
Abstract
Background:
Understanding how the age of dementia symptom onset affects the longitudinal course of dementia can assist with prognosis and care planning.
Objective:
To synthesize evidence regarding the relationship of age of symptom onset with the longitudinal course of sporadic Alzheimer’s disease (AD), vascular dementia (VaD), and frontotemporal dementia (FTD).
Methods:
We searched Medline, CINAHL, Embase, PsycINFO, PubMed, and Scopus for longitudinal studies that examined the impact of sporadic AD, VaD, or FTD symptom onset age on measures of cognition, function, or behavioral symptoms. Studies that examined age at diagnosis only were excluded. Quantitative meta-analysis was conducted where studies reported sufficient data for pooling.
Results:
Thirty studies met all inclusion criteria (people with AD (n = 26), FTD (n = 4)) though no studies examined VaD. Earlier onset of AD was associated with more rapid annual cognitive decline (estimate = –0.07; 95% CI –0.14 to 0.00; p = 0.045). Most studies that stratified their sample reported that younger AD onset (usually < 65 years) was associated with more rapid cognitive decline. Other evidence was inconclusive.
Conclusion:
Younger people with AD appear to have a poorer prognosis in terms of faster cognitive decline than older people with AD. More research is required to determine the impact of symptom onset age in VaD and FTD, and on functional decline in all dementias.
INTRODUCTION
The incidence of dementia increases exponentially with age although up to 10% of people with dementia experience symptom onset in midlife [1]. While directly-inherited (i.e., autosomal-dominant) dementias are more common among those with young onset dementia (15% versus 5%) [2, 3], most cases of both young onset and late onset dementia have sporadic causes.
The most common causes of dementia are Alzheimer’s disease (AD), vascular dementia (VaD), and frontotemporal dementia (FTD), which collectively account for more than 92% of cases [4]. Younger and older people with sporadic AD, FTD, and VaD appear to have a similar risk factor profile [5–7], but younger people present with more severe cortical atrophy and greater neuropathology load than their older counterparts [8, 9]. Younger people are also more likely to report a non-amnestic presentation or other less common early symptoms [3, 10]. Care needs and experiences differ based on differences in life circumstances (for example, being of working age versus retired), health, cohort effects, and frailty [11–13].
Despite these differences, it is not clear whether the longitudinal clinical course of dementia differs with age of onset. A common clinical assumption is that dementias that emerge earlier in life are more aggressive and associated with faster cognitive decline [14]. However, the evidence to support or refute this claim has not yet been synthesized. While some studies demonstrate a faster cognitive decline with younger symptom onset (e.g., [15, 16]), others do not (e.g., [17]). Differences in study design, sampling, assessment, and analysis may account for these differences but the effect of these factors has not been examined. The clinical impact of the rate of neuropathological change may also be moderated by age- and cohort-related factors including genetic factors, cognitive reserve, vascular health, and frailty. In addition, the appropriateness of 65 years as a point at which to divide younger and older people with dementia remains an active matter of debate [11]. Examining differences in the course of clinical symptoms between groups will help to clarify the validity of categorizing people with dementia in this way.
As such, the aim of this review is to synthesize evidence regarding the relationship between age of symptom onset and the longitudinal course of sporadic AD, FTD, and VaD. The research questions are: Is the age at symptom onset associated with the rate of cognitive, functional, and behavioral decline among people with sporadic AD, FTD, and VaD?, and Are there differences in the rate of cognitive, functional, and behavioral decline between those with symptom onset before and after 65 years of age?
A better understanding of the role of age of symptom onset in the longitudinal course of dementia will allow for improved prognostic accuracy and targeted provision of clinical services, as well as tailored support for people with dementia and their supporters based on the estimated rate of change.
METHODS
This systematic review protocol was prospectively registered on the PROSPERO database (CRD42020185931). We report according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [18].
Search strategy
Database searches of titles, abstracts, and keywords were conducted to identify English-language publications describing longitudinal studies that used age of dementia symptom onset as a predictor variable and change in cognition, change in function, or change in neuropsychiatric symptoms as the outcome variable. We used a search strategy that combined terms related to dementia, the outcomes of interest, and a longitudinal design (see Supplementary Table 1 for the full search strategy). Articles published any time to November 2021 were sourced from Medline, CINAHL, Embase, PsycINFO, PubMed, and Scopus. The reference lists of all included studies were hand searched for additional relevant publications.
Included study characteristics
aof 77 at follow up; bcorrelation with age at onset r = 0.95. AD, Alzheimer’s disease; bvFTD, behavioral variant frontotemporal dementia; CBD, corticobasal degeneration; CR, carer-reported; FTD, frontotemporal dementia; LOD, late onset dementia; nr, not reported; P, prospective; PNFA, progressive non-fluent aphasia; PPA, primary progressive aphasia; PSP, progressive supranuclear palsy; R, retrospective; SD, semantic dementia; SR, self-reported; UK, United Kingdom; USA, United States of America; YOD, young onset dementia.
Inclusion and exclusion criteria
Observational studies were included if they: 1) were longitudinal in design; 2) assessed cognition OR function OR neuropsychiatric symptoms as outcome variables using standardized assessments; 3) included age of symptom onset as a predictor variable (either as a continuous variable or dichotomized as younger versus older), and; 4) included people with sporadic (i.e., non-autosomal dominant) AD, VaD, or FTD diagnosed using appropriate diagnostic criteria (e.g., criteria for the diagnosis of AD described by the National Institute of Neurological and Communicative Disorders and Stroke and Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) [19]). Studies that included more than one dementia type were required to report outcomes for each type separately. Studies including only people with directly inherited dementia (e.g., autosomal-dominant AD, CADASIL, autosomal-dominant FTD) were not included because these dementias are known to have a distinct longitudinal course when compared to sporadic cases [20]. However, studies that did not distinguish between sporadic and autosomal-dominant causes of dementia among their sample were retained.
Articles were excluded if: 1) the sample included only people with directly inherited dementia (e.g., autosomal-dominant AD, CADASIL, autosomal-dominant FTD); 2) outcomes were assessed using only imaging or pathology without measurement of clinical features; 3) the predictor variable was age of diagnosis (rather than age at symptom onset); 4) they were trials, single case studies, case-control studies, or cross-sectional studies, or; 5) only a conference abstract was available with insufficient detail about study design, method, or results.
Study selection process
Search results were combined, and duplicate studies removed. Two authors (SD and SR) screened titles and abstracts for relevance and potentially eligible citations were accessed and the full texts reviewed against eligibility criteria. Consensus was reached via discussion and a third author (MC) was consulted in the case of disagreement.
Data extraction
Data was extracted independently by two authors (SD and SR) using a standardized data extraction sheet that was tested with two studies and then revised. Extracted data was reviewed for accuracy by a third author (MC). Data extraction included country, study design, data collection period and measures, sample size, demographics (including age of symptom onset), and relevant results describing the impact of age of symptom onset on cognition, function, and/or behavior.
Assessment of study quality
Two authors (SD and SR) independently evaluated the methodological quality of each study using the Critical Appraisal Skills Programme (CASP) [21] checklist for cohort studies. The checklist asks twelve questions under three broad headings: ‘Is the study valid?’, ‘What are the results?’, and ‘Will the results help locally?’. The CASP cohort checklist assesses the validity and potential sources of bias in cohort studies. CASP checklists are not a tool designed to be scored but rather emphasize transparency in assessing the key indicators of methodological quality [22]. The quality appraisal outcomes were not used in the data synthesis, however a reflection of the quality of the studies is included in the interpretation of the results to identify potential bias.
Data synthesis
Quantitative meta-analysis was conducted where comparable data related to the indicator variable type (i.e., dichotomized versus continuous), outcome, and type of dementia were available. Meta-analysis was conducted using the package robumeta [23] in R, version 4.0.2 (The R Foundation for Statistical Computing). Beta estimates for eligible associations from studies were rescaled to correspond to an association of annual rate of change with each year of age of onset, and the sign of the estimate flipped when necessary so that negative estimates were indicative of younger age of onset associated with faster decline. When standard error (SE) of the beta estimate was not provided the SE was calculated from the p-value according to the procedure detailed in the Cochrane Handbook for Systematic Reviews of Interventions [24]. To account for the non-independence of multiple eligible associations within studies, multivariate analyses were performed using robust variance estimation (RVE) based on a correlational model with rho = 0.8 [25]. Heterogeneity across studies was quantified using τ2 and expressed as a proportion of overall variance using the I2 statistic [26, 27]. Prediction intervals of the pooled estimate were calculated to assess the dispersion of true effects across settings [28]. Small-study effect was assessed by visually inspecting funnel plots of beta estimate versus SE [29]. A sensitivity analysis excluding a study that sampled only participants with young onset dementia [17] was also conducted.
Where additional data were required for inclusion in meta-analysis, we contacted authors of studies published within the past five years. Additional data were not sought for older studies because it was unlikely that data would be retained by the study authors. Where data were not suitable for meta-analysis, a qualitative synthesis was used to examine outcome trends and assess risk of bias.
RESULTS
From 16,559 unique records, most were excluded (n = 16,104) prior to full text-review due to non-relevance or not meeting the inclusion criteria in title and abstract review (Fig. 1). Ninety-nine articles were accessed in full text. Following review, 30 studies met all inclusion criteria by reporting the longitudinal impact of age of dementia symptom onset on cognition, function, or behavior, including two publications reporting on the same dataset [30, 31].
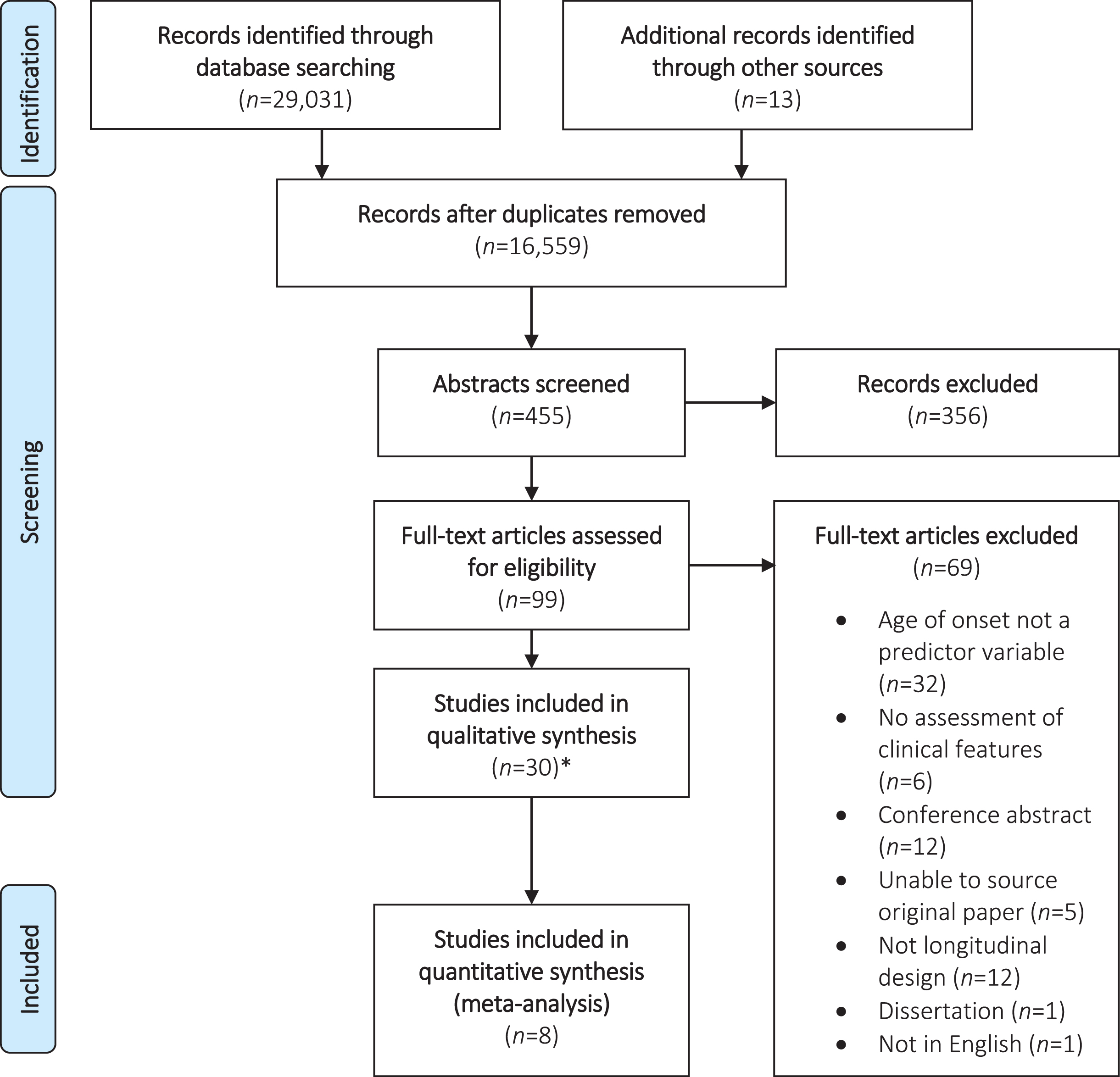
PRISMA Flow Chart. * Includes two publications using the same dataset.
Included studies were published between 1987 and 2021 and most were conducted in the US (Table 1). Most studies included people with AD (n = 27) and four studies included people with FTD variants. There were no studies that included people with VaD. The predictor variable (age of symptom onset) was used as a continuous variable in seventeen studies, four of which also repeated analyses after dichotomizing groups as young onset dementia (YOD) and late onset dementia (LOD) [32–35]. Ten studies used a dichotomized predictor variable only [16, 36–42]. All but two studies that dichotomized groups defined YOD as aged under 65 years at symptom onset; the remaining two studies categorized at±70 years [43, 44]. Outcomes assessed in the included studies included cognition (n = 25), function (n = 11), and behavior (n = 2). Most samples were recruited via specialist diagnostic clinics (n = 15) or research centers (n = 9).
Quality assessment
Results of the quality assessment are presented in Supplementary Table 2. Most studies were well designed to eliminate study bias and adequately identified and managed confounding factors. Common methodological limitations included a small sample size (i.e., fewer than 60 people; n = 7) [30, 45–47] and high levels of attrition from baseline to final assessment without reporting sufficient detail about data loss [32, 48–50]. Two papers did not clearly describe how many participants were retained at follow up or the demographic features of these participants [16, 32]. While all included papers used age of symptom onset as a predictor variable, nine did not report the onset age of their sample in the paper [15, 50]. Seven studies did not report potentially confounding factors (e.g., level of education), nor explain their strategy to manage these factors in their analysis [16, 42–44]. Four studies used composite measures comprised of elements of several standardized assessments to assess cognition, rather than the full standardized measures themselves [30, 51]. None of the studies identified and distinguished between sporadic and autosomal-dominant causes of dementia.
Cognition
Of 12 studies examining the impact of age of symptom onset (as a continuous variable) on longitudinal change in cognition in AD (Table 2), eight reported sufficiently comparable data for meta-analysis. The pooled effect estimate across these eight studies demonstrated that earlier onset of AD symptoms was associated with faster annual cognitive decline (estimate = –0.07; 95% CI –0.14 to 0.00; p = 0.045; τ2 = 0.002; I2 = 83%, Fig. 2). There was substantial heterogeneity between studies and funnel plot asymmetry was visible, indicating possible small-study effect (Fig. 3). The pooled effect estimate remained significant after exclusion of one study that included only participants with young onset dementia [17] (estimate = –0.08; 95% CI –0.16 to –0.01; p = 0.037; τ2 = 0.002; I2 = 84%, Supplementary Figure 1).
Results of studies assessing impact of age on onset on cognition decline in Alzheimer’s disease
aReports indicative rate of decline for onset age 60 years (–1.61) and onset age 70 years (–1.37); bMemory sub-score of SNSB-D; cFrontal/executive function sub-score of the SNSB-D; dtime between assessments not reported; eTime between assessments not reported, range from first to last assessment 7 months to 16 years. ADAS-Cog, Alzheimer’s Disease Assessment Scale-Cognitive Decline Subscale; BIMC, Blessed Information-Memory-Concentration test; CAMCOG, Cambridge Cognitive Examination; CI, confidence interval; C-MMSE, Chinese Mini-Mental Status; COWAT, Controlled Oral Word Association Test; DRS, Dementia Rating Scale; K-BNT, Korean Boston Naming Test; K-MMSE, Korean Mini-Mental Status Examination; LOD, late onset dementia; MMSE, Mini-Mental Status Examination; mMMSE, Modified Mini-Mental Status Examination; nr, not reported; ns, not significant; SD, standard deviation; SE, standard error; SNSB-D, Seoul Neuropsychological Screening Battery; YOD, young onset dementia.
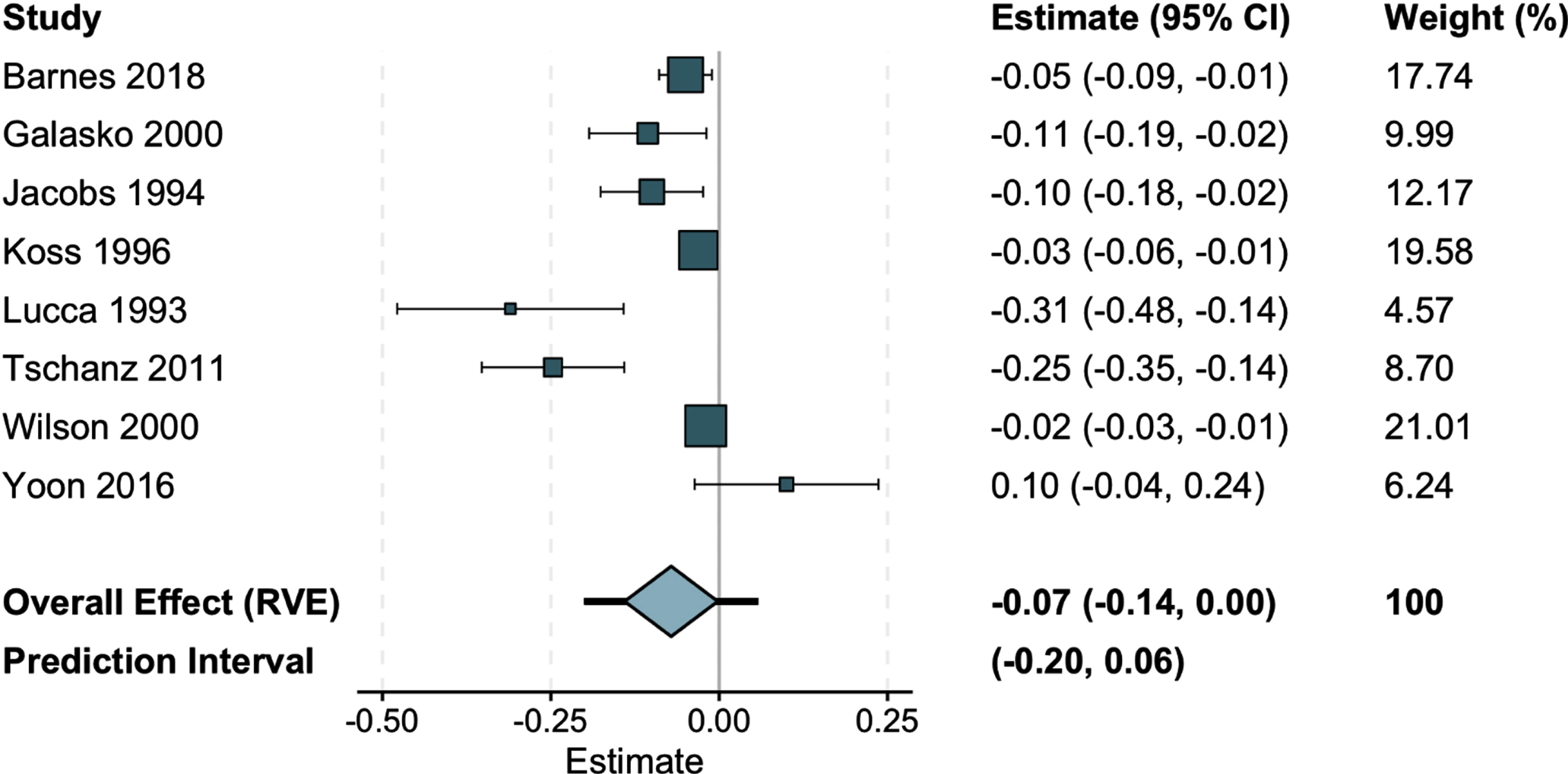
Pooled annual rate of change in cognition with each additional year of age of onset. Tips of the Overall Effect polygon are the upper and lower bounds of the confidence interval; lines extending from the tips represent the prediction interval. CI, confidence interval; RVE, robust variance estimation.
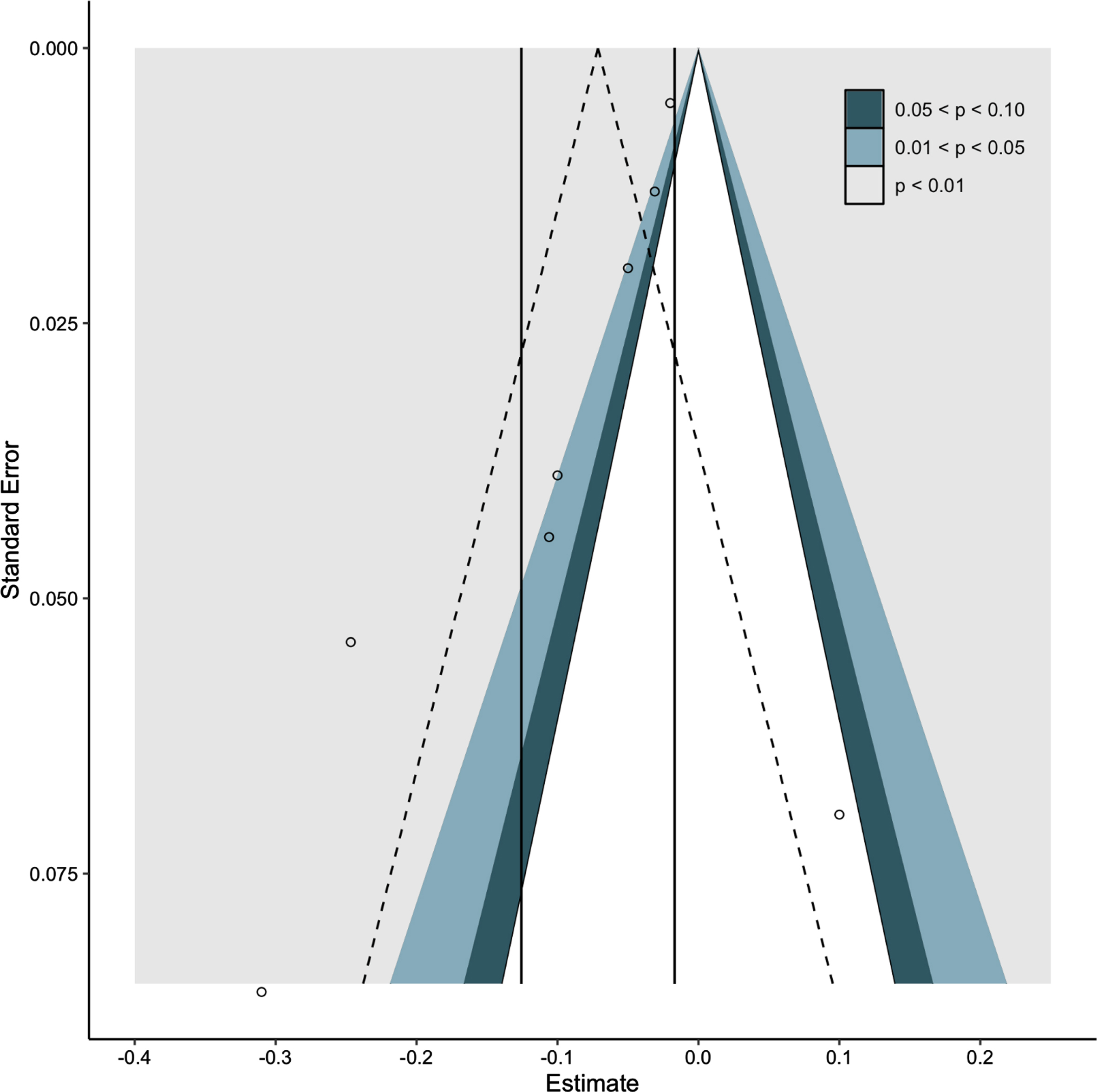
Funnel plot of studies included in meta-analysis.
Two additional papers, not included in meta-analysis because they reported data in a way that could not be used to calculate a standardized effect size (e.g., no reported slope co-efficient), also reported that younger onset of AD was associated with more rapid cognitive decline [52, 53]. The two other studies reported in-text only that age of symptom onset had no significant effect on cognitive decline [34, 54]. Of the 12 studies that dichotomized age at symptom onset, six reported that those with symptom onset prior to 65 years experienced more rapid cognitive decline than those aged 65 years and older [16, 43].
Function and behavior
The eleven papers examining the impact of symptom onset age on the rate of functional and behavioral decline were insufficiently comparable for meta-analysis (Table 3). Functional decline in AD was examined in five studies using the Clinical Dementia Rating Scale Sum of Boxes (CDR-SOB) [15, 56], the Blessed Dementia Scale (BDS) [32], or the Seoul Instrumental Activities of Daily Living scale [17]. Two studies (n = 328, and n = 214 respectively) reported faster functional decline with younger age at symptom onset [15, 52], while one small study (n = 77) reported the opposite effect [32]. Two other studies (n = 3,960 and n = 288 respectively) reported no significant effect of onset age on functional decline [17, 55].
Results of studies assessing impact of age on onset on functional and behavioral outcomes
aSecond deficit or symptom was considered significant when associated to impairment in daily living (e.g., behavioral disorder) according to the patient and family history. AD, Alzheimer’s disease; ADL, Activities of Daily Living; BDS, Blessed Dementia Scale; CDR-SOB, Clinical Dementia Rating Scale Sum of Boxes; CI, confidence interval; FTD, frontotemporal dementia; HR, hazard ratio; IADL, Instrumental Activities of Daily Living; LOD, late onset dementia; NPI, Neuropsychiatric inventory; nr, not reported; ns, not significant to p < 0.05; PPA, primary progressive aphasia; SD, standard deviation; SE, standard error; SIADL, Seoul Instrumental Activities of Daily Living scale; YOD, young onset dementia.
An additional five studies dichotomized younger and older people with AD and compared the rate of functional decline using the BDS [32, 39], the CDR-SOB [30], or a measure of activities of daily living [44]. Results were inconsistent. One found no effect, though their small sample may have been underpowered to detect an effect (n = 54) [39]. A second study did not statistically compare the rate of change between groups but did descriptively report equal average change over 60 months [44]. Two studies reported that younger age at symptom onset was associated with faster decline [30, 33]. Conversely, the fifth study reported that older age was associated with faster decline [32]. The three studies that examined the rate of functional decline among those with FTD found no significant effect of onset age [46, 56].
Two studies examined the impact of dementia onset age on the progression of neuropsychiatric symptoms using the Neuropsychiatric Inventory [15, 48]. Both reported no significant effects for participants with AD. Chow et al. [48] noted that the severity of behavioral symptoms at study entry impacted the relationship between FTD onset age and rate of progression of these symptoms. Those with fewer neuropsychiatric symptoms at baseline (as measured by the NPI) reported no effect of onset age on symptom progression while younger age was associated with worsening of symptoms among those with baseline symptoms of moderate severity. Among those with more severe symptoms at baseline, older age was associated with faster decline.
DISCUSSION
The aim of this review was to identify and synthesize studies that examined the relationship between the age of symptom onset and the longitudinal course of AD, FTD, and VaD. Thirty eligible studies were identified, though none included participants with VaD. Pooled estimates supported the common clinical assumption that earlier onset of AD symptoms is associated with faster cognitive decline. However, evidence regarding the impact of onset age for other dementias and on functional and behavioral decline was inconclusive.
Our pooled analysis identified that each year of delay of onset of AD symptoms is associated with a slowed progression in cognitive impairments. There are several possible mechanisms that may contribute to this effect. Younger people with dementia report high rates of exposure to non-genetic risk factors including cumulative exposures (for example, low educational attainment leading to low complexity lifetime occupation) [57]. These factors may impact the rate of both pre-symptomatic and post-symptomatic AD progression particularly where they inhibit cognitive reserve [58]. Such a suggestion is supported by emerging evidence that the rate of post-symptomatic cognitive decline can be slowed via prevention of modifiable risk exposure (e.g., [59]) Young people are also more likely to carry vulnerability genes, including the apolipoprotein susceptibility gene and its ɛ4 allele (APOE4) [60], and additive exposure to known genome-wide significant loci for dementia modulates the age of onset of AD [61]. The impact of these genetic vulnerabilities on the rate of AD progression remains unclear [62], but one study included in our review noted that the accelerated decline with younger onset age was most pronounced with the additional presence of the APOE4 allele [52]. Some research has suggested that the relationship between susceptibility genes and rate of cognitive decline is modulated by single nucleotide polymorphisms within the genes rather than the mere presence of the genes themselves [63].
Studies examining the impact of AD onset age on the rate of functional decline reported inconsistent results. This may be related to methodological differences between the studies, as two studies that reported a more rapid decline with younger symptom onset included longer follow up periods [15, 52] than those studies that reported no significant effects [17, 55]. In addition, Yoon et al. [17] included only participants with YOD. The impact of AD onset age on functional decline may vary with time and become more pronounced with years lived with the illness. Another possibility is that typical measures of function may be less sensitive to change. Frailty is likely an important confounding factor in this relationship, consistent with data from Barnes et al. [55] demonstrating a sharp increase in the rate of functional decline after age 90. The relationship between dementia onset age and the rate of functional decline may not be linear and the impact of other factors including comorbidity and frailty should be examined in future studies.
We found insufficient evidence about the impact of onset age on the longitudinal course of VaD or FTD. Some studies that included participants with these diagnoses were excluded from this review on the basis that they did not stratify results by dementia type (e.g. [64, 65]). Indeed, cases of ‘pure’ VaD may be relatively uncommon, especially in late life when co-occurring AD and VaD pathology is present in most people with dementia [66]. In addition, FTD is a heterogeneous syndrome group with onset typically before age 65 and with a strong heritability profile [67]. The difficulty with accurately estimating the onset of dementia may have also contributed to the limited number of robust studies in this area. Examination of the clinical course of specific dementia types and the role of onset age is nonetheless warranted because disease-specific data can improve prognostic accuracy and impact upon care planning for people with dementia and their supporters.
Limitations of evidence included in this review
We were surprised by the relatively low number of high-quality studies to include in our review. The use of age at diagnosis as a predictor variable was a common reason for study exclusion and is important because delays to diagnosis of dementia in young people are well documented [68, 69] and can result in misclassification. None of the included studies identified or distinguished between dementias with sporadic and genetic causes, even though there are important differences in the clinical profile and course between them [20]. Many of the included studies were small, and some reported significant drop outs without describing why or the characteristics of those who remained in the study ([32, 37] and, e.g., [49, 50]).
While our review does provide evidence that younger and older groups differ in terms of their rate of cognitive decline, the biological relevance of 65 years as a division point between young- and late-onset dementia remains unclear. The use of linear regression methods to analyze non-linear data in one of our included studies [39] has been previously criticized [70]. Some more recent studies included in this review similarly applied linear analysis techniques without reporting the distribution of their data (e.g., [35]) and several arbitrarily dichotomized groups at±65 years rather than examining the distribution of the outcome data for points of change (e.g., [16, 31]). As such, key inflection points at which the progression of symptoms slows have yet to be identified. Further research to identify these inflection points will be useful for improving prognosis estimation and understanding the clinical relevance of the division of groups at 65 years of age.
The use of the MMSE in many studies of cognitive decline is another potential source of bias in our review. Though the MMSE is a validated and widely-used cognitive screening tool, it lacks sensitivity for measuring cognitive change, particularly for less common forms of dementia. Scores on the MMSE can also be influenced by progressive sensory impairment and language fluency [71], which may be more common early symptoms among younger people with AD than older people [10]. The validity and reliability of each tool will also differ between dementia types. Future studies should consider including a suite of validated measures to examine factors associated with specific cognitive and functional domains.
Strengths and limitations of this review
We searched six comprehensive databases of literature with broad search terms for this review and examined studies for which age of onset was not the primary focus for results to be included. Nonetheless, it is possible that relevant data were missed especially where they were embedded into papers outside the scope of our search terms. Results of only eight of the 24 studies that examined the impact of AD onset age on rate of cognitive decline could be pooled in meta-analysis. Our results may be affected by publication bias, though this possibility is mitigated by the inclusion of several studies for which onset age was not the primary focus of the study.
The use of age of symptom onset, rather than age at diagnosis, was intended to overcome the known differences in delays to diagnosis that occur by age. However, this method has limitations of its own. In most cases, the age of symptom onset is reported by the person with dementia or their carer and is subject to recall bias. The risk of recall bias may change with age as the impact of cognitive and/or functional impairments on familial and employment responsibilities reduces. In addition, the onset of VaD symptoms can be abrupt and closely followed by diagnosis. Our exclusion of studies that only report age of diagnosis may explain why we did not identify any studies of VaD for inclusion. Finally, clinicians may benefit from data that allows for estimating prognosis based on the age at diagnosis. A future review of the impact of diagnosis age on longitudinal outcomes is warranted.
Our exclusion of studies that did not report on individual dementia types is also associated with limitations. As mentioned, most dementias are characterized by a mix of pathologies, particularly co-occurring AD and vascular pathology [4]. Understanding the longitudinal course of these mixed dementias and factors that affect this course will assist with prognosis estimation for a broader population.
Conclusion
This review provides evidence that younger onset of AD is associated with a poorer prognosis in terms of cognitive decline than later life onset. These data can be used for clinical planning and suggest that younger people with AD will require more frequent review over the course of their illness and more rapid access to support services. This has implications for researchers, clinicians, and policy-makers in terms of addressing modifiable risk factors for dementia to potentially delay symptom onset (such as the evidence for physical activity, controlling vascular risk factors, avoiding head injury, hearing loss, and social isolation) [72]. There are economic benefits of slowing progression of cognitive impairments, potential large impacts on quality of life, and also implications for recommendations and access to earlier interventions, potential therapeutics and clinical trials, and for future planning.
The impact of confounding factors like frailty should be examined in future longitudinal studies examining the impact of onset age on functional decline. More research is required to determine the impact of symptom onset age in VaD and FTD, to assist with prognosis and clinical planning.
Footnotes
ACKNOWLEDGMENTS
This research was funded by a Dementia Australia Research Foundation project grant. MC is supported by a South Australian Hospital Research Foundation Early Career Fellowship and a Medical Research Future Fund/National Health and Medical Research Council Investigator Grant. SML is supported by a National Health and Medical Research Council Early Career Fellowship. KEL is supported by an Australian Research Council Discovery Early Career Researchers Fellowship. ABF is supported by a National Health and Medical Research Boosting Dementia Research Leadership Fellowship.