
Abstract
Background:
Previous studies have shown that impaired pulmonary function may be associated with cognitive decline, posing the question of whether peak expiratory flow (PEF) % pred could present a modifiable risk factor.
Objective:
To assess the association between PEF% pred and future cognitive function among Chinese participants aged 45 years and above.
Methods:
Data came from four waves fielded by the China Health and Retirement Longitudinal Study. Cognitive function was assessed by a global cognition score. Multivariate linear regression models and generalized estimating equation (GEE) were used to investigate associations between PEF% pred and later cognitive function.
Results:
A total of 2,950 participants were eligible for the final data analysis. After adjustment for baseline cognition and potential confounders, the association remained statistically significant (β = 0.0057, p = 0.027). Domains with increases were focused on episodic memory (β= 0.0028, p = 0.048) and figure drawing (β= 0.0040, p = 0.028). But these associations were not found in women (β= 0.0027, p = 0.379). However, GEE suggested that the rates of decline in global cognition decreased by 0.0096 (p < 0.001) units per year as baseline PEF% pred increased by 1% in middle-aged and elderly individuals, regardless of sex. And higher baseline PEF% pred correlated with declined rates of decrease of in episodic memory, figure drawing, and Telephone Interview of Cognitive Status (TICS).
Conclusion:
Higher baseline PEF% pred was significantly associated with slower cognitive decline in global cognition, episodic memory, figure drawing, and TICS in middle aged and elderly Chinese adults.
INTRODUCTION
Cognitive impairment is a category of mental health disorders that primarily affect cognitive abilities such as learning, memory, perception, and problem solving and is one of the most common chronic conditions in the elderly [1]. In 2016, almost 43.8 million individuals worldwide were diagnosed with dementia [2], with this figure projected to 132 million by 2050 [3]. As the population ages in China, the number of individuals with cognitive impairment is increasing [4]. In 2020, the overall prevalence of mild cognitive impairment (MCI) was 15.5% and of dementia was 6.0%, representing 38.77 million individuals with MCI and 15.07 million individuals with dementia [5]. The increasing number of cognitive impairments contributes to a heavy economic burden, negatively affecting families, communities, and health-care systems around the world [2]. Therefore, to prevent cognitive decline in older adults, it is important to identify risk factors that can be modified.
Impaired pulmonary function is a potentially modifiable risk factor for cognitive decline, which may be caused by ischemic damage to the brain through hypoxia [6]. Peak expiratory flow (PEF) is defined as the maximum instantaneous flow rate generated during expiration, starting after full inspiration and performed with maximal force [7]. PEF% pred is a physiological measure that has been used as one of the most direct measurements of lung function, especially in the diagnosis of asthma [8]. Although it is a rougher measure of lung function than formal spirometry, it is a quickly and easily administered test, which makes it feasible to use as an indicator of general robustness in large surveys and clinical settings [9]. In populations aged 70 years and over, a decreased PEF% pred may increase the risk for dementia [10]. Moreover, PEF% pred is a marker of general robustness in older adults.
Nevertheless, their cross-sectional and longitudinal associations have not been fully investigated. More importantly, little is known about the PEF% pred levels associated with cognitive function in China. Therefore, we used a large nationally representative sample followed up for 7 years, the China Health and Retirement Longitudinal Study (CHARLS), to explore the association between baseline PEF% pred levels and future cognitive function.
METHODS
Participants
The data were obtained from the longitudinal CHARLS survey conducted by the National School of Development at Peking University in China on people above 45 years of age. The details of the sampling design of this survey have been described previously [11]. The survey included four waves covering 150 counties/districts distributed in 28 provinces of China. The baseline (W1) survey was conducted in 2011–2012 on 17,708 participants who were followed up every 2 or 3 years. Of the 13,976 participants, 12,401 participants with baseline PEF were included (903 participants were excluded due to a lack of data, 251 participants were excluded because they were less than 45 years old, and 412 participants were excluded due to stroke/memory-related diseases at W1). The fourth wave (W4) survey successfully reinterviewed 9006 individuals, and 3,395 (27.4%) were lost to follow-up. Finally, 2,950 individuals were included in this study (2,400, 1,936, 1,100, and 620 individuals did not complete the cognitive test and 10-item Center for Epidemiologic Studies Short Depression Scale (CES-D 10) test in W1, W2, W3, and W4, respectively). The study diagram and exclusion criteria are provided in Fig. 1.
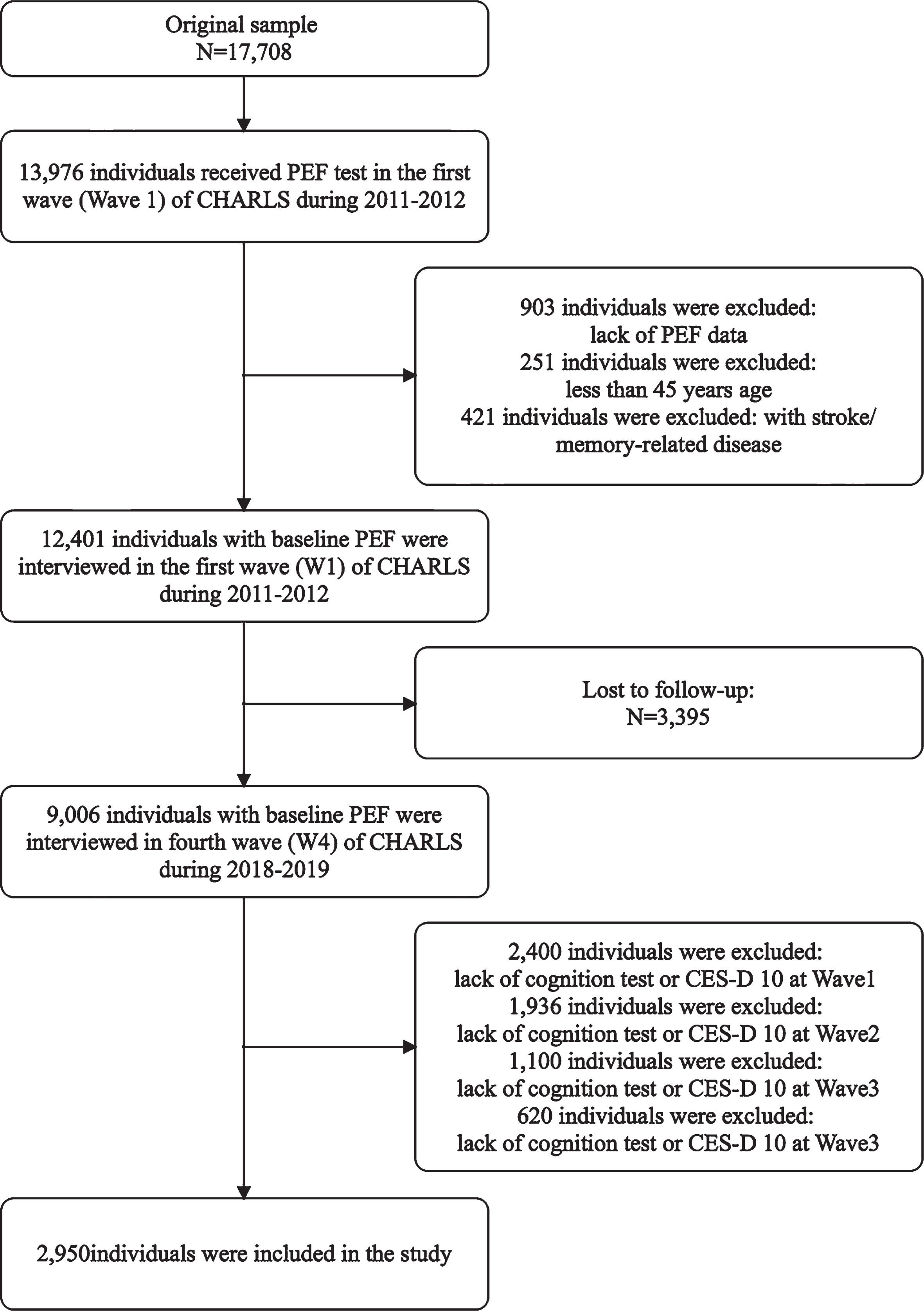
Flow chart of the sample selection and exclusion criteria.
Assessment of cognition
Cognitive function was calculated using three categories: episodic memory, figure drawing, and Telephone Interview of Cognitive Status (TICS). In episodic memory, interviewers were asked to memorize and repeat the words immediately (immediate recall) and five minutes later (delayed recall) after interviewers read 10 Chinese words [12]. The final episodic memory score was the average score of immediate recall and delayed recall, ranging from 0 to 10. The test examined memory function. In the figure-drawing test, the interviewers were shown a picture and asked to redraw it. If the participant failed, the figure-drawing score was 0, and if the participant succeeded, the score was 1 [13]. The test reflected the visuospatial function. In the TICS test, the participants were asked to repeatedly subtract 7 from 100 and to identify the date, season, and day of the week. The scores could range from 0 to 10 [14]. The test reflected numerical ability and time orientation. Serving as the primary outcome, the global cognition score was the sum of the three test scores. The global cognition score ranges from 0 to 21. All tests were tested in Waves 1 to 4.
PEF
PEF (L/min) was estimated through the lung peak flow meter and a disposable blowout with plastic packaging (Shanghai Everpure Medical Plastic Co. Ltd, Shanghai, China). Participants were required to stand and do their best to inhale deeply, hold their breath, and completely seal the blowout with their mouths to avoid air leakage, and do their best to perform the blowout as quickly as possible. The participant needed to repeat the measurement 3 times and select the maximum value as the baseline PEF. Demonstrations were made by trained professionals prior to formal measurements. It is known that age, sex, and body height are determinants of PEF. PEF% pre after being adjusted for age, sex, and height can better reflect the condition of an individual’s lung function. Therefore, we decided to use PEF% pred for data analysis. We can calculate PEF% pred based on the measured and predicted PEF. PEF% pred = PEF/predicted PEF*100 (Male predicted PEF (L/min) = 75.6 + 20.4×age-0.41×age2+0.002×age3+1.19×Height, Female predicted PEF = 282.0 + 1.79×age-0.046×age2+0.68×Height).
Potential confounders
Because of socioeconomic status, the cognitive function of older women in China is lower than that of men. A cross-sectional study reported gender differences when assessing dementia or MCI among the elderly in China. Therefore, we studied men and women separately.
The other covariates included age, residential area, geographic region, educational attainment, smoking, drinking, body mass index (BMI), depressive symptoms, hypertension, dyslipidemia, diabetes or high blood sugar, history of chronic lung disease and asthma. Participants were classified into thin (BMI <18.5 kg/m2), normal (18.5 kg/m2 ≤BMI <24 kg/m2), and overweight (BMI ≥24 kg/m2) groups. The residential area was classified as urban and rural, which was categorized into six geographic regions, namely, East China, North China, Northeast China, Northwest China, South Central China, and Southwest China. Educational attainment was classified as illiterate, literate (did not finish primary school), primary education, middle-school education, and high school education and above. Smoking and drinking habits were classified as either “never” or “yes”. Depressive symptoms were assessed using the CES-D 10 test. The cutoff point for depressive symptoms was 10 [15, 16]. Others were dichotomized as either “no” or “yes.”
Statistical analysis
Descriptive statistics are used to show the characteristics of the study from Wave 1 to Wave 4. Normally distributed metrical data are represented as the mean±SD. Categorical data are presented as absolute counts and percentages. Sktests were performed to assess normality, and Bartlett’s test was performed to assess the homogeneity of variances, followed by ANOVA (for parametric data: p < 0.05 by sktest and p > 0.05 by Bartlett’s test) or Kruskal–Wallis test (for nonparametric data: p < 0.05 by sktest or p < 0.05 by Bartlett’s test). In addition, the Mantel–Haenszel chi-square test was also used for comparison of characteristics from Wave 1 to Wave 4. Linear correlations between baseline PEF and cognitive function in W4 were estimated using multivariate linear regression models (MLRMs) with potential confounders. A generalized estimating equation (GEE) was used to examine the predictive capability of baseline PEF for changes in cognitive function over a period of 7 years. First, MLRMs were used to analyze the association between baseline PEF% pred and cognitive function in Wave 4. Model 1 was adjusted for age, education, residential area, and geographic region. Model 2 was adjusted for Model 1+BMI, smoking, drinking, depression, hypertension, dyslipidemia, diabetes or high blood sugar, history of chronic lung disease and asthma. Then, the association was further analyzed after adjusting for baseline cognition. Model 1′ and Model 2′ were further adjusted as Model 1 and Model 2 with baseline cognition, respectively. Data cleaning and analysis were performed using Stata statistical software (version 15.0; Stata Corporation, College Station, TX, USA). A P value <0.05 was regarded as statistically significant.
Ethics statement
Ethics approval for the data collection in the CHARLS was obtained from the Biomedical Ethics Review Committee of Peking University (IRB00001052–11015). Ethics approval for the use of CHARLS data was obtained from the University of Newcastle Human Research Ethics Committee (H-2015-0290).
RESULTS
Demographic and health characteristics in Wave 1 to Wave 4
A total of 2,950 participants (1,650 men and 1,300 women) aged 45 years old and over were included in the current study. The mean±SD of baseline PEF% pred among the male and female participants was 85.28±0.38% and 85.28±0.38%, respectively. At baseline, the mean age of the individuals was 56.3±0.1 years, and follow-up was performed in 2013, 2015, and 2018. Meanwhile, 12.3% of the participants were from urban areas. The gender, residence setting, geographic region and educational attainment of those participants were consistent with the baseline at the 3 follow-up visits. We found that global cognition function (p < 0.001) decreased with prolonged follow-up among those aged 45 years old and over. The trend was attributed to a decline in TICS (p < 0.001) and visuospatial function (p < 0.001) over time. We found that the number of participants with different BMIs significantly varied between different waves. Additionally, patients with hypertension, dyslipidemia, diabetes or high blood sugar, chronic lung disease, asthma, depressive symptoms, and smokers increased gradually with prolonged follow-up (p < 0.001). We found no statistically significant difference in drinking between the four waves. The demographic and health characteristics of the study population in Wave 1 to Wave 4 are presented in Table 1.
Demographic and health characteristics of the study population in Wave1 to Wave 4
aANOVA test, bKruskal-Wallis test, cMantel-Haenszel Chi-square test.
Association between baseline PEF% pred and cognitive function in Wave 4 by MLRMs
For males, a higher baseline PEF% pred was significantly associated with a higher global cognition score in Wave 4 (p < 0.001 for both Model 1 and Model 2). The domains with increases were focused on episodic memory (p < 0.001 for Model 1 and p = 0.001 for Model 2), figure drawing (p = 0.016 for Model 1 and p = 0.007 for Model 2) and TICS (p = 0.003 for Model 1 and p = 0.007 for Model 2). For females, a higher baseline PEF% pred was also significantly associated with a higher global cognition score in Wave 4 (p = 0.006 for both Model 1 and p = 0.007 Model 2). The domain showing an increased score was TICS (p = 0.005) in Model 1 but TICS (p = 0.007) and figure drawing (p = 0.010) in Model 2 (Table 2).
Association between baseline PEF% pred and cognition function in Wave 4 by multivariate linear regression
Model 1: adjusted for age, education, residential area, Geographic region. Model 2: adjusted for Model 1+BMI, smoking, drinking, depression, hypertension, dyslipidemia, diabetes or high blood sugar, history of chronic lung disease, and asthma.
Association between baseline PEF% pred and cognitive function in Wave 4 after adjusting for baseline cognition by MLRMs
After adding baseline cognition function (Wave 1) as a covariate in males, a higher baseline PEF% pred was significantly associated with a higher global cognition score in Wave 4 (p = 0.013 for Model 1′ and p = 0.027 for Model 2′). Domains showing increased scores were episodic memory (p = 0.019 for Model 1′ and p = 0.048 for Model 2′) and figure drawing (p = 0.038 for Model 1′ and p = 0.028 for Model 2′). After adjusting for potential confounders and baseline cognition, we found no evidence for associations between baseline PEF% pred and cognition score in females (Table 3).
Association between baseline PEF% pred and cognitive in Wave 4 after adjusting for baseline cognition by multivariate linear regression
Model 1′: adjusted for baseline cognition+ Model 1. Model 2′: adjusted for baseline cognition+ Model 2.
Longitudinal cognition at baseline PEF% pred among middle-aged and elderly Chinese participants: GEE. Adjusted for all potential confounders
Table 4 summarizes the results from the GEE for baseline PEF% pred as a predictor of cognition over a period of 7 years among middle-aged and elderly Chinese participants.
Longitudinal cognition by baseline PEF% pred among middle-aged and elderly Chinese participants: Generalized estimating equation
Adjusted for all potential confounders.
GEE suggested that the rates of decline in global cognition decreased by 0.0096 (p < 0.001) units per year as baseline PEF% pred increased by 1% in middle-aged and elderly individuals, regardless of sex. And higher baseline PEF% pred correlated with declined rates of decrease of in episodic memory, figure drawing and TICS.
DISCUSSION
As one of the longest prospective follow-up studies on this topic among people aged 45 and older in China, we revealed that higher baseline PEF% pred was significantly associated with slower cognitive decline in global cognition, episodic memory, figure drawing, and TICS in middle aged and elderly Chinese adults. The major findings of the study indicated that global cognition function decreased with prolonged follow-up. In addition, as the level of baseline PEF% pred increases, the rate of decline in global cognition slowed even after adjustments for cognitive function at baseline and other potential confounders, regardless of sex. Higher baseline PEF% pred correlated with declined rates of decrease of in episodic memory, figure drawing, and TICS.
Previous studies demonstrated that dementia was related to several well-known risk factors, including education, age, body mass index, living in rural areas, geographic region, smoking, drinking, hypertension, dyslipidemia, diabetes or high blood sugar, history of chronic lung disease, asthma, and depressive symptoms [5, 17–24]. Therefore, we adjusted for the above relevant known confounders and baseline cognitive function to better explore the relationship between PEF% pred and later cognitive function.
We used MLRMs to explore the associations between baseline PEF% pred and cognitive function 7 years later after adjustments for baseline cognition and other potential confounders. The results found that a higher baseline PEF% pred was significantly associated with a higher global cognition score (p = 0.027 for Model 2′), and the domains showing increased scores were episodic memory (p = 0.048 for Model 2′) and figure drawing (p = 0.028 for Model 2′) in men. However, there was no evidence for associations between baseline PEF% pred and cognition scores in women. However, the GEE model took into account the association of cognitive function and time, which demonstrated that the rates of decline in global cognition decreased by 0.0096 (p < 0.001) units per year as baseline PEF% pred increased by 1% in middle-aged and elderly individuals, regardless of sex. And higher baseline PEF% pred correlated with declined rates of decrease of in episodic memory, figure drawing, and TICS. In fact, longitudinal data at multiple time points can be used to accurately infer the causal relationship between variables. Our study found that PEF% pred may be an independent factor of cognitive status among middle-aged and elderly Chinese, which was similar to the finding of the previous study [25]. However, there are several differences between this study and the present study. First, the longitudinal follow-up period (7 years) in our study was longer than that in the study (nearly 5 years), and the data were complete from each follow-up in every respect. Second, we used PEF% pred for analysis to reduce the impact of sex, age, and height on PEF. Third, the PEF% pred data were treated as a continuous variable in our study, and we performed a separate sex-stratified analysis. However, pulmonary function was grouped by quintiles of PEF. Fourth, the age of the enrolled subjects (≥45 years) in our study was lower than that in the previous study (≥50 years). Our research demonstrated that PEF% pred was significantly associated with future cognitive function. Therefore, improving respiratory function may help delay the cognitive-function decline.
In fact, a previous systematic review including 10 studies relating lung function to later dementia risk and 11 studies on respiratory disease and dementia demonstrated that individuals with poor pulmonary function experience have an increased risk of dementia [17]. An additional study found that midlife reduced pulmonary function and that pulmonary disorders were associated with modestly increased odds of MCI and dementia later in life [26]. Nevertheless, the main indicators of pulmonary function in these studies were forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC). PEF, as a quickly and easily administered test, was to be ignored. In addition, a 29-year longitudinal study suggested that the level of PEF in midlife was negatively associated with developing dementia risk in later life among women [27], which was consistent with our research. Meanwhile, a cross-sectional study showed that decreased PEF may increase the risk for dementia in the population aged 70 years and older [10]. Specifically, these findings suggested that the PEF level was correlated with cognitive function. The level of PEF, as a measure of lung function, can reflect the oxygen deficiency level to some extent. Recent evidence indicates that hypoxia and proinflammatory mediators of neuroinflammation may precede cognitive decline [28]. Inflammation caused by hypoxia has been shown to cause tissue damage and neurological defects in the central nervous system associated with the elevation of nuclear transcription factors that rely on oxygen. The increase in hypoxic induction factor-1α precedes white matter damage and neuroinflammation [29]. However, frailty-associated indicators were not included as a confounding factor in this study due to the high number of missing values in the database. In fact, a longitudinal study (follow-up 6 years) showed PEF is associated with frailty development [9]. The association between PEF and frailty can be explained by the loss of muscle strength, quantity, and quality that characterizes the aging process [30]. Therefore, it is necessary to include frailty-associated indicators as the collection objects in the analysis of covariates in future studies.
This study has the following advantages. First, the CHARLS is a nationally representative survey targeting populations aged 45 and older, which enabled us to estimate the correlation between PEF and cognitive function in this age group. Second, in this study, the GEE model was used to analyze longitudinal data, and the data were complete at each time point, which could more accurately reflect the causal relationship between variables. Third, strict quality control ensured high quality and the reliability of the findings. However, this study also has several limitations. First, we excluded subjects with incomplete data for various aspects of our analysis, which may have induced information bias. Second, the study did not analyze the competing risk of death due to the lack of details on lost at follow-up. Third, frailty-associated indicators were not analyzed due to the high number of missing data. Fourth, the follow-up was only seven years in our study, and future studies with longer follow-ups are needed, particularly if dementia is the primary outcome.
In conclusion, higher baseline level of PEF% pred was significantly associated with slower cognitive decline in global cognition, episodic memory, figure drawing and TICS in middle aged and elderly Chinese adults. Thus, respiratory health is important for cognitive function, and improving lifestyle and lung function or treating respiratory problems may help reduce the risk of dementia.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/21-5407r2).