
Abstract
Background:
Subjective cognitive decline (SCD), an at-risk condition of Alzheimer’s disease (AD), can involve various cognitive domains, such as memory, language, planning, and attention.
Objective:
We aim to explore the difference in amyloid load between the single memory domain SCD (sd-SCD) and the multidomain SCD (md-SCD) and assess the relationship of amyloid pathology with quantitative SCD scores and objective cognition.
Methods:
A total of 63 SCD participants from the SILCODE study underwent the clinical evaluation, neuropsychological assessment, and 18F-florbetapir PET scan. Global amyloid standard uptake value ratio (SUVr) was calculated. Additionally, regional amyloid SUVr was quantified in 12 brain regions of interests. A nonparametric rank ANCOVA was used to compare the global and regional amyloid SUVr between the md-SCD (n = 34) and sd-SCD (n = 29) groups. A multiple linear regression analysis was conducted to test the relationship of amyloid SUVr with quantitative SCD scores and objective cognition.
Results:
Compared with individuals with sd-SCD, individuals with md-SCD had increased global amyloid SUVr (F = 5.033, p = 0.029) and regional amyloid SUVr in the left middle temporal gyrus (F = 12.309, p = 0.001; Bonferroni corrected), after controlling for the effects of age, sex, and education. When pooling all SCD participants together, the increased global amyloid SUVr was related with higher SCD-plus sum scores and lower Auditory Verbal Learning Test-delayed recall scores.
Conclusion:
According to our findings, individuals with md-SCD showed higher amyloid accumulation than individuals with sd-SCD, suggesting that md-SCD may experience a more advanced stage of SCD. Additionally, increased global amyloid load was predictive of a poorer episodic memory function in SCD individuals.
INTRODUCTION
Subjective cognitive decline (SCD) refers to the self-perceived cognitive decline without objective cognitive impairment, which is regarded as the first observable clinical indicator of preclinical Alzheimer’s disease (AD) [1–3]. Previous studies have demonstrated that individuals with SCD have an increased risk of AD biomarker abnormalities, subsequent cognitive decline, and conversion to AD dementia [2, 5]. However, SCD is etiologically heterogeneous. Identifying SCD individuals at high risk of dementia is necessary for the early intervention in clinical practice.
Amyloid accumulation, the earliest defining signature of AD [6], starts decades before the initiation of objective cognitive decline and increases continuously during the preclinical stage of AD [7]. Converging findings have established the association of amyloid pathology with the presence and the severity of SCD, suggesting that amyloid accumulation, in many cases, might be the pathological basis underlying the manifestation and progression of SCD [8–10]. Moreover, longitudinal studies have also suggested that higher amyloid load in individuals with SCD was indicative of steeper rate of objective cognitive decline (such as episodic memory, attention/executive and language functions) [11, 12] and higher risk of developing dementia [13, 14]. Exploring specific SCD features which are associated with increased amyloid deposition could be useful to identify a high-risk SCD population.
Memory complaint is the most common symptom in individuals with SCD [15] and its association with amyloid pathology has been widely reported [9, 16]. However, the reported cognitive decline in SCD is not restricted to memory function but can also involve other domains [2, 18]. Several previous studies have found that the self-reported SCD in executive [16], organization [19], and attention [20] functions was also related with amyloid and tau pathology [19]. Additionally, another study revealed a quantitative relationship between the total number of SCD domains involved and lower cerebrospinal fluid (CSF) amyloid-β 42 (Aβ42) levels [21]. According to these findings, it is plausible to assume that the extension of subjective cognitive complaints from single memory domain to multidomain may predict a more severe AD pathological alterations. Thus, we divided SCD participants into two subgroups: single memory domain SCD (sd-SCD) and multidomain SCD (md-SCD); difference in amyloid load between these two SCD subtypes has not yet been studied.
In the present study, we aim to investigate the differences in global and regional amyloid burden between the sd-SCD and md-SCD groups and examine the relationship of amyloid load with quantitative SCD scores and objective cognition in all SCD participants. We hypothesized that individuals with md-SCD would show higher global and regional amyloid burden in AD-signature regions than individuals with sd-SCD. We also estimated that the quantitative SCD scores and the episodic memory function would relate to elevated amyloid burden in all SCD participants.
METHODS
Participants
The present study is a part of the Sino Longitudinal Study on Cognitive Decline (SILCODE), an ongoing longitudinal observational study on cognitive decline, with the main aims to evaluate cognitive decline and to predict the clinical outcome of SCD [22].
A total of 63 individuals with SCD were recruited from local community by advertisement. All participants received the standardized clinical evaluations, physical examinations, and comprehensive neuropsychological assessments. In the present study, SCD is defined with the following criteria: 1) self-experienced memory decline; 2) normal performance on the standardized neuropsychological tests, adjusted by age and education, and failure to meet the criteria for mild cognitive impairment (MCI) or dementia. The exclusion criteria are as follows: 1) A history of other neurological conditions that could cause cognitive decline (e.g., cerebrovascular disease, brain trauma, epilepsy, or Parkinson’s disease); 2) Current major psychiatric disorders (e.g., bipolar disorder, severe depression, or anxiety); 3) Other systematic disease that could cause cognitive decline (e.g., thyroid dysfunction, syphilis, or severe anemia); 4) A history of psychosis or congenital mental developmental delay; 5) A history of substance abuse or traumatic brain injury; 6) contraindications for magnetic resonance imaging (MRI) or positron emission tomography (PET) scanning [22].
The SILCODE study was registered on ClinicalTrials.gov (identifier: NCT03370744). This study was approved by the local ethics committee of Xuanwu Hospital of Capital Medical University (2017[046]), and written informed consent was obtained from all participants after the complete description of the study.
Neuropsychological assessment
Subjective cognition was evaluated using SCD-interview (SCD-I), a semi-structured interview designed by the German Center for Neurodegenerative Disease-Longitudinal Cognitive Impairment and Dementia Study (DELCODE) [21, 24]. The SCD-I allows assessments of SCD in five different cognitive domains (memory, language, planning, attention, other). All interviews were administered by trained study physicians. The interviewer asked for specific changes of mental abilities during the past few years (memory: “Has your memory become worse?”; language: “Do you have increasing word finding difficulties?”; planning: “Do you have increasing difficulties planning ahead or staying organized?”; attention: “Do you make increasingly more errors when not paying full attention to a task?”; others: “Have you noticed any other cognitive changes? Please describe briefly.”). For each endorsed question, the interviewer also asked for the onset time, concerns, comparison with peers, and the history of visiting a physician because of these changes. All questions in this SCD-I were translated into Chinese. If SCD subjects reported SCD only in memory domain, they were classified as sd-SCD group (n = 29). If SCD subjects reported SCD in one or more other cognitive domains (language, planning, attention, and others) besides memory domain, they were classified as md-SCD group (n = 34).
Additionally, the number of fulfilled SCD-plus features (decline in memory, onset within the last 5 years, worries associated with a decline in a cognitive domain, feeling of worse performance than others for the same age group) was calculated (maximum score = 4). Because most subjects were not accompanied by a study partner in our study, we did not take the SCD-plus feature confirmation of cognitive decline by an informant into account when calculating the number of fulfilled SCD-plus features. SCD questionnaire with 9 items (SCD-Q9) was also conducted to quantify the severity of SCD (the range of scores: 0–9) [25, 26]. The questions in SCD-Q9 involve the daily memory function exclusively.
Regarding objective cognition, the global cognition and episodic memory function were evaluated in all SCD subjects. The Auditory Verbal Learning Test (AVLT)-immediate recall, AVLT-delayed recall, and AVLT-recognition were conducted to assess episodic memory function. The Montreal Cognitive Assessment Basic Version (MoCA-B) was conducted to assess global cognition (the range of scores: 0–30) [27].
PET acquisition and preprocessing
All participants underwent 18F-florbetapir PET and T1-weighted MRI scans on a 3.0 T TOF PET/MR scanner (Signa, GE Healthcare) at Xuanwu Hospital of Capital Medical University. For the acquisition of 18F-florbetapir PET data, subjects received an intravenous injection of 7–10 mCi [18F] florbetapir. About 40 min post-injection, a 20 min static PET scan was acquired. The PET data was acquired using a time-of-flight ordered subset expectation maximization algorithm with the following parameters: eight iterations, 32 subsets matrix = 192×192, FOV = 350×350 mm2, half-width height = 3 and correction for attenuation, scatter, random counts, and dead-time. High-resolution T1-weighted anatomical images were acquired using the following parameters: SPGR sequence, field of view (FOV) = 256×256 mm2, matrix = 256×256, slice thickness = 1 mm, gap = 0, slice number = 192, repetition time (TR) = 6.9 ms, echo time (TE) = 2.98 ms, inversion time (TI) = 450 ms, flip angle = 12°, and voxel size = 1×1×1 mm3.
The processing of PET data was performed using PETSurfer (http://surfer.nmr.mgh.harvard.edu/), a set of tools of FreeSurfer for partial volume correction (PVC) [28, 29]. First, a high-resolution segmentation was created for each subject based on the segregation results of the T1-weighted image from the recon-all command. Then, the PET images were registered to the anatomical data of each subject. Next, region of interest (ROI)-based PVC using the symmetric geometric transfer matrix (SGTM) was performed using the ROI of the Desikan-Killiany atlas. Subsequently, the standard uptake value ratio (SUVr) of each region was computed by normalization against the whole cerebellum. The global cortical amyloid SUVr was computed as the average of 68 cortical regions. In addition, the regional amyloid SUVr was quantified in 12 a priori defined ROIs, including the bilateral precuneus, anterior cingulate, posterior cingulate, middle temporal, inferior parietal, and medial orbitofrontal. We selected these ROIs because histopathological [30] and in vivo PET studies [31, 32] have found that they are susceptible to amyloid pathology in the early stage of AD.
Statistical analysis
Group differences in demographics and neuropsychological measures were compared with two-sample t-tests for continuous variables and chi-squared tests for categorical variables. Due to the non-normal distributions of amyloid SUVr, we performed a nonparametric rank analysis of covariance (ANCOVA) [33] to evaluate the differences in global and regional amyloid SUVr between the sd-SCD and md-SCD groups, with age, sex, and years of education as covariates. Bonferroni correction was used for multiple comparisons. Finally, in all SCD participants, a multiple linear regression analysis was employed to determine the relationships of amyloid SUVr with quantitative SCD scores (the number of fulfilled SCD-plus features and SCD-Q9 scores), global cognition (measured by MoCA-B) and episodic memory function (measured by AVLT-immediate recall, delayed recall and recognition) with age, sex, and years of education as covariates. All of the statistical analyses were performed using SPSS v25.00 (IBM).
RESULTS
Demographics and neuropsychological assessment
The demographic and neuropsychological characteristics of all participants are presented in Table 1. No significant difference was found in age, sex, or years of education between the sd-SCD and md-SCD groups (all p > 0.1). Global cognition and episodic memory function exhibited no group difference between the sd-SCD and md-SCD groups (all p > 0.1). A summary of the prevalence of SCD domains is given in Table 1. Out of the 63 SCD individuals, all reported a memory decline, 39.7% endorsed a decline in language function, 34.9% reported a decline in attention, and only 15.9% reported a decline in planning. The md-SCD group had higher number of fulfilled SCD-plus features (t = –3.266, p = 0.002) and higher SCD-Q9 scores (t = –2.724, p = 0.008) compared with the sd-SCD group.
Demographic and neuropsychological differences between the sd-SCD and md-SCD groups
Means and standard deviation are shown for the continuous variables and number and percentage are shown for categorical variables. t value was presented for continuous variables, χ2 values for categorical variables. p value indicates significant differences using the independent t test or χ2 Test for continuous and categorical variables, respectively. p value < 0.05 is reported in bold. sd-SCD, single memory domain subjective cognitive decline; md-SCD, multidomain subjective cognitive decline; AVLT, Auditory Verbal Learning Test; MoCA-B, Montreal; Cognitive Assessment Basic Version; SCD-I, subjective cognitive decline-interview; SCD-Q9, subjective cognitive decline questionnaire with 9 items.
Between-group differences in global and regional amyloid SUVr
Figure 1 summarizes the significant differences in global and regional amyloid SUVr between the sd-SCD and md-SCD groups (p < 0.05; Bonferroni corrected). Compared with the sd-SCD group, the md-SCD group showed significantly increased global amyloid deposition (F = 5.033, p = 0.029; Fig. 1A). In the analyses of regional amyloid SUVr, the md-SCD group showed significantly higher amyloid burden in the left middle temporal gyrus (F = 12.309, p = 0.001, Bonferroni corrected; Fig. 1B), while no elevated amyloid deposition was found in other ROIs after Bonferroni corrections (Table 2).
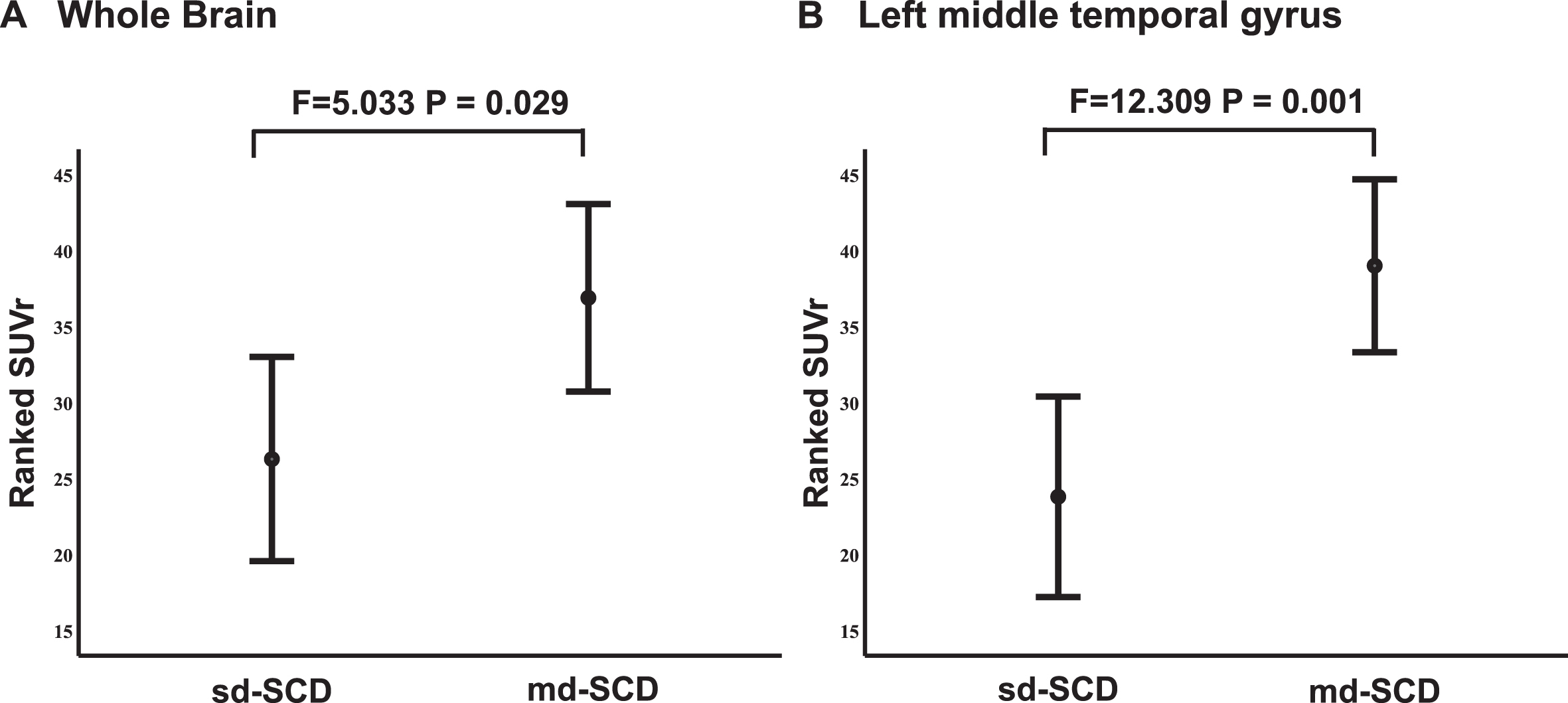
Differences in global and regional amyloid load between the sd-SCD and md-SCD groups. A) The md-SCD group exhibited higher global amyloid SUVr than the sd-SCD group. B) The md-SCD group showed higher amyloid SUVr in the left middle temporal gyrus than the sd-SCD group after Bonferroni corrections. Due to the non-normal distributions of amyloid SUVr, a nonparametric rank ANCOVA was performed, where the effects of age, sex and years of education were controlled. Geometric points indicate mean values of the ranked SUVr, whereas error bars indicate upper and lower 95% confidence intervals. F and p values correspond to the nonparametric rank ANCOVA. sd-SCD, single memory domain subjective cognitive decline; md-SCD, multidomain subjective cognitive decline; SUVr, standard uptake value ratio.
Differences in global and regional amyloid SUVr between the sd-SCD and md-SCD groups
Nonparametric rank ANCOVA was used with age, sex, and years of education as covariates. Median and interquartile range are shown for two groups, as well as p values, to indicate statistically significant group differences. p value < 0.05 in global level and p value < 0.004 (0.05/12, Bonferroni corrected) in ROI level are reported in bold. SUVr, standard uptake value ratio; ROI, region of interest; sd-SCD, single memory domain subjective cognitive decline; md-SCD, multidomain subjective cognitive decline.
Relationship between amyloid SUVr and quantitative SCD scores (the number of fulfilled SCD-plus features and SCD-Q9 scores)
The number of fulfilled SCD-plus features was significantly associated with global amyloid SUVr (standard β= 0.413, p = 0.001) and regional amyloid SUVr in the bilateral precuneus (right: standard β= 0.380, p = 0.002; left: standard β= 0.387, p =0.001), bilateral posterior cingulate cortex (right: standard β= 0.360, p = 0.002; left: standard β=0.393, p = 0.001), bilateral anterior cingulate cortex (right: standard β= 0.408, p = 0.001; left: standard β= 0.402, p = 0.001), right middle temporal cortex (standard β= 0.381, p = 0.002), and right medial orbitofrontal cortex (standard β= 0.424, p < 0.001) after Bonferroni corrections (Table 3). However, there was no significant association between amyloid SUVr and SCD-Q9 scores.
Relationship between amyloid SUVr and quantitative SCD scores in all SCD individuals
Linear regression analysis was used with age, sex, and years of education as covariates. Standard β values, t values, and p values were shown. p value < 0.05 in global level and p value < 0.004 (0.05/12, Bonferroni corrected) in ROI level are reported in bold. SUVr, standard uptake value ratio; ROI, region of interest; SCD-I, subjective cognitive decline-interview; SCD-Q9, subjective cognitive decline questionnaire with 9 items.
Relationship between amyloid SUVr and objective cognition
According to the results of between-group comparisons of amyloid SUVr, global amyloid SUVr and left middle temporal amyloid SUVr were introduced into the multiple linear regression models as independent variables separately. In all SCD participants, there was a negative correlation between global amyloid SUVr and AVLT-delayed recall scores (standard β= –0.282, p = 0.029; Fig. 2). However, there was no significant association between global amyloid SUVr and other cognitive measures. The relationship between left middle temporal amyloid SUVr and objective cognitive measures was also not significant.

Scatter plot of global amyloid SUVr by AVLT delayed recall scores in all SCD participants. Age, sex, and years of education were adjusted. SCD, subjective cognitive decline; SUVr, standard uptake value ratio; AVLT, Auditory Verbal Learning Test.
DISCUSSION
Our main results demonstrated that individuals with md-SCD showed higher global and regional amyloid burden than individuals with sd-SCD. Moreover, the increased global amyloid burden was associated with higher SCD-plus sum scores and lower AVLT-delayed recall scores in all SCD participants. Our findings suggest that, compared with sd-SCD, md-SCD may represent a more advanced stage of SCD and may be at an increased risk of future cognitive decline.
We found that the md-SCD group showed higher amyloid accumulation compared with the sd-SCD group. Several previous studies have reported that the relationship between amyloid pathology and SCD was not restricted to memory but also significant for other SCD domains, including language, executive and attention functions [16, 20]. Another study of CSF amyloid biomarker confirmed that the existence of subjective language complaints indicated lower CSF Aβ42 levels [21]. These findings are actually consistent with our results. In our current research, md-SCD individuals reported SCD in at least one cognitive domain of language, attention, and planning, which have been proven to be associated with higher amyloid burden. Our results showed that, in both the whole sample and the md-SCD subgroup, memory and language difficulties were the most prevalent complaints, followed by subjective attention decline, while complaints in planning were relatively rare. The prevalence of SCD domains in our study was consistent with the only publication with the SCD-I [21]. The results also qualify that the complaints of memory and language difficulties may contribute to the md-SCD report mainly. Additionally, SCD individuals recruited from memory clinic, considered as a frailer SCD population with faster cortical atrophy over time, have been shown to have stronger multidomain SCD report [20, 34]. Although SCD individuals in our study were recruited from the community, our findings support the notion that multidomain SCD reported in community-recruited SCD is also predictive of a more severe amyloid pathology. Also, in line with that multidomain MCI showed severe cortical atrophy and higher risk of dementia than single domain MCI [35], the generalized complaints in md-SCD individuals with higher amyloid burden may alike indicate that they experienced a more advanced stage of SCD and may have greater risk of future cognitive decline than sd-SCD individuals [34]. The current “SCD-plus” criteria, proposed by the SCD-Initiative, is considered as an enrichment strategy for the likelihood of preclinical AD in individuals with SCD [2, 36]. However, characteristics in the criteria were not meant to be arbitrary. Our findings may provide novel evidence that involving single memory domain or multidomain in SCD might be a potential valuable feature of SCD-plus for AD risk and could be used as a simple screening tool for enrichment strategies for clinical trials.
The ROI analysis showed that the brain region with elevated amyloid deposition in md-SCD individuals exclusively located in the left middle temporal gyrus. Histopathological research has revealed the evolution of amyloid deposition in brain, which initiates from the neocortex regions in the preclinical stage, including the temporal, frontal, and parietal cortex [30, 37]. A study in living persons also found the similar result: SCD participants showed higher amyloid burden than healthy controls in the temporal cortex [38], which is consistent with our current result.
We have also evaluated SCD quantitatively and found a significant association between the number of fulfilled SCD-plus features and amyloid pathology in the whole sample. This association is consistent with the study conducted by Miebach et al., where the number of fulfilled SCD-plus features was related with CSF Aβ42 levels [21]. These findings suggest that SCD individuals who endorse more SCD-plus features have higher amyloid burden and may thus be in higher risk of preclinical AD and subsequent conversion to AD dementia. We did not find any association between SCD-Q9 scores and amyloid pathology. However, the Anti-Amyloid Asymptomatic Alzheimer’s (A4) study team has measured SCD using the Cognitive Function Index (CFI) and found that cognitively normal individuals with elevated amyloid burden reported greater subjective cognitive changes on the total CFI score [39]. Further item-level investigation showed that 7 of 15 CFI items reported by participants were associated with amyloid burden, such as whether “a substantial decline in memory” had occurred in the last year, whether the participant had “seen a doctor about memory” and whether the participant had “trouble driving” [40], supporting that only particular patterns of complaints indicate underlying AD pathology.
When pooling all SCD participants together, we found a negative relationship between global amyloid burden and AVLT-delayed recall scores. Although the difference in AVLT-delayed recall scores between the sd-SCD and md-SCD groups did not reach statistical significance, the mean value of AVLT-delayed recall scores in the md-SCD group was slightly lower than that in the sd-SCD group. Our finding agrees with a previous study conducted by Teipel and colleagues [41]. They found that higher global amyloid load was associated with poorer global cognition, episodic memory, and attention function in SCD individuals. Our finding is also supported by the results in healthy individuals [24, 42–46]. A previous study with a large sample has established the association between amyloid deposition and memory performance in cognitively normal individuals [46]. Furthermore, Wolfsgruber et al. recently described that the association between amyloid pathology and cognition was significantly amplified in cognitively normal subjects with SCD versus those without SCD, which indicates that amyloid initially leads to subtle cognitive dysfunction in SCD—the transitional stage between healthy control and MCI [24].
Several limitations of the present study should be considered. First, this is a cross-sectional study; therefore, it is unable to describe the clinical outcome of the sd-SCD and md-SCD groups. However, the ongoing SILCODE study, a longitudinal observational study, will play a vital role in adding support to our present conclusion. Second, in the current study, we assessed the severity of SCD using SCD-Q9, which only involves subjective memory function. Quantifying SCD with a more comprehensive measurement involving various cognitive domains, such as Cognitive Difficult Scale, may be valuable in exploring the association between the severity of SCD and AD pathology. Third, the sample size is relatively small. The validation of the findings in a larger sample is needed.
In summary, our study clarifies the amyloid pathological difference between individuals with sd-SCD and md-SCD. We also verify the association of amyloid burden with the SCD-plus sum scores and the episodic memory function in a Chinese SCD population. According to our findings, md-SCD may represent a more advanced stage of SCD and be at an increased risk of future cognitive decline. Differentiating SCD by involving single memory domain or multiple domains may be used as a simple screening tool for enrichment strategies for clinical trials and early preventions.