2). Additionally, after adjusted for APOE ɛ4, smoking, alcohol drinking, depression mood, type 2 diabetes, hypertension, hyperlipidemia, and stroke (Model 3), the HR increased compared with Model 1 and 2 (HR = 3.38 [95% CI 1.50–7.63]). However, although with no significance, compared with the reference group, high BMI had slightly reduced risk of dementia in all models. A sensitivity analysis (Model 4) that excluded participants with central obesity demonstrated similar results that low BMI was associated with higher fully-adjusted HR (3.77, 95% CI [1.43–9.92]), while high BMI did not present significant HR increase (1.04, 95% CI [0.63–1.71]). The Bayesian approach also exhibited consistent model parameters but more stable ones than maximum likelihood did.
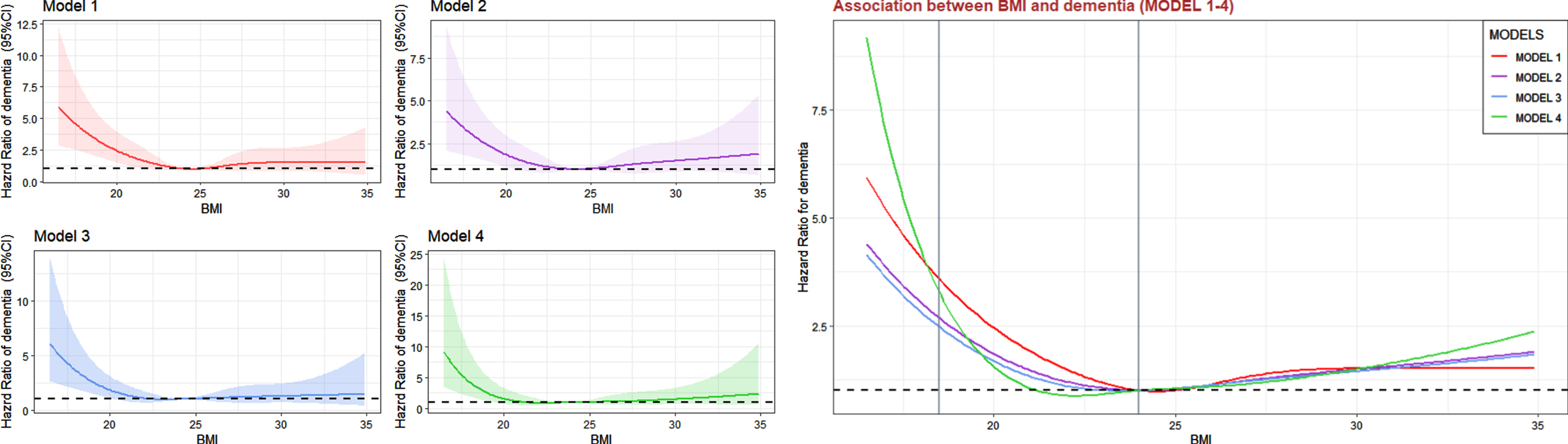
Association between BMI and dementia among old adults (Model 1–4).
BMI-based hazard ratios of incident dementia in Chinese urban elderly
*Model 1 adjusted for BMI. Model 2 adjusted for BMI, age, gender, and education years. Model 3 adjusted for BMI, age, gender, years of education, APOE ɛ4, smoking, alcohol drinking, depression mood, type 2 diabetes, hypertension, hyperlipidemia, and stroke. §Additionally, Model 4 excluded participants with central obesity for sensitivity analysis.
Subgroup analysis
As shown in Fig. 3, the associations of low and high BMI (reference: moderate BMI) with incident dementia were examined in subgroups by multivariate Cox model (Model 3). Among male participants, lower BMI were associated with higher risk of incident dementia (adjusted HR = 3.11, 95% CI 1.19 to 5.03) but no significance association was found in high BMI (adjusted HR = 0.88, 95% CI 0.63 to 1.31). While neither low or high BMI had significance among female. Among participants with stroke, low BMI (n = 7, 3% of strokers) had higher risk of incident dementia (adjusted HR = 7.81, 95% CI 1.49 to 40.9). but low BMI among non-strokers (n = 40, 3% of non-strokers) had much lower HR without significance (adjusted HR = 1.88, 95% CI 0.83 to 4.26). Low BMI tended to have higher risk of incident dementia although they did not reach statistical significance in some subgroups.
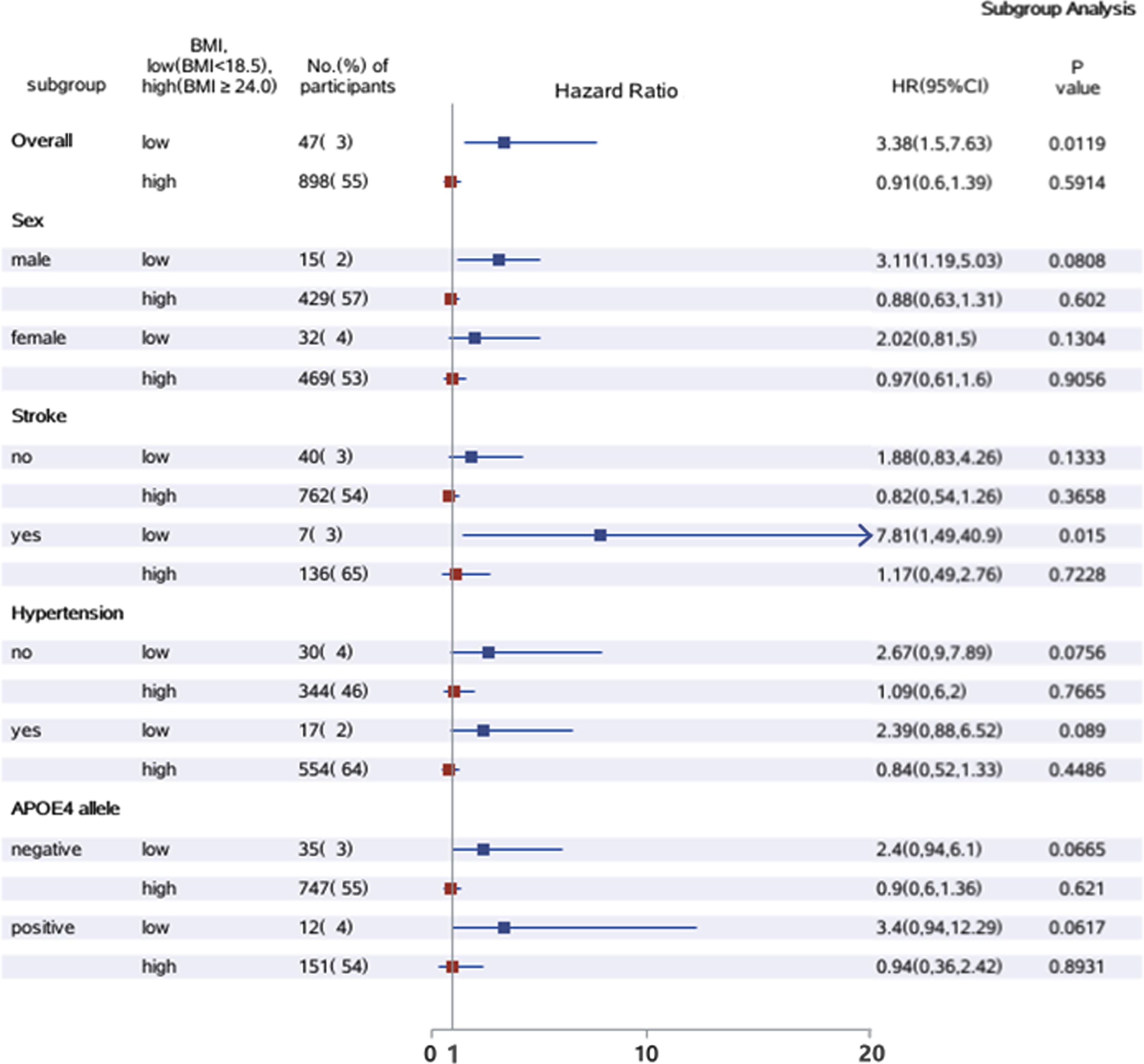
Subgroup analysis of sex, stroke, hypertension, and APOE4 allele of Model 3.
DISCUSSION
This community-based prospective study demonstrated that low BMI was associated with higher risk of dementia in Chinese older adults living in urban area, after controlling for demographic characteristics, lifestyle, mood, biochemical indicators, and medical history of participants. In our study, we conducted a sensitivity analysis in participants without central obesity, and the association was still significant with even higher HR.
Our findings are consistent with some previous studies. A cohort study conducted in Japan suggested that underweight and lower BMI were related to higher incidence of dementia [11]. They observed significant trends of lower BMI and a higher incidence of dementia in both sexes. A meta-analysis included 32 cohort studies among 5 million participants worldwide found that underweight individuals were more likely to have dementia and other neurodegenerative diseases, while being overweight put individuals at a relatively lower risk of dementia compared with normal BMI participants [39]. Qu et al. also indicated that late-life underweight served as a positive risk associated with incident dementia, while overweight and obesity were negatively associated with dementia in old-age people [13].
However, some other studies reported different findings. A cohort study using Clinical Practice Research Datalink (CPRD) in England estimating both short and long-term (10–14.9 years after BMI measurement) associations between BMI and incident dementia found that worse cognition function was significantly associated with being obese in the longer-term [6]. Another prospective study in America found that obese people (BMI≥30 kg/m2) had a 74% increased risk of dementia (HR 1.74, 95% CI 1.34–2.26), while overweight (BMI 25.0–29.9 kg/m2) had a 35% greater risk of dementia compared with those of normal weight (BMI 18.6–24.9 kg/m2) [9]. Sabia et al. indicated that long-term obesity and long-term underweight in adulthood were both associated with lower cognitive scores in late midlife. It was also reported that obesity in middle age increased the risk of future dementia independently of comorbid conditions [40]. In the above three studies, all the cognitive functions were measured mainly by MMSE scores rather than a clinical diagnosis based on neuropsychological and neurological assessments. Their source of participants was health database, same working unit, or certain health plan, which was quite different from our study. It should be noted that they had longer observation time since midlife while we collected data since late life. A meta-analysis conducted by Albanese et al. reported that, midlife obesity may increase the risk of dementia [41]. Kivimäki et al. also indicated that a harmful effect of higher BMI is observable in long follow-up, and a reverse-causation effect that makes a higher BMI to appear protective when the follow-up is short [42], which may help explain the inconsistency between our study and previous articles to a large extent.
Several mechanisms may help to explain the association between reduced BMI and dementia. First, the association of low BMI with dementia onset might be related to changes in body composition [10]. Aging is characterized by the loss of lean body mass [43], while high lean body mass can be protective due to improved glucose metabolism and serum urate, which is positively correlated with BMI, as an antioxidant in the brain to prohibit development of neurodegeneration [44, 45]. Second, BMI is an important WHO recommended indicator of nutritional status measurement [8]. Lower indicators of nutritional status, e.g., BMI, fat mass, and fat free mass index were associated with more medial temporal atrophy scores and microbleeds, with largest effect sizes in MCI [46]. Malnutrition is also a well-recognized risk factor incurrence of unexpected diseases, infections, and deaths among old [47, 48]. Furthermore, physical inactivity, poor diet, and obesity are drivers of insulin dysregulation, which can contribute to conditions of pathological brain aging [49]. Third, lower BMI in late-life may decrease estrogen production as well as leptin hormone levels and adiponectin. Estrogen has been shown to have beneficial effects on the entire bioenergetic system of the brain [50]. Leptin and adiponectin have been found as protective compounds against the development of cognitive decline [51]. Circulating levels of leptin are directly proportional to the amount of adipose tissue in the body [50]. It is bound to receptors on hippocampus and is related to regulation of neuron excitability and prevention of cell death caused by amyloid-β [52–54]. Adiponectin plays an important role in modulating insulin sensitivity and has been suggested to protect against amyloid-β toxicity in AD [55]. This could explain why lower BMI and insufficient levels of estrogen, leptin, and adiponectin at later stages of life are risk factors for dementia [56]. Fourth, interaction between genetic and environmental factors may clarify the underlying mechanism of dementia. It is hypothesized that BMI modified the generic association of APOE ɛ4 allele with cognitive impairment and it is reported that the association of APOE ɛ4 allele with cognition decline was significantly lower in obese participants compared to those with normal BMI [57]. Fifth, lower BMI is negatively related to uric acid, a natural antioxidant that reduces oxidative stress by scavenging free radicals in vitro. Lower levels of uric acid might be associated with relatively sooner cognitive decline [59].
In the subgroup analysis, we found that the association between baseline BMI status and dementia was slightly modified by sex and stroke: men with lower BMI were more likely to develop dementia than women while men with high BMI had less risk to develop dementia. This might because of the interaction of low BMI with gender; strokers with low BMI had higher risk of dementia than non-strokers while non-strokers had similar HR with strokers with high BMI. However, we did not find any different patterns of hypertension and APOE ɛ4 allele subgroups. Nevertheless, the results of subgroups need to be verified in future with lager sample sizes with longer observation time.
There are several strengths of our study. This is a large community-based prospective study with a comprehensive battery of neuropsychological tests involving global cognition, executive function, spatial construction function, memory, language, and attention. To the best of our knowledge, this is one of a few prospective studies based on general older population which explores the association of BMI and the risk of dementia in Asia. Additionally, the present study was based on our previous research experience and also developed our former knowledge on the cross-sectional literature on the approximate U-shape relationship between smoothed BMI and MCI [19].
Our study also had potential limitations. First, our results might be impacted by the relatively high lost-to follow-up rate and the treatment on filling missing data dealing with baseline parameters might result in a more conservative result. Participants included in our study were younger and had higher BMI and MMSE score with lower proportion of complications (type 2 diabetes, hypertension, stroke) at baseline (Table 1); therefore, the association between BMI and dementia incidence might be underestimated. But we applied a Bayesian approach to improve the accuracy of estimates from censored data set. Second, anthropometric measurements were conducted to all the participants throughout a year which might lead to inevitable random errors. However, the data was collected by uniformly-trained investigators using the same model of scales in the morning. Third, there might be a reciprocal causation of BMI and dementia. Participants with dementia or pre-dementia (dementia-to-be) may be more likely to develop eating disorder and malnutrition and thus have more probability to lose weight. Our study had comparatively short observation period since late life, which may make a higher BMI to appear protective. However, the drop of BMI induced by cognitive decline usually happens at the terminal stage of the disease, and we also excluded participants enrolled less than 2 years to lighten the reversal effects. Additionally, our findings may not be well-representative because our study participants had relatively longer education experience as well as better economic status than average conditions in developing areas; but our findings may be comparable with those from developed regions.
Conclusion
Low BMI may contribute to high risk of incident dementia, even in individuals without central obesity. Our study suggests that keeping BMI≥18.5 kg/m2 may be helpful to maintain cognitive function. Being central obese might be associated with a protective influence on underweight participants, while having too much belly fat does no good to cognition preserve on those who were too heavy. Further studies are needed to verify the L-shaped curve of BMI and dementia and explain the potential pathophysiological mechanisms.
Footnotes
ACKNOWLEDGMENTS
This study was supported by the Shanghai Muni-cipal Science and Technology Major Project (2018SHZDZX01) and ZJ LAB, National Natural Science Foundation of China (82173599, 81773513), Key Project of the Ministry of Science and Technology, China (2020YFC2005003, 2021YFE0111800).